Embed Size (px)
Citation preview

Valvular Heart DiseaseSheldon Litwin, M.D.
• Heart valves open and close 86,000 x each day, 31 million x each year, and 2.3 billion times in an average human life span

Clinical Approach to Valvular Disease
• Make the diagnosis
• Slow the disease progression
• Prevent complications
• Intervene at just the right time– Not too soon– Not too late

Organization of Talk
• Definition
• Etiology
• Pathophysiology
• Diagnosis
• Treatment

Valvular Stenosis
• Normal heart valves are thin and very pliable• They open widely and allow blood to flow across
them with very low resistance (normally only 1-2 mmHg pressure gradient required)
• Stenotic valves do not open normally and higher pressure is required to open them
• Over time, the “upstream” pressure overloaded chambers enlarge
• The process is generally progressive and severe stenosis may eventually cause congestive heart failure
Aortic Valve and Root Anatomy
• 3 cusps (right, left, noncoronary)• Coronary arteries important with pathologies
or surgeries involving aortic root
QuickTime™ and aMicrosoft Video 1 decompressorare needed to see this picture.

Etiology: Inherited Causes of “Aortic” Stenosis
• Bicuspid Valve– Usually asymptomatic until > 30 yrs– Associated aortic coarctation (40%)
• Unicuspid Valve– Generally repaired in early childhood
• Subvalvular (membrane or ridge)• Supravalvular (William’s syndrome)

Acquired Aortic Valve Stenosis: Etiology
• Degenerative (“senile”)– calcification of leaflets and commisures– Chronic inflammatory process?
• Bicuspid (congenital)– becomes stenotic later in life
• Rheumatic– Fibrosis and calcification of commisures
• Degeneration of prosthetic valves (especially bioprosthetic)

Aortic Stenosis
Inherited Causes of “AS”
QuickTime™ and aAnimation decompressorare needed to see this picture.QuickTime™ and aMicrosoft Video 1 decompressorare needed to see this picture.
Bicuspic Aortic Valve Subaortic Membrane

Age at time of presentation helps define etiology of stenosis
• Rheumatic: 30 - 40 years
• Bicuspid: 40-50 years– AI often occurs at a younger age (20’s)
• Degenerative: > 70 years

Aortic stenosis: pathophysiology
• Obstruction to flow across the valve is ultimately the cause of symptoms and complications
• Significant gradient usually doesn’t occur until valve area has ’d from ~ 3.0 cm2 to < 2.0 cm2
• Symptoms “usually” not seen until the valve area is < 1.0 cm2
• “Critical” AS = valve area < 0.7 cm2
• Progression ~ 0.1 cm2/year

Aortic Stenosis:Pressure Tracings
-pressure in LV is higher than pressure in aorta

LV Hypertrophy in Aortic Stenosis
• LV mass increases to maintain output through smaller valve orifice
• Usually, concentric hypertrophy– Small or normal sized cavity– Keeps wall stress normal• (pressure x radius) / wall thickness
• Contrast with eccentric hypertrophy that occurs with AI– Dilated cavity, normal thickness of wall

