
So You Want Universal Health
Care, Eh?
James E Calvin Jr MD MBA FRCPC FACC FACP
Chair Chief of Medicine
Western University
for

Goals
• Describe what it is like to work in a Canadian Health Care System (Ontario) in a relatable way
• Describe its principles
• Describe briefly how it is managed (COVID)
• Describe the good, bad and the ugly as I See IT
• Suggest what changes might be necessary to make such a system work in the US
This Photo by Unknown Author is licensed under CC

My Story
• American born
• Canadian educated
• Canadian and US trained
• Worked in Canada 8 y (CCU Director, Research Scholar)
• Moved to US in 1991(CCU Director, Associate Professor)
• Chair of Cardiology at CCH ’98-’01
• Cardiology Chief at RUMC ’02-’12
• Professor and Chair/Chief, Medicine, U.W.O, 2013-
• CMO and Exec VP, 2018
• President CAPM 2017-2019

People: Why We Act Like
CanadiansPeace, Order and Strong Government
“In Canada you are reminded of the government every day. It parades itself before you. It is not content to be the servant, but will be the master.”
Henry David Thoreau , 1866
Once a Loyalist
“Historically, a Canadian is an American who rejects the revolution”
Northrup Frye , 1953
An Important Difference
Egalitarianism vs Pursuit of Happiness
Pierre Berton, “Why We Act Like Canadians”

Principles of the Canada Health Act
(Federal Government)
• Public Administration – Macro-managed (seems like)
• Comprehensiveness ***
• Universality ****
• Portability ****
• Accessibility **


In Ontario,
the Health Plan (OHIP) Covers:
• Visits to doctors
• Hospital visits and stays
• Hospitalized procedures including abortions
• Eligible dental surgery in hospital
• Eligible optometry
• Podiatry
• Ambulance services
• Travel for health services

Ministry of Health &
Long- Term Care• Wait Times
• Adult CT 72% done within prescribed time
• Expected wait time of 28 d occurs on the average of 37 d
• Expected wait time of 10 d occurs on the average of 16 d
• Breast Cancer Surgery• Target within 84 d occurs in
99%
• Target within 28 d occurs in 99%
• Target within 14 d occurs in 80 %
• Long-Term Care Capacity continues to be a big problem
• Perfect Storm• Increased Costs
• Technology
• Drug therapies
• Fixed or reduced hospital revenue
• Hospital payments based on volumes experienced 2 y before
• Volumes mandated• Do less, paid less
• Do more , cost is yours
• More complex patient mix• Older, more comorbidity

Perceived Differences: Universal Health Care vs. Multiple Insurer System
PROs
• Cheaper to run overall:
• Smaller administrative cost
• All are insured
• Macro management (less need to regulate and control)
• Freedom of choice for patient; autonomy for MD (incorporation)
• Doctors are paid well by the health plan not by the institution
CONs
• Funding too closely linked to economic health of country or province and to change of governments
• Rigid – single platform
• But too many stakeholders
• Limited research funding especially for salary support
• Academic institutions face large deficits

Canadian Health Care System:
OverviewMD Education
• Basically the same
• Tuition much cheaper in Canada
• Length of specialty training is similar; post-doc common (largely in NA)
Billing
• Canadian system is straightforward – both FFS and AFP
• Codes/documentation is simpler
• Billing Cycle is shorter
• Macro-managed – MOH pays on time; few denials, rules driven by government
Attitudes
• Public satisfaction falling
• MDs’ satisfaction is variable

Compensation for Physicians
• Fee for Service
• Alternate Funding Plan
• Repair for academic doctors
• Take home pay is good
• Incorporation• Corporate tax rate is low
• Tax credit for research
• Poor research salary support
• Department imposes tithe to support research and education
• This is independent of hospital funding

Ok! So Where is the Pay-off?
• Depends on perspective
• Medicine is the same
inside the box
• Constraints and mindset
are different
The Medicine I learned in
medical school, residency
and fellowship
Inside

Can We Make Money To Support The Academic
Mission : Yes, At The Physician Level
Plan for Use of the Funds
▪ DOM continues to generate a surplus; assuming this continues:
▪ Recruitment plan has been modeled to allow recruitment of researchers over the next 10 years providing minimum of 3 y of start up and secure salary support through to promotion so long as:
❖we ensure sufficient additional annual investment in the development fund. This amount is modeled annually
▪ Recruitment plan is flexible enough that in the event that financial circumstances change then the recruitment plans can be revised

