Sample Case Presentation
Agatha Stanek
January 26, 2010

Case presentation
•5 year- old girl brought to paediatric clinic by her mother who says the patient is tired, sleeps more than usual, and has a very low appetite
•Unexplained bruises on arms and legs.
•Afebrile at home but patient’s skin is very pale, warm and dry

Presentation continued
•Child is alert but ill-appearing
•Height and weight are normal for a 5- year old
•No redness in throat
•Child admits to some tenderness in abdominal area
•Child not involved in any competitive sports

Patient History
Medical Hx
•Patient was a full- term infant from uncomplicated pregnancy and delivery
•All immunizations are current
•Only previous childhood disease- measles at age 2 years
•Mother reports child’s fatigue and other symptoms having steadily worsened in the past week

Family Hx
•Patient lives with parents and one older brother (healthy)
•Grandmother died at age 62 from gastric cancer.
•Patient not exposed to any form of radiation or chemicals
Social Hx
•Patient lives with family in urban area in proximity to heavily occupied roads
•Developmental milestones are up to par
Occupational Hx
•Patient goes to nearby elementary school and daycare 5 days a week

Physical ExamVS: Patient Normal range
Systolic BP= 109 mm (94-109 mm)Diastolic BP= 67 mm (56-69 mm)HR= 130/min (70-115/min awake)RR= 20/min (17-27/min)T= 37° C 37° CHT= 41 inches (41-43 inches)WT= 37 lbs (40-50 lbs)
HEENT: Pupils equal at 3 mm, round, and reactive to light and accomodationPetechiae of mucous membranes
Neck: mild adenopathy; neck not tender
Cardiac: No murmurs
MS/Ext: no bone or joint pain elicited by palpation
Abd: No masses but liver and spleen enlarged

Differential Diagnosis?

Laboratory Test Results
Hb 7.1 g.dLHct 21%
AST 80 IU/LALT 103 IU/L
RBC 2.9 million/mm3
Total bilirubin 0.8 mg/dLTotal protein 6.9 g/dLAlb 3.5 g/dLCa 9.2 mg/dLPhos 4.0 mg/dLUric acid 4.3 mg/dLPT 13.0 secPTT 25.0 secGlucose, fasting 90 mg/dL
WBC 12, 800/mm3 •Neutrophils 59%•Lymphocytes 26%•Monocytes 3%•Eosinophils 1%•Basophils 1%•Blasts 10%
Plt 28, 000/mm3

Additional Tests
Lumbar Puncture•Spinal fluid clear, colourless•Opening pressure 90 mg/dL•Glucose 50 mg/ dL•Total protein 18 mg/dL•No blasts present
Bone Marrow Aspirate•93% blasts, 3% erythroblasts, 4% all other cells•(-) for TEL-AML 1 fusion gene
Chest X-Ray•Normal with no mediastinal mass
Immunology•(+) for cytoplasmic µ heavy-chain proteins

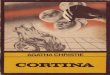
Peripheral Blood Smear Results
Rubin E, Farber JL. Pathology. 3rd Ed. Philadelphia: Lippincott Williams & Wilkins, 1999.)

Diagnosis!
Acute lymphoblastic leukemia
Why “acute”?
How does this vary from T cell acute lymphoblastic leukemia?
Diagnosis depends on detection of???
1- at least 2 surface immunoglobulins. ->CD 79-vs CD 3 in T cell ALL.
2-distinctive lymphoblast morphology ex: prominent vacuoles OR
3- expression of cytoplasmic immunoglobulin heavy-μchain proteins

Treatment
1- Remission and 2-induction therapy (peripheral blood count and bone marrow normalize) with....
Irradiated/ filtered platelets, packed RBCs, and allopurinol.
Chemotherapy: Involves use of 3-4 drugs
3- Consolidation: continue use of drugs but at higher doses
May require 2 or more years of continuiation therapy

Treatment of subclinical CNS leukemia
Intensive intrathecal (i.e., via spinal fluid) and systemic chemotherapy.
This strategy has produced excellent results with CNS relapse rates <2%.
Why is treatment important?
•Antibiotics?
•Peridex/ Biotine?

Possible complications of treatment
•Renal failure• sepsis• bleeding• thrombosis (i.e., intravascular blood clots)• encephalopathy (i.e., widespread degeneration of the brain)• seizures• secondary cancer (from therapy)• growth hormone deficiency, which can result in short stature• major cognitive defects

Prognosis/ Follow up
Good prognosis: absence of serious cytogenetic abnormalities a WBC count <30,000/cu mm, and complete remission within 4 weeks.
Poor prognosis: presence of serious cytogenetic abnormalities with a WBC count >100,000/cu mm, or failure to achieve complete remission within 4 weeks.
Prognosis is typically best for children ages 1–10.
Overall cure rate for ALL is currently 80- 85%.
Recommended