Role of Chemotherapy Role of Chemotherapy For Endometrial Carcinoma For Endometrial Carcinoma
Role of Chemotherapy Role of Chemotherapy For Endometrial Carcinoma For Endometrial Carcinoma
IGCS council, GCIG executive boardIGCS council, GCIG executive board
Sapporo Railway Hospital Sapporo Railway Hospital Vice-directorVice-director
Sapporo JapanSapporo Japan
IGCS council, GCIG executive boardIGCS council, GCIG executive board
Sapporo Railway Hospital Sapporo Railway Hospital Vice-directorVice-director
Sapporo JapanSapporo Japan
Satoru Sagae MD PhDSatoru Sagae MD PhDSatoru Sagae MD PhDSatoru Sagae MD PhD
IGCS 10,2006IGCS 10,2006IGCS 10,2006IGCS 10,2006

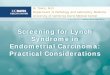
Endometrial Cancer - Treatment PlanEndometrial Cancer - Treatment PlanEndometrial Cancer - Treatment PlanEndometrial Cancer - Treatment Plan
Surgical Staging
Low Risk IA: G1-2
No treatment
Intermediate Risk IA: G3 IB, IC: G1-3 IIA, IIB: G1-3
Pelvic RT +/- cuff RT
High Risk/ Recurrent IIIA, IIIB, IIIC: G1-3 IVA, IVB: G1-3
Pelvic RT +/- cuff RT Aortic RT (+) ALN &/or Chemotherapy
< 5%*5-10%*
> 10%*IIIA + cytology
No treatment/Chemo/RT?
?**Recurrence risk

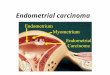
Up-to-date adjuvant therapy Up-to-date adjuvant therapy for endometrial cancerfor endometrial cancer
Up-to-date adjuvant therapy Up-to-date adjuvant therapy for endometrial cancerfor endometrial cancer
Radiation ( PRT ) or Chemotherapy
Radiation ( PRT ) or Chemotherapy
Surgical StagingSurgical Staging
Intermediate-riskIntermediate-risk
Low–riskLow–risk
Early stageEarly stage
Advanced stageAdvanced stage
IA/ IB , G1 / 2 IA/ IB , G1 / 2
Low? IA/ B G3 ,ICHigh? II, LVI (+) IIIa cytol(+) Ser., Clear
Low? IA/ B G3 ,ICHigh? II, LVI (+) IIIa cytol(+) Ser., Clear
III / IVA / BIII / IVA / B
RecurrenceRecurrence
Chemotherapy or Radiation
Chemotherapy or Radiation
Concurrent Chemo-Radiation
Concurrent Chemo-Radiation
High–riskHigh–risk
No treatment
Chemotherapy or Radiation
Chemotherapy or Radiation
→GOG 122
→GOG99→JGOG2033

Radiotherapy versus Observation in Radiotherapy versus Observation in early-stage endometrial cancerearly-stage endometrial cancer
Radiotherapy versus Observation in Radiotherapy versus Observation in early-stage endometrial cancerearly-stage endometrial cancer
NRHNRH PORTECPORTEC GOG 99GOG 99 **
Number of Patients
Local RecurrenceLocal Recurrence
Distant Metastasis
PFSPFS
OSOS
540 717 448
Obs >RTObs >RT
NS NS NS
NS NS NS NS NS NS
NS NS NS NS NS NS
Obs >RTObs >RT Obs >RTObs >RT
GOG99; high intermediate riskGOG99; high intermediate risk: : G2/G3, Lymph Vas Inv, Myomet Inv >2/3 G2/G3, Lymph Vas Inv, Myomet Inv >2/3
with 1) over 70 years old + 1 factor, 2) over 50 y.o. + 2 factors, 3) allwith 1) over 70 years old + 1 factor, 2) over 50 y.o. + 2 factors, 3) all 3 factors. 3 factors.

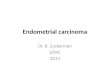
JGOG 2033JGOG 2033JGOG 2033JGOG 2033
- Endometrial ca.
-Hysterectomy + BSO ( complete resection )
- Myometrial inv. ≧ 1 / 2
Ran
do
mize
Regimen I
Regimen II
PelvicRadiation Therapy
CPA 333 mg / m2
Doxorubicin 40 mg / m2
CDDP 50 mg / m2
q 3 - 4 weeks, x 3 <
Phase III ( Phase III ( CAPCAP vs vs PRTPRT ) )
* 1994 to 2000 for 7 years 1994 to 2000 for 7 years 103 member institutions103 member institutions * Evaluable n=385
Sagae et al. ASCO 2005 abstr # 5002

