8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 1/21
4/28/
Alarming StatisticsAlarming Statistics TBI: leading cause of death and disability in
children
-- in USin US: 79/ 100000 admission for head injury,
chidren: 200000 head injury /year: 10%severe TBI
Nationa l Centers for Injury Prevention and Control.
-- in KSAin KSA: NGH: 1598 admissions :664MVA: 378: TBI:
24% severe TBI: 30 diedCrankson SJ; mo tor vehic le injuries in childhoo d: a hospita l-based study in Saud i Arabia, Ped iatr Surg Int 2006
Mortality : 22% severe TBIDucrocq. Epidem iology a nd predic tive fact ors of mo rtality and o utco me in children
with traumat ic severe b rain injury: experience of a French p ediat ric trauma ce nter.Pediat ric C rit Care Me d. 2006
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 2/21
4/28/
Result of the direct mechanical damage that occurs at
the time of trauma→ focal lesions: skull fracture, epidural hematoma, sub
ura ema oma, n racere ra ema oma
→ Diffuse axonal injury
Occurs after the initial trauma: the damage to neuronsdue to the systemic physiologic response to the initial injury
→ Release of cytokines, free radicals, glutamate:
→ deleterious cascade of continued cell membrane
break down that further harm the injured brain→ Hypotension and hypoxia are majors causes of
secondary brain injuryBishop . Curr Probl Pediatr Adolesc Health Ca re Oct 2006
PediatricPed iatric CritCrit Care MedCare Med 20032003Vol.Vol. 44, No., No. 33 (Suppl.)(Suppl.)
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 3/21
4/28/
Objectives
Review the new developments and
advances in the field pediatric TBI since
the 2003 guidelines
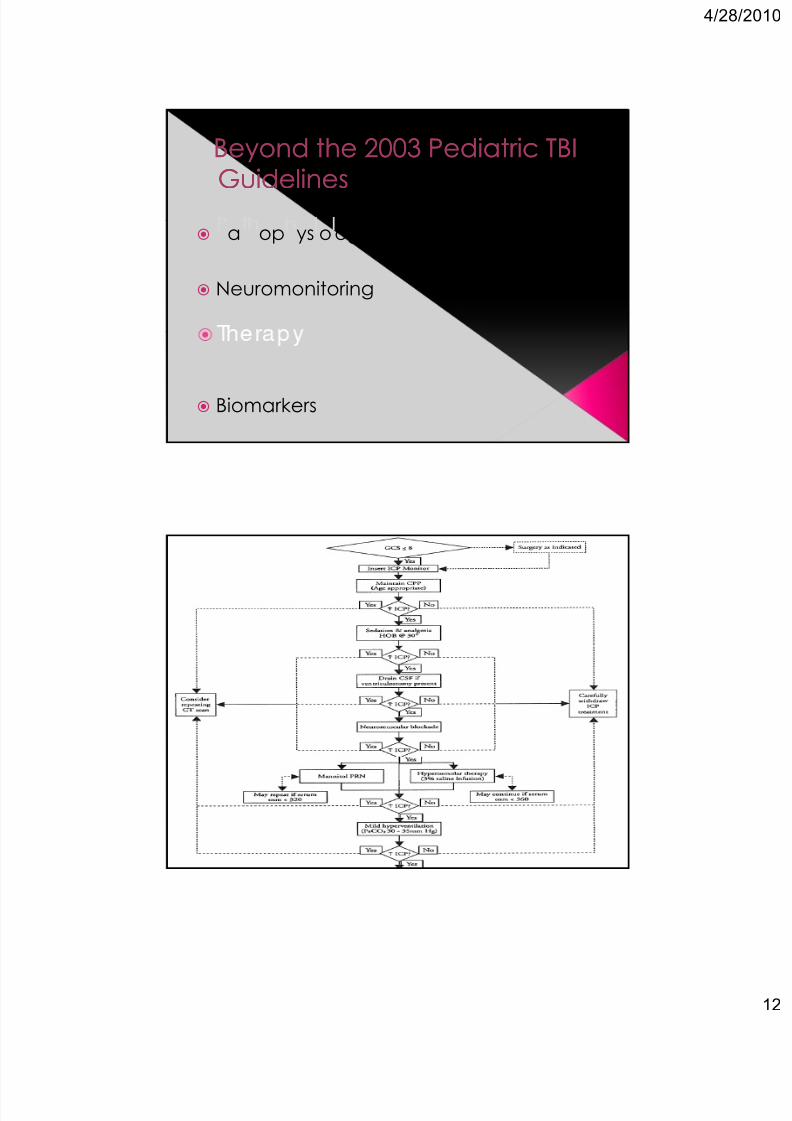
Beyond the 2003 Pediatric TBIBeyond the 2003 Pediatric TBIGuidelinesGuidelines
y y
Neuromonitoring
Biomarkers
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 4/21
4/28/
Beyond theBeyond the 20032003 Pediatric TBIPediatric TBIGuidelinesGuidelines
a op ys o ogy
Neuromonitoring
Biomarkers
Optimal CPP
Guidelines Guidelines .
