R
R
Bip
CV
a
b
c
d
e
RA
h0B
ev Bras Anestesiol. 2017;67(1):72---84
REVISTABRASILEIRA DEANESTESIOLOGIA Publicação Oficial da Sociedade Brasileira de Anestesiologia
www.sba.com.br
EVIEW ARTICLE
enefit of general anesthesia monitored by bispectralndex compared with monitoring guided only by clinicalarameters. Systematic review and meta-analysis
arlos Rogério Degrandi Oliveiraa,b,∗, Wanderley Marques Bernardoc,d,e,ictor Moisés Nunesd
Hospital Guilherme Alvaro, Departamento de Anestesiologia, Santos, SP, BrazilHospital Ana Costa, Departamento de Anestesiologia, Santos, SP, BrazilUniversidade de São Paulo, Faculdade de Medicina, Medicina Baseada em Evidência, São Paulo, SP, BrazilCentro Universitário Lusíada, Faculdade de Medicina de Santos, Santos, SP, BrazilPrograma Diretrizes da Associacão Médica Brasileira, Santos, SP, Brazil
eceived 14 July 2015; accepted 22 September 2015vailable online 14 April 2016
KEYWORDSGeneral anesthesia;Anesthetics;Inhalation;Intravenousanesthesia;Bispectralindex-monitoring
AbstractBackground: The bispectral index parameter is used to guide the titration of general anesthesia;however, many studies have shown conflicting results regarding the benefits of bispectral indexmonitoring. The objective of this systematic review with meta-analysis is to evaluate the clinicalimpact of monitoring with the bispectral index parameter.Methods: The search for evidence in scientific information sources was conducted duringDecember 2013 to January 2015, the following primary databases: Medline/PubMed, LILACS,Cochrane, CINAHL, Ovid, SCOPUS and TESES. The criteria for inclusion in the study were random-ized controlled trials, comparing general anesthesia monitored, with bispectral index parameterwith anesthesia guided solely by clinical parameters, and patients aged over 18 years. The crite-ria for exclusion were studies involving anesthesia or sedation for diagnostic procedures, andintraoperative wake-up test for surgery of the spine.Results: The use of monitoring with the bispectral index has shown benefits reducing timeto extubation, orientation in time and place, and discharge from both the operating roomand post anesthetic care unit. The risk of nausea and vomiting after surgery was reduced by
12% in patients monitored with bispectral index. Occurred a reduction of 3% in the risk ofcognitive impairment postoperatively at 3 months postoperatively and 6% reduction in the riskpatients monitored with bispectral index. Furthermore, the risk of been reduced by 1%.
of postoperative delirium inintraoperative memory has
∗ Corresponding author.E-mail: [email protected] (C.R. Oliveira).
ttp://dx.doi.org/10.1016/j.bjane.2015.09.001104-0014/© 2016 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is an open access article under the CCY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

Benefit of general anesthesia monitored by bispectral index 73
Conclusion: Clinically, anesthesia monitoring with the BIS can be justified because it allowsadvantages from reducing the recovery time after waking, mainly by reducing the administrationof general anesthetics as well as the risk of adverse events.© 2016 Sociedade Brasileira de Anestesiologia. Published by Elsevier Editora Ltda. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVEAnestesia geral;Anestésicos;Inalacão;Anestesiaintravenosa;Monitoracão doíndice bispectral
Benefício da anestesia geral com monitoracão do índice bispectral em comparacãocom o monitoramento guiado apenas por parâmetros clínicos. Revisão sistemática emetanálise
ResumoJustificativa: O parâmetro índice bispectral (BIS) é usado para guiar a titulacão da anestesiageral; no entanto, muitos estudos têm mostrado resultados conflitantes quanto aos benefíciosda monitoracão do BIS. O objetivo desta revisão sistemática com meta-análise foi avaliar oimpacto clínico da monitoracão do parâmetro BIS.Métodos: A busca por evidências em fontes de informacão científicas foi conduzida de dezembrode 2013 a janeiro de 2015 nas seguintes bases de dados: Medline/PubMed, LILACS, Cochrane,CINAHL, Ovid, SCOPUS e TESES. Os critérios de inclusão foram estudos randomizados e controla-dos, comparando anestesia geral monitorada com o parâmetro BIS com anestesia guiada apenaspor parâmetros clínicos em pacientes com idade superior a 18 anos. Os critérios de exclusãoforam estudos que envolveram anestesia ou sedacão para procedimentos de diagnóstico e testede despertar no intraoperatório de cirurgia da coluna vertebral.Resultados: O uso de monitoracão com o BIS mostrou benefícios como a reducão do tempo deextubacão, orientacão no tempo e no espaco, alta da sala de cirurgia e da sala de recuperacãopós-anestesia. O risco de náuseas e vômitos no pós-operatório foi reduzido em 12% em pacientesmonitorados com o BIS. Ocorreu uma reducão de 3% no risco de disfuncão cognitiva em trêsmeses do pós-operatório e 6% no risco de delírio pós-operatório em pacientes monitorados como BIS. Além disso, o risco de despertar com memória intraoperatória foi reduzido em 1%.Conclusão: Clinicamente, a monitorizacão com o BIS pode ser justificada, pois permite van-tagens em reduzir o tempo de recuperacão, principalmente reduzindo a administracão deanestésicos gerais e o risco de eventos adversos.© 2016 Sociedade Brasileira de Anestesiologia. Publicado por Elsevier Editora Ltda. Este e umartigo Open Access sob uma licenca CC BY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
M
Tm(tlafIMmBnR
Introduction
Bispectral index (BIS) is a multiprocessor EEG parameterspecially developed to measure the effects of anestheticson the brain hypnotic state, making it possible to mea-sure the depth of anesthesia. The introduction of the BISin clinical practice is a reliable method to assess brainfunction and allows the titration of hypnotics on corticalactivity.
Due to anesthesia may occur unpredictable responses atdifferent times of surgery with a great variability amongpatients, so the exact dosage of anesthetic to be adminis-tered still remains a challenge. However, many studies haveshown conflicting results regarding the advantages of BISand if this monitoring improves recovery times and hospitaldischarges, as well as minimizes adverse events.
The objective of this systematic review with meta-analysis was to clinically evaluate the objective BISmonitoring parameter, compared with the clinical param-eters in general anesthesia.
CCPa
ethods
he research for evidence in scientific sources of infor-ation was performed by two independent reviewers
CRDO, WMB) during the period from December 2013o January 2015, the following primary databases: Med-ine/PubMed, LILACS, Cochrane, CINAHL, Ovid, SCOPUSnd THESES. The search strategy was made with theollowing words: (Anesthesia, General OR Anesthetics,nhalation OR Anesthetics, Intravenous) AND (Consciousnessonitors OR Monitoring, Intraoperative OR Bispectral index-onitoring technology OR Bispectral index-monitoring ORispectral index monitoring OR Drug Monitoring OR Aware-ess OR Monitoring, Physiologic OR BIS monitoring) ANDandom*.
The criteria for inclusion in the study were Randomized
ontrolled Trials (RCTs) with level of evidence 1B/2B (Oxfordentre for Evidence-based Medicine) in English, Spanish orortuguese languages, comparing venous or inhaled generalnesthetics monitored with BIS parameter with anesthesia
74
Table 1 Considered outcomes.
