Version_29 November 2012
1
Report by the National Confidential Inquiry into suicides at
Leicestershire Partnership NHS Trust
INTRODUCTION
The National Confidential Inquiry into Suicide and Homicide by People with Mental
Illness (NCI) was approached by the Leicestershire Partnership NHS Trust (LPT) to
provide advice following eight suicides by inpatients during a 3 year period, 2010-
2012. Each of these deaths had been the subject of a serious untoward incident
investigation (SUI).
The following aims for the NCI review were agreed:
To review the eight investigation reports
To discuss these cases with key LPT staff
To consider relevant trust policies
To prepare a short report highlighting important issues and possible measures
for strengthening management of risk
To conduct a seminar for staff, linked to the features of the cases.
PROCESS
The review was carried out on behalf of the NCI by Professor Louis Appleby,
Director of the NCI, and Dr. Kirsten Windfuhr, Senior Project Manager, the authors
of this report.
We visited three wards, Heather, Aston, and Beaumont, at the LPT on the 23 October
2012 and discussed the cases with senior clinical staff and service managers. We
were shown around the units, in particular the outside areas, individual rooms, and
entry and exits to each unit. We want to acknowledge the help of Jackie Ardley in
providing us with the information we requested, and for making arrangements for our
visits on 23 October and 29 November 2012.
We examined the NCI database for patient suicides at LPT. The NCI holds clinical
data on suicides by all people since 1997 who have been in contact with mental health
Version_29 November 2012
2
services in the twelve months before death, covering the whole of England. This
clinical information is submitted via a standard questionnaire completed by the
