June 22, 2011
Nevada Partnership for Value-Driven Healthcare
HealthInsight
Peg M. Bradke, RN, MA
St. Luke’s Hospital, Cedar Rapids, Iowa
Teachback
St. Luke‟s Hospital
Member of Iowa Health System
• Private hospital
• Part of the Iowa Health System
• Licensed for 500 Beds with more than 17,000
admissions
• Top 100 Heart Hospital for three years
• Magnet designation 2009
• The Joint Commission Disease-Specific
Certification for Advanced Heart Failure since
2008
Transition to Home Team
Heart Failure team since 2001
St. Luke‟s joined the Institute for Health Care
Improvement (IHI) Innovation Project for Transitions
to Home in February 2006
Work concentrated on the Heart Failure patient to
provide the “ideal” transition to home
Goal: To Improve the reliability of the care patients
receive and resultant outcomes
Worked in tandem with compliance to CMS Core
Measures
Current State: Spread transition process to Pulmonary
population
Who Owns the Transition?
Are we placing the burden on the patient?
What is causing the readmissions? Do we know?
Are we being proactive?
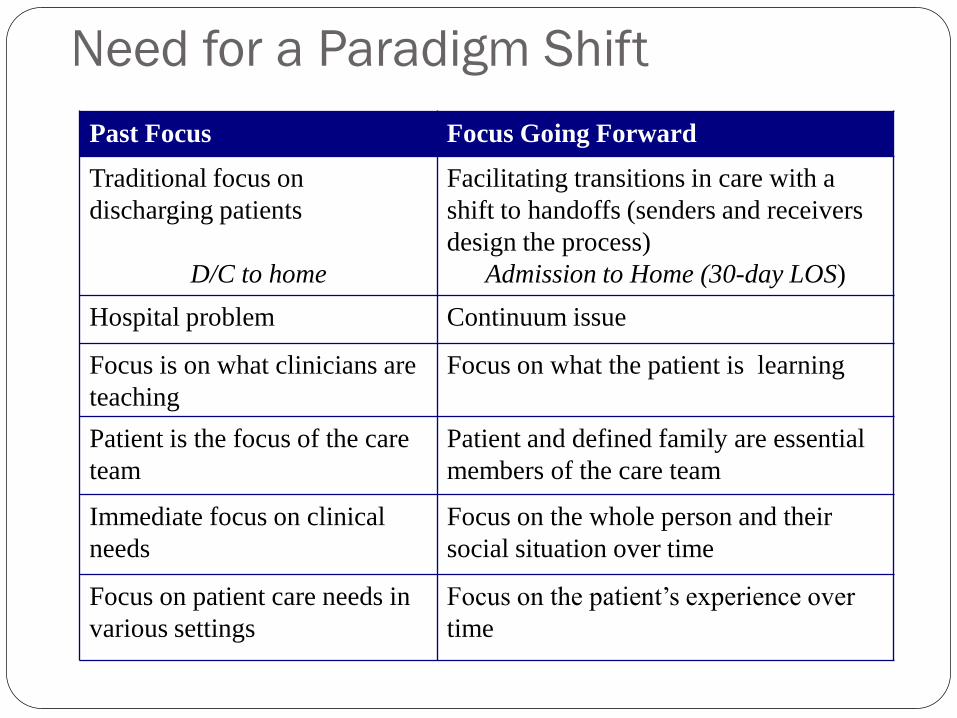
Need for a Paradigm Shift
Past Focus Focus Going Forward
Traditional focus on
discharging patients
D/C to home
Facilitating transitions in care with a
shift to handoffs (senders and receivers
design the process)
Admission to Home (30-day LOS)
Hospital problem Continuum issue
Focus is on what clinicians are
teaching
Focus on what the patient is learning
Patient is the focus of the care
team
Patient and defined family are essential
members of the care team
Immediate focus on clinical
needs
Focus on the whole person and their
social situation over time
Focus on patient care needs in
various settings
Focus on the patient’s experience over
time

St. Luke‟s Heart Failure Continuum
Standardized care through order sets
Patients identified via BNP daily reports
Written discharge instructions sent home with patient and available immediately on-line in clinic or community facilities with portals
Teach back - Utilizing Universal Health Literacy Concepts performed in hospital, at Home Care visit, at seven-day follow-up call
Touch points
Home Care - care coordination visit 24 to 48 hours post discharge
Follow-up physician clinic visit appointment in three to five days
APN - follow-up phone call on seventh day post discharge
Outpatient Heart Failure class – seeing increased participation
Collaboration with cardiology office Heart Failure Clinic

Degree of Will
This is important to our organization for two reasons: It is part of our Mission: “To give the care we would like our
loved ones to receive”
It is part of our strategic plan for preventing avoidable
readmission to be proactive for Health Care Reform changes.

Institute for Healthcare Improvement
How to Guide: Creating an Ideal Transition to Home
SNF
Office Practice
http://www.ihi.org/IHI/Topics/MedicalSurgicalCare/MedicalSurgicalCareGeneral/Tools/TCABHowToGuideTransitionHomeforHF.htm