Development Fund and Breakeven Analysis
-
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
2020 2021 2022 2023 2024 2025 2026 2027 2028
$$
Years
Development Fund Break-Even Point
Total Expenses
Development Fund (no profit)
Development Fund - AnnualProfit of $500K
Development Fund - AnnualProfit of $750K
Development Fund - AnnualProfit of $1 MM

So What About The System : Comparing
Universal Health Care Systems-You Might Not
Choose Canadian System


Health Care Problems Are
Usually Complex
• Large numbers of interacting elements
• Interactions are non-linear
• Systems are dynamic
• Systems have a history
• Agents and system constrain one another
• Hindsight does not correlate with foresight

Leadership Styles In Canada
• Model is primarily managerial
• Provinces follow the Federal rules
• Regions and hospitals do what the province mandates
• Physician colleges regulate physicians
• Strategic leadership/ visionary leadership is primarily at departmental or faculty level
• Movement towards salaried physicians would hinder innovation

Types of SystemsSimple
• Sense• Categorize• Respond
Complicated• Sense• Analyze• Respond
ComplexProbeSenseRespond
Chaotic• Act• Sense• Respond
Diagnose Problem
System 1
System 2
System 2

Response To Coronavirus-We
Thought We Were Pretty Good

Covid Cases-Wave 1-3, Outbreak
Wave 1: Supply Chain
Outbreak
Wave 2

Organization: When It Hits the FanLevel Role Status
Federal Government Supply Chain-PPE, VaccinesReporting, Modeling, border closing
We don’t manufacture vaccines. We depend on others. Thus, a very slow roll out
Provincial Government Patient movement/bed control(ICU)Restrict hospials to 85 % occupancyVaccine distributionLockdowns/Stay at home ordersICU beds
Supply chain sparse at the beginningThird wave has resulted in patients being transferred to other citiesSecond shots delayed in an attempt to get herd immunity
Ontario Health Team Regional coordination of Beds This is directed by a central command post
County Health Unit DirectivesDeclare outbreaksquarantines
Vaccination delivery
Very difficult to have two way conversation at the Department levelControlled cohorting within hospitals
Hospital Manpower-RN , AHP,cohortingInstitutional organizationBed and movement controlDrug acquisition
Bed expansion for third wave has created great strain
Portfolio/Program Day to day operations Relatively smooth organization of meetingsRedeployment of AHP
Department MD scheduling/ coverageTestingVaccination lists
Redeployment of physiciansManaging training programs

COVID-19 Case Status Access and Flow Bed Status Staff Status
Confirmed Cases (past 24hr) OccupancyAs of Midnight
Critical Care Beds AvailableCCIS as of 9am
Staff not available to
workAs of today
866
Staff returned to work
from March 18, 2020
1444Confirmed Admitted Cases Inpatient Ward Beds Available
As of Midnight
Number of staff sickAs of today
106
Staff home COVID-19
relatedAs of yesterday
760
ED Visits/RegistrationsAs of midnight
Staff Overtime Hours WorkedAs of 7am for prior day
Current validated # not available today.Bi-weekly results will be provided.
Staff Tested COVID-19 +As of 2:00 pm prior day
36 Total tested positive to date
23 of the total positive staff remain off work
Tests Pending Cases ED Admissions (Non COVID-19:COVID-19)
% of staff available to
work
91%
Staff redeployedAs of yesterday
382
ED admitted patients waitingAs of 7am
DAILY SNAPSHOT for April 27, 2020
WardCritical
Care
Lab conf’d tested
Deaths (New: Total to
Date)
27 11 335 0:14
N-COVID-19 COVID-19
Med Surg UH 67.3% aa%
Med Surg VH 64.3% aa%
Adult ICU UH 66.7% bb%
Adult ICU VH 60.0% bb%
Adult MH 59.1% cc%
Children’s Hospital
38.8% dd%
CH ICU 79.3% TBD
VH UH CH
142 97 47
VH UH CH
23:x 20:y 6:z
VH MH VH UH CH
0 2 0 0
As of 3pm As of 12amAs of 3pmAs of 3pm
11
16
0
5
6
0
UH Inpatient
VH Inpatient
CH Inpatient
UH Critical Care
VH Critical Care
CH Critical Care
16
2
0
0
15
3
UH Inpatient
UH Critical Care
CH Inpatient
CH Critical Care
VH Inpatient
VH Critical Care
154
4716
1145
Cardiac
Surgery
Oncology
Victoria Hospital
357
3433
102
Cardiac
Medicine
Epilepsy
University Hospital
742
C&A MH
Children's Hospital
941254
CSRUMSICUCCTCNICUPCCU
Daily Management-Early On