consultant psychiatrist responsible for the patient (occasionally by another senior
clinician).
We should emphasise that it was not our intention to repeat the earlier incident
reviews or to comment on matters of individual performance or responsibility. Our
review is intended to serve a positive purpose turning findings of the investigations
into lessons for the trust and its staff that will improve patient safety. These will be
incorporated into a seminar on suicide prevention to be held on 29 November 2012.
THE CASES
A summary of the key characteristics for all suicides is shown in Table 1. A summary
of the events leading up to the suicide, and a summary of the recommendations is
provided in Table 2.
In the eight cases, six of the patients were females under 45 years of age. Four of
these had a primary diagnosis of personality disorder, of whom three were under
thirty. The suicide methods in the eight cases were hanging (4 cases), jumping from a
height (2 cases) and overdose (2 cases). Of the three suicides that took place on the
ward, two were by hanging. Five of the patients were detained under the MH Act;
three were off the ward at the time of death.
Version_29 November 2012
3
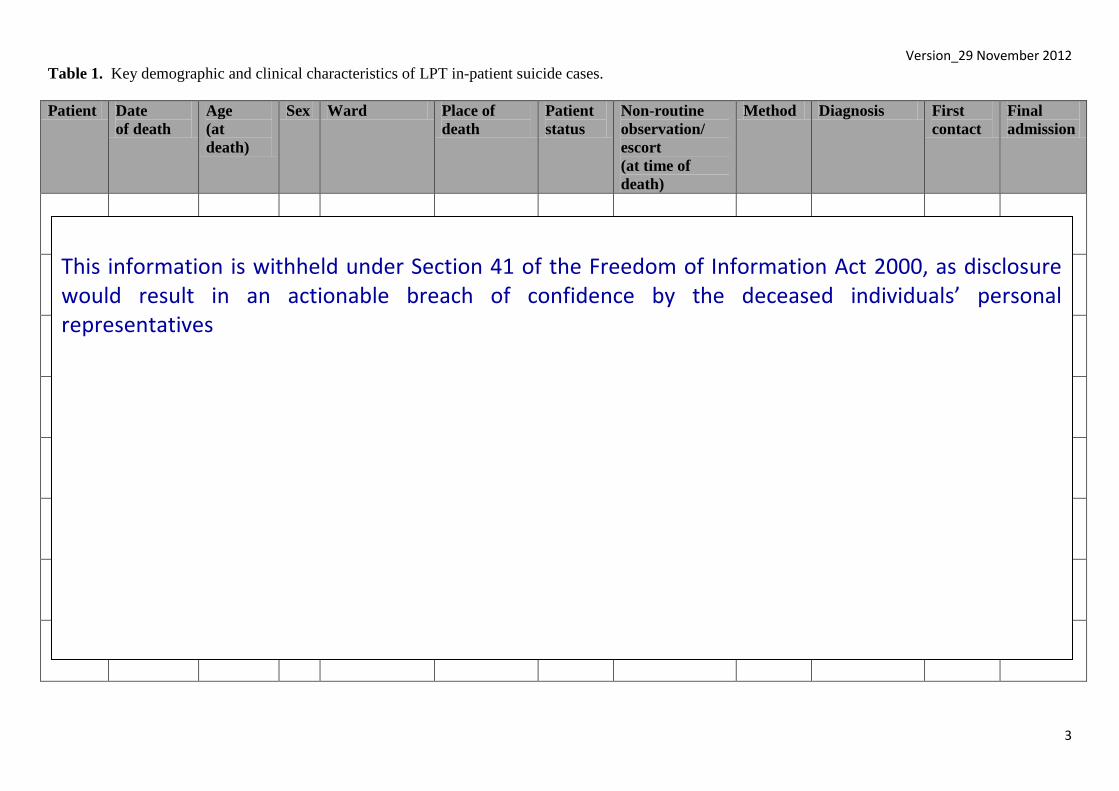
Table 1. Key demographic and clinical characteristics of LPT in-patient suicide cases.
Patient Date
of death
Age
(at
death)
Sex Ward Place of
death
Patient
status
Non-routine
observation/
escort
(at time of
death)
Method Diagnosis First
contact
Final
admission
This information is withheld under Section 41 of the Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives
Version_29 November 2012
4
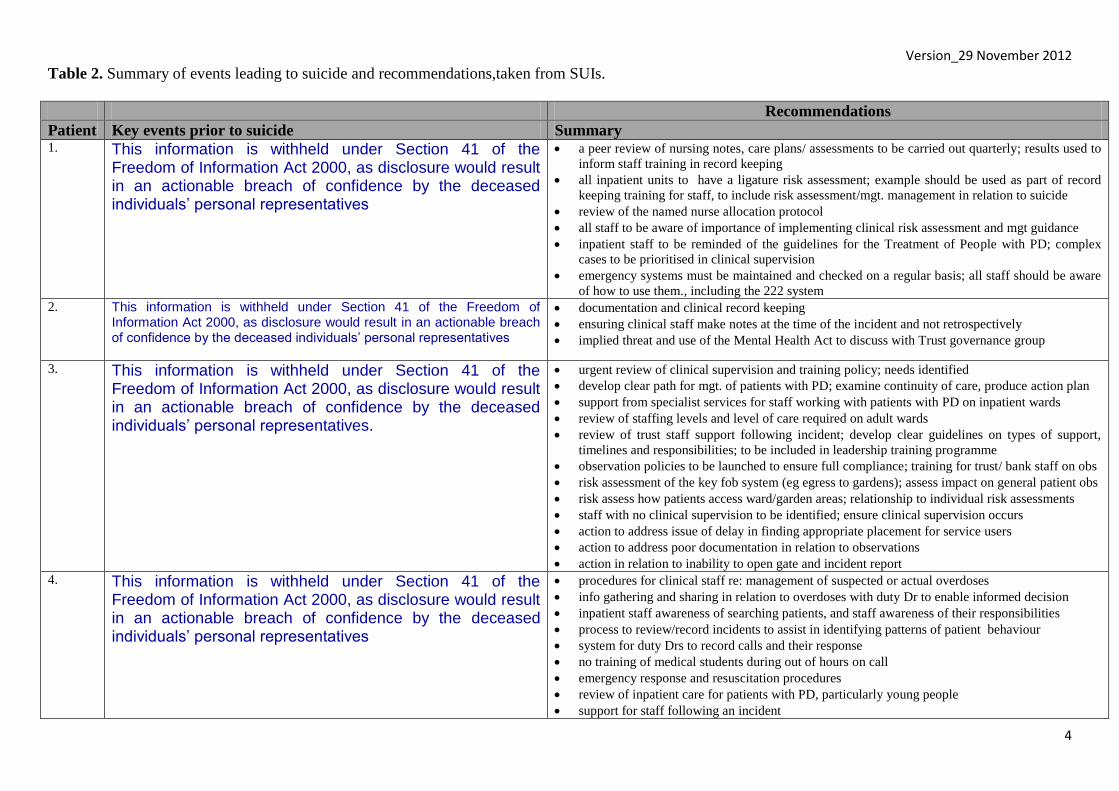
Table 2. Summary of events leading to suicide and recommendations,taken from SUIs.