How-to Guide: Creating an Ideal Transition Home
Creating an Ideal Transition Home
I. Perform Enhanced Admission Assessment for Post-Hospital Needs
A. Include family caregivers and community providers as full partners in completing
standardized assessments, planning discharge, and predicting home-going needs.
B. Reconcile medications upon admission.
C. Initiate a standard plan of care based on the results of the assessment.
II. Provide Effective Teaching and Enhanced Learning
A. Identify all learners on admission.
B. Customize the patient education process for patients, family caregivers, and
providers in community settings.
C. Use “Teach Back” daily in the hospital and during follow-up phone calls to assess the
patient‟s and family caregivers‟ understanding of discharge instructions and ability to
perform self-care.
III. Conduct Real-Time Patient and Family-Centered Handoff Communication
A.Reconcile medications at discharge.
B.Provide customized, real-time critical information to the next care provider(s).
IV. Ensure Post-Hospital Care Follow-Up
A. High-risk patients: Prior to discharge, schedule a face-to-face follow-up visit (home
care visit, care coordination visit, or physician office visit) to occur within 48 hours
after discharge.
B. Moderate-risk patients: Prior to discharge, schedule a follow-up phone call within 48
hours and schedule a physician office visit within five days.
Provide Effective Teaching and
Facilitate Enhanced Learning
Changes:
A. Customize the patient education materials and
processes for patients and family caregivers
B. Identify all learners on admission
C. Use teach back regularly throughout the hospital stay to
assess the patient’s and family caregivers’ understanding
of discharge instructions and ability to perform self-care

Provide Effective Teaching and Facilitate
Enhanced Learning
Typical Failures:
• Assuming the patient is the key learner
• Providing written discharge instructions that are confusing,
contradictory to other instructions, or not tailored to a
patient’s level of health literacy or current health status
• Failure to ask clarifying question about instructions and plan of
care – limited time for discussion
• Overestimating patient’s understanding of information
• Communicating too much information at one time

Patient Factors
Age – cognitive function decreases with age starting in
mid 50’s
Lower literacy rates
Language barriers
Nervousness, emotional response to information, lack of
focus, medications, in a hurry to be discharged
Language barriers

Provide Effective Teaching and
Facilitate Enhanced Learning
A.Customize the patient education materials and processes for
patients and family caregiversRedesign written materials using Health Literacy principles
Redesign teaching methods
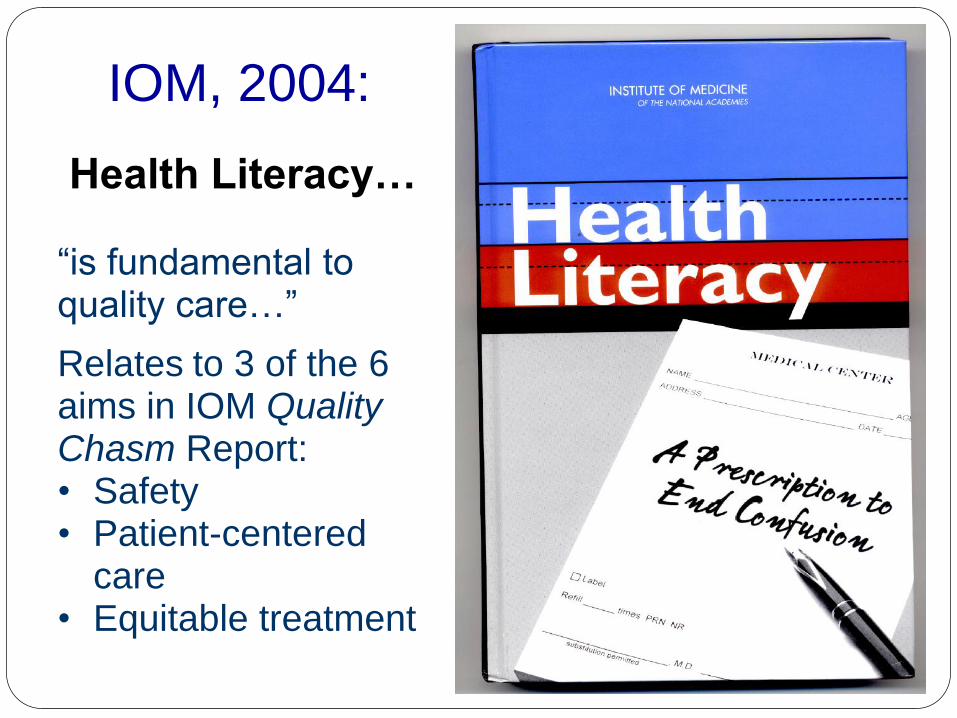
IOM, 2004:
Health Literacy…
“is fundamental to quality care…”
Relates to 3 of the 6 aims in IOM Quality Chasm Report:• Safety• Patient-centered
care• Equitable treatment
Inadequate Health Literacy
Literacy is a predictor of health status
Literacy is a stronger predictor than age, income,
employment status, educational level or racial or ethnic
group
Baker DW, et al. Am J of Public Health, 2002.
Schillinger et al. JAMA, 2002.

16
Universal Communication Principles
• Everyone benefits from clear information.•
• Many patients are at risk of misunderstanding
but it is difficult to identify them.
• Assessing reading levels in the clinical setting
does not ensure patient understanding.

People may hide their
limited reading ability
*Parikh N Pt Education and Counseling 1996
Percent Who Never Told*
19%
52%
62%68%
85%91%
75%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Supervisor Coworkers Health Care
Providers
Spouses Friends Children Anyone
17

Inadequate Health Literacy
Half of the US population may be at risk
Lower receipt of preventive services
Poorer knowledge of chronic conditions
Higher utilization of services (including hospitalizations)
Worse health outcomes
Williams MV, Baker DW, Parker RM, et al. Relationship of functional health
literacy to patient’s knowledge of their chronic disease. Arch Intern Med. 1998;
158:166-172.
Scott TL, Gazmararian JA, Williams MV, et al. Health literacy and preventive
health care use among Medicare enrollees in a managed care organization.
Medical Care. 2002; 40(5):395-404.
18
19
Keys to Success with Health Literacy
Use universal health literacy communications principles to redesign
written teaching materials
User-friendly written materials use:
Simple words (1-2 syllables)
Short sentences (4-6 words)
Short paragraphs (2-3 sentences)
No medical jargon
Headings and bullets
Highlighted or circled key information
Lots of white space
Two-word explanations: “water pill/blood pressure pill”
Increase font size
Remove ranges
On all written material, assure words/ terminology match
Use visual aids
Provide a health context for numbers or values
Two-word explanations: “water pill/blood pressure pill”
Keys to Success with Health Literacy
21
Universal Communication Principles
Focus on key points
Need to know vs. nice to know
Emphasize what patient should do
Avoid duplicating paperwork
Be careful with color

