B–1 BOARD OF REGENTS MEETING
B–1/207-17 7/12/17
UW Medicine Strategic Review – Project design, work plan, areas of emphasis, and analogs INFORMATION This item is for information only. BACKGROUND The Regents have engaged ReCon Strategy (http://reconstrategy.com/) to perform a strategic review of UW Medicine. An initial report out on project design, work plan, areas of emphasis and analogs will be provided. Full materials will be available on the day-of the meeting.

UW Board of RegentsUWM Strategic Review
Preliminary update
July 12 2017
ATTACHMENTB–1.1/207-17 7/12/17

1
Objectives for today’s discussion
Provide a process update and review some specifics of the work‐planning
Share some initial findings from review of analog systems
B–1.1/207-17 7/12/17

2
Key messages for today
Project is on track after “soft” kick‐off last month
Interviews with Regents suggest strong focus on assessing strategic risks and governance • Work plan tweaked to ensure appropriate breadth of analogs
Analog set matches UW Medicine core features (including state system challenges)
Academic medicine recognizes that it must transform to thrive in value‐based world
Analogs provide good illustrations of the scope of change underway• Stitching together broad, integrated systems across geographies and care continuum• Building capabilities to support population health and value‐based care• Investing heavily relative to local competition
Governance structures vary substantially across analogs• Governance must promote and support integration of clinical, teaching, and
research mission and activities• Empowerment plus local factors and culture likely key drivers of what works
B–1.1/207-17 7/12/17

3
Project on track after soft kick‐off last month
Completed Initial interviews with Regents, selective UW Medicine Board members and senior leadership within UW Medicine as part of “soft kick‐off”
Site visits for major elements of UW Medicine
Initial data collection
Selection of benchmarks for deep dives
Underway Detailed review of benchmarks (including interview targets)
Follow‐up data requests
Interviews with next layer of UW Medicine management
Narrowing on key analytical priorities
Development of pressure testing scenarios
B–1.1/207-17 7/12/17

4
Based on our interviews, Board of Regents is focused on strategic risks and governance challenges
Deep respect for UWMedicine accomplishments, capabilities and long‐term momentum
At a high level, strategy seen as consistent with market• Recognition that strategy has risks and requires investment (…and a strong desire
to understand these better)
Market changing fast: reimbursement uncertainty, able competitors, market entrants. Given that context, recent financial performance raising broader questions:
• Does it have required structures, capabilities and resources to execute?• What are the gaps and can these be addressed fast enough to ensure success?• Is the senior team overburdened given significant growth of enterprise?
Significant discomfort with current approach to governance• Several efforts to put improvements in place, but ambiguity of roles remains • Information flows seen as insufficient to support full engagement and oversight
B–1.1/207-17 7/12/17

5
No major changes to work plan requiredAdding additional analogs to ensure broad fact base
Preparation ImplicationsAnalysis
Engagement with UW and UW Medicine leadership throughout
Data collection Consistency andcompleteness
Alignment withenvironmental opportunity
Scenario characterization(high level)
Robustness checks
Key risks and implicationsfor governance
Benchmark selection Performance and strategycomparison with peers Financial implications and
outcome ranges
1 2 3
July Sept
Internal
Compar‐ables
Scenarios
Lenses
Originally planned 3‐4 analogs. Now: 5 full reviews + 1 for governance insights only
B–1.1/207-17 7/12/17