Time for spontaneous eye openingTime for eye opening upon verbal commandTime to tracheal extubationTime for orientation in time and placeTime for leaving operating roomTime for discharge from post anesthesia care unit (PACU)Time for hospital dischargePostoperative nausea and vomiting (PONV)Cognitive disorders in the postoperative period(1 week after extubation)Cognitive disorders in the postoperative period(3 months after extubation)
gy
siek
i
RVC
l
Maav
v5
iog
R
Ia1
eatac
s
tac
Postoperative deliriumIntraoperative memory
uided solely by clinical parameters; patients aged over 18ears.
The criteria for exclusion were studies involving anesthe-ia and sedation for diagnostic procedures. Studies involvingntraoperative wake-up test for surgery of the spine werexcluded. Nor were objects of study the clinical trials ofetamine as venous anesthetic.
This systematic review with meta-analysis was recordedn PROSPERO database under the number CRD42015017240.
The outcomes considered are described in Table 1.The results of the meta-analysis were obtained by the
evMan 5.2 software (Review Manager Computer program.
ersion 5.2 Copenhagen: The Nordic Cochrane Centre,ochrane Collaboration© 2014).Regarding meta-analysis, the difference was calcu-ated in risk difference for dichotomic variables with
rear
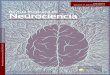
Records identified throughdatabase searching
(n=1744)
Ad
Records screened(n=1747)
Full-text articles assesfor eligibility
(n=53)
Studies included inqualitative synthesi
(n=17)
Studies included inquantitative synthes
(meta-analysis)(n=17)
Figure 1 Consolidated flow diagram
C.R. Oliveira et al.
antel---Haenszel (M-H) test with 95% Confidence Interval;nd in mean difference with fixed effect using Inverse Vari-nce (IV), with a 95% Confidence Interval, for continuousariables.
An I2 of 0% indicates no heterogeneity among studies,alues below 50% indicate a low heterogeneity, and above0%, high heterogeneity.
When the heterogeneity was greater than 50%, a sensitiv-ty analysis was performed, removing the studies that wereut of the ‘‘forest plot’’. To achieve reduction in hetero-eneity remained out of the study meta-analysis.
esults
nitially, the search resulted in 1.747 scientific articles. Afterpplying the inclusion and exclusion criteria were selected7 RCT (Fig. 1).
Table 2 shows the trials selected with the respective lev-ls of evidence, Jadad scale, number of patients randomizednd analyzed, patient numbers in the intervention and con-rol groups and PICO strategy. A total of 10,761 patients werenalyzed, 5668 in the intervention group and 5093 in theontrol group.
Table 3 shows the 36 full-text articles excluded with rea-ons.
The time for spontaneous eye opening is counted fromhe end of the last suture, when then inhaled or intravenousnesthetic is discontinued. The monitoring with the BIS,ompared exclusively with clinical parameters, showed a
eduction in the time for spontaneous opening 0.62 minye (95% CI −1.08, −0.16), with an I2 = 83%. In sensitivitynalysis, when removed the study Kreuer et al.7 wasemoved we have an I2 = 0%, with reduction of time forditional records identifiedthrough other sources
(n=3)
Records excluded(n=1694)
sed Full-text articles excluded,with reasons
(n=36)
s
is
(PRISMA Flow Diagram, 2009).

Benefit of general anesthesia monitored by bispectral index 75
Table 2 Selected randomized clinical trials (RCT).RCT EL J R/A I/C P I C ONelskylä et al.
(2001)12B 0 62/62 32/30 ASA I or II,
between 18 and 50years,gynecologicalsurgery.
BIS between 50and 60 years
‘‘Blinded’’monitor.Anesthesia wasadjusted accordingto clinicalparameters.
Time forspontaneous eyeopening,extubation,orientation in timeand place, hospitaldischarge andPONV.
Wong et al.(2002)2
1B 3 68/60 29/31 >60 years, ASAI---III, orthopedicsurgery.
BIS between 50and 60.
‘‘Blinded’’monitor.Anesthesia wasadjusted accordingto clinicalparameters.
Time forspontaneous eyeopening,orientation in timeand place andPACU discharge.
Luginbühlet al.(2003)3
2B 2 160/160 80/80 >18 years,gynecologicalsurgery.
BIS between 45and 55.
Anesthesia wasadjusted accordingto clinicalparameters.
Time to trachealextubation.
Ahmad et al.(2003)4
1B 3 99/97 49/48 >18 years,gynecologicalsurgery.
BIS between 50and 60.
Anesthesia wasadjusted accordingto clinicalparameters.
Time for hospitaldischarge.
Basar et al.(2003)5
2B 0 60/60 30/30 >18 years, ASA I orII, abdominalsurgery.
BIS between 40and 60.
‘‘Blinded’’monitor.Anesthesia wasadjusted accordingto clinicalparameters.
Time of eyeopening uponverbal command.
Puri andMurthy(2003)6
2B 2 30/30 14/16 >18 years,myocardialrevascularizationor valvereplacement withcardiopulmonarybypass, 18---70years.
BIS between 45and 55.
‘‘Blinded’’monitor.Anesthesia wasadjusted accordingto clinicalparameters.
Time of eyeopening uponverbal commandand extubation,intraoperativememory.
Kreuer et al.(2003)7
2B 2 120/120 40/40 >18 years, ASAI-III, orthopedicsurgery.
BIS 50 and in thelast 15 min of 60.
Anesthesia wasadjusted accordingto clinicalparameters.
Time forspontaneous eyeopening andextubation.
Myles et al.(2004)8
1B 5 2.503/2.463 1.225/1.238 >18 years with atleast one high riskfactor tointraoperativeawakening.
BIS between 40and 60.
Monitor turned off.Anesthesia wasadjusted accordingto clinicalparameters.
Time forspontaneous eyeopening, time fordischarge fromPACU andintraoperativememory.
Bruhn et al.(2005)9
2B 2 200/200 71/58 >18 years, ASAI-III.
BIS of 50. In thelast 15 min BIS of60.
Anesthesia wasadjusted accordingto clinicalparameters.
Time forspontaneous eyeopening andextubation, PONVand intraoperativememory.
Kreuer et al.(2005)10
1B 4 120/120 40/40 >18 years, ASAI-III, orthopedicsurgery.
BIS 50 and in thelast 15 min changeto 60.
Anesthesia wasadjusted accordingto clinicalparameters.
Time forspontaneous eyeopening,extubation andtime for leavingoperation room.
Vretzakis et al.(2005)11
1B 3 130/121 36/44 >18 years,myocardialrevascularizationor valvereplacement withcardiopulmonarybypass, ejectionfraction >45%.
BIS under 60. Anesthesia wasadjusted accordingto clinicalparameters.
Intraoperativememory.

76 C.R. Oliveira et al.
Table 2 (Continued)RCT EL J R/A I/C P I C OAimé et al.
(2006)122B 1 140/125 34/54 Age between 18
and 80 years, ASAI-III, urologic,orthopedic,abdominal andgynecologicalsurgery.
BIS between 40and 60.
‘‘Blinded’’monitor.Anesthesia wasadjusted accordingto clinicalparameters.
Time forspontaneous eyeopening andtraquealextubation.
Ibraheim et al.(2008)13
2B 0 30/30 15/15 >18 years, morbidobese, gastricband surgery.
BIS between 40and 60.
Anesthesia wasadjusted accordingto clinicalparameters
Time of eyeopening uponverbal command,time forextubation anddischarge fromPACU.
Kamal et al.(2009)14
2B 1 60/57 29/28 >18 years, ASAI-III, abdominalsurgery
BIS between 50and 60.