Covid Cases-Wave 1-3, Outbreak

Wave 3- Almost Out Of Control

Later
Occupancies went down to under 85 %
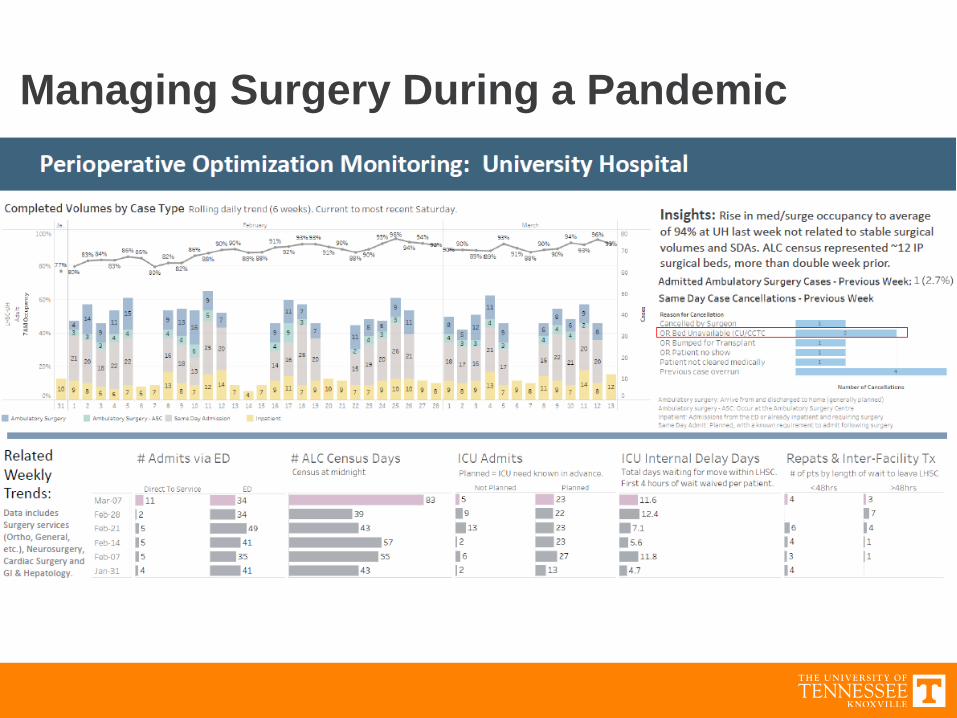
Managing Surgery During a Pandemic

Our Strategies For COVID
• Reduce Spread• PPE supply chain
• Staff/ Deployment
• Testing
• Vaccination
• Reduce surgery and ambulatory face to face
• Covid ambulatory care with remote monitoring
(over 1900 patients seen,~60 % need home monitoring)
• Bed Capacity Management• 85 % capacity- govt mandate
• Decrease elective surgery
• Regional approach/provincial and interprovincial
• Re-allocation
ImplicationsResident rotationsCancel examsCancel electivesWaiting lists/ ramp up$’s,$’s

COVID CHAOS
• Poor data- create data
• Inadequate supply chain – ration or find new suppliers
• Need to create capacity• Stop elective surgery sooner
• Transform ambulatory care to digital/electronic• Triage Covid+ from Covid- and uncertain cases
• ED to Cohort wards and teams
• Sufficient testing- this took way too much time.
• Aren’t vaccines supposed to protect? Sadie’s story
• Avoid Peter P.

Lessons Learned
• Don’t Get Cocky
• Supply Chain, Supply Chain, Supply Chain
• Faith in Vaccines needs to be guarded
• Control has to be balanced between front
line and centrally
• Politicians mean well but….

