Wrappin’ Up Rhythm – Wrappin’ Up Rhythm – ECG that is…ECG that is…
Degrees of DysrrhytmiasDegrees of Dysrrhytmias
Minor: Does not significantly reduce Cardiac Output
Major: Significant reduction in Cardiac Output and coronary blood flow
Lethal: Cardiac Output is negligible
Examples of “Minor” Examples of “Minor” Dysrrythmias:Dysrrythmias:
Atrial FibrillationAtrial output is negligible but only
contributes 20-30% to total COOccassional to frequent PVC’s*Atrial FlutterPJC, PAC
* In otherwise uncompromised heart
Examples of Major Examples of Major Dysrrythmias:Dysrrythmias: Supraventricular Tachycardia:
Sinus Tachycardia* Paroxysmal Atrial Tachy (PAT) Paroxysmal Junctional Tachy (PJT)
Atrioventricular Block: R- R rate is between 20-40
Extreme Bradycardia *Coronaries fill between T- P
waves (Diastole)
Examples of Lethal Examples of Lethal Arryhthmias:Arryhthmias:
Cardiac Output is negligible Sustained V-TachV-FibVentricular
Standstill/Asystole: “Flat Line”

More on PVC’sMore on PVC’s PVC’s are “ubiquitous” and
usually “innocuous” Easy to Spot: No P wave and
wide and bizarre QRS complex Generally followed by
Compensatory Pause: Impulse doesn’t pass retrograde back to AV node, must “wait” for SA node to reset
However: However: 80-90% of Infarcting
patients have them: Some are more “ominous” than others:Multiform (focus)2+ consecutive PVC’s“R - on – T”
–PVC is so early it initiates V-Fib

The Prognostic Strength The Prognostic Strength of PVC’sof PVC’s Not “Independent” predictors BUT when accompanied by
Infarction Ischemia LV dysfunction PVC’s of LV Foci (+ in V1)
Should Not Be Ignored!

CONDUCTION CONDUCTION ARRHYTHMIASARRHYTHMIAS
Springhouse: Chapter 8

Ectopic Focus or Ectopic Focus or Conduction Disturbance?Conduction Disturbance? Ectopic Beats:
Premature and/or wide QRS complexes
Absent and / or abnormal P waves AV Blocks:
Prolonged P-R intervals Irregular P:R ratios
Ventricular blocks: Bundle Branch Blocks Wide QRS / Normal P-R

Bottom Line:Bottom Line:The Speed of conduction in the
Atria and ventricles is similar (Very Fast)
The AV Node Necessarily slows down conduction to allow time for the ventricles to fill before contraction
About 50% of the cardiac cycle is “held up” at the AV-Node
BLOCKS:BLOCKS:Conduction is slowed or
interruptedA-V Blocks occur in the
conduction between the atria and ventricles
Ventricular Blocks: Occur in the Bundle Branches

12 Lead ECG12 Lead ECGClinical Exercise Clinical Exercise
ElectrocardiographyElectrocardiography
Springhouse: Chapter 11
and
Brubaker et. al: Chapter 6
Clinical Indications for Clinical Indications for Exercise Testing:Exercise Testing:
Diagnosis: Reproduce symptoms CP, SOB, Poor work tolerance ECG changes?
Functional Testing: Work Capacity, BP response to exercise, Exercise
duration
Prognosis: AHA, AACVPR, ACP: Risk Stratification, Duke’s
5-Year Mortality prognosis
(Brubaker Chapter 7)
Diagnosis:Diagnosis:
Indications:Confirm or rule out suspected
myocardial ischemiaMechanisms for syncope (LOC)Suspected arrhythmias
(palpitations with symptoms) during exercise
Functional Capacity:Functional Capacity:Indications:
Assessing work capacity for return to work/leisure activites
Used in determining risk/prognostic stratification
Used in determining therapy choices
Exercise Prescription: Phase II Entrance requirements