‘‘Blinded’’monitor.Anesthesia wasadjusted accordingto clinicalparameters.
Time forspontaneous eyeopening,extubation,orientation in timeand place, leavingoperating room,discharge fromPACU andintraoperativememory.
Zhang et al.(2011)15
1B 5 5.309/5.228 2.919/2.309 >18 years, totalintravenousanesthesia
BIS between 40and 60.
‘‘Blinded’’monitor.Anesthesia wasadjusted accordingto clinicalparameters.
Intraoperativememory.
Chan et al.(2013)16
1B 3 921/902 450/452 >60 years, electivenon-cardiacsurgery.
BIS between 40and 60.
Anesthesia wasadjusted accordingto clinicalparameters.
Time forspontaneous eyeopening, time fordischarge fromPACU, cognitivedysfunction in thepostoperativeperiod (one weekand three monthslater) anddelirium.
Radtke et al.(2013)17
1B 3 1.277/1.155 575/580 >60 years BIS between 40and 60.
‘‘Blinded’’monitor.Anesthesia wasadjusted accordingto clinicalparameters.
Cognitivedysfunction in thepostoperativeperiod (one weekand three monthslater) anddelirium.
ASA, American Society of Anesthesiologists Physical Status; RCT, Randomized Clinical Trial; EL, Evidence Level; J, Jadad score; R/A,patients randomized and analyzed; I/C, intervention group/control group; P, population; I, intervention; C, control or comparison; O,
sH(
ciaow(
cIw
0t(
t(srm(
outcome.
pontaneous eye opening of 0.28 min (95% CI −0.75, 0.20).owever, the statistically significant difference was lost
Fig. 2).The time for eye opening upon verbal command is
ounted from the end of last suture, when the inhaled orntravenous anesthetic is discontinued and the patient issked to open his eyes. There was a reduction in time to eyepening at verbal command of 0.63 min (95% CI −1.30, 0.05),ith an I2 = 67%, with no statistically significant difference
Fig. 3).
The use of BIS reduced 1.18 min in the time of tra-heal extubation (95% CI −1.65, −0.70), with an I2 = 79%.n sensitivity analysis, when the study Kreuer et al.7
as removed, the time to tracheal extubation reduced
t2t
.87 min (95% CI −1.36, −0.38), with an I2 = 59%, main-aining, therefore, a statistically significant differenceFig. 4).
The combination of three studies1,2,14 demonstrated thathe time for orientation in time and place reduced 3.08 min95% CI −3.70, −2.45) with an I2 = 73%. In sensitivity analy-is, when the study Nelskylä et al.1 was removed we have aeduction of 3.76 min (95% CI −4.55, −2.97) with an I2 = 0%,aintaining, therefore, a statistically significant difference
Fig. 5).
When using the BIS, the time for the patient to be ableo get out of the operating room and go to PACU reduced.93 min (95% CI −3.68, −2.18), with an I2 = 92%. In sensi-ivity analysis, when removed the study Kreuer et al.,10 we

Benefit of general anesthesia monitored by bispectral index 77
Table 3 Full-text articles excluded with reasons.
Article Reason of exclusion
Sebel et al. (1997)18 Before incision tetanus stimulation was applied to the ulnar nerve. Any presence ofmovement, anesthesia was deepened. In the absence of movement, anesthesia wasmaintained. After incision any movement was considered for the deepening of anesthesia.The study goes out of focus --- BIS intervention compared to the control group (consciousnessguided by clinical parameters only).
Yli-Hankala et al. (1999)19 The data expression of the outcomes was made in medians.Mi et al. (1999)20 Patients were monitored with BIS and outcomes were analyzed due to different anesthetic
regimens. The study goes out of focus --- BIS intervention compared to the control group(consciousness guided by clinical parameters only).
Nakayama et al. (2002)21 All patients were monitored with BIS and outcomes were analyzed due to different anestheticregimens (only propofol or propofol and fentanyl). The study goes out of focus --- BISintervention compared to the control group (consciousness guided by clinical parametersonly).
Lehmann et al. (2002)22 All patients were monitored with BIS and analyzed outcomes resulting from differentanesthetic techniques (with manual propofol infusion vs. propofol in Target ControlledInfusion --- TCI). The study goes out of focus --- BIS intervention compared to the control group(consciousness guided by clinical parameters only).
Paventi et al. (2002)23 All patients were monitored with BIS and analyzed outcomes resulting from differentanesthetic techniques (manual propofol infusion vs. propofol in TCI). The study goes out offocus --- BIS intervention compared to the control group (consciousness guided by clinicalparameters only).
Lehmann et al. (2003)24 All patients were monitored with BIS (group BIS 50 and group BIS 40). The study goes out offocus --- BIS intervention compared to the control group (consciousness guided by clinicalparameters only).
Yamaguchi et al. (2003)25 All patients were monitored with BIS and analyzed outcomes resulting from differentanesthetic drugs and techniques (propofol group/iv induction and sevoflurane group withinhalational induction in adult by the vital capacity technique). The study goes out of focus ---BIS intervention compared to the control group (consciousness guided by clinical parametersonly).
Buyukkocak et al. (2003)26 All patients were monitored with BIS and outcomes were analyzed due to different anestheticdrugs, four different methods of sedation associated with topical anesthesia. The study goesout of focus --- BIS intervention compared to the control group (consciousness guided byclinical parameters only).
Forestier et al. (2003)27 All patients were monitored with BIS and analyzed five groups with different concentrations ofsufentanil. The study goes out of focus --- BIS intervention compared to the control group(consciousness guided by clinical parameters only).
Schneider et al. (2003)28 All patients were monitored with BIS and analyzed four different anesthetic regimens. Thestudy goes out of focus --- BIS intervention compared to the control group (consciousnessguided by clinical parameters only).
Schneider et al. (2003)29 All patients were monitored with BIS and analyzed two different anesthetic regimens. Thestudy goes out of focus --- BIS intervention compared to the control group (consciousnessguided by clinical parameters only).
Liu (2004)30 Meta-analysis. The criteria for inclusion in the systematic review were randomized controlledtrials.
Bauer et al. (2004)31 All patients were monitored with BIS and analyzed two different anesthetic regimens (TCI vs.manual propofol infusion). The BIS was used but is not described whether it was blinded. Thestudy goes out of focus --- BIS intervention compared to the control group (consciousnessguided by clinical parameters only).
Bestas et al. (2004)32 All 50 patients (two groups of 25) were monitored with BIS and were blinded, with analysis oftwo different anesthetic regimes. The study goes out of focus --- BIS intervention compared tothe control group (consciousness guided by clinical parameters only).
Boztug et al. (2006)33 Article not found.Puri et al. (2007)34 All patients were monitored with BIS, with analysis of two different types of propofol infusion.
The study goes out of focus --- BIS intervention compared to the control group (consciousnessguided by clinical parameters only).

78 C.R. Oliveira et al.
Table 3 (Continued)
Article Reason of exclusion
Lindholm et al. (2008)35 The paper analyzes the degree of proficiency in handling the BIS by nurses’ anesthetists. Thestudy goes out of focus --- BIS intervention compared to the control group (consciousnessguided by clinical parameters only).
Avidan et al. (2008)36 In the control group, anesthesia was maintained with BIS ‘‘blinded’’ but with an expiredfraction of 0.7---1.3 minimum alveolar concentration of inhaled anesthetic.
