Embed Size (px)
Citation preview

Endometrial carcinoma
Dr. B. ZuckermanSZMC2014

Endometrial Carcinoma in US (2011)
• The most common gynecological malignancy• 46,470 new cases• 8,120 deaths• Median age of diagnosis: 61 (most – 50-60 )• 90% - over the age 50• 20% - before menopause• 5% - before age 40
Siegel R, Ward E, Brawley O, Jemal A. CA Cancer J Clin. 2011;61:212-36

Endometrial Carcinoma
• 90% experiencing abnormal uterine bleeding
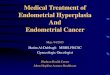
• 75% - early stage disease
• Stage 1 – 72% Stage 2 – 12% Stage 3 – 13% Stage 4 – 3%
Stage
St 1St 2St 3St 4

Endometrial Carcinoma
• Early onset of symptoms• Well-established diagnostic guidelines• Overall – good prognosis
• High-risk or advanced disease – poor prognosis and death

Malignancies of uterine body: Classification
• Epithelial – 90% Endometrioid, serous,
clear cell, mucinous• Mesenchymal – 5% Endometrial stromal
sarcoma, leiomyosarcoma, other sarcomas
• Mixed – 3% Carcinosarcoma,
adenosarcoma• Secondary – 2%
Uterine malignancies

Carcinoma of endometrium

Types of endometrial carcinoma

Epidemiological risk factors
• Chronic estrogenic stimulation• Associated medical illness• Demographic characteristics

Chronic estrogenic stimulation
Relative risk Factors
2-12 Estrogen replacement (no progestin)
1.6-4.0 Early menarche / Late menopause
2-3 Nulliparity
ND Anovulation
ND Estrogen-producing tumors

Associated medical illness
Relative risk Factors
3 Diabetes mellitus
2-4 Obesity
1.5 Hypertension
3.7 Gallbladder disease
8 Prior pelvic radiotherapy

Demographic characteristics
Relative risk Factors
4-8 Increasing age
2 White race
1.3 High socioeconomic status
2-3 European/North American country
2 Family history of endometrial cancer

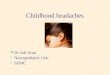
Precursors of endometrial carcinoma
Simple hyperplasia
Increased number of glands but regular glandular architecture

Precursors of endometrial carcinoma
Complex hyperplasia without atypia
Crowded irregular glands. Cytological atypia is absent

Precursors of endometrial carcinoma
Simple atypical hyperplasia
Simple hyperplasia with presence of cytological atypia (prominent nucleoli and nuclear pleomorphism)

Precursors of endometrial carcinoma
Complex atypical hyperplasia
The endometrial glands are irregular in size and shape with branching and outpouchings (complex hyperplasia) with cytological atypia

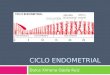
Precursors of endometrial carcinomaFoci of well-differentiated endometrioid adenocarcinoma
Areas of complex atypical hyperplasia

Precursors of endometrial carcinoma
Malpica, Deavers, and Euscher. Biopsy interpretation of the uterine cervix and corpus. Lippincott, William & Wilkins, p. 167-168, 2010

Hereditary Syndromes
• Endometrial cancer is not typically a hereditary disorder
• Genetic predisposition is seen in up to 10% of patients (5% women with Lynch syndrome)

Lynch syndrome
• Hereditary non-polyposis colorectal cancer (HNPCC)• Autosomal dominant inherited cancer susceptibility
syndrome

Lynch syndrome
• Germ line mutation in one of the DNA mismatch repair genes (MSH2, MLH1, MSH6, PMS2)
• Early age at cancer diagnosis and the development of multiple cancer types, particularly colon and endometrial cancers
• 40% to 60% risk of endometrial cancer

Cellular classification
Endometrioid type 80%• G1 Well differentiated• G2 Moderately differentiated• G3 Poorly differentiated• Other
Non-endometrioid type (G3) 20%
• Papillary serous <10%• Clear cell 4%• Mucinous 1%• Squamous cell <1%• Mixed 10%• Undifferentiated

Natural history
Primary sign: abnormal bleeding

Natural history
Myometrial invasion

Natural history
Lymph vascular invasion

Natural history Lymph none metastases

Staging
Surgical

Stage 1
IB: Invasion >= ½ of the myometrium
IA: No or < ½ myometrial invasion

Stage 2
II: Invasion of cervical stroma, but does not extend beyond the uterus.