Concentric LVH in AS

“Compensation” in AS
• LVH initially beneficial compensation
• Interstitial fibrosis ’d myocardial stiffness ’d LV filling pressures
• Eventually wall stress ’d• Inadequate capillary growth to maintain
blood flow to thick-walled, high-pressure ventricle
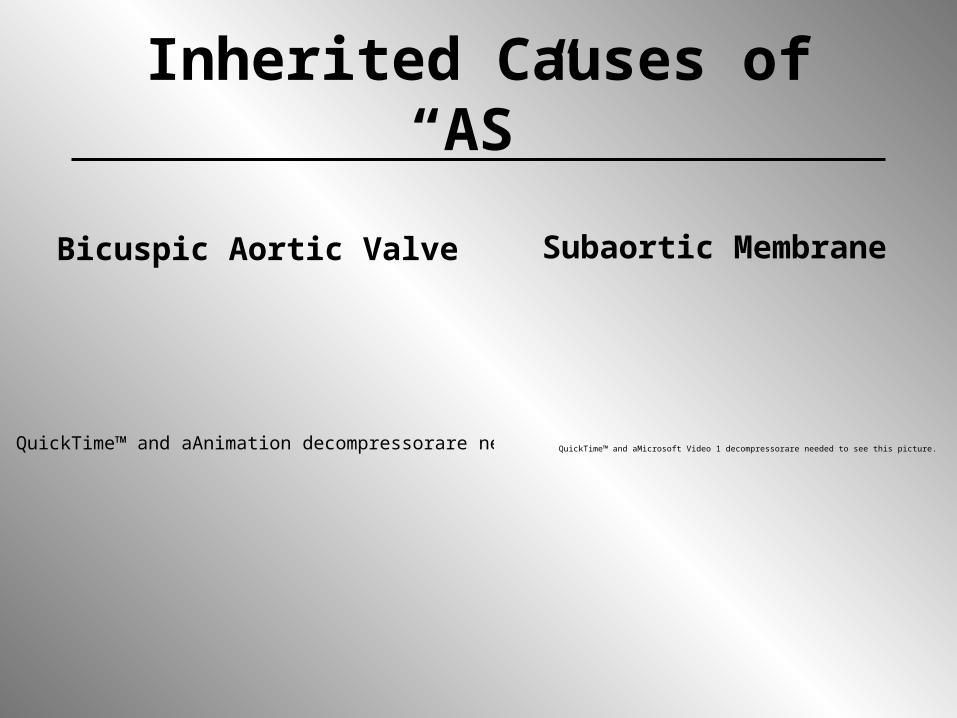
Aortic Stenosis: Symptoms
• Angina (5 yr survival)
• Syncope (3 yr survival)
• Congestive Heart Failure (1-2 yr surv)
Age

Angina in AS
• 2/3 patients with AS• Only half have significant CAD– High wall stress– Low coronary perfusion pressure– Systolic compression of coronary vessels– Hypertrophied myocytes– Inadequate capillary growth
• Need to determine the cause of the angina - will affect surgical decisions

Syncope in AS
• Usually exertional
• Peripheral vasodilatation
• Cardiac output does not increase across fixed stenosis
• Decreased cerebral perfusion
– Tachy or bradyarrhythmias

“End stage” Aortic Stenosis
QuickTime™ and aAnimation decompressor
are needed to see this picture.
LV Systolic Dysfunction
Should have operated sooner

Cardiac Output in Aortic Stenosis
• Pressure gradient proportional to square of flow across valve and inversely proportional to square of valve area
• During exercise, or other high flow states, cardiac output ’s and so gradient will increase
• Conversely, low output will make the Conversely, low output will make the gradient less, even though valve gradient less, even though valve area is unchangedarea is unchanged

Flow vs. Gradient
Diagnosis
• High pitched systolic murmur at upper sternal border with radiation to carotids; single S2; small and slow carotid upstroke
• CXR: possible cardiomegaly• ECG: LVH
• Echo: calcification of leaflets, reduced valve opening, pressure gradient measured by CW Doppler, valve area
• Cath: increased gradient between LV and aorta in systole, valve area

Severity of Aortic Stenosis
-Mean gradient across valve mild < 20 mmHg mild-mod 20 - 30 mmHg mod- sev 30 - 40 mmHg sev > 40 mmHg
-Valve area Insignificant > 1.5 cm2
Mild 1.2 - 1.5 cm2
Moderate 1.0 - 1.2 cm2
Severe 0.7 - 1.0 cm2
Critical < 0.7 cm2
Doppler measurement ofAortic gradient

Echo vs. Cath for Measuring Aortic Valve Area

Medical Treatment of Aortic Stenosis
• Vasodilators (NTG, ACEI, etc.) are potentially dangerous, although beneficial if given in ICU with careful monitoring
• Diuretics, digoxin if CHF present (surgical indication)
• Re-establish/maintain sinus rhythm• SBE prophylaxis• Rheumatic Fever prophylaxis• Treating symptoms, not underlying
disease

Treatment of AS
• Balloon valvuloplasty– Does not work well (poor initial
success)– High complication rate– Rapid restenosis– Almost completely abandoned in
clinical practice

Timing of Valve Surgery
• Balance of immediate operative risks (1-5% surgical mortality + morbidity) vs. hope for long term improvement in symptoms or survival
• Improvement is not guaranteed - especially if the symptoms aren’t due to the valvular pathology
• Especially difficult decision in elderly patients