CPP in children with TBI should be
maintained > 40mmHg
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 5/21
4/28/
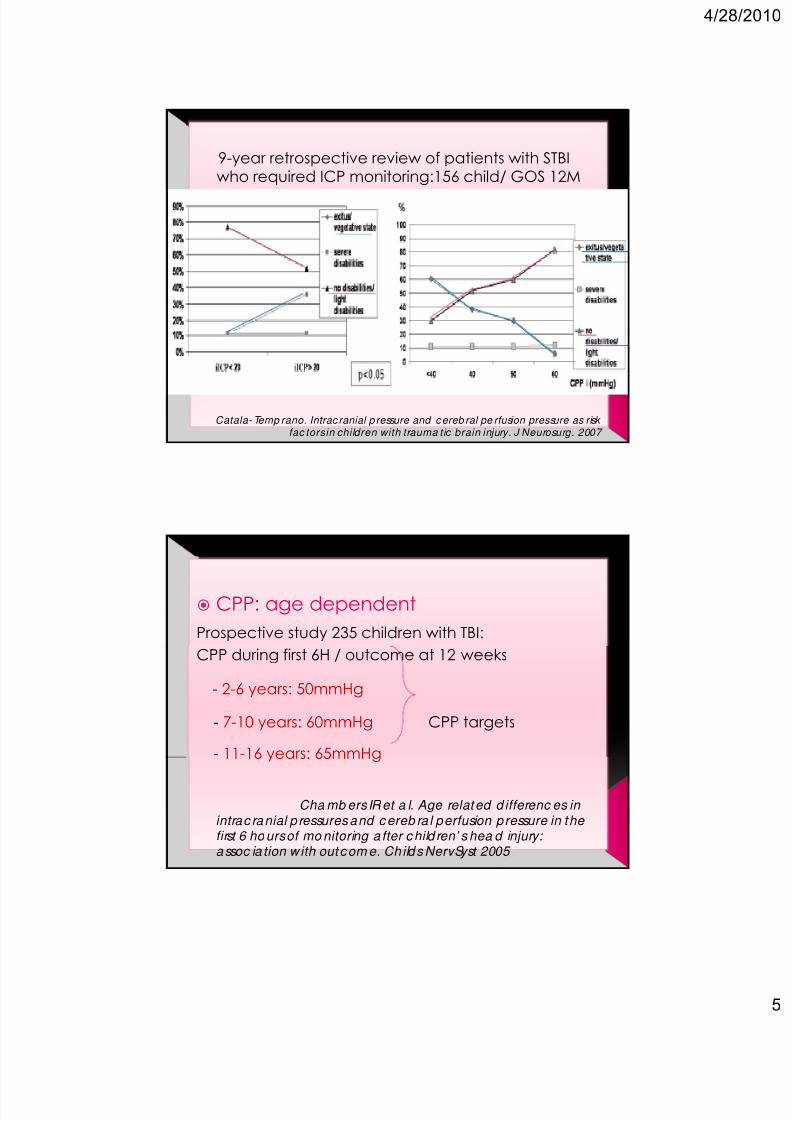
9-year retrospective review of patients with STBIwho required ICP monitoring:156 child/ GOS 12M
Catala- Temp rano. Intrac ranial p ressure and c ereb ral pe rfusion pressure as risk fac torsin children with trauma tic brain injury. J Neurosurg. 2007
CPP: age dependent
Prospective study 235 children with TBI:
CPP during first 6H / outcome at 12 weeks
- 2-6 years: 50mmHg
- 7-10 years: 60mmHg CPP targets
- 11-16 years: 65mmHg