Recommendations
Patient Key events prior to suicide Summary 1. This information is withheld under Section 41 of the
Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives
a peer review of nursing notes, care plans/ assessments to be carried out quarterly; results used to
inform staff training in record keeping
all inpatient units to have a ligature risk assessment; example should be used as part of record
keeping training for staff, to include risk assessment/mgt. management in relation to suicide
review of the named nurse allocation protocol
all staff to be aware of importance of implementing clinical risk assessment and mgt guidance
inpatient staff to be reminded of the guidelines for the Treatment of People with PD; complex
cases to be prioritised in clinical supervision
emergency systems must be maintained and checked on a regular basis; all staff should be aware
of how to use them., including the 222 system 2. This information is withheld under Section 41 of the Freedom of
Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives
documentation and clinical record keeping
ensuring clinical staff make notes at the time of the incident and not retrospectively
implied threat and use of the Mental Health Act to discuss with Trust governance group
3. This information is withheld under Section 41 of the Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives.
urgent review of clinical supervision and training policy; needs identified
develop clear path for mgt. of patients with PD; examine continuity of care, produce action plan
support from specialist services for staff working with patients with PD on inpatient wards
review of staffing levels and level of care required on adult wards
review of trust staff support following incident; develop clear guidelines on types of support,
timelines and responsibilities; to be included in leadership training programme
observation policies to be launched to ensure full compliance; training for trust/ bank staff on obs
risk assessment of the key fob system (eg egress to gardens); assess impact on general patient obs
risk assess how patients access ward/garden areas; relationship to individual risk assessments
staff with no clinical supervision to be identified; ensure clinical supervision occurs
action to address issue of delay in finding appropriate placement for service users
action to address poor documentation in relation to observations
action in relation to inability to open gate and incident report
4. This information is withheld under Section 41 of the Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives
procedures for clinical staff re: management of suspected or actual overdoses
info gathering and sharing in relation to overdoses with duty Dr to enable informed decision
inpatient staff awareness of searching patients, and staff awareness of their responsibilities
process to review/record incidents to assist in identifying patterns of patient behaviour
system for duty Drs to record calls and their response
no training of medical students during out of hours on call
emergency response and resuscitation procedures
review of inpatient care for patients with PD, particularly young people
support for staff following an incident

Version_29 November 2012
5
Table 2 (cont’d). Summary of events leading to suicide and recommendations,taken from SUIs.
Recommendations
Patient Key events prior to suicide Summary 5. This information is withheld under Section 41 of the
Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives
ensure clear policies in place for escorting & observing patients
procedures for identifying nurse in charge; ensure same procedure across the unit
ensure qualified staff understand their accountability and responsibility in delegating duties
formal review of the qualified nurses and OTs involved
identify competencies required for Bank staff/ support workers; robust induction processes
ensure OT team take responsibility in monitoring patients and their needs; procedures in place to
share information even if OT working part-time; OT procedures to receive patients appropriately
revised round documentation is shared across adult mental health; share good practice
ensure risk management/plans documented and shared
6. This information is withheld under Section 41 of the Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives
fill vacancies and gaps in provision of psychological therapies/occupational therapies; increase
capacity and opportunities for engagement
documentation for different levels of observation to be kept in separate folders (e.g. 10, 15 min obs)
scenario based training to support staff; levels of staff confidence in assessing risk to be reviewed
procedures for identifying nurse in charge
complete formal review of staff involved in case
routine planned clinical supervision to discuss complex clinical decision making
nurse in charge to be responsible for written documentation of handover so all staff are aware of the
content of the handover even if handover not attended
named nurse to be articulated within standard operating procedures for ward
7 This information is withheld under Section 41 of the Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives
risk assessment (leave feedback to be obtained from carers/relatives following return to ward,
assessments of risk/ rationale for decision making must be documented in clinical notes, document
indicators of increased risk; verbally hand over to admitting staff to record)
communication (clear explanations to families/carers, protocols for communication between
services with link person identified, wards to use standardised networking sheet)
record keeping (physical assess. done w/in 24 hours of admission; named nurse to ensure paperwork
completed, assess. checklists updated, CPA paperwork to be completed by all involved clinicians
access to services (standard set and monitored for maximum number of days for reallocation of a
patient to an alternative CPN, standard set for following up psychology referrals).
