Pediatric Pulmonology
The Respiratory Management of Patients With DuchenneMuscular Dystrophy: A DMD Care Considerations
Working Group Specialty Article
David J. Birnkrant, MD,1* Katharine M.D. Bushby,2 Raouf S. Amin, MD,3 John R. Bach, MD,4
Joshua O. Benditt, MD,5 Michelle Eagle, PhD,2 Jonathan D. Finder, MD,6 Maninder S. Kalra, MD,3
John T. Kissel, MD,7 Anastassios C. Koumbourlis, MD,8 and Richard M. Kravitz, MD9
Summary. In 2001, the Muscular Dystrophy Community Assistance, Research and Education
Amendments (MD-CARE Act) was enacted, which directed federal agencies to coordinate the
development of treatments and cures for muscular dystrophy. As part of the mandate, the Centers
for Disease Control and Prevention (CDC) initiated surveillance and educational activities, which
included supporting development of care considerations for Duchennemuscular dystrophy (DMD)
utilizing the RAND/UCLA Appropriateness Method (RAM). This document represents the
consensus recommendations of the project’s 10-member Respiratory Panel and includes advice
on necessary equipment, procedures and diagnostics; and a structured approach to the
assessment and management of the respiratory complications of DMD via assessment of
symptoms of hypoventilation and identification of specific thresholds of forced vital capacity, peak
cough flow and maximum expiratory pressure. The document includes a set of Figures adaptable
as ‘‘pocket guides’’ to aid clinicians. This article is an expansion of the respiratory component of
the multi-specialty article originally appearing in Lancet Neurology, comprising respiratory
recommendations from the CDC Care Considerations project. Pediatr Pulmonol.
� 2010 Wiley-Liss, Inc.
Key words: consensus statement; cough; muscular dystrophy; noninvasive ventilation;
prolonged survival; pulmonary function.
INTRODUCTION
In 2001, the Muscular Dystrophy Community Assis-tance, Research and Education Amendments (MD-CAREAct) was enacted, which directed federal agencies tocoordinate the development of treatments and cures formuscular dystrophy. As part of the mandate, the Centers
for Disease Control and Prevention (CDC) initiatedsurveillance and educational activities, which includedsupporting development of care considerations forDuchenne muscular dystrophy (DMD).Consensus statements regarding the respiratory man-
agement of patients with DMD have been previouslypublished.1 However, this is the first consensus statement
1Department of Pediatrics, MetroHealth Medical Center, Cleveland, Ohio.
2Institute of Human Genetics, Newcastle University, Newcastle upon Tyne,
UK.
3Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio.
4University of Medicine and Dentistry of New Jersey, Newark, New Jersey.
5University of Washington School of Medicine, Seattle, Washington.
6Children’s Hospital of Pittsburgh, Pittsburgh, Pennsylvania.
7Ohio State University and Nationwide Children’s Hospital, Columbus,
Ohio.
8Children’s National Medical Center, Washington, District of Columbia.
9Duke University, Durham, North Carolina.
This manuscript is derived from two multi-specialty articles appearing in
Lancet Neurology and includes text and/or Figures taken verbatim from
and/or adapted from those articles and used with permission. (Bushby K.,
Finkel R., Birnkrant D.J. et al. Diagnosis and management of Duchenne
muscular dystrophy. Part 1: diagnosis, and pharmacological and psycho-
social management.2 Part 2: implementation of multi-disciplinary care.3)
Grant sponsor: National Center on Birth Defects and Developmental
Disabilities/Centers for Disease Control and Prevention.
*Correspondence to: David J. Birnkrant, MD, Department of Pediatrics,
MetroHealth Medical Center, 2500 MetroHealth Drive, Cleveland, OH
44109. E-mail: [email protected]
Received 21 December 2009; Revised 25 February 2010; Accepted 26
February 2010.
DOI 10.1002/ppul.21254
Published online in Wiley InterScience
(www.interscience.wiley.com).
� 2010 Wiley-Liss, Inc.

based on the Rand/UCLA Appropriateness Method(RAM). The participants and sponsors of this projectrecognized that there is a lack of randomized, controlledstudies in this field, precluding development of evidence-based guidelines. The RAM methodology was designedfor just such circumstances and aims to objectify theconsensus process, through repeated anonymous query ofan expert panel regarding the appropriateness andnecessity of clinically relevant scenarios extracted fromextensive review of the medical literature. The scenariosand the results from the RAM questionnaires were refinedthrough telephone and in-person meetings of the panelmembers, optimizing the clinical relevancy of theconsensus recommendations. This document was adaptedfrom a two-part multi-specialty article originally pub-lished in Lancet Neurology.2,3 This respiratory specialtyarticle includes expanded sections on respiratory recom-mendations and areas of controversy. The Figures inthis document were specifically designed to aid cliniciansand they can be used as ‘‘pocket guides’’ to the assessmentand management of the respiratory complications ofDMD.