6
SystemHosp‐itals Beds
Affili‐atedphysi‐cians
CoreMSA pop (M)
Share (in
MSA)5
Primarycompetition
(share in MSA) KaiserCIN, ACOactivity
NIH$M1
Med stud.
Prim. care rank
Univ. con‐trol
System leader
report to SoM dean
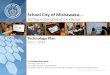
UWMedicine 5 1,380 2,799 3.8 33% Swedish/Prov(26%) Now 2 employers,
Premera 639 1,022 1 Yes Yes
Johns Hopkins Medicine 7 2,415 3,454 2.8 23% UMD (34%) Yes CMS MSSP 565 471 27 No2 Yes
(joint)
UCSF Health 5 1,039 1,372 4.7 51% Sutter (23%) Yes Canopy Payer ACOs 577 633 3 Yes No
UCSD Health 4 671 1,168 3.3 16% Sharp (37%) Yes Humana ACO 330 507 12 Yes Yes
UC Health(Colorado) 83 1,706 2,806 2.9 27% HealthOne
(33%) Yes UCHealth IN Cigna ACO 195 697 8 No No
UNC Healthcare 154 2,918 3,477 2.26 26% Duke (26%) UNC Alliance
BCBSNC ACO 278 834 2 Yes Yes(joint)
Michigan Medicine 3 1,008 2,548 1.26 43% St. Joseph
Mercy (32%)Together HealthCMS MSSP 402 719 5 Yes Yes
(joint)(1) Based on NIH data compiled through the US News methodology except University of Colorado(2) Johns Hopkins University and Johns Hopkins Health System are separate legal entities(3) Primary hospitals. System also has several small hospitals and several under construction.(4) Large share of hospitals outside the core MSA(5) Based on inpatient Medicare Fee For Service charges (non-Medicare Advantage); may not fully include Kaiser in all markets(6) Expanded geographies used for UNC (Raleigh-Durham-Chapel Hill CSA) and Michigan Medicine (combined Ann Arbor, Flint, Lansing MSAs)Sources: NIH, US Census, Medicare inpatient charges dataset FY2014, health system websites, press releases, US News & World Report, AHD, Definitive Health, Recon analysis
Our six analogs match key features of UW MedicineNote: Michigan Medicine to be analyzed on governance topics only
Clinical Research Academics Governance
B–1.1/207-17 7/12/17

7
Each analog also has specific features which make them useful comparisons on strategy
• Strong research branding and medical education legacy• Sophisticated ability to manage risk (e.g. own health plan)• Yet remains “boxed in” to the #2 market share position
• Sustained market leadership vs. strong local competition (Sutter)• Strategic partnership driven growth (esp. John Muir system)• Aspirational model especially given public university position
• Slower pace on value‐based transition and partnership strategy• Facing reinvigorated Kaiser competition (new hospital)• Share position behind 2 strong local competitors (Sharp, Scripps)
• Holding its own against strong in‐market academic competition • Moving quickly on regional/multiregional/rural network and population
health transition
• Competing vs. mix of non‐profit, for profit systems, and Kaiser• Moving quickly on regional/rural network and population health
transition
• Broad regional set of primary clinics + recent hospital acquisition• Recently changed governance structure to consolidate clinical and
educational leadership roles
B–1.1/207-17 7/12/17

8
Academic medicine recognizes need for radical change to thrive in value‐based environment
Note: Adapted from Advancing the Academic Health System for the Future: A Report from the AAMC Advisory Panel on Health Care (2014)
Scope Broad regional scope and services across the continuum of care
System Organization and systems which promote unified direction and accountability
Governance Governance structures which promote strategic alignment with universities on critical challenges and how they should be addressed
Leadership Academic and physician leadership structures will need to grow as the clinical and organizational cultural requirements rapidly evolve to demands of new era
Transparency Transparency of progress towards value‐based care demonstrated in quality outcomes and financial performance
Operations Operating model restructured and focused on delivering value‐based care and operational efficiency
Population health Leadership on population health strategies for attributed lives and communities
Cultural readiness Culture of candor and rigorous self‐assessment to support rapid evolution towards the new model
Key recommendations from “Advancing the Academic Health System for the Future” study
B–1.1/207-17 7/12/17

9
Analogs illustrate several key themes
The importance of health systems encompassing services across the care continuum increases as networks are “hardened”
Academic medicine is building capabilities to position for continued transition from fee‐for‐service to value‐based care/reimbursement; how far along varies greatly
As a whole, academic medicine is investing heavily – often outpacing local competitors
No one‐size‐fits‐all model for governance, however initial findings suggest that empowered dedicated healthcare boards support success
B–1.1/207-17 7/12/17

10
Analog systems tightening control of referral flowResult of network expansions and hardening of competitor networks
Note: System-ness defined as: (total # of in-system encounters for all Medicare Fee For Service admissions within 30 days of admission)/(Total # of encounters for all Medicare Fee For Service admissions within 30 days of admission). Source: Definitive Health (Medicare data from CMS 2013-2015 Physician Referral Patterns datasets); Recon analysis
System 2013
Gains fromfirming
affiliations
Losses from reduced external
referrals 2015
UWMedicine 60% 6% 6% 72%
Johns Hopkins 62% 4% 5% 71%
UCSF 60% 2% 4% 66%
UCSD 68% 4% 2% 74%
UCHealth (CO) 67% 4% 3% 74%
UNC 67% 5% 4% 76%
Average 64% 4% 4% 72%
Degree of “system‐ness” of Medicare Fee For Service patientsadmitted to system flagship academic hospital
B–1.1/207-17 7/12/17