Cha mb ers IR et a l. Age related d ifferenc es in intrac ranial p ressures and c ereb ra l perfusion pressure in the first 6 ho urs of mo nitoring a fter c hild ren’ s hea d injury: assoc ia tion w ith out com e. Childs NervSyst 2005
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 6/21
4/28/
Beyond theBeyond the 20032003 Pediatric TBIPediatric TBIGuidelinesGuidelines
a op ys o ogy
Neuromonitoring
erapy
Biomarkers
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 7/21
4/28/
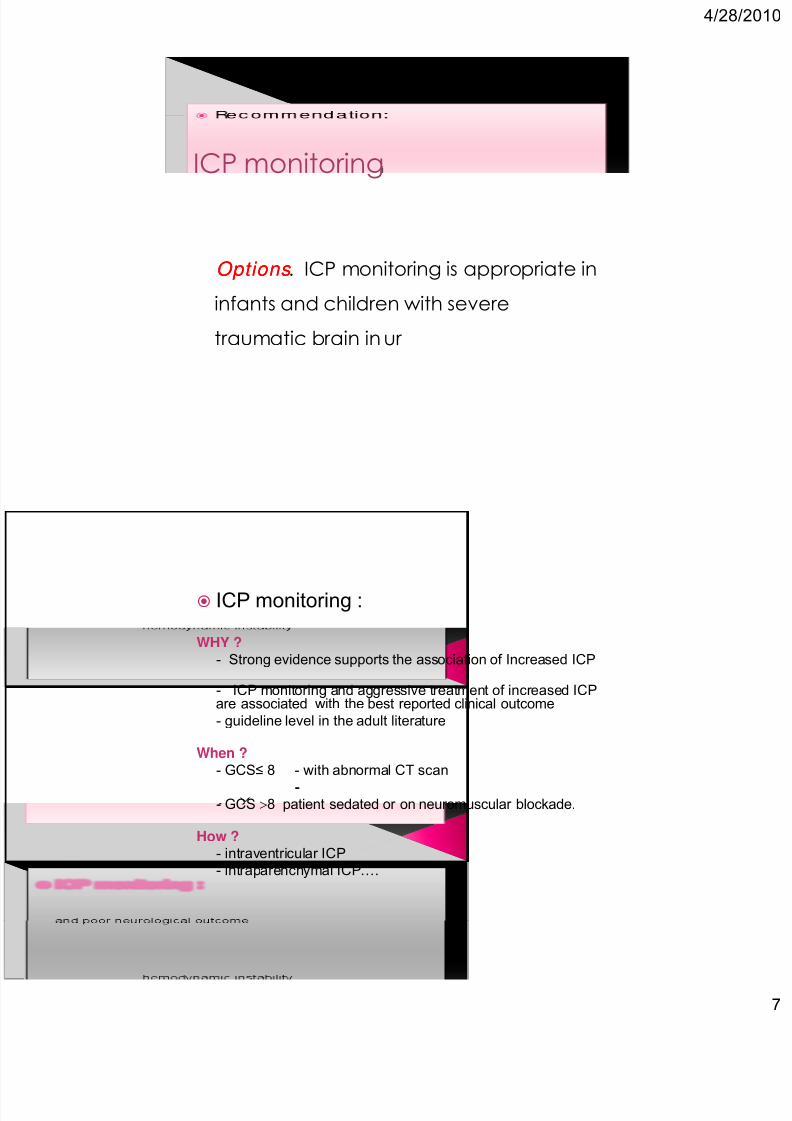
ICP monitoring
Options Options . ICP monitoring is appropriate in
infants and children with severe
traumatic brain in ur
ICP monitoring :
WHY ?