22
Redesign Patient Teaching Materials
During acute care hospitalizations for HF, only essential
education is recommended
Reinforce within one to two weeks after discharge
Continue for three to six months
Adams, KF et al: HFSA 2006 Comprehensive Heart Failure Practice Guideline. Journal of Cardiac Failure
Vol. 12, No. 1, pg. 61 February 2006

23
Intervention: Patient Education Material
Key “small tests of change”
Cross-Continuum Team reviewed content of educational
materials utilizing health literacy concepts with goal to have
similar material that built on each other
Outpatient Heart Failure class utilized as focus group for
content
Family member on team, along with her siblings, reviewed
content for understanding Health Literacy

24
Evaluation of New Patient Education
Material
Results from 15 follow-up phone calls:
“Information very helpful.”
Able to state where information was and reported that they
were referring to it.
Understood content.
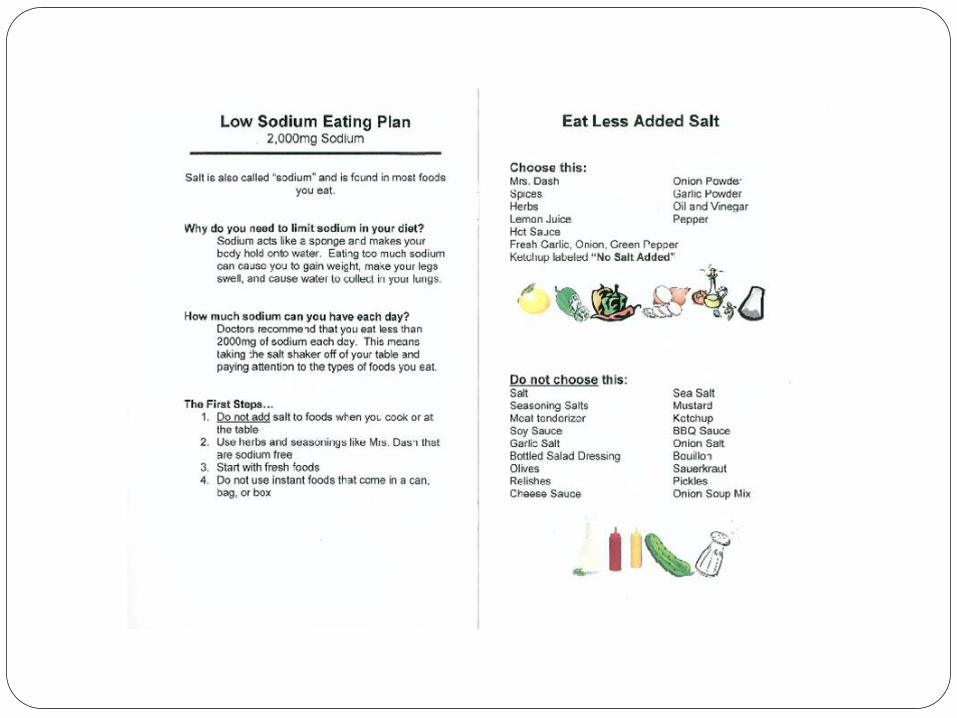
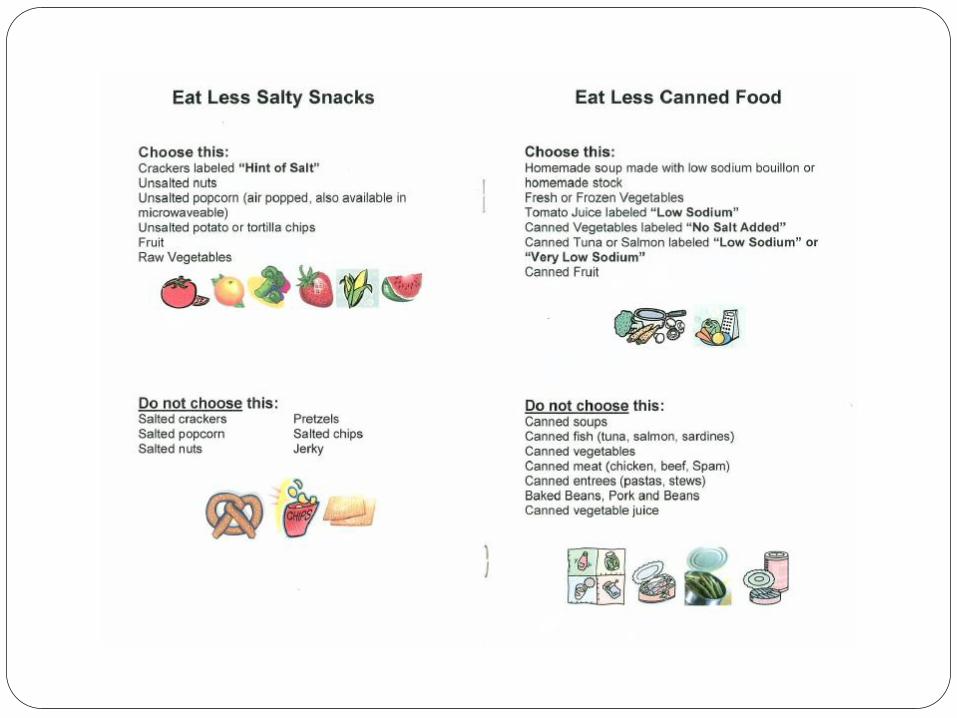
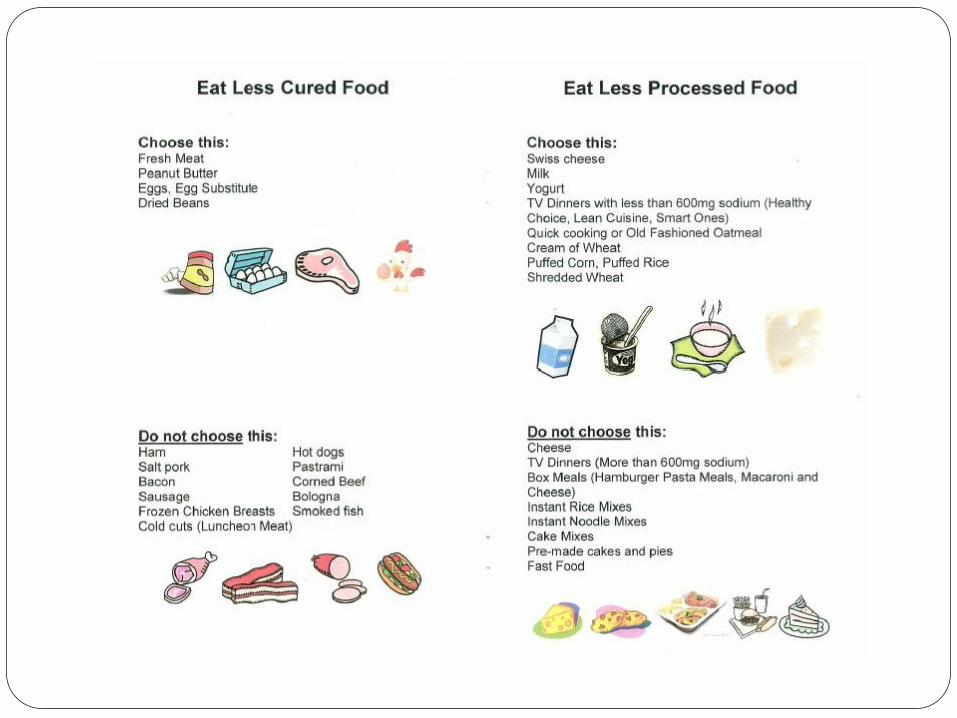
St Luke‟s Hospital, Cedar Rapids, Iowa