Prognostic BenchmarksPrognostic Benchmarks<5 METs: poor prognosis
especially under 65 years old10 METs: considered normal
fitness: survival good – regardless of intervention
13 METs: good prognosis even with CAD present
Contraindications: Contraindications: ACSM Guidelines
Co-existing conditions or unstable cardiovascular statusRecent AMIUnstable anginaCHFRBP >200/120Active infectionsUncontrolled Diabetes, other
endocrine disorders
Stress Test ProtocolsStress Test Protocols
ACSMAHAModalities
Bicycle Ergometer
Treadmill

BikeBike vs. vs. TreadmillTreadmill
Less expensiveLess spaceQuieterLess ECG
artifactEasier BP’sNon-Weight
dependent
More flexibility in protocols
More reproducible (not-patient dependent)
More accurate work determinations
Disadvantages? Homework Disadvantages? Homework – Due Tuesday– Due Tuesday
Brubaker: Chapter 6Brubaker: Chapter 6List the disadvantages of each
modalityDescribe the variables monitored
and the recommended intervals for monitoring them before, during and after the test
Treadmill Protocols:Treadmill Protocols:Treadmill Speed: IndividualizeIncrement Size: Age, condition
Larger incremental increases for younger, more fit patients
Smaller incremental increases for elderly, de-conditioned
Test Length: Between 8-12 minutes

Estimating Work Capacity: Estimating Work Capacity: Selecting ProtocolsSelecting ProtocolsHealthy Men >40 years old
75% have 12.5 MET capacity50% ~ 10 METs
Healthy Women >40 years old75% have 10 MET capacity50% ~8-9 METs
Choose a protocol that achieves the estimated MET capacity between 8-12 minutes
Commonly Used Clinical Commonly Used Clinical Protocols: Protocols: Naughton: 2.0 mph X 3.5%
increases every 2 minutesMax METs = 9 /16 minutes
Balke: 3.3 mph X 3% increases every 3 minutesMax METs = 12 /18 minutes
McHenry: Similar to Balke but Stage I is 2.0 mph/3% grade
Critical Measurements:Critical Measurements:Work Loads: MET calculationsECG: Clean ST-Segment
changesBP: Accurate work SBP/DBPRPP: MVO2 eliciting CPElicited Symptoms: CP, SOB,
Syncope, RPE
Rating Anginal Rating Anginal Symptoms: Symptoms:
1+: Light, barely noticeable
2+: Moderate, bothersome
3+: Severe, very uncomfortable
4+: Most severe pain ever experienced
Exercise Test Endpoints:Exercise Test Endpoints:Pre-determined HR achievedPre-determined Workload achievedPatient c/o CP, SOB, leg pains,
fatigueECG changes:
Significant ST changesNew Bundle branch or AV block Increasing PVC frequency, VT or Fib

Post Exercise Period: Post Exercise Period: For Maximal Diagnostic
Sensitivity:No Cool Down10-sec ECG immediately 6-8 minutes of supine monitoring*
- record ECG every minute or after any irregularity
*Unless patient is severely dyspneic – then sitting preferred

Testing Competencies: Testing Competencies:
Know Absolute and Relative indications for test termination:3+ to 4+ anginaSuspected MIDrop in SBP with increased workSerious arrhythmiasSigns of poor perfusionPatient request
12-Lead ECG 12-Lead ECG InterpretationsInterpretations

Why a 12-Lead ECG?Why a 12-Lead ECG?
Gives a “3-D” view of the heart
Especially important in revealing ischemia / infarct
Is more sensitive in assessing LV function

Prepping the Patient:Prepping the Patient: Electrode Sites:
Flat, Fleshy (not over bone/large muscles
Shave excess hair Clean excess oil –
alcohol scrub
Respect Modesty! Use a drape Explain procedure
12-Lead ECG: Electrode 12-Lead ECG: Electrode PlacementPlacementRA/LA:
On Shoulders at distal ends of clavicles: (Not over large muscle masses or directly over bone)
RL/LL:Base of Torso: Just medial to the
iliac crests Chest Leads: V1-V6
Traditional pre-cordial positioning

V1-V2: 4th intercostal space –R/L of sternumV4: 5th intercostal space – midclavicle lineV3: Between V2 and V4V5: At horizontal level of V4, anterior to axillaV6: Midaxillary at horizontal level of V4