- Strong evidence supports the association of Increased ICP
- ICP monitoring and aggressive treatment of increased ICPare associated with the best reported clinical outcome
- guideline level in the adult literature
When ?
- GCS≤ 8 - with abnormal CT scan
--- GCS 8 patient sedated or on neuromuscular blockade.
How ?
- intraventricular ICP
- intraparenchymal ICP….
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 8/21
4/28/
Aim:Aim:
to monitor the effect of intervention
( hyperventila tion to test fo r auto-reg ula tory c apab ilities within the bra in…)
to detect significant cerebral hypoxia
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 9/21
4/28/
PbO2 > 25mmHg +
( ICP< 20mmHg, CPP> 60mmHg): decreasedmortalit 44%vs 25%, <0.O5
Stiefel MF et a l. Red uce d m ortality rat e in pa tient with sever trauma tic b rain injury trea ted with b rain tissue oxygen m onito ring. J Neurosurg 2005
- PbO2 < 20mmHg in 11/14 after standardresuscitation to ICP and CPP goals
- PbO2 respond to O2
- PbO2 was increased in survivors (p=0.009)Narotam PK et a l cerebral oxygenation in ma jor ped iatric trauma a nd its relevance to trauma severity and outco me . J ped Surg 2006
- mean (Vm> 30cm/s) diastolic (Vd>20cm/s) blood flow velocity /MCA
- Pulsatility index( PI= (Vs-Vd/Vm<1.4)
CPPni = MBP x Vd/Vm +14
Reactivity to CO2 : cerebral autoregulation
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 10/21
4/28/
TCD «TCD « goalgoal-- directed therapydirected therapy »»
Assess Vm, Vd, PI at T0 and treat with mannitol andnorepinephrine:
46% abnormal TCD value and 2 @ the time of
insertion of ICP monitoring
ICP was greater in patients with abnormal TCD @admission
CPP and SjvO2 were normal: more adequatecere ra resusc a on
Rac t C et al. Transc ranial Dopple r ultrasound goal-direc ted therapy for the ea rly ma nage ment of severe traumatic brain injury.Intensive Ca re Me d. 2007
The specificity of PI for detecting an ICP≥ 20mmHg is high, but the sensitivity is verylow.
The relationship between PI and the CPPappears to be stronger.
Figag i AA et al. Transc ranial Dop pler pulsat ility index is not a reliab le indic a to r of intrac rania l p ressure in ch ild ren with severe TBI.
Surgic a l Ne urolog y 2009
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 11/21
4/28/
Detection of convulsion:
-
convulsive seizure in adult TBI/ increased
ICP and interstitial Lactate/pyruvate
Vespa PM. Et al. Nonc onvulsive elec trograp hic seizures aft er
traum at ic brain injury result in a d elayed , prolonged inc rease in intrac ranial pressure and m eta bolic c risis. Crit Ca re Med . 2007
Evaluation of brain function by analysisof the synchronous nature of cEEG
EEGEEG Prognostic value in patient with disorder of
consciousness post TBI.
Bag at o S et a l. Prognostic va lue of stand ard EEG in trauma tic
and non traum at ic d isorders of c onsiousness following co ma . Clin Neurop hysiol 2010
EEG-SEP changes identify brain function
deterioration. changes can precede an ICPincrease and they can constitute acomplementary tool to interpret ICP trends.