Heart Failure Magnet

Heart Failure Zones
EVERY DAY
Every day:
Weigh yourself in the morning before breakfast and write it down.
Take your medicine the way you should. Check for swelling in your feet, ankles, legs and stomach Eat low salt food Balance activity and rest periods
Which Heart Failure Zone are you today? Green, Yellow or Red
GREEN ZONE
All Clear This zone is your goal Your symptoms are under control You have:
No shortness of breath No weight gain more than 2 pounds
(it may change 1 or 2 pounds some days) No swelling of your feet, ankles, legs or stomach No chest pain
YELLOW ZONE
Caution This zone is a warning Call your doctor’s office if:
You have a weight gain of 3 pounds in 1 day or a weight gain of 5 pounds or more in 1 week
More shortness of breath More swelling of your feet, ankles, legs, or stomach Feeling more tired. No energy Dry hacky cough
Dizziness Feeling uneasy, you know something is not right It is harder for you to breathe when lying down. You are needing to
sleep sitting up in a chair
RED ZONE
EMERGENCY Go to the emergency room or call 911 if you have any of the following:
Struggling to breathe. Unrelieved shortness of breath while sitting still
Have chest pain Have confusion or can’t think clearly
2/6/09
Heart Failure Zones

27
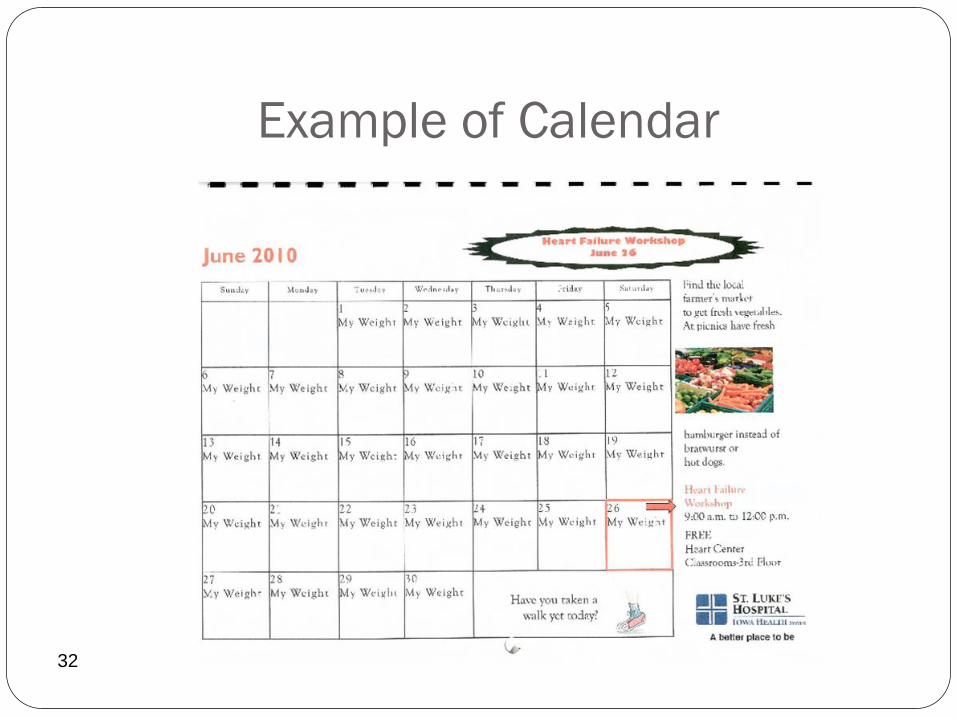
Example of Calendar
32

Provide Effective Teaching and
Facilitate Enhanced Learning
B. Identify all learners on admission
Identify the appropriate family caregivers who will assist the patient with self-care after discharge
Be sure that the right learners are involved in all critical self-care education
List the names of the key learners on the whiteboard and care plan
Who Are Key Learners?
Caregiver and/or patient may not be the “key learner”.
Who helps the patient with:
Understanding what’s being said
Self-care activities at home
Setting up or taking medications
Getting to appointments
Navigating care and treatments
Ask key learners how they prefer their education, e.g. written, verbal, video
34