Stage 3
IIIC: Cancer has spread to lymph nodes in the pelvis - IIIC1 and/or around the aorta - IIIC2
IIIB: Cancer has spread to the vagina and/or to the parametrium
IIIA: Cancer has spread to the outer layer of the uterus and/or to the fallopian tubes, ovaries, or ligaments of the uterus

Stage 4
IVA: Cancer has spread into the bladder and/or bowel
IVB: Cancer has spread beyond the pelvis to other parts of the body

Diagnosis: endometrial biopsy
• Abnormal uterine bleeding (older than 40)• Atypical glandular cells in PAP (older than 35)

Ultrasound
96% of bleeding postmenopausal women with cancer have endometrial thickness greater than 5 mm

US triage patients with PMB

Hysteroscopy
Indication: symptoms of AUB continue and cannot by explained by the office biopsy

Preoperative evaluation
Type I tumors• Physical examination• Chest radiograph• Electrocardiogram
Type II tumors• CT or MRI (CT scan imaging changed
treatment in 11%)
• Serum CA 125 (may be a predictor of
extrauterine disease)

Comprehensive surgical staging • Hysterectomy• Bilateral salpingo-oophorectomy• Pelvic and para-aortic lymphadenectomy

Surgical staging controversy Proponents
• Full staging should be performed on all patients regardless of tumor grade or depth of invasion
Opponents • No staging in clinical early
stage disease: low likelihood of lymph
node metastases and the risks of a lymphadenectomy outweigh the potential benefits of having the information gained from staging
A third group: surgical staging is indicated in a select group of women at highest risk for extrauterine disease; however, the precise definition of a high-risk patient remains elusive

Italian trial
• 514 patients, 31 centers in two countries, 10-year period
• Both early and late postoperative complications occurred more frequently in patients who had undergone a pelvic lymphadenectomy
• The 5-year disease-free and overall survival rates were similar between the two groups (81% and 86%)
Systematic pelvic lymphadenectomy vs. no lymphadenectomy in early-stage endometrial carcinoma: randomized clinical trial. Panici PB, Stefano S, Maneschi F, et al. J Natl Cancer Inst 2008;100:1707.
Surgical staging controversy: RCT

ASTEC (A Study in the Treatment of Endometrial Cancer)
• Objective: to determine if lymphadenectomy increases survival independent of adjuvant irradiation
• 1,408 women, 85 centres, 4 countries, over 7 years
Efficacy of systematic pelvic lymphadenectomy in endometrial cancer (MRC ASTEC trial): a randomized study. The writing committee on behalf of the ASTEC study group. Lancet 2009;373:125.
Surgical staging controversy: RCT

ASTEC (A Study in the Treatment of Endometrial Cancer)
• 1st randomization: standard surgery vs. standard surgery plus lymphadenectomy
• 2nd randomization in intermediate and high-risk group (IA or IB with high-grade pathology, or IIA): radiation vs. no further therapy
• no evidence of a benefit in terms of overall survival or recurrence-free survival for pelvic lymphadenectomy in women with early endometrial cancer

Retrospective data
• The outcomes of 27,063 women with unstaged endometrioid uterine cancer.
• From Surveillance, Epidemiology and End Results (SEER) database
• 39,396 patients• Surgical staging procedures that included a
lymphadenectomy vs. no lymphadenectomy
Chan JK, Wu H, Cheung MK, et al. Gynecol Oncol 2007;106:282.
Surgical staging controversy

Retrospective data
• In stage I grade 3 patients, those who underwent lymphadenectomy had a better 5-year disease-specific survival than those without lymphadenectomy
• no benefit for lymphadenectomy was seen for patients with stage I grade 1 and grade 2

Additional studies are needed to determine the role of lymphadenectomy, the extent of lymphadenectomy, and the indications for surgical staging in patients with endometrial cancer
Surgical staging controversy

Lymphatic mapping and sentinel lymph node biopsy
• Alternative to complete pelvic and para-aortic lymphadenectomies
• Endometrial cancer tumors: difficult to visualize and to inject