METHODOLOGY
The CDC selected 84 national and international expertsand organized them into multi-disciplinary panels repre-senting the range of specialties involved inDMDcare. Thepanels developed a comprehensive plan of patient careusing the RAM. During this process, 1981 peer-reviewarticles on assessments and interventions used in thetreatment of DMDwere analyzed, of which 489were usedto create 389 matrices representing 70,302 hypotheticalclinical scenarios.The respiratory panel consisted of 10 members from a
wide geographic distribution, representing the disciplinesof adult and pediatric pulmonology and critical caremedicine, neurology, sleep medicine, rehabilitation med-icine, and respiratory/physical therapy.In the initial round, 36 respiratorymatrices representing
606 hypothetical clinical scenarios were rated anony-mously for appropriateness on an ordinal scale of 1–9.Median ratings for each clinical scenario were tabulatedand analyzed according to RAM guidelines. During aseries of in-person and telephone conferences, the paneldiscussed the results and edited thematrices for the secondround of rating, which included 33 matrices comprising269 clinical scenarios. Assessments and interventionsdeemed appropriate without disagreement (27 matricesrepresenting 115 clinical scenarios) were further rated fornecessity on a similar 1–9 scale. After three rounds ofindependent ratings, the expert panelists reviewed andinterpreted the ratings to develop a clinically relevantconsensus document. There were no disagreementsamong the panelists regarding the final recommendations.
The interventions deemed necessary and/or appropriatewithout disagreement by the panel describe an infra-structure for provision of optimal respiratory care topersons with DMD, described in this document. Thisdocument includes the expert panel’s recommendationson necessary equipment, procedures, tests, and diagnosticevaluations. It also provides a structured approach to theassessment and management of the respiratory complica-tions of DMD, emphasizing the assessment of hypoventi-lation and the identification of specific thresholds of forcedvital capacity (FVC), peak cough flow, and maximumexpiratory pressure.
RESULTS AND PANEL RECOMMENDATIONS
Necessary Equipment, Procedures,and Diagnostics
Clinics caring for persons with DMD should have thecapacity to perform and interpret the tests listed in Table 1.In order to perform these tests, the following equipmentshould be available in the inpatient and outpatient medicalsettings:
. Pulse oximeter.
. Capnograph.
. Spirometer.
. Manometer for measurement of maximum inspiratory
and expiratory pressure levels.
. Peak flow meter for measurement of peak cough flow.
. Lip seal adapters for patients with weak buccal
musculature, for use with spirometers, manometers,
and peak flow meters.
. Mechanical insufflation–exsufflation device, such as
the Cough Assist1.
. Volume recruitment/deep lung inflation devices, such
as self-reinflating manual ventilation devices (e.g.,
Ambu1 bag).
. Mechanical ventilators and bi-level devices capable of
providing noninvasive and invasive positive pressure
ventilation.
. A selection of noninvasive ventilation interfaces
(including lip seal, nasal, and full face masks).
. Tracheostomy tubes.
Pediatric Pulmonology
TABLE 1—Recommended Diagnostic Testing for PatientsWith Duchenne Muscular Dystrophy
Testing that should be available in the clinic
Pulse oximetry
Spirometry
Capnography
Peak cough flow
Maximum inspiratory and expiratory pressure levels
Arterial blood gas sampling and analysis
Testing that should be available by referral
Overnight pulse oximetry or simultaneous pulse oximetry and
capnography measured in the patient’s home during sleep
Polysomnography
2 Birnkrant et al.

Necessary Personnel
Patients withDMDwho have respiratory complicationsshould be cared for by physicians and respiratory/physicaltherapists who are skilled in the initiation and manage-ment of noninvasive respiratory aids, including non-invasive ventilation and associated interfaces, lungvolume recruitment techniques, and manual and mechan-ically assisted cough (see the Recommendations forAssessment and Therapy Section). These personnel,techniques and equipment, including an infrastructurefor patient and caregiver education, should be available inthe clinic and hospital settings.
The home care of patients with DMD who haverespiratory complications should include close involve-ment of respiratory/physical therapists familiar with thetechniques and equipment outlined above. Sleep techni-cians performing polysomnograms on patients with DMDshould be familiar with the patterns of sleep disorderedbreathing manifested by patients with neuromuscularweakness, and should be skilled in titration and adjust-ment of noninvasive ventilation pressure levels. The panelacknowledges the intimate association between re-spiratory, cardiac, and gastrointestinal considerations inpatients with DMD. Thus, the care of persons with DMDshould take place in multi-disciplinary clinics that includea pulmonologist or other physician with respiratoryexpertise, as well as a respiratory/physical therapist,cardiologist, gastroenterologist, and nutritionist.