Sample of White Board
Helping Staff Make It Happen
Including family caregivers in learning is essential, but hard
Make it easy for the front line caregivers to:
Know who needs to participate in learning & how/when to reach them
Give learners access to getting their questions answered in the hospital and after
discharge
Know and pass along critical information about learners to next care settings
E.g. patient and family caregivers cannot teach back or have low confidence in doing
self care

Provide Effective Teaching and
Facilitate Enhanced Learning
C.Use teach back regularly throughout the hospital stay to assess the
patient’s and family caregiver’s understanding of discharge
instructions and ability to perform self-care
• Include all the learners
• Assess patient’s ability to understand and
Do critical self-care activities
Take medications
Access care: next appointments, medications, etc.
• Close the gap in understanding or develop a new plan of care
38
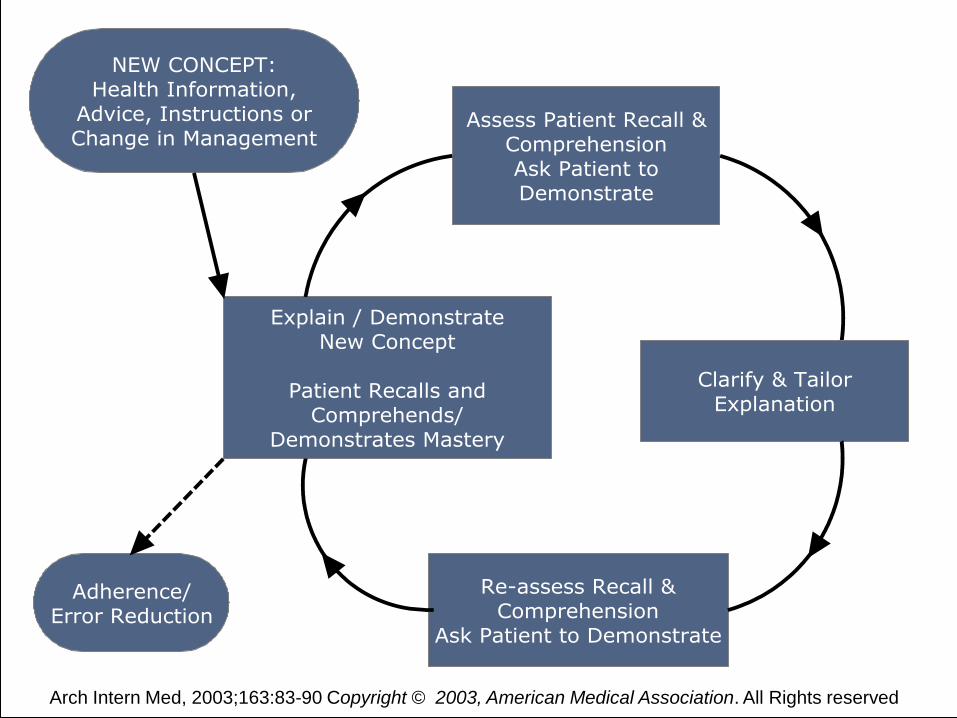
Arch Intern Med, 2003;163:83-90 Copyright © 2003, American Medical Association. All Rights reserved

How Often Do We Close the Loop?
Checkpoints to evaluate how well transactions are going.
How well are we doing giving the information?

Paradigm Shift
“The patient is noncompliant”
vs.
Asking: What is our responsibility as the sender of the
information?