Surgical treatment of AS
• Valve replacement– Bioprosthetic• Porcine (with or without struts)
– Human homograft – “Ross procedure” (pulmonary autograft
and pulmonic bioprosthesis)
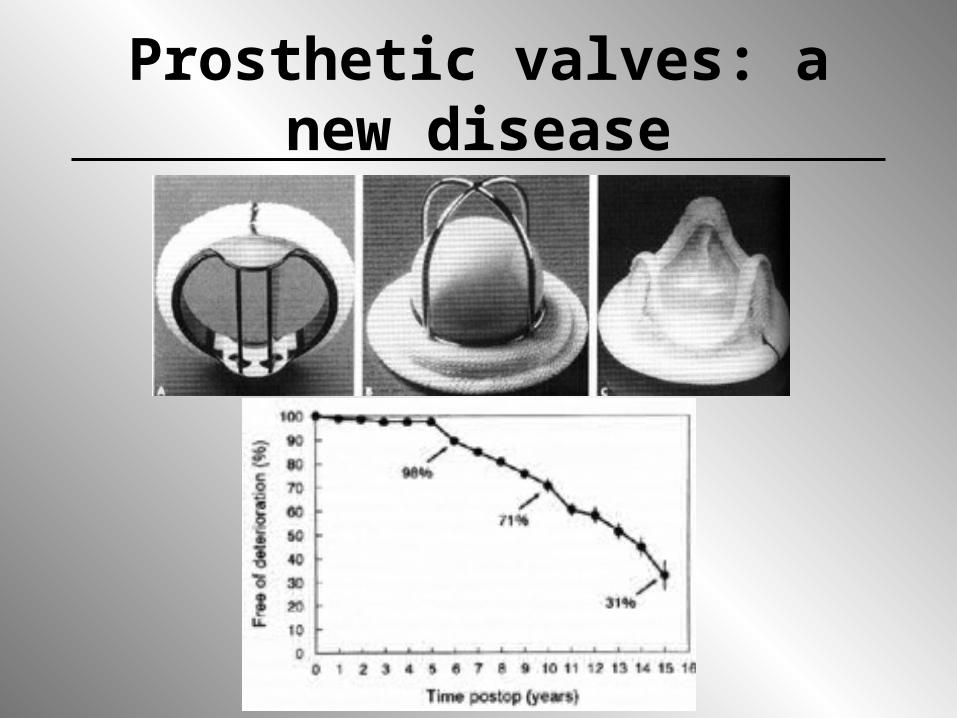
Prosthetic valves: a new disease

Timing of surgery in AS
• Symptomatic operate• Asymptomatic– Careful history (denial of sx)– Stress to elicit symptoms?– Serial echo to look for LV fx– Adverse clinical events (i.e. sudden cardiac
death) – Cardiac surgery planned for other reason
(e.g. CAD)– Frequent follow up (3-12 months)

Reasons to put off surgery
ThrombusPannusInfection
QuickTime™ and aMicrosoft Video 1 decompressorare needed to see this picture.QuickTime™ and aMicrosoft Video 1 decompressorare needed to see this picture.

Complications of Valve Replacement
Fungal infection of aortic root

Mitral Valve Anatomy
• Anterior leaflet longer• Posterior leaflet shorter but occupies more
of the annulus
QuickTime™ and aVideo decompressorare needed to see this picture.QuickTime™ and aVideo decompressorare needed to see this picture.

Mitral Stenosis
• Rheumatic– Fibrosis and calcification of leaflet tips,
commisures, and subvalvular apparatus
• Severe annular calcification (MAC)– Obstruction due to myxoma or
thrombus– Cor triatriatum– Degeneration of prosthetic valves

Rheumatic Mitral Stenosis
Mild MS Moderate MS
“hockey stick” deformity
LA
LVQuickTime™ and a
Video decompressorare needed to see this picture.

Rare Causes of Mitral Stenosis
QuickTime™ and aMicrosoft Video 1 decompressorare needed to see this picture.
Mitral stenosis: pathophysiology
• Gradient across valve is the most important cause of symptoms and complications
• Gradient of as little as 10 mm Hg may be enough to cause pulmonary edema (contrast with aortic valve where gradient > 40 mmHg = severe stenosis)
• Significant gradient usually doesn’t occur until valve area has ’d from ~ 4.5 cm2 to < 2.5 cm2
• Symptoms usually not seen until valve area < 1.5 cm2