Recommendations for Assessment and Therapy
Monitoring of respiratory status enables timely pre-vention and management of the respiratory complicationsof DMD. A structured, proactive approach to respiratorymanagement that includes the use of assisted cough andnocturnal ventilation has been shown to prolong sur-vival.4–6 Patients with DMD are at risk for respiratorycomplications as their conditions deteriorate due toprogressive loss of respiratory muscle strength. Thesecomplications include impaired respiratory secretionclearance, atelectasis, and susceptibility to pulmonaryinfections due to ineffective cough7–15; nocturnal hypo-ventilation, progressing to hypoventilation during wake-fulness, and sleep disordered breathing.16–24 Guidelinesfor the respiratory management of DMD have alreadybeen published.3 Critical therapies include noninva-sive ventilation,25–31 lung volume recruitment techni-ques,32–34 and manual and mechanically assistedcough.35–42
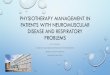
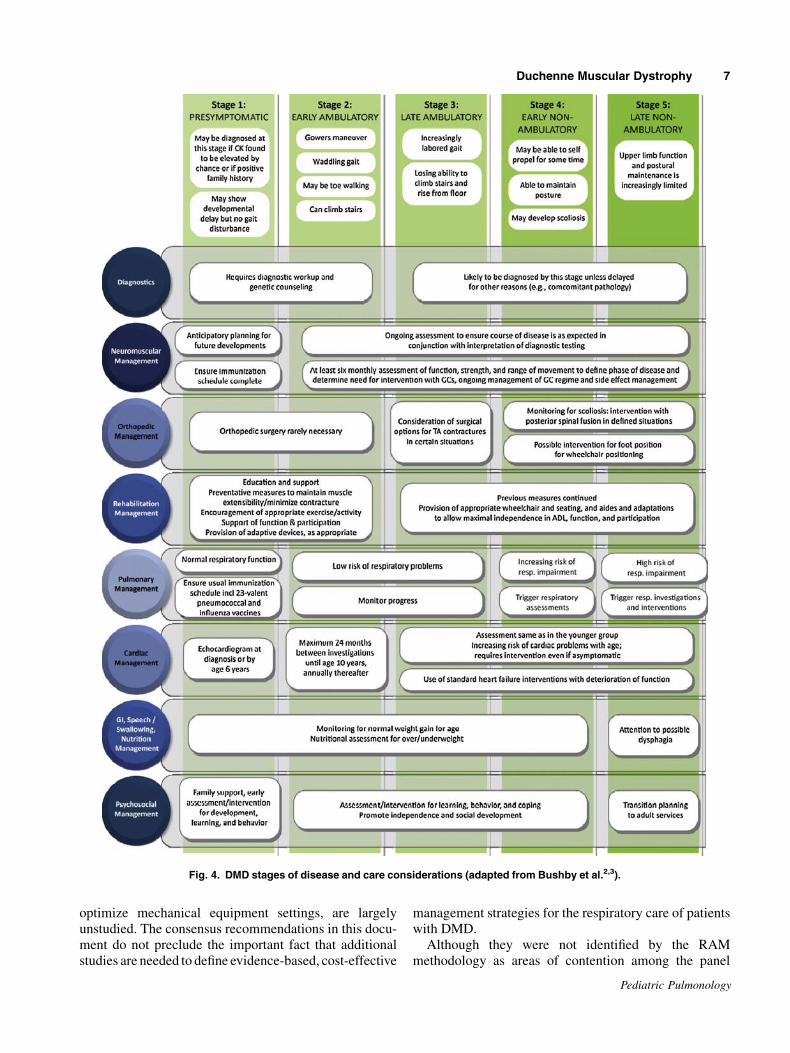
The schema, presented in Figures 1–3, outlines thewaythat assessments and interventions should be utilized inpatients with DMD as their clinical course progresses. Inthe ambulatory stage of DMD, the initial assessment ofpulmonary function (e.g., measurement of FVC at leastannually) familiarizes the patient with respiratory testing
and permits identification of each patient’s peak level ofFVC.Most active respiratorymanagement occurs after thepatient becomes nonambulatory and pulmonary functiondeclines. The pulmonary section of Figure 4 linksrecommended assessments and interventions to thevarious stages of disease and comprises a respiratoryaction plan that can be enacted as the patient progresses toincreasing levels of disease severity. Particular attention torespiratory status is required around the time of plannedsurgery (see the Respiratory Considerations for PatientsUndergoing Surgical Procedures Section).