Bejjani et al. (2009)37 All patients were monitored with BIS with memory processing analysis. The study goes out offocus --- BIS intervention compared to the control group (consciousness guided by clinicalparameters only).
Delfino et al. (2009)38 All patients were monitored with BIS or cerebral state index, with analysis of propofol infusionwith these two types of monitoring. The study goes out of focus --- BIS intervention comparedto the control group (consciousness guided by clinical parameters only).
Kerssens et al. (2009)39 Study of intraoperative memory and retrieval of words heard during the trans-operative,through memory tests postoperatively.
Mashour et al. (2009)40 Cohort study. The criteria for inclusion in the systematic review were randomized controlledtrials.
Satisha et al. (2010)41 Cohort study. The criteria for inclusion in the systematic review were randomized controlledtrials.
Meybohm et al. (2010)42 Protocol study. The criteria for inclusion in the systematic review were randomized controlledtrials.
Leslie et al. (2010)43 Retrospective cohort study. The criteria for inclusion in the systematic review wererandomized controlled trials.
Avidan et al. (2009)44 Protocol study. The criteria for inclusion in the systematic review were randomized controlledtrials.
Ellerkmann et al. (2010)45 Inhalation or intravenous anesthesia, complemented by regional anesthesia (combinedanesthesia). The study goes out of focus --- BIS intervention compared to the control group(consciousness guided by clinical parameters only).
Yufune et al. (2011)46 The 38 patients were monitored with BIS and outcomes were analyzed due to differentanesthetic regimens, as well as different concentrations of remifentanil. The study goes outof focus --- BIS intervention compared to the control group (consciousness guided by clinicalparameters only).
Liu et al. (2011)47 All patients were monitored with BIS and outcomes were analyzed due to different anestheticregimens, target controlled infusion of propofol vs. closed-loop management. The study goesout of focus --- BIS intervention compared to the control group (consciousness guided byclinical parameters only).
Avidan et al. (2011)48 The control group was adjusted for maintaining an expired fraction of 0.7---1.3 minimumalveolar concentration of inhaled anesthetic.
Aimé et al. (2012)49 The 102 patients were monitored with BIS or Entropy, in both groups, the values were blinded,and anesthesia was conducted by clinical parameters. The study goes out of focus --- BISintervention compared to the control group (consciousness guided by clinical parametersonly).
Mashour et al. (2012)50 The control group was blinded, but adjusted to a minimum alveolar concentration of inhaledanesthetic by age.
Persec et al. (2012)51 The results of this study cannot be meta-analyzed as they provide no standard deviation.Fritz et al. (2013)52 Retrospective cohort study. The criteria for inclusion in the systematic review were
randomized controlled trials.Villafranca et al. (2013)53 Retrospective cohort study. The criteria for inclusion in the systematic review were
randomized controlled trials.
hIf
i4i
ww(
BIS, bispectral index.
ave a reduction of 4.89 min (95% CI −5.95, −3.83) with an2 = 0%, maintaining, therefore, statistically significant dif-erence (Fig. 6).
The time for patients to achieve the discharge criteria
n the PACU (Aldrete-Kroulik modified index) was reduced.05 min (95% CI −7.23, −0.87), with I2 = 91%. In sensitiv-ty analysis, when removed the study Ibraheim et al.,13tsI
e have a reduction of 22.35 min (95% CI −31.01, −13.69)ith I2 = 20%, maintaining statistically significant difference
Fig. 7).There was no statistically significant difference between
he intervention and control in the evaluation of the neces-ary time to hospital discharge (95% CI, −22.08, 30.52) with2 = 0% (Fig. 8).

Benefit of general anesthesia monitored by bispectral index 79
Study or Subgroup
Nelskylä KA 2001
Nelskylä KA 2001
Wong J 2002
Wong J 2002
Kreuer S 2003
Kreuer S 2003
Kreuer S 2005
Kreuer S 2005
Aimé I 2006
Aimé I 2006
Kamal NM 2009
Kamal NM 2009
Total (95% CI)
Total (95% CI)
Heterogeneity : Chi2=34.57, df=6 (P<.00001); I2=83%
Heterogeneity : Chi2=2.29, df=5 (P=.81); I2 = 0%
Test for overall effect: Z=2.64 (P=.008)
Test for overall effect: Z=1.13 (P=.26)
275
235 241
281 100.0%
100.0%
Bruhn J 2005
Bruhn J 2005
5
4
3.5 2.9 40 9.3 5.2 40
3.5 2.9 40 9.3 5.2 40
5.6 2.5 58
4.7 2.2 40
3.9 54
1.9 28
–10 –5 0 5 10
–10 –5 0 5 10
58
4054
28
8
4.4
713.4
2.1 40
4.1 34
1.6 29
5.9
5.6 2.5713.45.9
4.2
4.7 2.22.1 404.2
7.6
3.984.1 347.6
4.1
1.94.41.6 294.1
2.1 29
5 32 5
4.9 3.4 31
4 2.1 29 4.9 3.4 31
2 30
5 5 32 5 2 30
6.1% 2001
2002
2003
2005
2005
2006
2009
2001
2002
2003
2005
20052006
2009
10.6%
6.3%
20.5%
24.0%
7.1%
25.5%
6.5%
11.3%
0.0%
21.9%
25.6%7.6%
27.2%
0.00 [–1.87, 1.87]
–0.90 [–2.32, 0.52]
–5.80 [–7.65, –3.95]
0.30 [–0.72, 1.32]
–0.50 [–1.44, 0.44]
–0.40 [–2.13, 1.33]
–0.30 [–1.21, 0.61]
0.00 [–1.87, 1.87]
–0.90 [–2.32, 0.52]
–5.80 [–7.65, –3.95]
0.30 [–0.72, 1.32]
–0.50 [–1.44, 0.44]–0.40 [–2.13, 1.33]
–0.30 [–1.21, 0.61]
–0.62 [–1.08, –0.16]
–0.28 [–0.75, 0.20]
Mean MeanSD SD Total Tota l Weigh t Year
Year
IV, Fi xed, 95% C I IV, Fi xed, 95% CIBIS Control Mean difference
Study or Subgroup Mean MeanSD SD Total Tota l Weigh t IV, Fi xed, 95% CIBIS Control Mean difference
Mean difference
IV, Fi xed, 95% CIMean difference
BIS Control
BIS Control
ntane
aIc(
D
Trt4cso
Figure 2 Time for spo
The incidence of PONV was lower in anesthesia conductedwith BIS, with a risk reduction of 12% (95% CI −0.22, −0.01)with I2 = 61%, which was statistically significant (Fig. 9).
There was no risk reduction of cognitive disorders in thepost operatory with 1 week after extubation, in patientsusing BIS (95% CI, −0.06, 0.01, I2 = 0%). There was no statis-tically significant difference between the intervention andcontrol (Fig. 10).
The cognitive disorders after surgery at 3 months afterextubation had a risk reduction of 3% (95% CI −0.05, −0.00),and I2 = 52%, which was statistically significant (Fig. 11).
There was a 6% reduction in the risk of delirium inthe post operatory in patients monitored with BIS (95% CI−0.10, −0.03) I2 = 11%, which was statistically significant(Fig. 12).