Pressure Tracings in Mitral Stenosis
Normal Stenosis
LV
LA

Heart Rate in Mitral Stenosis
• Pressure gradient proportional to square of flow across valve and inversely proportional to square of valve area
• All of the forward flow occurs in diastole• Since diastole is selectively shortened
during tachycardia, flow per unit time must increase just to maintain output
• During exercise,cardiac output also ’s• Exercise intolerance may be severe

Exercise Intolerance in MS
Mitral Doppler
Pulmonary pressuresestimated from TRvelocity
16 mmHg 30 mmHg

The “second stenosis”
• Slow development of high LA pressure transmitted back to the pulmonary vessels may gradually lead to thickening of pulmonary vascular walls
• Severe pulmonary hypertension may develop (in “series” with stenotic mitral valve)
• Hemoptysis, right heart failure• Imparts poor prognosis

LA enlargement in MS
• Most severe with combined MS/MR
• Does not lower the pressure gradient
• High incidence of AF with very high thromboembolic risk (~15%/year)
QuickTime™ and aVideo decompressor
are needed to see this picture.
QuickTime™ and aVideo decompressor
are needed to see this picture.
Complications of Mitral Stenosis
RV OverloadLA thrombus
Atrial Fibrillation

Severity of Mitral Stenosis
-High gradient across valve mild < 4 mmHg mild-mod 4 - 8 mmHg mod 9 - 12 mmHg mod- sev 12 - 15 mmHg sev > 15 mmHg
-Prolonged pressure half time valve area = 220/PHT
Significant < 1.5 cm2
Severe < 1.0 cm2
Treatment of Mitral Stenosis (Medical)
• Prevention of tachycardia (beta blockers)
• Diuretics
• Anticoagulation for afib (? Prophylactic)
• Endocarditis prophylaxis
• Rheumatic Fever prophylaxis

Treatment of MS (mechanical)
• Commisurotomy - cuting or tearing the commisures (surgical, balloon)– Fibrotic valve is favorable, calcific valve is
unfavorable– Significant MR is contraindication
• Valve replacement (repair usually not an option)
Mitral Stenosis in Pregnancy
• May be first presentation of mitral stenosis
• Tolerated poorly because of increased blood volume, increased cardiac output, and increased heart rate
• Beta blockers
• Balloon valvuloplasty to get them through pregnancy if needed

Valve Stenosis Summary
• Pathophysiology related to severity of pressure gradient across valve
• Slowly progressive
• Gradient (and symptoms) related to flow
• “Upstream” compensation
• Operate when symptoms occur and BEFORE irreversible dysfunction develops

A 75 year old patient with known aortic stenosis has an episode of syncope. Upon further questioning, he admits to experiencing chest pressure during exertion for the past 3 months. You should perform an exercise stress test to look for coronary artery disease prior to scheduling surgery for aortic valve replacement.
True or False? Why?
• False. Exercise testing is relatively contraindicated in severe aortic stenosis because of the risk of sudden death - particularly in a patient with recent syncope. Chest pain may be due to AS alone and not CAD. Coronary angiography is a better test in this patient.

If someone with critical AS has angina, is nitroglycerine helpful?
• NTG is relatively contraindicated because it may excessively decrease preload and thus decrease cardiac output resulting in cardiovascular collapse.
• NTG may also decrease coronary perfusion pressure and thus render the ventricle ischemic. This can initiate a rapid cycle of deteriorating cardiac function.
A 25 year old woman from Thailand develops severe shortness of breath and tachycardia at 8 months of pregnancy. She denies prior cardiac symptoms. ECG shows sinus tachycardia, left atrial enlargement and right axis deviation. On cardiac auscultation (performed in the emergency department), no murmurs are reported. What diagnosis should you suspect?
• Mitral stenosis. Symptoms that are mild normally, are classically brought out during pregnancy because of the tachycardia and increased cardiac output. The murmur is typically hard to hear (particularly in noisy places). The finding of LA enlargement on the ECG in the absence of LV enlargement is suggestive of MS.

What factors are likely to limit the efficacy of mitral valve replacement in a pt with
mitral stenosis?
• Pulmonary hypertension and RV dysfunction
• Atrial fibrillation













![[38]Varghese-Frankel-Fischer. 2007 Modeling Transition to Turbulence in Eccentric Stenotic Flows](https://img.pdfslide.us/doc/110x75/577cc54f1a28aba7119bfcd1/38varghese-frankel-fischer-2007-modeling-transition-to-turbulence-in-eccentric.jpg)