42
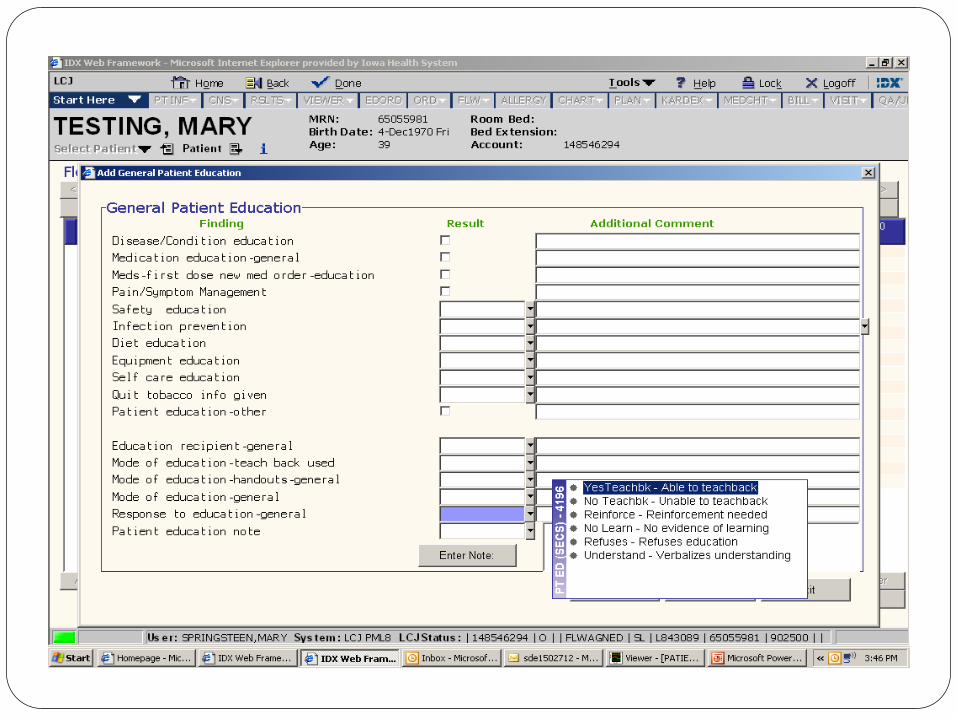
Enhanced Teaching and Learning
Ask in a non-shaming way for the individual to explain in his or
her own words what was understood
Example: “I want to be sure that I did a good job of teaching
you today about how to stay safe after you go home. Could
you please tell me in your own words the reasons you should
call the doctor?”
43
Enhanced Teaching and Learning
Utilizing “Teach Back”
Explain needed information to the patient or family caregiver.
You do not want your patient to view Teach Back as a test, but
rather of how well you explained the concept. You can place
the responsibility on yourself.
Can be both a diagnostic and teaching tool
44
Enhanced Teaching and Learning Slow down when speaking to the patient and family and
break messages into short statements
Take a pause
Use plain language, breaking content into short statements
Segment education to allow for mastery
45
Enhance Teaching and Facilitate Learning
Use Teach Back daily:
In the hospital
During home visits and follow-up visits/calls
To assess the patients’ and family caregivers’ understanding of
discharge instructions and ability to do self-care.
The teach back method not only can uncover
misunderstanding, but also can reveal the nature of the
misunderstanding, so communication can be corrected or
tailored to the patient needs.
46
Enhanced Teaching and Learning
Redesign patient teaching:
Stop and check for understanding using teach back after teaching each segment of the information
If there is a gap, review again
If your patient is not able to repeat the information accurately, try to re-phrase the information rather than just repeating it. Then, ask the patient to repeat again until you feel comfortable that the patient understood.
Try to use teach back as many times as you can when you interact with the patient
Common perception is:
It will take more time
It should not substantially take more time

48
HF Teach Back Questions
What is the name of your water pill?
What weight gain should you report to your doctor?
What foods should you avoid?
Do you know what symptoms to report to your doctor?
St Luke‟s Hospital, Cedar Rapids, Iowa