Prevention and Treatment ofRespiratory Infections
Immunization with 23-valent pneumococcal polysac-charide vaccine (PPV23) is recommended for patients2 years of age and older. Annual immunization withtrivalent inactivated influenza vaccine (TIV) is indicatedfor patients 6 months of age and older. PPV23 and TIVarenot live vaccines, so either can be administered to patientstreated with glucocorticoids. Up-to-date, detailed infor-mation on immunization indications, contraindications,and schedules can be obtained from various sources,including the American Academy of Pediatrics (http://aapredbook.aappublications.org) and CDC (http://cdc.gov/flu). Access to the latest vaccine information isessential since recommendations can change quickly, asillustrated by the recent emergence of H1N1 influenzavirus. Moreover, the development of new vaccines (e.g.,the 13-valent conjugated pneumococcal vaccine) has thepotential to affect recommendations regarding the use ofcurrent vaccines (e.g., the 23-valent pneumococcalvaccine).In addition to the use of manually and mechanically
assisted cough, antibiotic therapy is necessary if evidenceof a lower respiratory tract infection is established byculture, and antibiotic therapy is recommended, regard-less of culture results, if a patient’s Sp02 remains below95% in room air. Supplemental oxygen therapy mayimpair central respiratory drive and exacerbate hyper-capnia.31,35,43 Thus, supplemental oxygen therapyshould be used with caution, as it can improve hypoxemiawhile masking the underlying cause, such as atelectasis,mucus plugging, or hypoventilation. When patientsexperience hypoxemia due to hypoventilation, retainedrespiratory secretions, and/or atelectasis, then manuallyand mechanically assisted cough and noninvasiveventilatory support should be used to maintainSpO2� 95% at all times; substitution by oxygen therapyalone is dangerous.6
Indications for hospitalization include the inability tomaintain SpO2 at 95% or greater in room air despitemaximal use of manually and mechanically assistedcough and noninvasive ventilation. When endotracheal
Pediatric Pulmonology
Duchenne Muscular Dystrophy 3
intubation is necessary, noninvasive ventilation can beused to facilitate extubation, even in patients with poorbaseline pulmonary function. This approach will usuallyavert the need for chronic ventilation via tracheos-tomy.44,45
Respiratory Considerations for PatientsUndergoing Surgical Procedures
The panel endorsed the recommendations of theAmerican College of Chest Physicians statement on therespiratory and relatedmanagement of patientswithDMDwho undergo anesthesia or sedation.46 The exclusive useof a total intravenous anesthetic (TIVA) technique isstrongly recommended due to the risk of malignant-
hyperthermia-like reactions and rhabdomyolysis whenpatients with DMD are exposed to inhalational anestheticagents.47,48 Depolarizing muscle relaxants like succinyl-choline are absolutely contraindicated due to the risk offatal reactions.47,48
Interventions are aimed at providing adequate respira-tory support during induction of, maintenance of, andrecovery from procedural sedation or general anesthesiaand at reducing the risk of postprocedure endotrachealextubation failure, postoperative atelectasis and/or pneu-monia.46 These goals can be achieved by providingnoninvasively assisted ventilation and assisted cough aftersurgery for patients with significant respiratory muscleweakness as indicated by sub-threshold preoperativepulmonary function test results. Preoperative training in,
Pediatric Pulmonology
Fig. 1. Respiratory assessment of a patient who has DMD (in the clinic) (adapted from Bushby
et al.2,3).
4 Birnkrant et al.
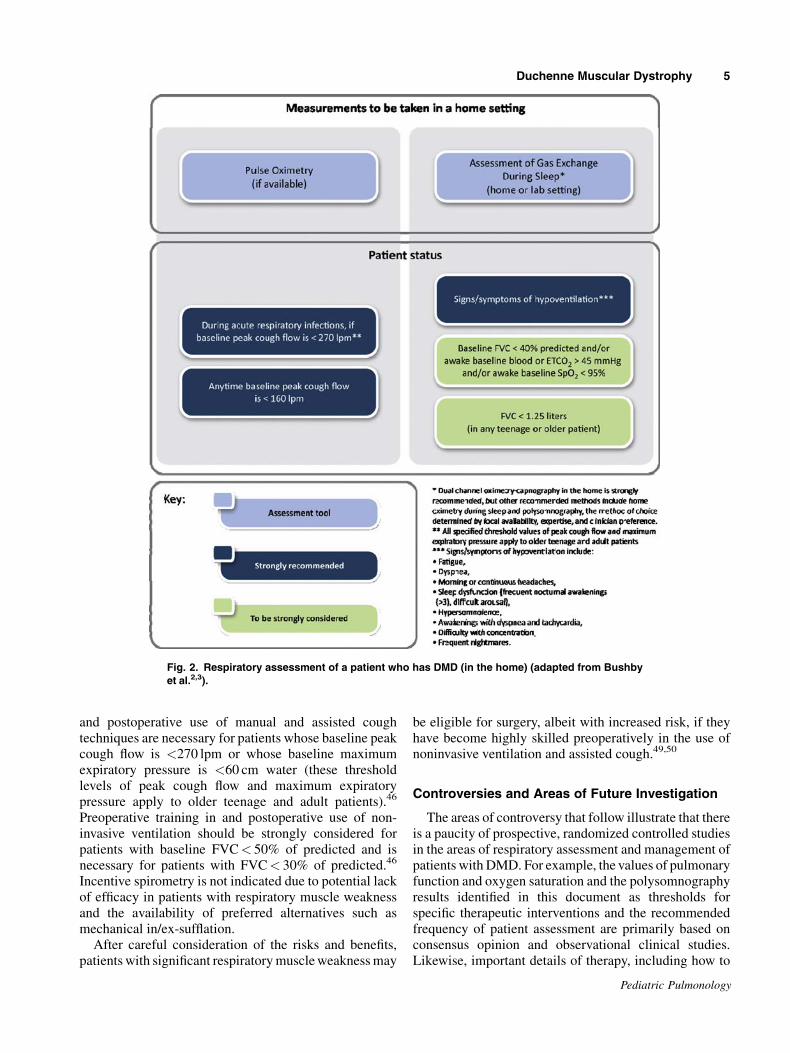
and postoperative use of manual and assisted coughtechniques are necessary for patients whose baseline peakcough flow is <270 lpm or whose baseline maximumexpiratory pressure is <60 cm water (these thresholdlevels of peak cough flow and maximum expiratorypressure apply to older teenage and adult patients).46
Preoperative training in and postoperative use of non-invasive ventilation should be strongly considered forpatients with baseline FVC< 50% of predicted and isnecessary for patients with FVC< 30% of predicted.46
Incentive spirometry is not indicated due to potential lackof efficacy in patients with respiratory muscle weaknessand the availability of preferred alternatives such asmechanical in/ex-sufflation.