11
UCHealth building geographically diverse, cross‐continuum system
GeographyPhysician
practices / clinicsCommunityhospitals
Tertiary / Quaternary Behavioral
Post‐acute / long‐term
North(Fort Collins)
Central(Denver)
South
Colorado Health Medical Group
Poudre ValleyHospital
Medical Centerof the Rockies Mountain Crest
O/P facilitiesAnchutz campus + 9
other clinics
University of Colorado Hospital
Center for Dependency,
Addiction, Rehab(50 beds residential)
Associates in Family Medicine
Memorial Hospital Central
University of Colorado Medicine / UPI
Affiliated O/P facilitiesHospital campuses +
Medical Plaza
Parkview Medical Center
Parkview Medical Group
Kindred
Vivage QualityHealth Partners
Colorado SpringsPueblo
SoM practice group long affiliated with UCHealth but with ownership participation in the Integrated Network
Creation of behavioral health service line,
integrated into clinics
7/2012 – Joint Operating Agreement with PVHS
2015 – Various strategic initiatives10/2012 – Long term lease of MHS operations
2017 – Launch of UCHealth Integrated Network
Pre‐2012 core UCHealth
Physicians part of Colorado Health Medical Group
B–1.1/207-17 7/12/17

12
UCSF uses affiliations to expand geographic footprint
GeographyPhysician
practices / clinicsCommunityhospitals
Tertiary / Quaternary Behavioral
Post‐acute / long‐term
East(East Bay)
Central(San Francisco)
North (Marin/Sonoma)South(San Mateo)
SF General – long‐standing partnership for primary, secondary,
hospital care (staffed by UCSF faculty/residents)
7 hospitals & 3 medical groups join UCSF/JMH ACO; renamed “Canopy Health”
2013 – Begin affiliation strategy
2015 – Upgrade UCSF assets2014 – Launch of UCSF/John Muir network
2016 – Expansion of UCSF/JMH ACO
Pre‐2013 core UCSF
Future – New development under UCSF, BayHealth
UCSF Medical Center at Mission Bay opens (289‐
beds);Parnassus upgraded for
specialty services
2015 – Intro of “UCSF Health” as integrated healthcare network, incorporating all UCSF hospitals and SoM
Hospice by the Bay affiliation
Children’s Oakland partnership
Washington Hospital affiliation (341‐bed acute, Gamma Knife Center, rad
onc, OP surg)
Expanded affiliation to include medical oncology
UCSF/John Muir Health create JV “Bay Area Health Network”, cornerstone of new ACO
Network expands med spec (transplant)
UCSF Parnassus original campus (hospital, ambulatory care)
UCSF Porter Psychiatric Institute at Parnassus
UCSF Mount Zion becomes outpatient hub once Mission Bay
campus opens Plans to open new Berkeley OP center via JV development company
BayHealth
UCSF plans for new psych building at Mission Bay, will double UCSF OP
capacity
UCSF Benioff Children’s
7 hospitals & 3 medical groups join UCSF/JMH ACO; renamed “Canopy Health”
Richard H Fine People’s Clinic (staffed by UCSF faculty/residents)
Source: UCSF website, press releases, local coverage
B–1.1/207-17 7/12/17

13
Analogs illustrate several key themes
The importance of health systems encompassing services across the care continuum increases as networks are “hardened”
Academic medicine is building capabilities to position for continued transition from fee‐for‐service to value‐based care/reimbursement; how far along varies greatly
As a whole, academic medicine is investing heavily – often outpacing local competitors
No one‐size‐fits‐all model for governance, however initial findings suggest that empowered dedicated healthcare boards support success
B–1.1/207-17 7/12/17

14
UNC investing considerable organizational resources in value‐based care capabilities
Strategic leadership and architecture
Strong cadre for implementation
Selected key initiatives
Creation of the UNC Institute for Healthcare Quality Improvement (2013)• Intellectual leadership with model
development and research
Appointment of a Chief Analytics Officer reporting to the CEO (2016)• Strategy to maximally leverage Epic
across system “Epic@UNC”
VP for Practice Quality & Innovation Management• Focus on supporting transformation of
physician clinical practice• Care management • Population health
VP for Operational Efficiency• Focus on lean hospital operations
Director of Performance Improvement for UNC hospitals• Focus on hospital quality, e.g.
readmissions
Dedicated System VP for post‐acute care
Primary Care Improvement Initiative (2013)
Outpatient Transitions Collaborative (2014)
Reducing Patient Harm (2015)
Enhanced attractiveness of UNC Health Alliance Clinically Integrated Network for non‐affiliated community practicesAbility to deliver on accountable care and engage in value‐based contracting
Sources: UNC public documentsB–1.1/207-17 7/12/17