JGOG 2033Patient Characteristics
JGOG 2033Patient Characteristics
RT (%) CAP (%)
Median ageMedian age 59 (37-85) 59 (32-75)
StageStage
ICIC 63.7 58.3
II AII A 5.2. 4.2
II BII B 5.2 13.0
III AIII A 14.5 11.5
III BIII B 0 0.5
III CIII C 11.4 12.5
Grade 1Grade 1 55.4 55.2
Grade 2Grade 2 27.5 33.3
Grade 3Grade 3 17.1 10.4Sagae et al. ASCO 2005 abstr # 5002

SUBGROUP ANALYSIS SUBGROUP ANALYSIS WITH NEW CRITERIA FOR INTERMEDIATE RISKWITH NEW CRITERIA FOR INTERMEDIATE RISK
SUBGROUP ANALYSIS SUBGROUP ANALYSIS WITH NEW CRITERIA FOR INTERMEDIATE RISKWITH NEW CRITERIA FOR INTERMEDIATE RISK
Low intermediate risk (LIR)
stage IC patients under 70 years of age and with G1/2 endometrioid adenocarcinoma
High intermediate risk (HIR)
(1) stage IC patients over age 70 years or having G3 endometrioid adenocarcinoma
(2) stage II or IIIA (positive cytology) patients with deeper than 50% myometrial invasion in the corpu
s. Sagae et al. ASCO 2005 abstr # 5002

SITES OF INITIAL RECURRENCESITES OF INITIAL RECURRENCE
Site* PRT (n=186) CAP (n=188)
No. of recurrent cases 28(15.1%) 31(16.5%)
Pelvis 10 5
Vagina only 1 7
Peritoneal Cavity 2 2
Liver 3 1
Lung 11 14
PAN LN 2 9
others 7 3
*Include multiple recurrences Sagae et al. ASCO 2005 abstr # 5002

JGOG 2033 CONCLUSIONSJGOG 2033 CONCLUSIONS
1. Both pelvic radiation therapy and chemotherapy were equally effective with 85% of 5 year survival
in all 374 pts with stage Ic (75%) through stage II, IIIc (25%).
2. In subgroup analysis, among 184 pts with low interm
ediate risk, the survival of both treatments was over 90% without any statistical significance.
3. However, among 119 pts with high intermediate risk, CAP arm significantly 15% improved PFS and OS when compared with PRT.
Sagae et al. ASCO 2005 abstr # 5002

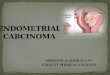
GOG 122GOG 122GOG 122GOG 122
- Endometrial ca.
- Surgical stage III / IV
- Hysterectomy + BSO
- PAN ( - )
- PAN ( + ) with negative scalene node and negative chest CT
Ran
do
mize
Regimen I
Regimen II
Whole AbdomenRadiation Therapy
Doxorubicin 60 mg / m2
CDDP 50 mg / m2
q 4 weeks
Phase III ( Phase III ( AP AP vs vs WAI WAI ))
Randall ME, et al. J Clin Oncol 24:36,2006Randall ME, et al. J Clin Oncol 24:36,2006

Randall ME, et al. J Clin Oncol 24:36,2006Randall ME, et al. J Clin Oncol 24:36,2006

GOG #122GOG #122
• Adjuvant chemotherapy appears to benefit all substages and histologic subtypes of stage III disease (not analyzed by grade)
• Hazard ratio for death with chemotherapy for all stage III disease combined is 0.68
• 5 year PFS for stage III disease is 50%-60%
• 5 year OS for stage III disease is 55%-65%
• 35% of recurrences on chemotherapy arm were initially limited to the pelvis
Randall ME, et al. J Clin Oncol 24:36,2006Randall ME, et al. J Clin Oncol 24:36,2006

Effects of Single agentEffects of Single agentEffects of Single agentEffects of Single agentAgent
Doxorubicin ( ADM )Doxorubicin ( ADM )EpirubicinPirarubicin
CyclophosphamideIfosphamide
Response rate (%)
CisplatinCarboplatin
VincristineVinblastine
Etoposide (oral )Medroxyprogesterone acetateTamoxifen
372610
18 8
20241415
142510

Effects ofEffects of ADMADM - - base therapybase therapyEffects ofEffects of ADMADM - - base therapybase therapy
Regimen Mean response rate ( range )
ADM ADM + CPA+ CPACPA 500 mg/m2 + ADM 60 mg/m2
ADM ADM ++ CDDPCDDPCDDP 50-60 mg/m2 + ADM 50-60 mg/m2
ADMADM + CPA + + CPA + CDDPCDDPCDDP 50-60 mg/m2 + ADM 40-50 mg/m2
+ CPA 400-600 mg/m2
39% ( 31 - 46% )39% ( 31 - 46% )
58% ( 33 - 81% )58% ( 33 - 81% )
46% ( 26 - 56% )46% ( 26 - 56% )