After careful consideration of the risks and benefits,patients with significant respiratorymuscleweaknessmay
be eligible for surgery, albeit with increased risk, if theyhave become highly skilled preoperatively in the use ofnoninvasive ventilation and assisted cough.49,50
Controversies and Areas of Future Investigation
The areas of controversy that follow illustrate that thereis a paucity of prospective, randomized controlled studiesin the areas of respiratory assessment and management ofpatients with DMD. For example, the values of pulmonaryfunction and oxygen saturation and the polysomnographyresults identified in this document as thresholds forspecific therapeutic interventions and the recommendedfrequency of patient assessment are primarily based onconsensus opinion and observational clinical studies.Likewise, important details of therapy, including how to
Pediatric Pulmonology
Fig. 2. Respiratory assessment of a patient who has DMD (in the home) (adapted from Bushby
et al.2,3).
Duchenne Muscular Dystrophy 5
Pediatric Pulmonology
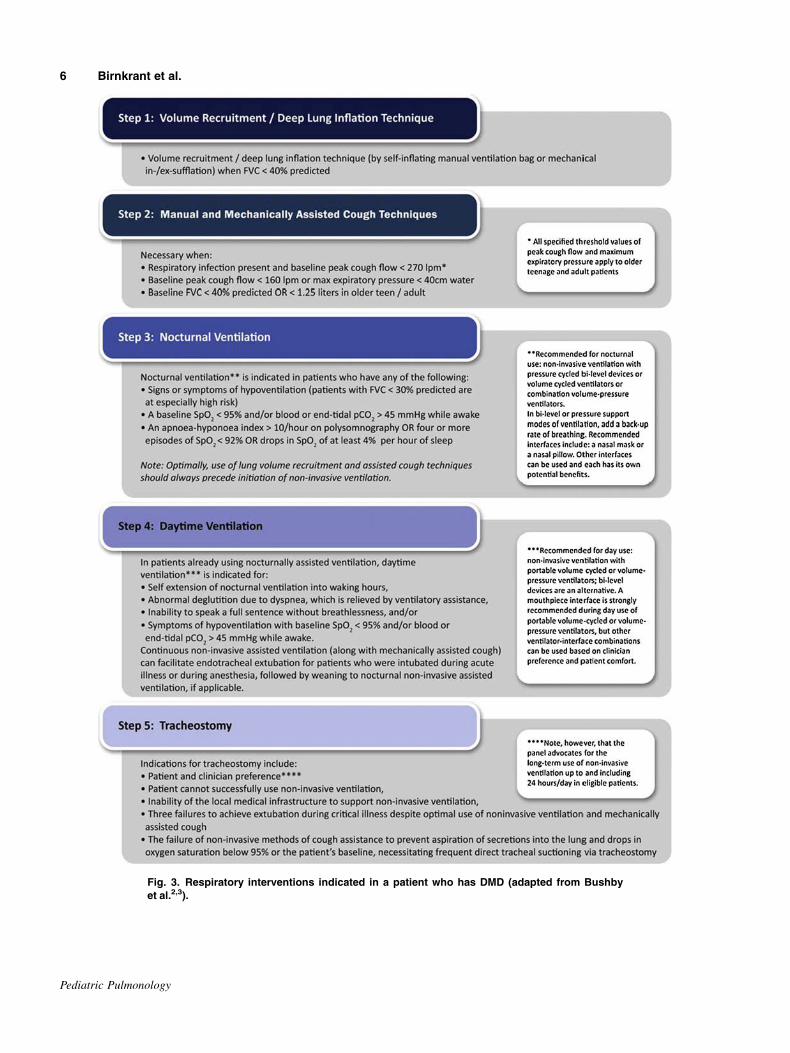
Fig. 3. Respiratory interventions indicated in a patient who has DMD (adapted from Bushby
et al.2,3).
6 Birnkrant et al.
optimize mechanical equipment settings, are largelyunstudied. The consensus recommendations in this docu-ment do not preclude the important fact that additionalstudies are needed to define evidence-based, cost-effective
management strategies for the respiratory care of patientswith DMD.Although they were not identified by the RAM
methodology as areas of contention among the panel
Pediatric Pulmonology
Fig. 4. DMD stages of disease and care considerations (adapted from Bushby et al.2,3).