COPD Teach-back Questions
What should you do first if you are having more trouble with your breathing?
What is the name of your fast-acting/rescue inhaler?
How often do you use it?
If your shortness of breath continues without getting better, what should you do?
What are the warning signs for you that would indicate that you should call your doctor?
What should you do to prevent from having a flare-up (getting worse) with your breathing and lungs?
50
Teach-back with Discharge Instructions
• Can you show me on these instructions:
• how you find your doctors’ office
appointment?
• What other tests you have scheduled? and
when?
• Is there anything on these instructions that could
be difficult for you to do?
• Have we missed anything?
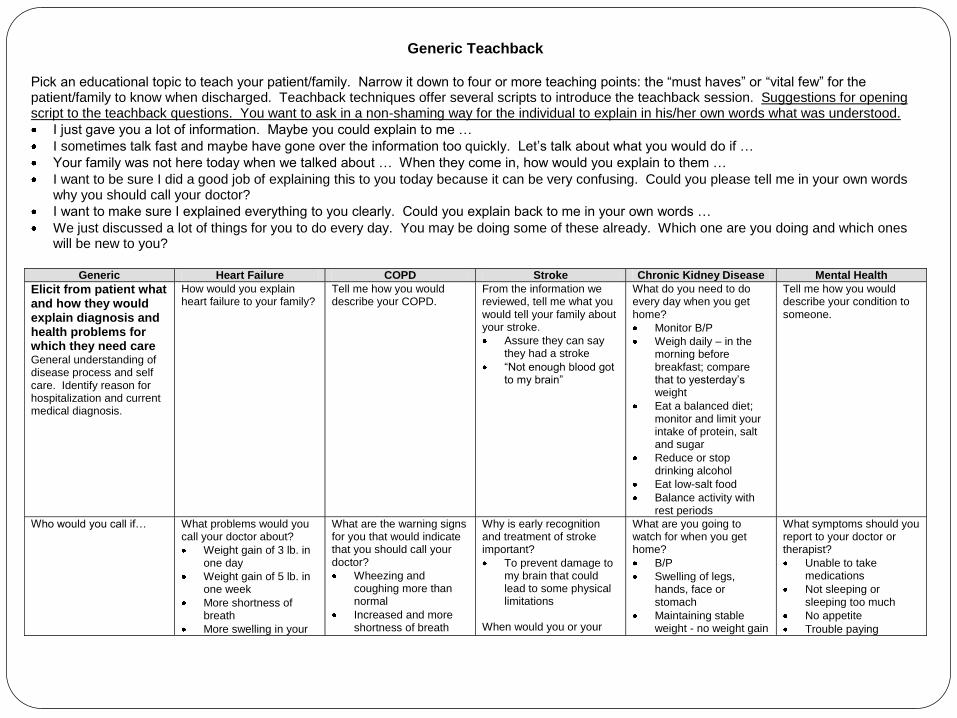
Generic Teachback
Pick an educational topic to teach your patient/family. Narrow it down to four or more teaching points: the “must haves” or “vital few” for the patient/family to know when discharged. Teachback techniques offer several scripts to introduce the teachback session. Suggestions for opening script to the teachback questions. You want to ask in a non-shaming way for the individual to explain in his/her own words what was understood.
I just gave you a lot of information. Maybe you could explain to me …
I sometimes talk fast and maybe have gone over the information too quickly. Let‟s talk about what you would do if …
Your family was not here today when we talked about … When they come in, how would you explain to them …
I want to be sure I did a good job of explaining this to you today because it can be very confusing. Could you please tell me in your own words why you should call your doctor?
I want to make sure I explained everything to you clearly. Could you explain back to me in your own words …
We just discussed a lot of things for you to do every day. You may be doing some of these already. Which one are you doing and which ones will be new to you?
Generic Heart Failure COPD Stroke Chronic Kidney Disease Mental Health
Elicit from patient what and how they would explain diagnosis and health problems for which they need care General understanding of disease process and self care. Identify reason for hospitalization and current medical diagnosis.
How would you explain heart failure to your family?
Tell me how you would describe your COPD.
From the information we reviewed, tell me what you would tell your family about your stroke.
Assure they can say they had a stroke
“Not enough blood got to my brain”
What do you need to do every day when you get home?
Monitor B/P
Weigh daily – in the morning before breakfast; compare that to yesterday‟s weight
Eat a balanced diet; monitor and limit your intake of protein, salt and sugar
Reduce or stop drinking alcohol
Eat low-salt food
Balance activity with rest periods
Tell me how you would describe your condition to someone.
Who would you call if… What problems would you call your doctor about?
Weight gain of 3 lb. in one day
Weight gain of 5 lb. in one week
More shortness of breath
More swelling in your
What are the warning signs for you that would indicate that you should call your doctor?
Wheezing and coughing more than normal
Increased and more shortness of breath
Why is early recognition and treatment of stroke important?
To prevent damage to my brain that could lead to some physical limitations
When would you or your
What are you going to watch for when you get home?
B/P
Swelling of legs, hands, face or stomach
Maintaining stable weight - no weight gain
What symptoms should you report to your doctor or therapist?
Unable to take medications
Not sleeping or sleeping too much
No appetite
Trouble paying
52
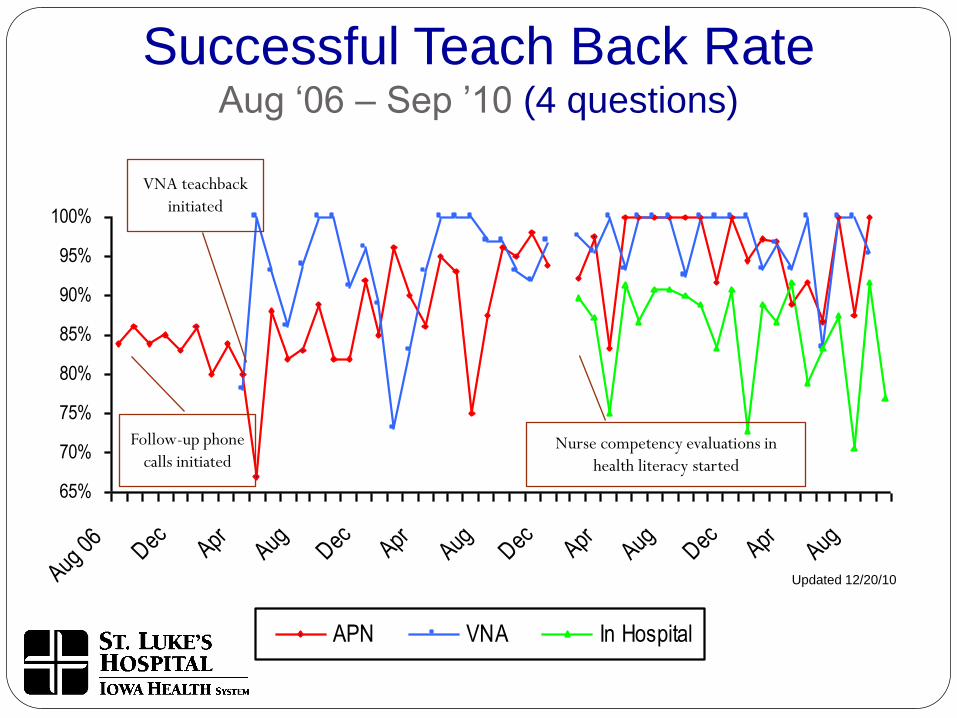
Teach Back Success
Percent of time patients can teach back 75% or more of
content taught related to the transition to home utilizing
the four questions related to self management of heart
failure
Stop and check for understanding using teach back after
teaching each segment of information
Assess patient’s, family’s or caregiver’s ability and
confidence
Go Observe: “Be a Patient”
What can you learn about the current state of patient teaching
and learning?
For patients being taught self-care, e.g., reasons to call the
physician after discharge
Look for teaching and teach back: staff tone of voice, attitude,
non-shaming language, body language, plain terminology,
request for teach back in the patient’s own words, and no “do
you understand” questions
Small Tests of Change Using Teach Back
Test 1: One nurse on one day tests whether Teach Back with one
patient helps the patient learn the reasons to call the physician for
help after discharge (e.g., weight gain, difficulty breathing, or
exhaustion). Documents % of patients who taught back 75%.
Test 2: Nurse tests whether a video is more effective than verbal
teaching. Documents % who taught back 75% after the video.
Test 3: Nurse tests whether using Teach Back on every day of the
patient’s stay increases retention.
Process Measure
Enhanced Teaching and Learning
Percent of nurses with Teach Back competency
Percent of patients with:
Preferred learning method documented on admission
75% recall and restate on Teach Back for:
Reasons to call the physician after returning home
Medications, uses, doses
65%
70%
75%
80%
85%
90%
95%
100%
Aug 0
6Dec Apr
Aug Dec AprAug Dec Apr
Aug Dec AprAug
APN VNA In Hospital
Successful Teach Back RateAug „06 – Sep ‟10 (4 questions)
Updated 12/20/10
VNA teachback
initiated
Follow-up phone
calls initiatedNurse competency evaluations in
health literacy started
What Are We Learning About Enhanced
Teaching and Facilitation of Learning?
Team members generally have readily embraced teach back to enhance patient teaching.
Team members on medical and surgical units can immediately test this approach to
enhance patient education.
Teach back must be practiced and perfected over time.
There is value in multiple teaching sessions with patients and family caregivers.
Many hospitals have spread teach back competencies to all hospital staff and include
these competencies in the yearly competency certification process.
There is a need for uniform and patient-friendly teaching materials in all clinical
settings for the common clinical conditions.

