The Use of Tapered Self-Expanding Stents and EmbolicProtection Devices in The Treatment of Stenotic Ectatic
Coronary Arteries: A Report of Two Cases
Vu Le,1 MD, Mazen Abu-Fadel,2* MD, and Thomas A. Hennebry,2 MB, BCh, BAO, FSCAI
Objective: The Usage of tapered self-expanding stents and embolic protection devicesin the treatment of stenotic ectatic coronary arteries. Background: Coronary arteryectasia (CAE) is an uncommon disease that is occasionally found during cardiac cathe-terization. A high incidence of artherosclerotic disease is associated with CAE. Cur-rently, there is no evidence-based approach for the management of stenotic ectaticcoronary arteries (SEC). Methods: Percutaneous intervention with carotid stenting sys-tem and embolic protection system to recanalize SEC. Results: We describe twopatients who presented with acute coronary syndrome and were found to have CAEwith significant stenosis. Both patients underwent percutaneous intervention with RXACCULINKTM Carotid stenting system and ACCUNETTM embolic protection system(Abbott Laboratories, Abbott Park, IL), successfully. This carotid stenting system isapproved by FDA for stenting of extracranial carotid artery stenosis. Conclusion: Tothe best of our knowledge, this is the first case report illustrating the usage of thesedevices as an alternative for the treatment of SEC. ' 2008 Wiley-Liss, Inc.
Key words: acute coronary syndrome; aneurysm; coronary; percutaneous coronaryintervention
INTRODUCTION
Coronary artery ectasia (CAE) is an uncommon dis-ease that is occasionally found during cardiac catheter-ization. A high incidence of artherosclerotic disease isassociated with CAE. Currently, there is no evidence-based approach to the management of stenotic ectaticcoronary arteries (SEC). Because of coronary arteryenlargement, regular stents are too small to be used invarious types of ectatic coronaries, and biliary stentshave been implanted to treat SEC.
Case 1
A 63-year-old Caucasian male with past medical his-tory of hypertension, chronic obstructive lung disease,abdominal aortic aneurysm, dyslipidemia, congestiveheart failure, and obesity presented with Non-Q-wavemyocardial infarction (NSTEMI). Electrocardiogram(ECG) showed non specific T waves changes in thelateral leads, and cardiac markers were elevated withtroponin 2.07 n/mL. Angiographic study of the coro-nary arteries illustrated three diseased vessels includingextensive ectasia of the left anterior descending coro-nary artery (LAD) with 80% stenosis (Fig. 1), 100%stenosis of the mid left circumflex artery, 100% steno-sis in the first obtuse marginal artery, and 100% steno-
sis of right coronary artery. Cardiothoracic surgery wasconsulted for three vessels bypasses. However, thepatient denied further invasive treatment including per-cutaneous coronary intervention (PCI) of his LAD, andhe was discharged on maximal medical treatment.He returned to the hospital 4 months later with
increased shortness of breath and chest pain. Cardiacenzymes and ECG were within normal limits. At this
Conflict of interest: Nothing to report.
1Department of Internal Medicine, University of OklahomaHealth Science Center, Oklahoma City, Oklahoma2Section of Cardiovascular Medicine, Department of InternalMedicine, University of Oklahoma Health Science Center,Oklahoma City, Oklahoma
*Correspondence to: Mazen Abu-Fadel, MD, Assistant Professor of
Medicine, Section of Cardiovascular Medicine Department of Medi-
cine, University of Oklahoma Health Science Center, 920 Stanton L.
Young Blvd., WP3010 Oklahoma City, OK.
E-mail: [email protected]
Received 11 July 2008; Revision accepted 16 July 2008
DOI 10.1002/ccd.21740
Published online 16 September 2008 in Wiley InterScience (www.
interscience.wiley.com).
' 2008 Wiley-Liss, Inc.