Duchenne Muscular Dystrophy 7

members, a number of the recommendations in thisconsensus document may be viewed as controversial.With regard to the importance of multi-disciplinaryclinics, the unavailability of specific personnel, such asgastroenterologists with an interest in neuromusculardiseases, may make our recommendations impractical. Inthe diagnostics section of our document, we endorsemeasurement of FVC, MEP, and PCF. The equipmentneeded to measure these parameters is generally readilyavailable, and advanced skills are not required to performthe testing. However, alternative measurements such assniff inspiratory pressure,39 or use of the spirometer, ratherthan a peak flowmeter, to determine peak cough flow,mayhave merit and require further study. Also, it is not knownif there are threshold levels below which serial measure-ment of pulmonary function are no longer clinicallyuseful; for example, after patients have begun usingassisted cough devices, or after they have progressedto daytime use of assisted ventilation, there may be noclinical implications to continued deterioration intheir pulmonary function test results. With regard totherapeutics, our recommendation regarding the initia-tion of antibiotic therapy in any patient with DMD whois experiencing a respiratory infection and SpO2 below95% is controversial, because such patients may haveatelectasis rather than bacterial lower respiratory tractinfection.In addition to the areas identified above, a number of
areas were identified as uncertain and/or controversial viathe RAMmethodology, with dispersion or polarization ofopinion among the panel members. These include: the useof large tidal volumes or high-pressure span bi-levelventilation for all or most patients; the utility of chronichome use of mucus mobilizers, such as high-frequencychest wall oscillation or intrapulmonary percussiveventilation; the relative merits of polysomnographycompared with overnight oximetry or oximetry/capnog-raphy; the use of bronchodilators to aid respiratorysecretion mobilization; and the use of anticholinergics,mucolytics, or botulinum toxin for uncontrolledrespiratory secretions. The best method of assistingventilation— that is, whether to choose noninvasiveventilation or ventilation via tracheostomy—can be acontentious issue. Agreement, however, was strongamong the panel members, all of whom favored non-invasive ventilation in almost all clinical situations, asoutlined in Figure 3.Finally, the prolonged survival of patients with DMD,
which is due substantially to contemporary cardiopulmo-nary therapies, has had profound medical and psychoso-cial implications, affecting patients, their families,healthcare providers, health care delivery systems, andsociety.51 The implications of prolonged survival need tobe explored through a multi-disciplinary approachinvolving the relevant stakeholders, with the goal that
technological advances in cardiopulmonary managementthat prolong life will be accompanied by improvements inpatient quality of life.
ACKNOWLEDGMENTS
This study was funded by the National Center on BirthDefects and Developmental Disabilities/Centers for Dis-ease Control and Prevention with cooperation from theMuscular Dystrophy Association, the National Instituteon Disability and Rehabilitation Research, Parent ProjectMuscular Dystrophy, and TREAT-NMD. The authorsthank Richard S. Finkel, MD, Division of Neurology,Children’s Hospital of Philadelphia, for his advice andsupport with the production of this specialty article, andfor his careful reading of the manuscript. Dr. Amindisclosed study funding from procter and gamble and theSystic Fibrosis Foundation Therapeutics developmentNetwork and Vertes.
REFERENCES
1. Finder JD, Birnkrant D, Carl J, Farber H, Gozal D, Iannaccone
ST, Kovesi T, Kravitz RM, Panitch H, Schramm C, Schroth M,
Sharma G, Sievers L, Silvestri JM, Sterni L. Respiratory care of
the patient with Duchenne muscular dystrophy: an official ATS
consensus statement. Am J Respir Crit Care Med 2004;170:456–
465.
2. Bushby K, Finkel R, Birnkrant DJ, Case LE, Clemens PR,
Cripe L, Kaul A, Kinnett K, McDonald C, Pandya S, Poysky J,
Shapiro F, Tomezsko J, Constantin C, DMD Care Consid-
erations Working Group. Diagnosis and management of
Duchenne muscular dystrophy, part 1: diagnosis, and pharma-
cological and psychosocial management. Lancet Neurol
2010;9:77–93.
3. Bushby K, Finkel R, Birnkrant DJ, Case LE, Clemens PR, Cripe
L, Kaul A, Kinnett K, McDonald C, Pandya S, Poysky J, Shapiro
F, Tomezsko J, Constantin C, DMD Care Considerations Working
Group. Diagnosis and management of Duchenne muscular
dystrophy, part 2: implementation of multidisciplinary care.
Lancet Neurol 2010;9:177–189.
4. Phillips MF, Quinlivan CM, Edwards RH, Calverley PM.
Changes in spirometry over time as a prognostic marker in
patients with Duchenne muscular dystrophy. Am J Respir Crit
Care Med 2001;164:2191–2194.
5. Eagle M, Baudouin SV, Chandler C, Giddings DR, Bullock
R, Bushby K. Survival in Duchenne muscular dystrophy:
improvements in life expectancy since. 1967 and the impact of
home nocturnal ventilation. Neuromuscul Disord 2002;12:926–
929.