8. This information is withheld under Section 41 of the Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives
staff to be aware of responsibility for following all trust policies (e.g. observation, risk assessment,
record keeping) and consequences of failure to do so
develop standard procedure for handovers; ensure timely, accurate handover
acute inpatient staff to know observation policy; understand level of responsibility when making
decisions in relation to the delegation of observations and in carrying out observation
a review of AMH acute inpatient SOP; responsibility of nurse in charge when handing over the shift
disciplinary procedures for staff involved in case, where appropriate
review by duty doctor of any patient leaving the ward w/out permission; risk levels updated
Version_29 November 2012
6
COMPARISONS BASED ON NCI DATA
Suicide numbers
We know from NCI and other national data that in recent years just under one suicide
on average occurs annually for every 10,000 general population, that 25% of people
dying by suicide are current or recent mental health patients and that 13% of these are
current inpatients. This allows a crude calculation of the expected numbers of
inpatient suicides in LPT.
The trust covers a population of just under 1 million people. This translates into
around 80-90 suicides per year in the general population, 800-900 over the most
recent 10-year period for which the NCI has comprehensive figures, i.e. 2000-2009.
Of these, 200-225 should be mental health patients of whom 26-29 should be
inpatients. The actual figures known to the NCI are 211 patients and 29 inpatients.
Inpatients are 14% of all patient suicides.
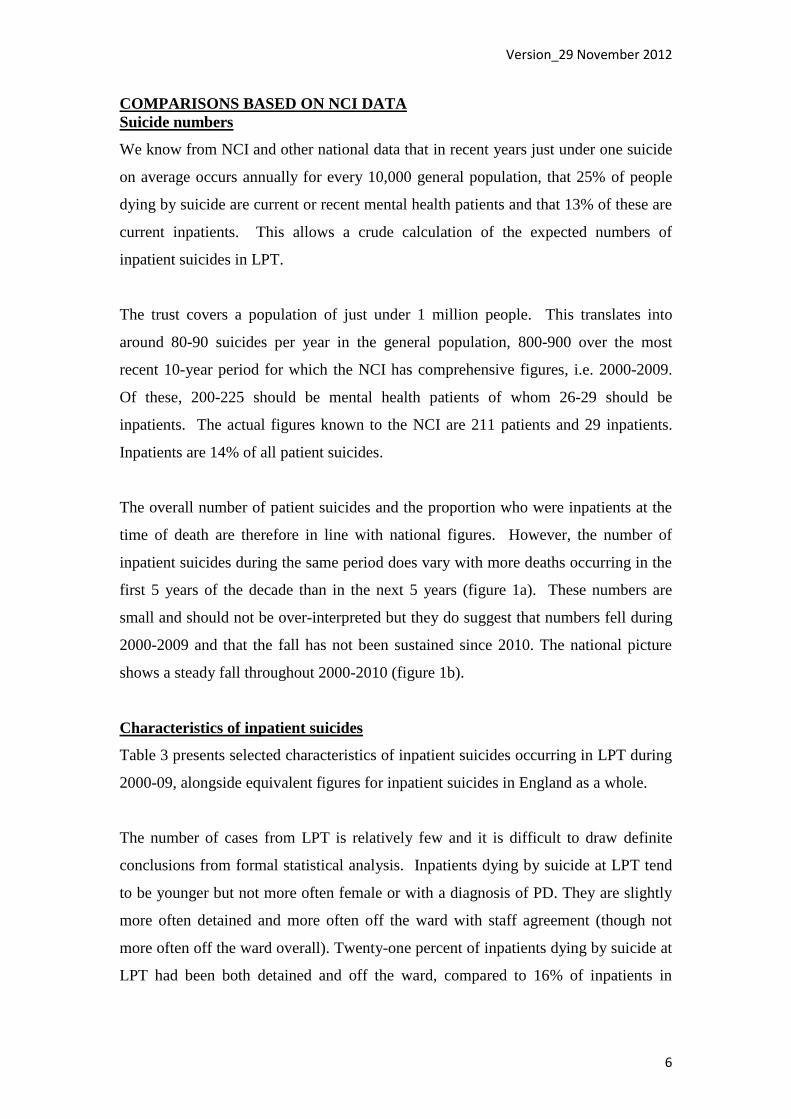
The overall number of patient suicides and the proportion who were inpatients at the
time of death are therefore in line with national figures. However, the number of
inpatient suicides during the same period does vary with more deaths occurring in the
first 5 years of the decade than in the next 5 years (figure 1a). These numbers are
small and should not be over-interpreted but they do suggest that numbers fell during
2000-2009 and that the fall has not been sustained since 2010. The national picture
shows a steady fall throughout 2000-2010 (figure 1b).