59
Teach Back Competency Validation
St Luke’s Hospital, Cedar Rapids, Iowa
Nursing Competency Assessment
Annual competency validation day
Methodology
The learning station will use discussion, role playing and
patient teaching scenarios to help RN’s communicate
effectively to patient/family.

60
Staff Competency Validation for Teach
Back
Each participant will participate in a role-play providing
education to a patient. The following will be assessed:
Ability to do teach back in a shame-free way, e.g., tone is
positive
Utilizes plain language for explanations
Does not ask patient, “Do you understand?”
Staff Competency Validation for Teach
Back
Uses statements such as:
“I want to make sure I explained everything clearly to you. Can you please
explain it back to me in your own words?”
OR
“I want to make sure I did a good job explaining this to you because it can be
very confusing. Can you tell me what changes we decided to make and how
you will take your medicine now?”
If needed, participant will clarify and reinforce the explanation to
improve patient understanding

Teach Back Practice #1
Read the following exactly as written as if you are teaching a patient.
“I am going to talk to you about the signs of heart failure. The signs of heart failure are:
Dyspnea on exertion
Weight gain from fluid retention
Edema in your lower extremities and abdomen
Fatigue
Dry, hacky cough
Difficulty breathing when supine”
Teach Back Practice #1
Read the following as written as if you are teaching a patient.
“I am going to talk to you about the signs of heart failure. The signs of heart failure are:
Shortness of Breath
Weight gain from fluid build-up
Swelling in feet, ankles, legs or stomach
Dry, hacky cough
Feeling more tired, no energy
It’s harder for you to breath when lying down”

Teach back Practice #5-B
Read the following as written as if you are teaching a patient.
“I am going to talk to you about the signs of heart failure. The signs of heart failure are:
Shortness of Breath
Weight gain from fluid build-up
Swelling in feet, ankles, legs or stomach
Dry, hacky cough
Feeling more tired, no energy
“Do you understand these?” “Do you have questions?”
Teach back Practice #5-G
Read the following as written as if you are teaching a patient.
“I am going to talk to you about the signs of heart failure. The signs
of heart failure are:
Shortness of Breath
Weight gain from fluid build up
Swelling in feet, ankles, legs or stomach
Dry hacky cough
Feeling more tired. No energy
“I know we just talked about a lot of things. Your wife wasn’t able to be with us today. When she asks you what we talked about, what are you going to tell her?”

Evaluation What was the patient’s reaction?
What was it like for you as the nurse doing teach back?
Did it feel like extra work?
How would you build teach back into the daily work?
How could you use teach back to communicate to the team?

Teach back #2-B
Read the following as if you are really busy and hurried. Have your voice show being rushed or irritated.
“I’m going to talk to you about what you need to do every day at home to control your heart failure.
Every day: Weigh yourself in the morning before breakfast and write it down Take your medication the way you should Check for swelling in your feet, ankles, legs and stomach Eat low-salt food Balance activity and rest periods”

Teach back #2-GRead the following as if you have all the time in the world to teach this patient. Your
voice sounds positive, helpful and pleasant.
“I’m going to talk to you about what you need to do every day at home to control your heart failure.
Every day:
Weigh yourself in the morning before breakfast and write it down
Take your medication according to this record
Check for swelling in your feet, ankles, legs and stomach
Eat low-salt food
Balance activity and rest periods
Teach back Practice #3-BRead the following as if you are quizzing the patient. You are making the patient feel like they
are on the spot by asking them to repeat the information you just told them. It sounds like a test for the patient.
“ I’m going to talk to you about what you need to do every day at home to control your heart failure.
Every day:
Weigh yourself in the morning before breakfast and write it down
Take your medication the way you should
Check for swelling in your feet, ankles, legs and stomach
Eat low-salt food
Balance activity and rest periods.
List four things for me that you are going to do everyday?”

Teach back Practice #3-G
Read the following as written as if you are teaching a patient.
“I’m going to talk to you about what you need to do every day at home to control your heart failure.
Every day:
Weigh yourself in the morning before breakfast and write it down
Take your medication the way you should
Check for swelling in your feet, ankles, legs and stomach
Eat low-salt food
Balance activity and rest periods.
I teach people about this every day, and sometimes I go over it quickly or may not make myself clear. I want to make sure you know what you need to do. So, can you tell me some things you will do each day?

Teach back Practice #3-G
Read the following as written as if you are teaching a patient.
“I’m going to talk to you about what you need to do every day at home to control your heart failure.
Every day:
Weigh yourself in the morning before breakfast and write it down
Take your medication the way you should
Check for swelling in your feet, ankles, legs and stomach
Eat low-salt food
Balance activity and rest periods.
We just discussed a lot of things for you to do every day. You might be doing some of these already. Have you already been doing any of these things? What do you think will be the hardest one for you to do at home?”

Health Literacy
“If they don’t do what we want, we haven’t given them the right
information.”
Vice Admiral Richard Carmona,
Former Surgeon General
Recommended