6. Gomez-Merino E, Bach JR. Duchenne muscular dystrophy:
prolongation of life by noninvasive ventilation and mechanically
assisted coughing. Am J Phys Med Rehabil 2002;81:411–
415.
7. Bach JR, Saporito LR. Criteria for extubation and tracheostomy
tube removal for patients with ventilatory failure: a different
approach to weaning. Chest 1996;110:1566–1571.
8. Dohna-Schwake C, Ragette R, Teschler H, Voit T, Mellies U.
Predictors of severe chest infections in pediatric neuromuscular
disorders. Neuromuscul Disord 2006;16:325–328.
Pediatric Pulmonology
8 Birnkrant et al.
9. Bianchi C, Baiardi P. Cough peak flows: standard values for
children and adolescents. Am J Phys Med Rehabil 2008;87:461–
467.
10. Kang SW, Bach JR. Maximum insufflation capacity: vital
capacity and cough flows in neuromuscular disease. Am J Phys
Med Rehabil 2000;79:222–227.
11. Daftary AS, Crisanti M, Kalra M, Wong B, Amin R. Effect of
long-term steroids on cough efficiency and respiratory muscle
strength in patients with Duchenne muscular dystrophy. Pedia-
trics 2007;117:e320–e324.
12. Gauld LM, Boynton A. Relationship between peak cough flow
and spirometry in Duchenne muscular dystrophy. Pediatr
Pulmonol 2005;39:457–460.
13. Suarez AA, Pessolano FA, Monteiro SG, Ferreyra G, Capria ME,
Mesa L, Dubrousky A, DeVito EL, Peak flow and peak cough
flow in the evaluation of expiratory muscle weakness and bulbar
impairment in patients with neuromuscular disease. Am J Phys
Med Rehabil 2002;81:506–511.
14. Domenech-Clar R, Lopez-Andreu JA, Compte-Torrero L, De
Diego-Damia A, Macian-Gisbert V, Perpina-Tordera M, Roques-
Serradilla JM. Maximal static respiratory pressures in children
and adolescents. Pediatr Pulmonol 2003;35:126–132.
15. Szeinberg A, Tabachnik E, Rashed N, McLaughlin FJ, England S,
Bryan CA, Levison H. Cough capacity in patients with muscular
dystrophy. Chest 1988;94:1232–1235.
16. Smith PE, Calverley PM, Edwards RH. Hypoxemia during sleep
in Duchenne muscular dystrophy. Am Rev Respir Dis 1998;137:
884–888.
17. Phillips MF, Smith PE, Carroll N, Edwards RH, Calverley PM.
Nocturnal oxygenation and prognosis in Duchenne muscular
dystrophy. Am J Respir Crit Care Med 1999;160:198–202.
18. Hukins CA, Hillman DR. Daytime predictors of sleep hypo-
ventilation in Duchenne muscular dystrophy. Am J Repir Crit
Care Med 2000;161:166–170.
19. Ragette R, Mellies U, Schwake C, Voit T, Teschler H. Patterns
and predictors of sleep disordered breathing in primary
myopathies. Thorax 2002;57:724–728.
20. Khan Y, Heckmatt JZ. Obstructive apnoeas in Duchenne muscular
dystrophy. Thorax 1994;49:157–161.
21. Barbe F, Quera-Salva MA, McCann C, Gajdos P, Raphael JC, de
Lattre J, Agusti AG. Sleep-related respiratory disturbances in
patients with Duchenne muscular dystrophy. Eur Respir J
1994;7:1403–1408.
22. Uliel S, Tauman R, Greenfeld M, Sivan Y. Normal polysomno-
graphic respiratory values in children and adolescents. Chest
2004;125:872–878.
23. Toussaint M, Steens M, Soudon P. Lung function accurately
predicts hypercapnia in patients with Duchenne muscular
dystrophy. Chest 2007;131:368–375.
24. Culebras A. Sleep-disordered breathing in neuromuscular dis-
ease. Sleep Med Clin 2008;3:377–386.
25. Eagle M, Bourke J, Bullock R, Gibson M, Mehta J, Giddings D,
Straub V, Bushby K. Managing Duchenne muscular dystrophy—
the additive effect of spinal surgery and home nocturnal
ventilation in improving survival. Neuromuscul Disord 2007;17:
470–475.
26. Ward S, Chatwin M, Heather S, Simonds AK. Randomised
controlled trial of non-invasive ventilation (NIV) for nocturnal
hypoventilation in neuromuscular and chest wall disease patients
with daytime normocapnia. Thorax 2005;60:1019–1024.
27. Bach JR, Alba AS. Management of chronic alveolar hypoventi-
lation by nasal ventilation. Chest 1990;97:52–57.
28. Mellies U, Ragette R, Dohna Schwake C, Boehm H, Voit T,
Teschler H. Long-term noninvasive ventilation in children and
adolescents with neuromuscular disorders. Eur Respir J
2003;22:631–636.