Catheterization and Cardiovascular Interventions 72:643–646 (2008)

point, the patient decided to go with PCI and stentingof the LAD.PCI of his LAD lesion was done using an 8F XB 3.5
Guide. An Asahi grand slam wire was used to cross theLAD lesion. Balloon angioplasty was performed using a4.0 mm 3 30 mm RX balloon with satisfactory results.A 6–8 mm 3 40 mm Acculink carotid stent wasdeployed over the stenotic LAD lesion. Post dilatationwas done with a 6.0 mm 3 20 mm peripheral balloonwith excellent angiographic results (Fig. 2).The patient tolerated the procedure very well with-
out any complications. He was discharged to homewith clopidogrel 75 mg daily for 3 months. At the 2-year follow up, the patient was doing well without anycardiac symptoms. Unfortunately, he was recentlydiagnosed with stage 4 non small cell lung cancer andis on chemotherapy.
Case 2
This is a 61 year old non smoker male with historyof migraine, gastroesophageal reflux disease, andrecent bronchitis presented with NSTEMI. ECGshowed normal sinus rhythm with premature ventricu-lar contractions, and cardiac enzymes peaked with tro-ponin level 1.96 ng/mL and CK-MB at 16.7 ng/mL.Diagnostic left heart catheterization illustrated ecta-
sia of left main coronary artery, left anterior descend-ing artery, and left circumflex artery. In addition, theright coronary artery (RCA) was extensively ectatic
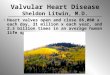
with 85% stenosis and a large filling defect consistentwith a thrombus (Fig. 3).An 8F JR4 guiding catheter was used to canulate
the right coronary artery. A 6.5-mm Accunet filterwire was used to cross the lesion and was deployed inthe distal RCA. PCI was done using a 7–10 mm 3 40 mm
Fig. 1. Etactic LAD with significant stenosis.Fig. 2. LAD after Self-Tapered RX ACCULINKTM.
Fig. 3. Ectatic RCA with significant stenosis and thrombus.
644 Le et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

Acculink carotid stent (Fig. 4). The Accunet distal em-bolic protection wire was collapsed and removed afterthe stent was deployed and final angiogram showedminimal residual stenosis, with no post PCI complica-tions. He was discharged to home on clopidogrel75 mg daily for 2 months, and aspirin 325 mg indefi-nitely. He has been doing well without any chest pain2 years after the procedure.
DISCUSSION
CAE is an uncommon finding and is diagnosed inup to 4.9% of patients undergoing coronary angiogra-phy [1–5]. Various definitions of CAE have been usedincluding enlargement of the coronary artery 1.5 timesor more than the adjacent normal coronary artery [2],or 1.5 times larger than the mean diameters of the nor-mal proximal and distal parts of the ectatic segment[6]. Ectasia involves the right coronary artery morefrequent than the left [3–5,7]. The prevalence of ectaticcoronaries is reported to be about 2% of the generalpopulation, and atherosclerotic lesions are associatedwith up to 95% of CAE cases [1–3,5,8–10]. Markiset al. [10] first classified four types of CAE in 1976.Type I involves diffuse disease in more than two coro-nary arteries. Type II includes diffuse disease in onevessel and localized dilation in another. Type III hasdiffuse disease in one vessel, and Type IV encom-passes localized or segmented ectasia.Currently, there are very limited data on the use of
a specific stenting system for SEC. Because of the
abnormally enlarged artery, different kinds of stentsincluding biliary and venous graft stent systems havebeen utilized to revascularize SEC. In 2000, Agirbasliet al. [11] were first to report the successful use of bil-iary stents to canalize SEC of three patients. In addi-tion, a covered stent designed for autologous venousgraft stenosis, Zeus VG Stent, has been used [12]. In2007, Rha et al. [13] reported using sirulimus-elutingstents to canalize a SEC in a parallel fashion in whichtwo stents were deployed simultaneously next to eachothers in the same stenotic ecstatic segment. Overall,there are many reports of stenosis associating withCAE, but evidence for the use of a specific stents islacking [5].To the best of our knowledge, we report the first
use of a tapered self-expanding stenting system,ACCULINKTM, in the revascularization of two ectaticcoronaries in two patients without any complications.The diameters of the ectatic coronary segments, inwhich the proximal ends were larger than the distal,were not uniform in both the cases. Therefore, thetapered stent was suited for its purpose as it reducedthe risk of over-expanding the smaller segment of thecoronary arteries. In addition, the application of theembolic protection device, ACCUNETTM, allowed usto protect the distal vessel and collect embolic debrisduring the revasculization process of the SEC withthrombus. In conclusion, self expanding stents couldbe considered as alternatives to the current manage-ment of SEC. However, more studies are needed toevaluate the effectiveness and safety in these devices,in the ecstatic coronary circulation.