Chemotherapy for Endometrial cancerChemotherapy for Endometrial cancerChemotherapy for Endometrial cancerChemotherapy for Endometrial cancer
ADM
AP
GOG 107GOG 107CA
RR.PFSRR.PFSNSNS
EORTCEORTC5587255872
GOG 48GOG 48
Standard regimen = ADM + CDDPStandard regimen = ADM + CDDP
ATNSNS
GOG 163GOG 163

ADMADM + CDDP + CDDP vsvs ADMADM + TXL+ TXL + CDDP + CDDPADMADM + CDDP + CDDP vsvs ADMADM + TXL+ TXL + CDDP + CDDP
- Endometrial ca.
- Stage III / IV or Recurrent disease
- Measurable disease
- No prior cytotoxic chemotherapy
Ran
do
mize
Regimen I
Regimen II
Doxorubicin 60 mg / m2
CDDP 50 mg / m2
G-CSF
Doxorubicin 45 mg / m2
CDDP 50 mg / m2
Paclitaxel 160 mg / m2
G-CSF
GOG 177GOG 177Phase III studyPhase III study
q3 weeksx 7
q3 weeksx 7

Results of GOG 177Results of GOG 177Results of GOG 177Results of GOG 177
Regimen CR (%) OR (%) Alive without PD (%)
6.8 33.3 8.3
21.6 * 56.7 * 23.9 *
AAPP
TTAAPP
Treatment may have contributed to the death of 5 patients onthe TAP regimen. Treatment and disease may have contributed to the death of 5 patients on the TAP regimen. * p < 0.05

Chemotherapy for Endometrial cancerChemotherapy for Endometrial cancerChemotherapy for Endometrial cancerChemotherapy for Endometrial cancer
ADM
AP
GOG 107GOG 107CA
EORTCEORTC5587255872
GOG 48GOG 48
AT
GOG 163GOG 163
TTAAPPGOG 177GOG 177 Toxic !Toxic !

GOG 209GOG 209GOG 209GOG 209
- Endometrial ca.
- Surgical stage III / IV or Recurrent
- Measurable disease
- ER, PR status
Ran
do
mize
Regimen IRegimen I
Regimen IIRegimen II
Doxorubicin 45 mg / m2
CDDP 50 mg / m2
day 1Paclitaxel 160 mg / mPaclitaxel 160 mg / m22
day 2G-CSF
Paclitaxel 175 mg / mPaclitaxel 175 mg / m22 CBDCA AUC = 6 day 1
TTAAP P vs vs TTCCPhase III study Phase III study
Ongoing with GOG Japan (JGOG)

Japanese Phase II studiesJapanese Phase II studiesJapanese Phase II studiesJapanese Phase II studies
- Advance, Recurrent- Advance, Recurrent Endometrial cancer Endometrial cancer
- 23 Pts.- 23 Pts.
- Advance, Recurrent- Advance, Recurrent Endometrial cancer Endometrial cancer
- 32 Pts.- 32 Pts.
Paclitaxel ( Taxol )Paclitaxel ( Taxol ) 210 mg / m210 mg / m22
q 3 weeksq 3 weeks
Docetaxel ( Taxotere )Docetaxel ( Taxotere ) 70 mg / m70 mg / m22
q 4 weeksq 4 weeks
RR = 30.4 %RR = 30.4 %
RR = 31.3 %RR = 31.3 %
- Prior CT or RT- Prior CT or RT
- Prior CT or RT- Prior CT or RT
Hirai et al. Gynecol Oncol 94;471,2004Hirai et al. Gynecol Oncol 94;471,2004
Katsumata et al. Br J Cancer 93;999,2005Katsumata et al. Br J Cancer 93;999,2005

Option of Taxanes / PlatinumOption of Taxanes / PlatinumOption of Taxanes / PlatinumOption of Taxanes / Platinum
Docetaxel Docetaxel
Paclitaxel Paclitaxel
CBDCACBDCA
CDDPCDDP
Taxanes Taxanes Platinum Platinum
SCOTROC, SGCTC, OV-10, GOG 111, SCOTROC, SGCTC, OV-10, GOG 111, AGO, GOG 158, JGOG 3016, AGO, GOG 158, JGOG 3016, JGOG P II study 2041, JGOG P III study 2043 JGOG P II study 2041, JGOG P III study 2043