Am an tini A e ta l. Co ntinuous EEG-SEP monito ring in seve re bra in injury. Neurop hysiol Clin. 2009
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 12/21
4/28/
Beyond the 2003 Pediatric TBIBeyond the 2003 Pediatric TBIGuidelinesGuidelines
a op ys o ogy
Neuromonitoring
Biomarkers
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 13/21
4/28/
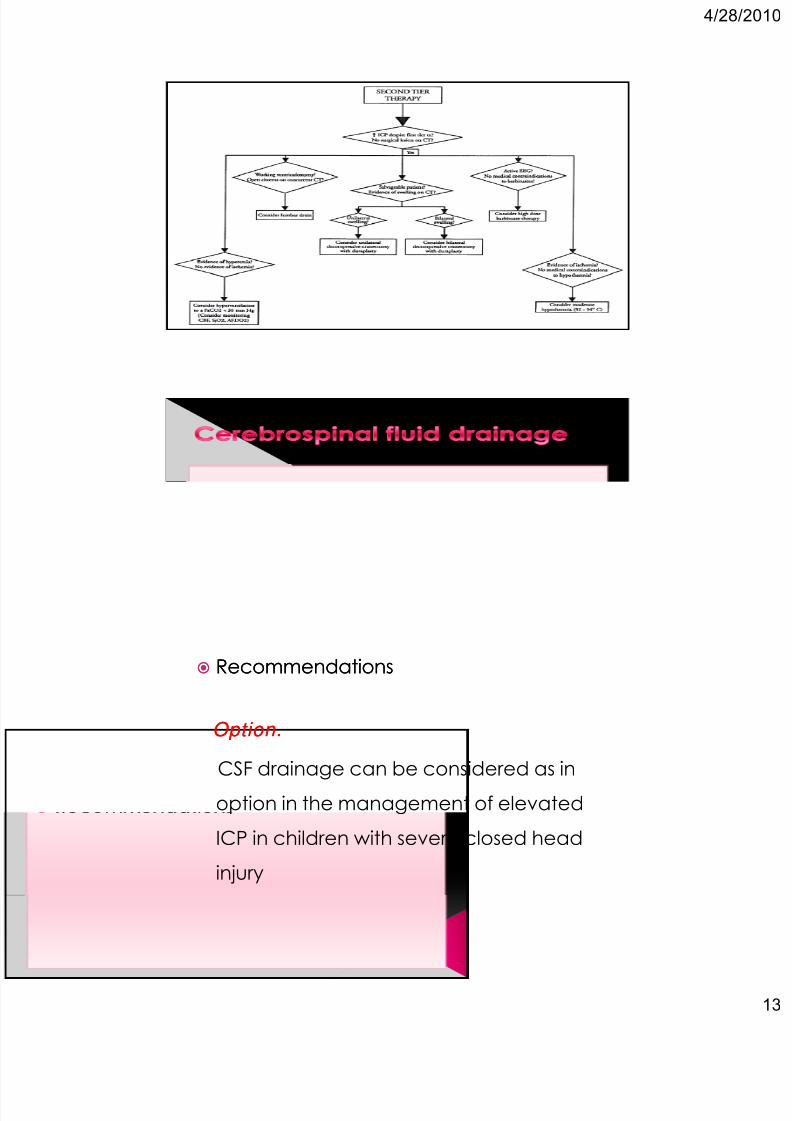
RecommendationsRecommendations
Option.Option.
CSF drainage can be considered as in
option in the management of elevated
ICP in children with severe closed head
injury
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 14/21
4/28/
continuous CSF drainage > intermittentcontinuous CSF drainage > intermittentCSF drainage ?CSF drainage ?
ompare o c ra nage, ra nage wasassociated with :
- 2 fold greater CSF concentrations of CSF
mediator (p < 0.05)
- ≈1/2 the volume of CSF removal (p = 0.002).
- Higher mean ICPs (21.8 vs13.6 mm Hg, p < 0.0001).