The use of BIS had a risk reduction of 1% for the intraoper-ative memory (Recall), a statistically significant difference(−0.01 [95% CI, −0.01, −0.00]) with I2 = 0%. The intraoper-
wcr
Study or Subgroup
Total (95% CI) 59 61 100.0%
Mean
Basar H 2003 8.25
18.5
6.8 2.1 15 8.66 2.6 15 15.9%
11.5 14 28 16 0.5%15
1.8 30 8.59 1 30 83.6%
Puri GD 2003
Ibraheim O 2008
Heterogeneity: Chi2=5.97, df=2 (P=.05); I2=67%
Test for overall effect: Z=1.82 (P=.07)
MeanSD SDTotal Total WeighBIS Control
Figure 3 Time for eye opening u
ous eye opening (min).
tive memory is the awakening confirmed by the patient.t was not made a differentiation of studies with patientslassified as low or high risk for intraoperative memoryFig. 13).
iscussion
he use of monitoring with the BIS showed benefits byeducing the time to extubation in 0.87 min, orientation inime and place in 3.76 min and leaving operating room in.89 min. Patients had a reduction in 22.35 min to reach theriteria for PACU discharge. The combined results of thetudies showed that the incidence of PONV risk reductionf 12% in patients BIS monitoring.
Cognitive disorders in postoperative patients with 1eek after extubation did not show statistically signifi-ant difference. However, there was a 3% reduction in theisk of cognitive disorders in the postoperative patients
–0.63 [–1.30, 0.05]
BIS Control
–9.50 [–19.00, 0.00]
–1.86 [–3.55, 0.17]
–0.34 [–1.08, 0.40]
2003
2008
2003
–10 –5 0 5 10
t YearIV, Fixed, 95% CI IV, Fixed, 95% CIMean difference Mean difference
pon verbal command (min).

80 C.R. Oliveira et al.
Study or Subgroup
Total (95% CI)
Total (95% CI)
355
315
361
321
100.0%
100.0%
–1.18 [–1.65, –0.70]
–0.87 [–1.36, –0.38]
Nelskylä KA 2001 2
6.8 4.6 40 10.5 5.9 40 4.2%
4.4%
3.0%
6.5%
9.8%
21.8%
2.6%
7.2%
17.4%
40
16
40
40
58
54
15
28
6.1
3.2
5.3
4.4
2.4
9
2.9
2.3
8.3
6
9.7
5.4
6.3
14.2
11.8
4.8
4.1 40
14
40
40
71
34
15
29
4.3
2.9
2.2
3.5
5.1
2
2.1
6.5
7.2
4.1
4.4
6.6
11.1
9.26
4.3
2 32 3 2
2
6.8 4.6 40 10.5 5.9
6.1
3.2
5.3
4.4
2.4
9
2.9
2.3
8.3
6
9.7
5.4
6.3
14.2
11.8
4.8
4.1 40
14
40
40
71
34
15
29
4.3
2.9
2.2
3.5
5.1
2
2.1
6.5
7.2
4.1
4.4
6.6
11.1
9.26
4.3
2 32 3 2
30
40
40
16
40
40
58
54
15
28
30
23.0%
24.6%
4.5%
4.7%
3.2%
0.0%
10.5%
23.4%
2.8%
18.6%
–10 0 10 5–5
7.7%
–1.00 [–2.00, –0.00]
–1.00 [–2.00, –0.00]
–3.70 [–6.02, –138]
–3.70 [–6.02, –138]
–1.80 [–4.08, 0.48]
1.20 [–1.54, 3.94]
–5.60 [ –7.47, –3.73]
–1.00 [–2.52, 0.52]
0.30 [–0.72, 1.32]
–3.10 [–6.05, –0.15]
–2.54 [–4.32, –0.76]
–0.50 [–1.64, 0.64]
2001
2003
2003
2003
2003
2005
2005
2006
2008
2009
2001
2003
2003
2003
2003
2005
2005
2006
2008
2009
–1.80 [–4.08, 0.48]
1.20 [–1.54, 3.94]
–5.60 [ –7.47, –3.73]
–1.00 [–2.52, 0.52]
0.30 [–0.72, 1.32]
–3.10 [–6.05, –0.15]
–2.54 [–4.32, –0.76]
–0.50 [–1.64, 0.64]
Luginbühl M, 2003 (a)
Luginbühl M, 2003 (b)
Puri GD 2003
Kreuer S 2003
Kreuer S 2005
Bruhn J 2005
Aimé I 2006
Ibraheim O 2008
Kamal NM 2009
Nelskylä KA 2001
Luginbühl M, 2003 (a)
Luginbühl M, 2003 (b)
Puri GD 2003
Kreuer S 2003
Kreuer S 2005
Bruhn J 2005
Aimé I 2006
Ibraheim O 2008
Kamal NM 2009
Heterogeneity: Chi2=42.58, df=9 (P<.00001); I2=79%–10 –5 0 5 10
Test for overall effect: Z=4.83 (P<.00001)
Heterogeneity: Chi2=19.65, df=8 (P=.01); I2=59%
Test for overall effect: Z=3.45 (P=.0006)
Mean MeanSD SD Total Tota l Weight YearIV, Fixed, 95% CI IV, Fi xed, 95% CIBIS Control Mean difference Mean difference
Study or Subgroup Mean MeanSD SDTotal Total Weight YearIV, Fixed, 95% CI IV, Fixed, 95% CIBIS Control Mean dif ference Mean dif ference
BIS Control
BIS Control
Figure 4 Time to tracheal extubation (min). Luginbühl (2003) studied within a single outcome, two different anesthetic regimensw
3tuiB
r
ith propofol (a) and desflurane (b).
months after extubation. There was a 6% reduction inhe risk of delirium incidence of postoperative in patients
sing BIS monitoring. In addition, the memory of thentraoperative risk had a reduction of 1% after usingIS.rgc
Study or Subgroup Mean MeanSD SD Total Tota l WeightBIS Control
Study or Subgroup Mean MeanSD SD Total Tota l WeightBIS Control
Nelskylä KA 2001
Wong J 2002
6
9.5
7.4
2
3.1
1.5
32
29
29
3 2
3.813.1
11.2 1.9
30 38.8%
12.6%
48.6%28
31
Kamal NM 2009
Nelskylä KA 2001Wong J 2002
29.57.4
23.11.5
322929
3 23.813.1
11.2 1.9
30 0.0%20.6%79.4%28
31Kamal NM 2009
Total (95% CI) 90 89 100.0% Heterogeneity: Chi2=7.36, df=2 (P=.03); I2=73%
Test for overall effect: Z=9.71 (P<.00001)
Total (95% CI) 58 59 100.0 %Heterogeneity: Chi2=.04, df=1 (P=.84); I2=0%
Test for overall effect: Z= 9.28 (P<.00001)
Figure 5 Time for orientation
The 17 studies selected by the pre-established crite-ia showed a heterogeneity that was soon noticed. Factors
elated to anesthetic technique, the patient and the sur-ical procedure were observed. Studies that analyzed theonsumption of anesthetics showed no standardized meas-YearIV, Fixed, 95% CI IV, Fi xed, 95% CIMean difference Mean dif ference
YearIV, Fi xed, 95% CI IV, Fi xed, 95% CIMean difference Mean difference
–2.00 [–3.00, –1.00]
–3.60 [–5.35, –1.85]
–3.80 [–4.69, –2.91]
2001
2002
2009
2001
20022009
–10 –5 0 5 10
–2.00 [–3.00, –1.00]–3.60 [–5.35, –1.85]–3.80 [–4.69, –2.91]
–3.08 [–3.70, –2.45]
–3.76 [–4.55, –2.97]
–10 –5 0 5 10
BIS Control
BIS Control
in time and place (min).