JGOG 2041JGOG 2041JGOG 2041JGOG 2041
Randomized phase IIRandomized phase II
- Advance, recurrent endometrial cancer
- Measurable disease
- Prior CT, RTR
and
om
ize
Arm 1 : DPArm 1 : DP
Docetaxel 70 mg/mDocetaxel 70 mg/m22
CDDP 60 mg/m2
Arm 2 : DCArm 2 : DC
Arm 3 : TCArm 3 : TC
Docetaxel 60 mg/mDocetaxel 60 mg/m22
CBDCA AUC = 6
Paclitaxel 180 mg/mPaclitaxel 180 mg/m22
CBDCA AUC = 6Total 90 PtsClosed 2004

JGOG 2041 monitoring reportJGOG 2041 monitoring report(Oct, 2006)(Oct, 2006)
JGOG 2041 monitoring reportJGOG 2041 monitoring report(Oct, 2006)(Oct, 2006)
AE(>G3) DP (n=24) DC (n=30) TC (n=28)AE(>G3) DP (n=24) DC (n=30) TC (n=28)
GIGI 20.820.8 3.3 0.0 3.3 0.0 Neuro Neuro 0 0 0 0 7.17.1Hb Hb 8.3 8.3 31.0 28.631.0 28.6WBC 75.0 89.7 82.1 WBC 75.0 89.7 82.1 Neutro 83.3 89.7 82.1Neutro 83.3 89.7 82.1Platelet 4.2 Platelet 4.2 10.3 25.010.3 25.0
RR 51.7% 48.3% 60.0%
95%CI 32.5-70.6% 29.5-67.5% 40.6-77.3%

New RCT Phase III JGOG2043New RCT Phase III JGOG2043New RCT Phase III JGOG2043New RCT Phase III JGOG2043
Randomized Randomized comparative phase IIIcomparative phase III
- Intermediate risk I/II- Advanced III/IV- Adjuvant- First-line chemo.
-Primary endpoint-PFS
-Secondary endpoint-OS, AE, Tx, LN
- About 600 patients
Ran
do
mize
Arm 1 : APArm 1 : AP
Doxorubicin 60 mg/m 60 mg/m22
CDDP 50 mg/m2
Arm 2 : DPArm 2 : DP DOC 70 mg/mDOC 70 mg/m22
CDDP 60 mg/mCDDP 60 mg/m22
Arm 3 : TCArm 3 : TC
Paclitaxel 180 mg/mPaclitaxel 180 mg/m22
CBDCA AUC = 6

Future direction of Future direction of Adjuvant ChemotherapyAdjuvant Chemotherapy
Future direction of Future direction of Adjuvant ChemotherapyAdjuvant Chemotherapy
AP
TC
AP or AT
GOG163GOG163
TAP
GOG 209GOG 209
Taxane Taxane AnthracyclineAnthracycline PlatinumPlatinum
JGOG PIIIJGOG PIII20432043
GOG 177GOG 177
DDPP? ? ? ?
? ?

Biologic Therapies in Clinical TrialsBiologic Therapies in Clinical TrialsBiologic Therapies in Clinical TrialsBiologic Therapies in Clinical Trials
• PTEN/MMAC-1PTEN/MMAC-1
– 43% endometrial cancers
– Loss of function increases AKT, increase mTOR
– mTOR: Iº-70%, Rec-50%
• EGF-R EGF-R
over expressed in 60-80% over expressed in 60-80% (UPSC)(UPSC)
• mTOR inhibitorsmTOR inhibitors
– RAD001
– CCI-779 (NCIC)
(5/16 PR, 31%, Oza)
• EGF-R Targeted therapyEGF-R Targeted therapy– Gefitinib (GOG 229-C)
– Trastuzumab ( GOG 181b)
– Erlotinib, OSI-774 (NCIC)
7% response rate

ConclusionsConclusions
1.Chemotherapy may be an alternative modality with radiation therapy for high intermediate-risk and high-risk endometrial cancer.
2. Optimal chemotherapeutic agents are
AP, TAP, TC and others with current investigations.
3. Biologics as Future directions are including with
Gefitinib, Trastuzumab, Erlotinib, CCI-779 and others.

Endometrial Cancer State of the Science MeetingEndometrial Cancer State of the Science MeetingNCRI,UK NCI-US GCIGNCRI,UK NCI-US GCIG
Manchester, UK Manchester, UK November 28-29,2006November 28-29,2006
Endometrial Cancer State of the Science MeetingEndometrial Cancer State of the Science MeetingNCRI,UK NCI-US GCIGNCRI,UK NCI-US GCIG
Manchester, UK Manchester, UK November 28-29,2006November 28-29,2006
Review of molecular biologyRole of surgery, radiotherapy, chemotherapy, e
ndocrine therapy, biologic therapyPotential trials in early stage diseasePotential trials in advanced or recurrent disease Potential trials in clear cell and papillary serous
histologies Potential translational research
Recommended