Terminology: Terminology: Lead: Recording the wave of
depolarization between negative and positive electrodes
Einthoven Triangle: An equilateral triangle depicting the leads of the frontal plane (I-III and aVR – aVL)
Frontal Plane: Vertical plane of the body, separating the front from back
Transverse Plane: Horizontal plane separating the top from the bottom

Frontal Plane Leads:Frontal Plane Leads:Standard (bipolar) Leads:
I: RA- to LA+ II: RA- to LL+ III: LA- to LL+
Augmented Vector (Unipolar) LeadsaVR: to RA+aVL: to LA+aVF: to LL+

Blue Segment: -30° to +90° Is normal “QRS axis”

QRS Axis?QRS Axis?
Used to determine right or left heart hypertrophy or other anatomical anomalies
But How do we Determine Axis?

The heart is situated in The heart is situated in the chest at an angle from the chest at an angle from right arm to left hip:right arm to left hip:
Waves of Depolarization Travel from theRight shoulder To the left hip.
The ECG deflection (-/+) is The ECG deflection (-/+) is determined by the direction determined by the direction of the depolarization wave of the depolarization wave relative to the “reading” or relative to the “reading” or POSITIVE electrodePOSITIVE electrode

Like So:Like So:
- +
Depolarization wave
Lead I
ECG:
- +
- +
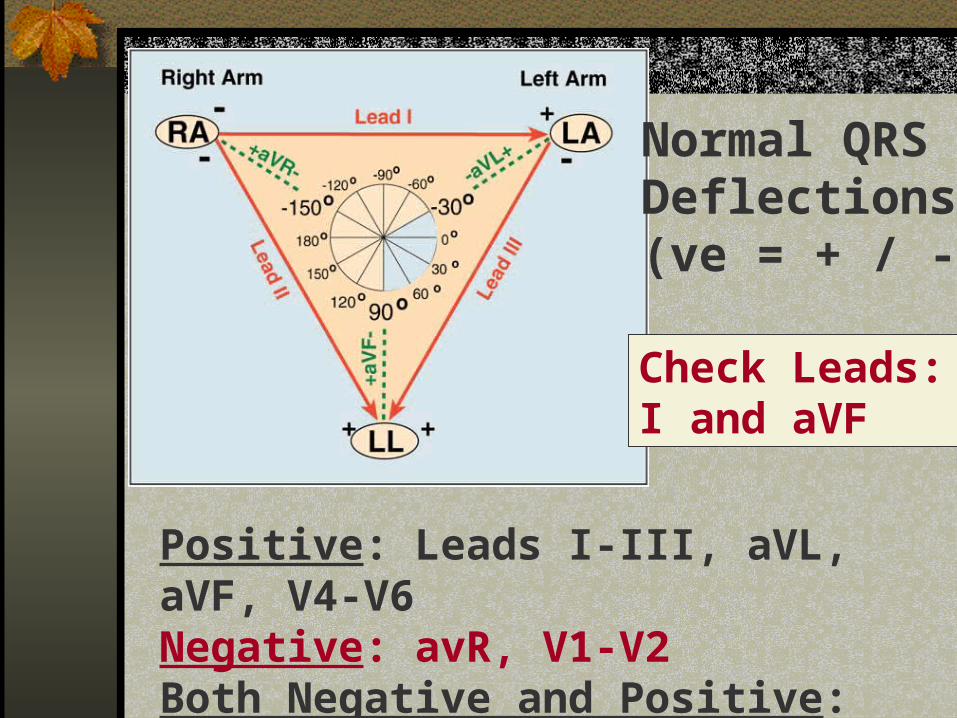
Normal QRS Deflections(ve = + / -)
Positive: Leads I-III, aVL, aVF, V4-V6Negative: avR, V1-V2Both Negative and Positive: V3
Check Leads: I and aVF

The Following Quadrant The Following Quadrant System Quickly Identifies System Quickly Identifies QRS Axis DeviationQRS Axis Deviation