Benefit of general anesthesia monitored by bispectral index 81
Study or Subgroup Mean MeanSD SDTotal Total Weight YearIV, Fixed, 95% CI IV, Fixed, 95% CIBIS Control Mean difference Mean difference
40
40
40
40
Kreuer S 2003
Kreuer S 2005
9.4
8.4
7
9.4
8.4
7
1.9
2.4
3.2
1.9
2.4
3.2
29
40
40
29
14.1
9.4
12.4
14.1
9.4
12.4
2.8
2.4
5.7
2.8
2.4
5.7
–4.70 [–5.95, –3.45]
–1.00 [–2.05, 0.05]
–5.40 [–7.43, –3.37]
2009
2005
2003
2009
2005
2003
–4.70 [–5.95, –3.45]
–1.00 [–2.05, 0.05]
–5.40 [–7.43, –3.37]
35.9%
72.5%
0.0%
27.5%
50.5%
13.6%
28
40
40
28Kamal NM 2009
Kreuer S 2003
Kreuer S 2005
Kamal NM 2009
Total (95% CI) 109 108 100.0% –2.93 [–3.68, –2.18]
Heterogeneity: Chi2=26.39, df=2 (P<.00001); I2=92%
Test for overall effect: Z=7.68 (P<.00001)
Total (95% CI) 69 68 100.0% –4.89 [–5.95, –3.83]
Heterogeneity: Chi2=.33, df=1 (P<.56); I2=0%
Test for overall effect: Z=9.03 (P<.00001)
Study or Subgroup Mean MeanSD SDTotal Total Weight YearIV, Fixed, 95% CI IV, Fixed, 95% CIBIS Control Mean difference Mean difference
–10 –5 0 5 10
–10 –5 0 5 10
BIS Control
BIS Control
Figure 6 Time for leaving operation room (min).
Wong J 2002 111 30 29 48 123 –12.00 [–32.12, 8.12]2.5%31
Wong J 2002 111 30 29 48 123 –12.00 [–32.12, 8.12]18.5%31
86.5%154.8131154.7429.8 –1.20 [–4.62, 2.22]Ibraheim O 2008
0.0%154.8131154.7429.8 –1.20 [–4.62, 2.22]Ibraheim O 2008
11.0%2821.578.62914.753.9 –24.70 [–34.29, –15.11]
2002
2008
2009
2002
2008
2009
Kamal NM 2009
81.5%2821.578.62914.753.9 –24.70 [–34.29, –15.11]Kamal NM 2009
Total (95% CI) 73 74 100.0% –4.05 [–7.23, –0.87]Heterogeneity: Chi2=21.07, df=2 ( P<.0001); I2=91%
Test for overall effect: Z=2.50 (P=.01)
Total (95% CI) 58 59 100.0% –22.35 [–31.01, –13.69]
Heterogeneity: Chi2=1.25, df=1 ( P=.26); I2=20%
Test for overall effect: Z=5.06 (P<.00001)
Study or Subgroup Mean MeanSD SDTotal Total Weight YearIV, Fixed, 95% CI IV, Fixed, 95% CIBIS Control Mean difference Mean difference
Study or Subgroup Mean MeanSD SDTotal Total Weight YearIV, Fixed, 95% CI IV, Fixed, 95% CIBIS Control Mean difference Mean difference
BIS Control–100 –50 0 50 100
BIS Control–100 –50 0 50 100
ischa
fr
Figure 7 Time for d
ures that enabled the selection of at least two studies forthe meta-analysis.
The study Ibraheim et al.13 involved morbidly obese
patients. Three studies were conducted exclusively withpatients over 60 years of age.2,16,17Puri et al.6 and Vretzakis et al.11 studied patients under-going cardiac surgery with extracorporeal circulation.
rhhfi
Study or Subgroup Mean MeanSD SD Total Tota l WeighBIS Control
Nelskylä KA 2001
Ahmad S 2003
306 85 32 298 124 30 24.4%
203 78 49 200 74 48 75.6%
Total (95% CI)
Heterogeneity: Chi2=0.03, df=1 (P=.87); I2=0%
Test for overall effect: Z=0.31 (P=.75)
81 78 100.0%
Figure 8 Time to hospi
rge from PACU (min).
Myles et al.8 studied patients with at least one high-riskactor for awakening with intraoperative memories (highisk heart surgery, cesarean sections, hypovolemic shock,
igid bronchoscopy, cardiovascular instability and expectedypotension during surgery, lung disease in advanced stages,istorical of awakening with intraoperative memories, dif-cult airway, high consumption of alcohol, chronic uset IV, Fi xed, 95% CI IV, Fi xed, 95% CIMean difference Mean difference
8.00 [–45.26, 61.26]
3.00 [–27.25, 33.25]
Year2001
2003
4.22 [–22.08, 30.52]
–100 –50 0 50 100
BIS Control
tal discharge (min).

82 C.R. Oliveira et al.
Study or Subgroup Events EventsTotal Total Weight M-H, Fi xed, 95% CI M-H, Fi xed, 95% CIBIS Control Risk dif ference Risk dif ference
Nelskylä KA 2001
Bruhn J 2005
5 32 12 30 32.7%
6 71 8 58 67.3%
–0.24 [–0.46, –0.03]
–0.05 [–0.16, 0.06]
Year2001
2005
Total (95% CI)
Total events
Heterogeneity: Chi2=2.59, df=1 (P=. 11); I2=61%Test for overall effect: Z=2.22 (P=.03)
103
11
88
20
100.0% –0.12 [–0.22, –0.01]
–1 –0.5 0 0.5 1
BIS Control
Figure 9 Postoperative nausea and vomiting (PONV) --- n (%).
Study or Subgroup Ev ents Ev entsTotal Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CIBIS Control Risk difference Risk difference
Chan 2013
Radtke 2013
9870
450 104 452 43.9% –0.01 [–0.07, 0.04]
575 90 580 56.1% –0.03 [–0.07, 0.01]
Total ev entsHeterogeneity: Chi2=.39, df=1 (P=.53); I2=0%Test for ov erall effect: Z=1.45 (P=.15)
168 194
–1 –0.5 0 0.5 1
BIS Control
Total (95% CI) 1025 1032 100.0% –0.02 [–0.06, 0.01]
Figure 10 Cognitive disorders in the postoperative period (1 week after extubation) --- n (%).
Study or Subgroup Events EventsTotal Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CIBIS Control Risk difference Risk difference
Chan 2013Radtke 2013
4621
450 66 452 43.9% –0.04 [–0.09, –0.00]575 28 580 56.1% –0.01 [–0.03, 0.01]
Total eventsHeterogeneity: Chi2=2.08, df=1 (P=.15); I2=52%Test for overall effect: Z=2.21 (P=.03)
67 94
–0.5 –0.25 0.25 0.50
BIS Control
Total (95% CI) 1025 1032 100.0% –0.03 [–0.05, –0.00]
Figure 11 Cognitive disorders in the postoperative period (3 months after extubation) --- n (%).
Study or Subgroup Events EventsTotal Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CIBIS Control Risk difference Risk difference
Chan 2013Radtke 2013
7095
450 109 452 43.9% –0.09 [–0.14, –0.03]575 28 580 56.1% –0.05 [–0.09, –0.00]
Year20132013
Total eventsHeterogeneity: Chi2=1.12, df =1 (P=.29); I2=11%Test for overall effect: Z=3.74 (P=.0002)
165 233
–1 –0.5 0.5 10
BIS Control
Total (95% CI) 1025 1032 100.0% –0.06 [–0.10, –0.03]
Figure 12 Postoperative delirium --- n (%).