15
UCSD Health System organizational groupings are more traditional
CHANCELLOR UCSD* Chief Human Resources
Officer Vice Chancellor forHealth Sciences and
Dean, School of MedicineChief Financial Officer, UCSD Health Sciences
Chief Executive Officer andChief Strategy Officer, UCSD Health
CEO Clinical Practice & Dean Clinical Affairs, Health Sciences
Chief Counsel,UCSD Health
Assistant Dean Clin Affairs, Health SciChief Operating Officer, Clinical Practice Org
Chief Compliance and Privacy Officer ** Chair, Dermatology ** Chair, Anesthesiology CAO Surgical, Anesth, Musc,
Neuro, Imaging ServicesChief of Staff UCSD Health System
Associate Dean Clinical Affairs, Health Sciences
** Director, MCC * Chair, Biomedical Informatics
CAO Cardiovascular, Derm & Hospital Medicine Chief Medical Officer Chief Executive Officer
Internat’l Clin Programs
** Chair, Pediatrics ** Chair, Emergency Medicine
CAO Oncology, Radiation Therapy Services
Director, Primary Care Operations
Associate Dean, GME and Designated Official ** Chair, Psychiatry ** Chair, Family Medicine
and Public HealthCAO, Women & Infants, Psychiatry, Ophth Services Director, Managed Care
Chief Quality andPatient Safety Officer
** Chair, Radiation Medicine & App Sciences ** Chair, Medicine
** Chair, Radiology ** Interim Chair, Neurosciences
** Chair, Reproductive Medicine
Acting Chief of Clinical Affairs, Neurosurgery
Director, SCVC Acting Chief of Academic Affairs, Neurosurgery
Director, SCVC ** Chair, Ophthalmology
** Chair, Surgery ** Chair, Orthopaedic Surgery
** Chair, Urology ** Chair, Pathology
Associate Vice Chancellor Health Sci Advancement
Board Of Governors
Chairs Chairs Chief Adm. Officers (CAO) Corporate Functions Medical Group
* Joint Health System and Health Sciences appointment
** Joint Health System and Health Sciences appointment (75% Health Sciences; 25% Health System)
Director, Telemedicine
Associate Medical Dir., Ambulatory Quality
Chief Operating Officer UCSD Medical Group
Chief Experience Officer
Medical Dir Ambulatory Primary Care – Family MedMedical Dir Ambulatory Primary Care – General
Internal Medicine
Executive Director, Student Health&Wellness
Chief Contracting Officer
Chief Operating Officer UCSD Clinical Integration
Network
Chief Clinical Officer
Chief Financial Officer
Chief Information Officer
Source: UCSD Health posted org chart, May 4 2017B–1.1/207-17 7/12/17

16
Analogs are stepwise committing business to value‐based reimbursement
System 2011 or earlier 2012 2013 2014 2015 2016 2017
JohnsHopkins
EHP (55K members); Priority Partners MCO; US FHP; PepsiCo CoE
CMS MSSP ACO (39K lives in ‘15); Walmart/Lowe’s/McKesson CoE
Medicare Advantage plan
UCSF Blue Shield ACO (city /county employees, 19K lives in ’12); Health Net HMO ACO (12K lives in ‘15)
Anthem ACO (employers, 13K lives in ‘15); BPCI (joint)
Canopy/ Health Net ACO (UC employees); Cigna ACO (PPO members, 8K lives); Blue Shield HMO ACO (12K lives in ‘15)
United ACO(self‐funded employers)
UCSD MedicareAdvantage/Humana
AccentCare BPCI (joint)
United ACO (self‐funded employers)
UCHealth CO Access RCCO Medicare Advantage/Anthem
Cigna ACO (CHMG);BPCI (joint)
CMS MSSP ACO
UNC BCBS Carolina Advanced Health pilot
CMS Next Gen ACO (~24K lives); Cigna ACO (health plan members)
Entry into risk‐based contracts:
GovernmentCommercial
Key:
ACO = Accountable Care Organization ; BPCI=‐ Bundled Payment for Care Improvement; EHP = Employer Health Program; MCO = Managed Care Organization (health plan); MSSP = Medicare Shared Savings Program; RCCO = Regional Care Collaborative Organization
B–1.1/207-17 7/12/17