Shore PM e t a l . Continuous versus intermittent
c ereb rospina l fluid drainage aft er seve re trauma tic b rain injury in c hildren: effec t o n b ioc hemica l markers. J Neurotrauma . 2004.
RecommendationsRecommendations
Options.Options.
Decompressive craniectomy should be
considered in pediatric patients with
severe TBI, diffuse cerebral swelling, and
intracranial hypertension refractory to
intensive medical management
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 15/21
4/28/
Decompressive craniectomy
Indications:Indications:
Diffuse cerebral swelling on CT brain
Within 48hrs of injury
No episodes of sustained ICP>40mmHg
GCS>3 at some point subsequent toinjury
Secondary clinical deterioration Evolving cerebral herniation
Dec omp ressive c raniectomy As Rescue therapyAs Rescue therapy:
Jaganna than J et al. Outc ome following dec omp ressive craniec tomy in children with severe TBI: a10-year single cente r experience with long term follow up . J Neurosurg 2007
As Early intervention:As Early intervention:
- Survival rate : 100% craniectomy group vs 33% in
the non-operative group.
- 1 year GOS was better in the craniectomy group.
Josan VA Sgouros S. Early dec omp ressive craniec tomy ma y be effec tive in the treat ment of refracto ry intracranial hypertension after trauma tic b rain injury .Ch ilds Nerv Syst. 2006
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 16/21
4/28/
Recommendations
Options.Options.
- Extrapolated from the adult data, hyperthermia
should be avoided in children with severe TBI
- Despite the lack of clinical data in children,
hypothermia may be considered in the setting of
refractory intracranial hypertension
Mechanisms of action
Antioxidant effect
Decrease metabolism and O2
consumption
Risk: coagulop athy , IC hemorrhage,
arrhythmia
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 17/21
4/28/
Phase II c linica l trial- Moderate HYPO after severe TBI in children was found
to be safe- early hypothermia : better mortality rate
Adelson PD Phase II clinical trial of mod erate hyp othermia a fter severe traumatic brain injury in children. Neurosurgery 2005
CANADIAN Phase III clinical trial:- Hypothermia group had worse outcome
- Methodology?
Hutchison J et al. Hy -HIT Investigators anad canad ian critical c are trial group . Hypotherm ia the rapy after TBI in child ren. N.Engl.j.Med .2008
Ongoing US Phase III TRIAL: Cool Kids TrialAdelson PD. Hypo thermia following ped iatric traum atic b rain injury.
J Neurotraum a. 2009 .
AntiAnti--seizure Prophylaxisseizure Prophylaxis
Recommendations:Recommendations:
Guidelines.Guidelines.
Prophylactic anti-seizure therapy may beconsidered to prevent early PTS in pediatric patient
Options.Options.
Prophylactic use of anti-seizure therapy is notrecommended for children with severe TBI for
Indications from adult guidelinesIndications from adult guidelines
Use of phenytoin has been shown to decrease therisk of early PTS. There is no evidence that outcomeis improved.
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 18/21
4/28/
New anti-epileptics drugs
LEV patients/ PHT patients:
- better long-term outcomes :
lower Disability Rating Scale score at 3 months
(P = 0.042) and higher GOS at 6 months (P = 0.039).
-occurrence during cEEG or at 6 months
and in mortality .