REFERENCES
1. Manginas A, Cokkinos DV. Coronary artery ectasias: Imaging,
functional assessment and clinical implications. Eur Heart J
2006;27:1026–1031.
2. Hartnell GG, Parnell BM, Pridie RB. Coronary artery ectasia. Its
prevalence and clinical significance in 4993 patients. Br Heart J
1985;54:392–395.
3. Gunes Y, Boztosun B, Yildiz A, Esen AM, Saglam M, Bulut M,
Karapinar H, Kirma C. Clinical profile and outcome of coronary
artery ectasia. Heart 2006;92:1159–1160.
4. Lam CSP, Ho KT. Coronary artery ectasia: A ten-year experi-
ence in a tertiary hospital in Singapore. Ann Acad Med Singa-
pore 2004;33:419–422.
5. Swaye PS, Fisher LD, Litwin P, Vignola PA, Judkins MP,
Kemp HG, Mudd JG, Gosselin AJ. Aneurysmal coronary artery
disease. Circulation 1983;67:134–138.
6. Suzuki H, Takeyama Y, Hamazaki Y, Namiki A, Koba S, Mat-
subara H, Hiroshige J, Murakami M, Katagiri T. Coronary spam
in patients with coronary ectasia. Cathet Cardiovasc Diagn
1994;32:1–7.
7. Giannoglou GD, Antoniadis AP, Chatzizisis YS, Damvopoulou
E, Parcharidis GE, Louridas GE. Prevalence of ectasia in human
coronary arteries in patients in northern Greece referred for cor-
onary angiography. Am J Cardiol 2006;98:314–318.
Fig. 4. Ectatic RCA after RX ACCULINKTM stent placement.
Self-Expanding Stents in Stenotic Ectatic Coronaries 645
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

8. Sorrell VL, Davis MJ, Bove AA. Current knowledge and signifi-
cance of coronary artery ectasia: A chronologic review of the
literature, recommendations for treatment. Possible etiologies,
and future considerations. Clin Cardiol 1998;21:157–160.
9. Swanton RH, Thomas ML, Colart DJ, Jenkins BS, Webb-Peploe
MM, Williams BT. Coronary artery ectasia-a variant of occlu-
sive coronary arteriosclerosis. Br Heart J 1978;40:393–400.
10. Markis JE, Joffe CD, Cohn PF, Feen DJ, Hermann MV, Gorlin
R. Clinical significance of coronary arterial ectasia. Am J Car-
diol 1976;37:217–222.
11. Agirbasli M, Morriss D, Marshall JJ. The use of intrastent pe-
ripheral stent in large coronary arteries: Report of three cases.
Cathet Cardiovasc Interv 2000;50:498–501.
12. Stefanadis C, Toutouzas K, Tsiamis E, Toutouzas P. New stent
design for autologous venous graft-covered stent preparation:
First human application for sealing of a coronary aneurysm.
Cathet Cardiovsc Interv 2002;55:222–227.
13. Rha SW, Wani SP, Oh DJ. Parallel stenting using two siroli-
mus-eluting stents in an ecstatic coronary artery stenosis. Heart
2007;93:976.
646 Le et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).
Recommended