17
Analogs illustrate several key themes
The importance of health systems encompassing services across the care continuum increases as networks are “hardened”
Academic medicine is building capabilities to position for continued transition from fee‐for‐service to value‐based care/reimbursement; how far along varies greatly
As a whole, academic medicine is investing heavily – often outpacing local competitors
No one‐size‐fits‐all model for governance, however initial findings suggest that empowered dedicated healthcare boards support success
B–1.1/207-17 7/12/17

18
Analogs reinvesting heavily into the businessOften outpacing competition
Note HCA, Medstar, Dignity are multi-regional systems with substantial presences and headquarters beyond the markets they share with the analogs; a significant portion of their capital expenditures is allocated centrally and therefore not captured in the regional market. *Note: 2012-2016 for Baltimore, San Francisco, and San Diego; 2011-2015 for Raleigh-Durham and SeattleSource: Definitive Health (Medicare data from CMS 2013-2015 Physician Referral Patterns datasets); Recon analysis
0
2
4
6
8
10
12
14
16
18
20
22
24
26
HCA
Virginia MasonUCSD
Sharp
Wake
JH
Swed/Prov
Sutter
UW
UNC
Dignity
MedStar
County Duke
UCSF
UMDScripps
LifeBridge
CHISLC
UC Health
5‐year average ratio of CapEx to Net Patient Revs, %*
B–1.1/207-17 7/12/17

19
Example: Johns Hopkins budgeted $500M in CapEx in 2015 relative to Net Patient Revenue of $5.6B
Source: Johns Hopkins Medicine: A Look at Our Books Fiscal Year 2015 Capital Budget and Annual Operating Plan
59
40
146
104
65
3734
25
JH SOM
529
Suburban Hospital
OtherHoward County Hospital
Sibley Hospital
2015 Capital Expenditures ($M)
Children’s Hospital
JH Hospital
Bayview Medical Center
JH Health System
19
Key investments and facility locations
Epic imple‐menta‐tion
New tower
Reno‐vation of
I/P facility
Build out of O/P cancer facilities
B–1.1/207-17 7/12/17

20
Analogs illustrate several key themes
The importance of health systems encompassing services across the care continuum increases as networks are “hardened”
Academic medicine is building capabilities to position for continued transition from fee‐for‐service to value‐based care/reimbursement; how far along varies greatly
As a whole, academic medicine is investing heavily – often outpacing local competitors
No one‐size‐fits‐all model for governance, however initial findings suggest that empowered dedicated healthcare boards support success
B–1.1/207-17 7/12/17

21
Wide range of governance systems which are the result of historical adaptations
Johns Hopkins SOM and Health System started out separate but joined in the 90s
University of Colorado SOM and Health system were separated in the early 90s
UNC Health system was granted substantial autonomy by the State in the early 00s
Position of Dean and CEO are combined under “JH Medicine” accountable to president of JHU and board of JH Medicine• Board of JH Medicine is self‐perpetuating
UCHealth has a CEO accountable to its Board and is independent from the University of Colorado• BoR has strong influence on Board of
UCHealth composition
Position of Dean and CEO are combined and reports to UNC leadership but is accountable to UNC Health Board of Directors with broad authority.
At least through an external view, each of these models seem to be working well for the systems they serve – there is no obvious “best model”
B–1.1/207-17 7/12/17

22
Strategic context’s implications for governancePreliminary thoughts
The landscape for each analog is anything but static….most are taking strategically active postures in response
• Fleshing out the care pyramid through alliances, acquisitions, build‐outs• Restructuring operations towards efficient care delivery and value• Commitment of substantial financial resources
An active posture requires accelerated decision making on complex investment and risk issues and opportunities, placing a significant burden on governance
• Effective governance will require active engagement at a high level of complexity
Possible outcomes ‐‐• Governance keeps pace with strategy and addresses strategic requirements• Strategy gated by governance, leading to missed opportunities and falling behind• Strategy moves faster than governance, creating stress and insufficiently pressure‐
tested decision‐making
B–1.1/207-17 7/12/17
Recommended