29. Simonds AK, Muntoni F, Heather S, Fielding S. Impact of nasal
ventilation on survival in hypercapnic Duchenne muscular
dystrophy. Thorax 1998;53:949–952.
30. Piastra M, Antonelli M, Caresta E, Chiaretti A, Polidori
G, Conti G. Noninvasive ventilation in childhood acute
neuromuscular respiratory failure. Respiration 2006;73:791–
798.
31. Niranjan V, Bach JR. Noninvasive management of pediatric
neuromuscular respiratory failure. Crit Care Med 1998;26:1952–
1953.
32. Bach JR, Bianchi C, Vidigal-Lopes M, Turi S, Felisari G. Lung
inflation by glossopharyngeal breathing and ‘‘air stacking’’ in
Duchenne muscular dystrophy. Am J Phys Med Rehabil 2007;86:
295–300.
33. Bach JR, Kang SW. Disorders of ventilation: weakness, stiffness
and mobilization. Chest 2000;117:301–303.
34. Bach JR. Management goals in noninvasive ventilation. In: Bach
JR, editor. Guide to the evaluation and management of neuro-
muscular disease. Philadelphia: Hanley and Belfus; 1999.
pp. 101–109.
35. Tzeng AC, Bach JR. Prevention of pulmonary morbidity for
patients with neuromuscular disease. Chest 2000;118:1390–
1396.
36. Dohna-Schwake C, Ragette R, Teschler H, Voit T, Mellies U.
IPPB-assisted coughing in neuromuscular disorders. Pediatr
Pulmonol 2006;41:551–557.
37. Miske LJ, Hickey EM, Kolb SM, Weiner DJ, Panitch HB. Use of
the mechanical in-exsufflator in pediatric patients with neuro-
muscular disease and impaired cough. Chest 2004;125:1406–
1412.
38. Boitano JL. Management of airway clearance in neuromuscular
disease. Respir Care 2006;51:913–922.
39. Fauroux B, Guillemot N, Aubertin G, Nathan N, Labit A,
Clement A, Lofaso F. Physiological benefits of mechanical
insufflation-exsufflation in children with neuromuscular diseases.
Chest 2008;133:161–168.
40. Chatwin M, Ross E, Hart N, Nickol AH, PolkeyMI, Simonds AK.
Cough augmentation with mechanical insufflation/exsufflation in
patients with neuromuscular weakness. Eur Respir J 2003;21:
502–508.
41. Winck JC, Goncalves MR, Lourenco C, Viana P, Almeida J, Bach
JR. Effects of mechanical insufflation-exsufflation on respiratory
parameters for patients with chronic airway secretion encum-
brance. Chest 2004;126:774–780.
42. Homnick DN. Mechanical insufflation-exsufflation for airway
mucus clearance. Respir Care 2007;52:1296–1307.
43. Smith PE, Edwards RH, Calverley PM. Oxygen treatment of
sleep hypoxaemia in Duchenne muscular dystrophy. Thorax
1989;44:997–1001.
44. Pope JF, Birnkrant DJ. Noninvasive ventilation to facilitate
extubation in a pediatric intensive care unit. J Intensive Care Med
2000;15:99–103.
45. Bach JR, Goncalves MR, Hamdami I, Winck JC. Extubation of
patients with neuromuscular weakness: a new management
paradigm. Chest 2009. DOI:10.1378/chest.09-2144.
46. Birnkrant DJ, Panitch HB, Benditt JO, Boitano LJ, Carter ER,
Cwik VA, Finder JD, Iannaccone ST, Jacobson LE, Kohn GL,
Motoyama EK, Moxley RT, Schroth MK, Sharma GD, Sussman
MD. American College of Chest Physicians consensus statement
on the respiratory and related management of patients with
Duchenne muscular dystrophy undergoing anesthesia or sedation.
Chest 2007;132:1977–1986.
Pediatric Pulmonology
Duchenne Muscular Dystrophy 9

47. Hayes J, Veyckemans F, Bissonnette B. Duchenne muscular
dystrophy: an old anesthesia problem revisited. Pediatr Anesth
2008;18:100–106.
48. Yemen TA, McClain C. Muscular dystrophy, anesthesia and the
safety of inhalational agents revisited, again. Paediatr Anaesth
2006;16:105–108.
49. Bach JR, Sabharwal S. High pulmonary risk scoliosis surgery:
role of noninvasive ventilation and related techniques. J Spinal
Disord Tech 2005;18:527–530.
50. Lumbierres M, Prats E, Farrero E, Monasterio C, Gracia T,
Manresa F, Escarrabill J. Noninvasive positive pressure ventila-
tion prevents postoperative pulmonary complications in chronic
ventilator users. Respir Med 2007;101:62–68.
51. Birnkrant DJ. New challenges in the management of
prolonged survivors of pediatric neuromuscular diseases: a
pulmonologist’s perspective. Pediatr Pulmonol 2006;41:1113–
1117.
Pediatric Pulmonology
10 Birnkrant et al.
Recommended