Six Aims for Quality Improvement
Health Care should be:
1. Safe
2. Effective
3. Patient Centered
4. Timely
5. Efficient
6. Equitable
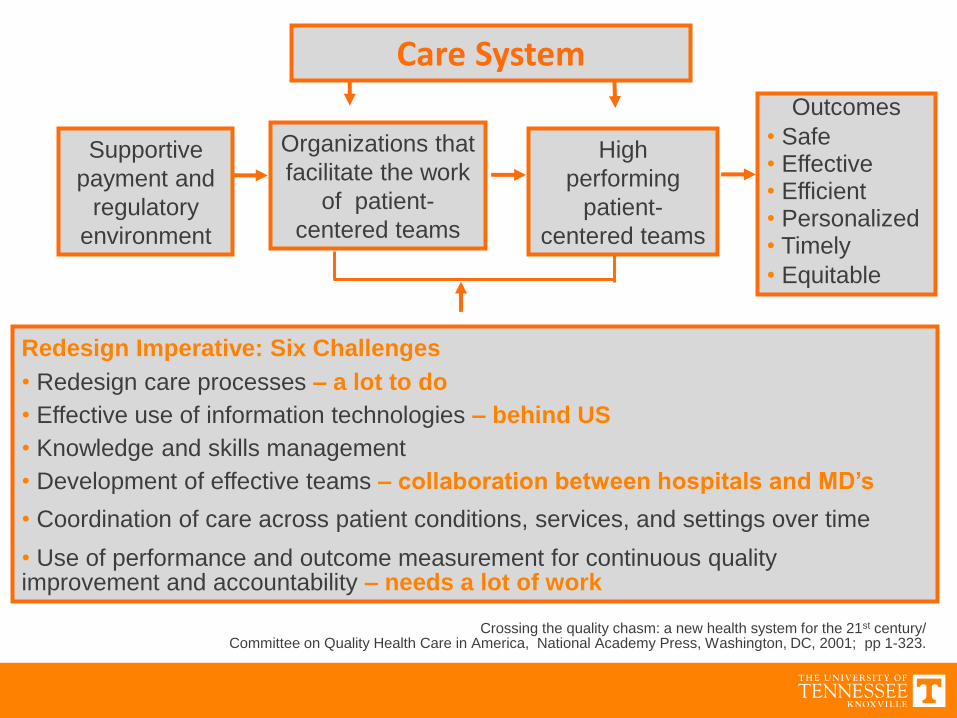
Outcomes
• Safe• Effective• Efficient• Personalized• Timely
• Equitable
Crossing the quality chasm: a new health system for the 21st century/Committee on Quality Health Care in America, National Academy Press, Washington, DC, 2001; pp 1-323.
Redesign Imperative: Six Challenges
• Redesign care processes – a lot to do
• Effective use of information technologies – behind US
• Knowledge and skills management
• Development of effective teams – collaboration between hospitals and MD’s
• Coordination of care across patient conditions, services, and settings over time
• Use of performance and outcome measurement for continuous quality improvement and accountability – needs a lot of work
Care System
Supportive
payment and
regulatory
environment
Organizations that
facilitate the work
of patient-
centered teams
High
performing
patient-
centered teams

Things To Make the Canadian
Health Care System Better
• Re-explore alignment of physicians with hospitals
• Enhance Dyadic leadership models- Needs to be a full partnership
• Improve financing of System User fees
Private tier
• Invest in Health Service Research to set appropriate standard of
care that is patient centered
• Monitor and reward true quality
• Enhance system’s flexibility, ingenuity, and innovation
• Invest (including private sector) in better systems of care

How To Make A Canadian-Style Health
Care System Palatable To Americans?
1. Emphasize patient’s freedom of choice of physician
2. Emphasize portability of care
3. Transfer present administrative cost savings into enhancing
existing services and reducing variations in care(need data)
4. Administer by states through regional, county councils
5. De-emphasize control by political parties and politicians.
6. Maintain some degree of privatization to support innovation, capital
expansion and infrastructure maintenance and upgrading
7. Control costs including drugs and technology, reduce waste
8. Ensure timely best practices by providers
9. Be selective about scope of services provided by the system
10. Create large Networks to support innovation and capital expansion

End of Presentation
So You Want Universal Health Care, Eh?James E Calvin Jr MD MBA
FRCPC FACC FACP
Questions?
Recommended

