Study or Subgroup Events EventsTotal Total Weight M-H, Fixed, 95% CI M-H, Fixed, 95% CIBIS Control Risk difference Risk difference
Puri GD 2003Myles PS 2004
Bruhn J 2005Kamal NM 2009Zhang C 2011
020
14 1 16 0.4% –0.06 [–0.23, 0.10]1225
7129
2919
04
11
00
15
123858
28
2309
31.4%1.6%0.7%
65.8%
–0.01 [–0.01, –0.00]
0.00 [–0.03, 0.03]0.00 [–0.07, 0.07]
–0.01 [–0.01, –0.00]
20032004200520092011
Total eventsHeterogeneity: Chi2=1.04, df=4 (P=.90); I2=0%Test for overall effect: Z=3.73 (P=.0002)
6 27
–0.1 –0.05 0.05 0.10
BIS Control
Total (95% CI) 4258 3649 100.0% –0.01 [–0.01, –0.00]
Year
Figure 13 Intraoperati
ve memory --- n (%).
1
1
1
1
1
1
1
1
1
1
2
2
2
2
Benefit of general anesthesia monitored by bispectral index
of benzodiazepines or opioids and therapy with proteaseinhibitors).
The outcomes analyzed with continuously variablerelated to the time of recovery and discharge of patientswere: time for spontaneous eye opening, time for eye open-ing upon verbal command, time for extubation, time fororientation in time and place, time for leaving operatingroom, time for PACU discharge and time for hospital dis-charge.
The outcomes of dichotomous variable, related toadverse events were PONV, cognitive disorders in the post-operative 1 week after extubation, cognitive disorders inthe postoperative 3 months after extubation, postoperativedelirium and intraoperative memory.
Some primary studies contributed only one outcomeanalyzed.3---5,11,15
The individualization of outcomes derived from studiesinvolving balanced anesthesia or total intravenous anesthe-sia was not made.
Clinically, the cost of implementation of BIS monitoringcan be justified by allowing advantages in the maintenanceof ambulatory surgeries as well as in the techniques of earlyawakening and especially it can reduce the incidence ofadverse events.
The cost of the disposable electrode is a cause of dis-cussion about the value in use of BIS. Thus, it is importantthe active participation of professionals, primarily withhealth administrators, in developing a policy plan that opti-mize resources and give greater safety and comfort for thepatients.
So far, there is no gold standard to span the entire spec-trum of anesthetic effect on the central nervous system, andthe BIS is undoubtedly the most studied, but is one of manymonitors derived from EEG used nowadays. Monitoring thedepth of anesthesia as new technology is in its beginning.The new boundary is the individualization of monitoring thehypnotic and its effects on the central nervous system.
Conflicts of interest
The authors declare no conflicts of interest.
References
1. Nelskylä KA, Yli-Hankala AM, Puro PH, et al. Sevoflurane titra-tion using bispectral index decreases postoperative vomitingin phase II recovery after ambulatory surgery. Anesth Analg.2001;93:1165---9.
2. Wong J, Song D, Blanshard H, et al. Titration of isoflurane usingBIS index improves early recovery of elderly patients undergoingorthopedic surgeries. Can J Anaesth. 2002;49:13---8.
3. Luginbühl M, Wüthrich S, Petersen-Felix S, et al. Different bene-fit of bispectal index (BIS) in desflurane and propofol anesthesia.Acta Anaesthesiol Scand. 2003;47:165---73.
4. Ahmad S, Yilmaz M, Marcus RJ, et al. Impact of bispectral indexmonitoring on fast tracking of gynecologic patients undergoing
laparoscopic surgery. Anesthesiology. 2003;98:849---52.5. Basar H, Ozcan S, Buyukkocak U, et al. Effect of bispectralindex monitoring on sevoflurane consumption. Eur J Anaesthe-siol. 2003;20:396---400.
2
83
6. Puri GD, Murthy SS. Bispectral index monitoring in patientsundergoing cardiac surgery under cardiopulmonary bypass. EurJ Anaesthesiol. 2003;20:451---6.
7. Kreuer S, Biedler A, Larsen R, et al. Narcotrend moni-toring allows faster emergence and a reduction of drugconsumption in propofol-remifentanil anesthesia. Anesthesiol-ogy. 2003;99:34---41.
8. Myles PS, Leslie K, McNeil J, et al. Bispectral index monitoring toprevent awareness during anaesthesia: the B-Aware randomisedcontrolled trial. Lancet. 2004;363:1757---63.
9. Bruhn J, Kreuer S, Bischoff P, et al. Bispectral index and A-lineAAI index as guidance for desflurane-remifentanil anaesthesiacompared with a standard practice group: a multicentre study.Br J Anaesth. 2005;94:63---9.
0. Kreuer S, Bruhn J, Stracke C, et al. Narcotrend or bispectralindex monitoring during desflurane-remifentanil anesthesia: acomparison with a standard practice protocol. Anesth Analg.2005;101:427---34.
1. Vretzakis G, Ferdi E, Argiriadou H, et al. Influence of bispectralindex monitoring on decision making during cardiac anesthesia.J Clin Anesth. 2005;17:509---16.
2. Aimé I, Verroust N, Masson-Lefoll C, et al. Does monitoringbispectral index or spectral entropy reduce sevoflurane use?Anesth Analg. 2006;103:1469---77.
3. Ibraheim O, Alshaer A, Mazen K, et al. Effect of bispec-tral index (BIS) monitoring on postoperative recovery andsevoflurane consumption among morbidly obese patients under-going laparoscopic gastric banding. Middle East J Anesthesiol.2008;19:819---30.
4. Kamal NM, Omar SH, Radwan KG, et al. Bispectral index moni-toring tailors clinical anesthetic delivery and reduces anestheticdrug consumption. J Med Sci. 2009;9:10---6.
5. Zhang C, Xu L, Ma YQ, et al. Bispectral index monitoring preventawareness during total intravenous anesthesia: a prospective,randomized, double-blinded, multi-center controlled trial. ChinMed J (Engl). 2011;124:3664---9.
6. Chan MT, Cheng BC, Lee TM, et al. BIS-guided anesthesiadecreases postoperative delirium and cognitive decline. J Neu-rosurg Anesthesiol. 2013;25:33---42.
7. Radtke FM, Franck M, Lendner J, et al. Monitoring depth ofanaesthesia in a randomized trial decreases the rate of postop-erative delirium but not postoperative cognitive dysfunction. BrJ Anaesth. 2013;110 Suppl. 1:i98---105.
8. Sebel PS, Lang E, Rampil IJ, et al. A multicenter study of bispec-tral electroencephalogram analysis for monitoring anestheticeffect. Anesth Analg. 1997;84:891---9.
9. Yli-Hankala A, Vakkuri A, Annila P, et al. EEG bispectral indexmonitoring in sevoflurane or propofol anaesthesia: analysis ofdirect costs and immediate recovery. Acta Anaesthesiol Scand.1999;43:545---9.
0. Mi WD, Sakai T, Singh H, et al. Hypnotic endpoints vs. the bispec-tral index, 95% spectral edge frequency and median frequencyduring propofol infusion with or without fentanyl. Eur J Anaes-thesiol. 1999;16:47---52.