Szaflarski JP et al. Prospe c tive, rand om ized , single-blinded c om pa rative trial of intravenous levetirac eta m versus phe nytoin for
seizure prop hylaxis. Neuroc rit Ca re 2010
Beyond theBeyond the 20032003 Pediatric TBIPediatric TBIGuidelinesGuidelines
y y
Neuromonitoring
Biomarkers
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 19/21
4/28/
Assesses neuronal death
Early peak level after TBI(<12h)Delayed in inflected neurotrauma
Marker of astrocyte death or injury
Maximal early peak after the insult
Biomarker of axonal injury
Increased only in TBI and inflectedneurotrauma and not HIE
Serum biomarker:- Adjunct to clinical examination in case of
inflicted trauma
- Prognostic factors
Berger s et a l Serum bioma rker c onc entrations and
outc ome afte r pe diatric trauma tic b rain injury. J Neurotraum a. 2007
Multiplex methods: /CSF analysis
- Assessments of multi le markers(cytokines)
- Assess the effect of therapy on the
biochemical response to TBI
Urine: source for biomarkers
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 20/21
4/28/
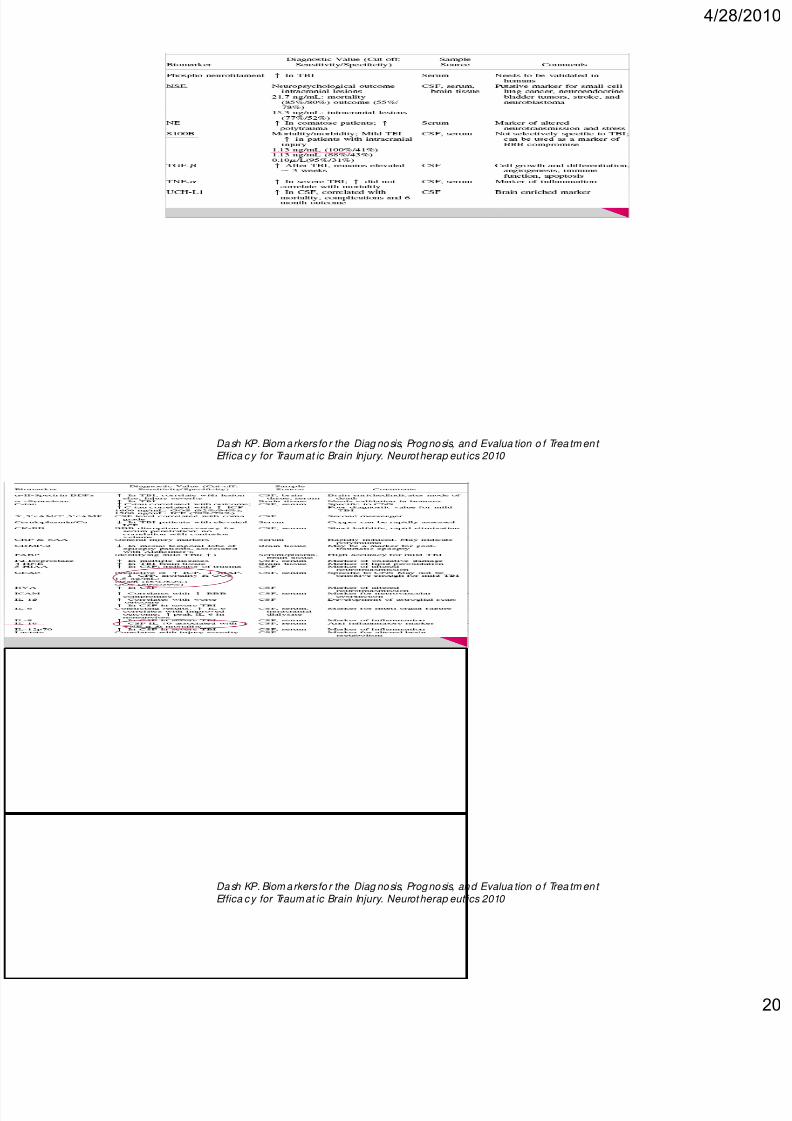
Dash KP. Biom arkers fo r the Diag nosis, Prognosis, and Evalua tion o f Trea tm ent Effica c y for Traumat ic Brain Injury. Neurotherap eut ics 2010
Dash KP. Biom arkers fo r the Diag nosis, Prognosis, and Evalua tion o f Trea tm ent Effica c y for Traumat ic Brain Injury. Neurotherap eut ics 2010
8/8/2019 TBI Children
http://slidepdf.com/reader/full/tbi-children 21/21
4/28/
Secondary prophylaxis: secondary injury
More study since 2003 guidelines
Need more pediatric study
Recommended