Interpreting Axis Interpreting Axis Deviation:Deviation:Normal Electrical Axis:
(Lead I + / aVF +)Left Axis Deviation:
Lead I + / aVF –Pregnancy, LV hypertrophy etc
Right Axis Deviation:Lead I - / aVF + Emphysema, RV hypertrophy etc.
NW Axis (No Man’s Land)NW Axis (No Man’s Land)Both I and aVF are –Check to see if leads are
transposed (Did you reverse the RA and LL electrodes?)
Indicates:EmphysemaHyperkalemiaVTach

“Seeing” the heart in the Transverse plane: The ChestLeads
V2V1 V3
V4
V5
V6
--
+ +
+
+
ST Segment Analysis: ST Segment Analysis: Ischemia DiagnosisIschemia DiagnosisKey Reference Points:
Isoelectric line: Use the PR segment as reference
J-Point: Point at which QRS complex ends and ST segment begins
Most Common Measurement: .06-.08 sec (>1-2 mm) past J-PointST Slope: Downsloping > Horizontal
> Upsloping (questionable/angina)
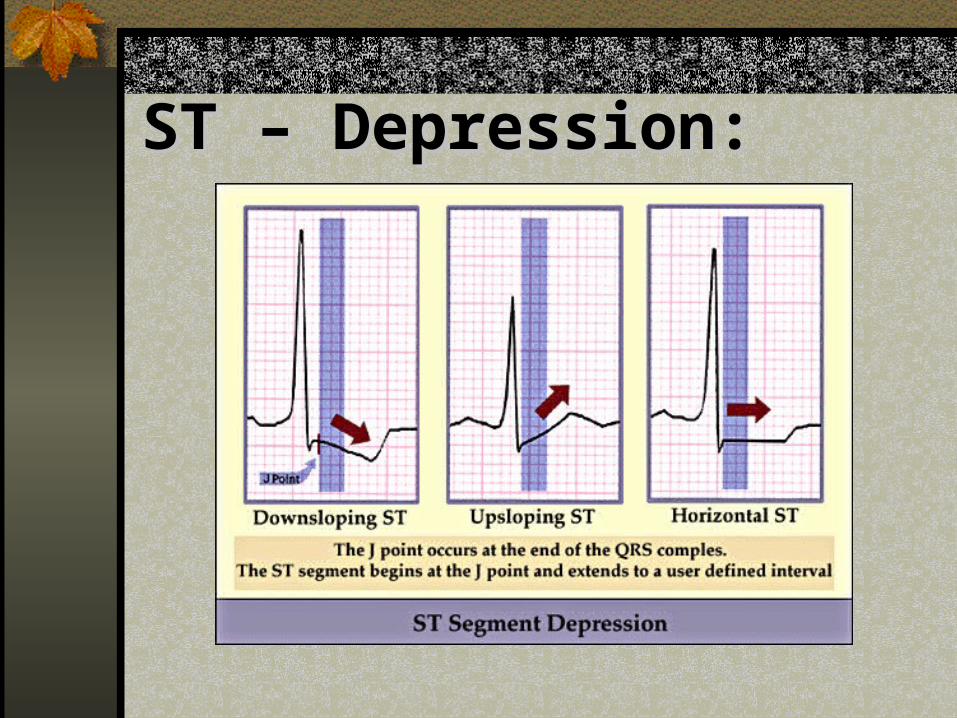
ST – Depression:ST – Depression:

ST-DepressionST-Depression
>1.0 mm depression: Downsloping: Very predictiveHorizontal: Very predictiveUpsloping: Predictive if angina
present>2.0 mm depression
Usually indicative of ischemia
Positive Co-Conditions – Positive Co-Conditions – Signals More Severe CAD:Signals More Severe CAD:Exertional HypotensionAngina that limits exerciseExercise capacity < 6 METsST changes at RPP < 15,000ST changes persist into
recovery

Determining Regions of Determining Regions of CAD: ST-changes in leads…CAD: ST-changes in leads…RCA: Inferior myocardium
II, III, aVFLCA: Lateral myocardium
I, aVL, V5, V6LAD: Anterior/Septal
myocardiumV1-V4

Regions of the Regions of the Myocardium:Myocardium:
InferiorII, III, aVF
LateralI, AVL, V5-V6
Anterior / SeptalV1-V4
Recommended