1. Nakayama M, Ichinose H, Yamamoto S, et al. The effectof fentanyl on hemodynamic and Bispectral Index changesduring anesthesia induction with propofol. J Clin Anesth.2002;14:146---9.
2. Lehmann A, Boldt J, Thaler E, et al. Bispectral Index in patientswith target-controlled or manually-controlled infusion of propo-fol. Anesth Analg. 2002;95:639---44.
3. Paventi S, Santevecchi A, Perilli V, et al. Effects of remifentanilinfusion BIS-titrated on early recovery for obese outpatientsundergoing laparoscopic cholecystectomy. Minerva Anestesiol.2002;68:651---7.
4. Lehmann A, Karzau J, Boldt J, et al. Bispectral Index-guidedanesthesia in patients undergoing aortocoronary bypass graft-ing. Anesth Analg. 2003;96:336---43.

8
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
53. Villafranca A, Thomson IA, Grocott HP, et al. The impactof Bispectral Index versus end-tidal anesthetic concentration-guided anesthesia on time to tracheal extubation in fast-trackcardiac surgery. Anesth Analg. 2013;116:541---8.
4
5. Yamaguchi S, Egawa H, Mishio M, et al. Bispectral monitoringduring vital capacity rapid inhalation induction with sevoflu-rane. J Clin Anesth. 2003;15:24---8.
6. Buyukkocak U, Ozcan S, Daphan C, et al. A compari-son of four intravenous sedation techniques and BispectralIndex monitoring in sinonasal surgery. Anaesth Intensive Care.2003;31:164---71.
7. Forestier F, Hirschi M, Rouget P, et al. Propofol and sufentaniltitration with the Bispectral Index to provide anesthesia forcoronary artery surgery. Anesthesiology. 2003;99:334---46.
8. Schneider G, Gelb AW, Schmeller B, et al. Detection of aware-ness in surgical patients with EEG-based indices-bispectralindex and patient state index. Br J Anaesth. 2003;91:329---35.
9. Schneider G, Elidrissi C, Sebel PS. Bispectral index-guidedadministration of anaesthesia: comparison between remifen-tanil/propofol and remifentanil/isoflurane. Eur J Anaesthesiol.2003;20:624---30.
0. Liu SS. Effects of Bispectral Index monitoring on ambulatoryanesthesia. Anesthesiology. 2004;101:311---5.
1. Bauer M, Wilhelm W, Kraemer T, et al. Impact of BispectralIndex monitoring on stress response and propofol consumptionin patients undergoing coronary artery bypass surgery. Anesthe-siology. 2004;101:1096---104.
2. Bestas A, Yasar MA, Bayar MK, et al. The effects of two dif-ferent anaesthesia techniques on bispectral index values andawareness during off-pump coronary artery bypass grafting. JClin Monit Comput. 2004;18:347---51.
3. Boztug N, Bigat Z, Akyüz M, et al. Does using the BispectralIndex (BIS) during craniotomy affect the quality of recovery? JNeurosurg Anesthesiol. 2006;18:1---4.
4. Puri GD, Kumar B, Aveek J. Closed-loop anaesthesia delivery sys-tem (CLADS) using bispectral index: a performance assessmentstudy. Anaesth Intensive Care. 2007;35:357---62.
5. Lindholm ML, Brudin L, Sandin RH. Bispectral index monitoring:appreciated but does not affect drug dosing and hypnotic levels.Acta Anaesthesiol Scand. 2008;52:88---94.
6. Avidan MS, Zhang L, Burnside BA, et al. Anesthesia awarenessand the Bispectral Index. N Engl J Med. 2008;358:1097---108.
7. Bejjani G, Lequeux PY, Schmartz D, et al. No evidence of mem-ory processing during propofol-remifentanil target-controlledinfusion anesthesia with Bispectral Index monitoring in cardiacsurgery. J Cardiothorac Vasc Anesth. 2009;23:175---81.
8. Delfino AE, Cortinez LI, Fierro CV, et al. Propofol consumptionand recovery times after bispectral index or cerebral state indexguidance of anaesthesia. Br J Anaesth. 2009;103:255---9.
9. Kerssens C, Gaither JR, Sebel PS. Preserved memory func-tion during Bispectral Index-guided anesthesia with sevoflu-rane for major orthopedic surgery. Anesthesiology. 2009;111:518---24.
0. Mashour GA, Tremper KK, Avidan MS. Protocol for the ‘‘MichiganAwareness Control Study’’: a prospective, randomized, con-
trolled trial comparing electronic alerts based on bispectralindex monitoring or minimum alveolar concentration for theprevention of intraoperative awareness. BMC Anesthesiol.2009;9:7.C.R. Oliveira et al.
1. Satisha M, Sanders GM, Badrinath MR, et al. Introduction ofbispectral index monitoring in a district general hospital operat-ing suite: a prospective audit of clinical and economic effects.Eur J Anaesthesiol. 2010;27:196---220.
2. Meybohm P, Gruenewald M, Höcker J, et al. Correlation andagreement between the bispectral index vs. state entropy dur-ing hypothermic cardio-pulmonary bypass. Acta AnaesthesiolScand. 2010;54:169---75.
3. Leslie K, Myles PS, Forbes A, et al. The effect of Bispectral Indexmonitoring on long-term survival in the B-Aware trial. AnesthAnalg. 2010;110:816---22.
4. Avidan MS, Palanca BJ, Glick D, et al. Protocol for the BAG-RECALL clinical trial: a prospective, multi-center, randomized,controlled trial to determine whether a bispectral index-guidedprotocol is superior to an anesthesia gas-guided protocol inreducing intraoperative awareness with explicit recall in highrisk surgical patients. BMC Anesthesiol. 2009;9:8.
5. Ellerkmann RK, Soehle M, Riese G, et al. The Entropy Mod-ule and Bispectral Index as guidance for propofol-remifentanilanaesthesia in combination with regional anaesthesia comparedwith a standard clinical practice group. Anaesth Intensive Care.2010;38:159---66.
6. Yufune S, Takamatsu I, Masui K, et al. Effect of remifentanilon plasma propofol concentration and bispectral index duringpropofol anaesthesia. Br J Anaesth. 2011;106:208---14.
7. Liu N, Chazot T, Hamada S, et al. Closed-loop coadmin-istration of propofol and remifentanil guided by BispectralIndex: a randomized multicenter study. Anesth Analg. 2011;112:546---57.
8. Avidan MS, Jacobsohn E, Glick D, et al. Prevention of intraoper-ative awareness in a high-risk surgical population. N Engl J Med.2011;365:591---600.
9. Aimé I, Gayat E, Fermanian C, et al. Effect of age on the com-parability of bispectral and state entropy indices during themaintenance of propofol---sufentanil anaesthesia. Br J Anaesth.2012;108:638---43.
0. Mashour GA, Shanks A, Tremper KK, et al. Prevention of intraop-erative awareness with explicit recall in an unselected surgicalpopulation. Anesthesiology. 2012;117:717---25.
1. Persec J, Persec Z, Kopljar M, et al. Effect of bispectral indexmonitoring on extubation time and analgesic consumption inabdominal surgery: a randomised clinical trial. Swiss Med Wkly.2012;142:w13689.
2. Fritz BA, Rao P, Mashour GA, et al. Postoperative recovery withBispectral Index versus anesthetic concentration-guided proto-cols. Anesthesiology. 2013;118:1113---22.
Recommended