Lymphatic mapping and sentinel lymph node biopsy
• In a prospective multicentre study (SENTI-ENDO) of sentinel lymph node biopsy via cervical injection, pelvic sentinel lymph nodes (SLNs) were detected in 89% of patients; and the sensitivity and negative predictive value of SLN biopsy were 84% and 97%, respectively.
Ballester M, Dubernard G, Lécuru F, et al. Lancet Oncol 2011;12:469-76

Surgical Approaches
• Surgery represents the cornerstone for treatment of endometrial cancer
• Standard approach: exploratory laparotomy, hysterectomy and bilateral salpingo-oophorectomy
• Comorbidity: severe obesity, diabetes mellitus, cardiovascular diseases

Surgical Approaches
• Minimizing surgical morbidity: minimally invasive surgery (Laparoscopic surgery, robotic-assisted surgery )
• Less blood loss, decreased transfusion rates, shorter length of hospitalization, and a faster return to daily activities

GOG trial: laparotomy vs. laparoscopy
• Laparoscopic surgical staging for uterine cancer is feasible and safe in terms of short-term outcomes (2010)
• Fewer complications and shorter hospital stays• Potential for a small increased risk of cancer
recurrence with laparoscopy versus laparotomy• 5-year overall survival being almost identical in both
arms at 89.8% (2012)
Walker JL, Piedmonte MR, Spirtos NM, et al. J Clin Oncol 2012;30:695-700

Robotics
• In 2005 the U.S. FDA approved the daVinci robotic system for gynecologic procedures
• The advantages of the robotic system over standard laparoscopy: high-definition three-dimensional vision, more surgical precision and dexterity, improved ergonomics for the surgeon, improved teaching capabilities for trainees
• The disadvantage: very high cost

Robotics
To date, there are no prospective trials comparing laparotomy vs. laparoscopy vs. robotic surgery in the management of patients with endometrial cancer

Uterine risk factors
Major prognostic factors
• Grade or cell type• Depth of myometrial invasion• Tumor extension to the cervix Less important
• Extent of uterine cavity involvement• Lymph–vascular space invasion• Tumor vascularity

Extrauterine risk factors
• Adnexal metastases• Pelvic or para-aortic lymph node spread• Peritoneal implant metastases• Distant organ metastases• Positive peritoneal cytology

Radiation Therapy
• Today it is delivered almost exclusively following surgery in women with adverse pathologic features
• External beam approach is whole pelvic radiotherapy• Brachytherapy

Adjuvant Radiation Therapy
• Reduces the risk of pelvic recurrence in early stage patients with adverse pathologic features
• Does not improve survival
Adjuvant external beam radiotherapy in the treatment of endometrial cancer (MRC ASTEC and NCIC CTG EN.5 randomized trials): pooled trial results, systematic review and meta-analysis. ASTEC/EN.5 Study Group, Blake P, Swart AM, et al. Lancet 2009;373:137

Adjuvant brachytherapy alone
• Brachytherapy vs. pelvic radiotherapy: no differences in overall or disease-free survival
• Less toxicity
Vaginal brachytherapy versus pelvic external beam radiotherapy for patients with endometrial cancer of high-intermediate risk (PORTEC-2): an open-label, non-inferiority randomised trial. Nout RA, Smit VT, Putter H, et al. Lancet 2010;375:816
Quality of life after pelvic radiotherapy or vaginal brachytherapy for endometrial cancer: first results of the randomized PORTEC-2 trial. Nout RA, Putter H, Jurgenliemk-Schulz IM, et al. J Clin Oncol 2009;27:3547

Adjuvant chemotherapy in early stage disease
• Pelvic radiotherapy versus chemotherapy (cyclophosphamide, doxorubicin, and cisplatin [CAP])
• No differences in progression-free or overall survivals were seen at 5 years
Randomized phase III trial of pelvic radiotherapy versus cisplatin-based combined chemotherapy in patients with intermediate and high-risk endometrial cancer: a Japanese Gynecologic Oncology Group study. Susumu N, Sagae S, Udagawa Y, et al. Gynecol Oncol 2008;108:226

Hormone (Progesterone) Therapy
• Complex atypical hyperplasia and low-grade endometrial cancers diagnosed in young women who are still considering child-bearing
• Very high risk surgery group