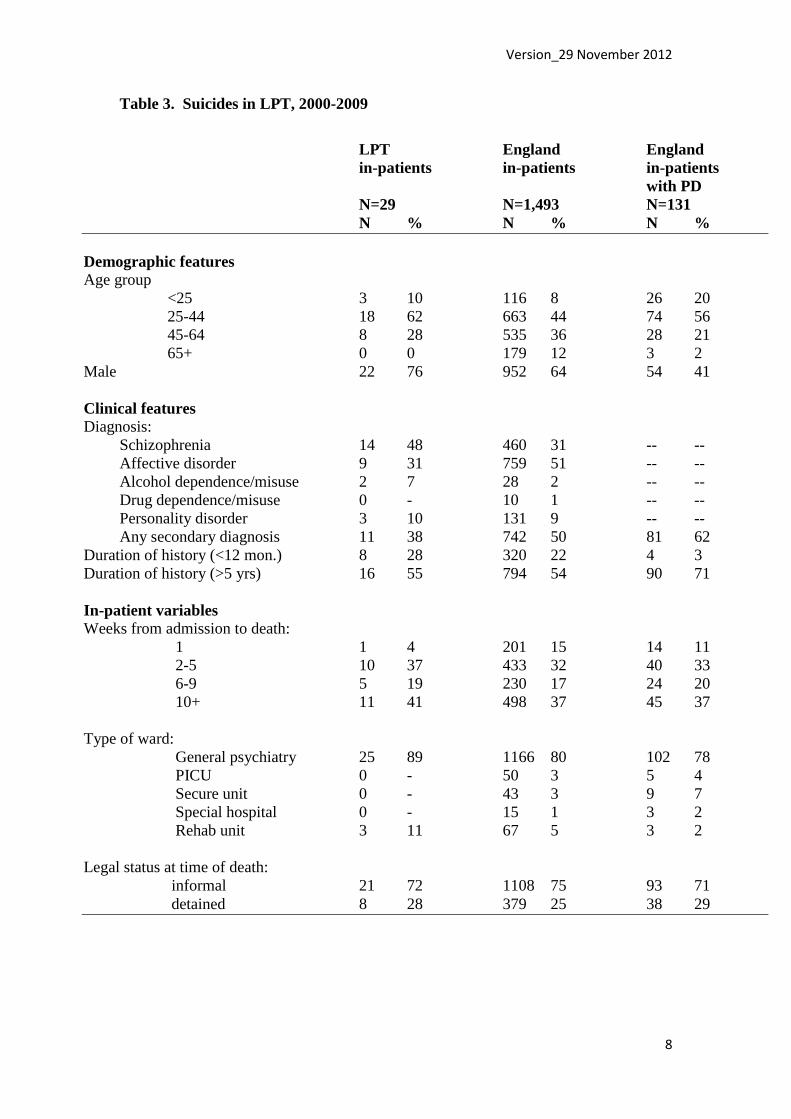
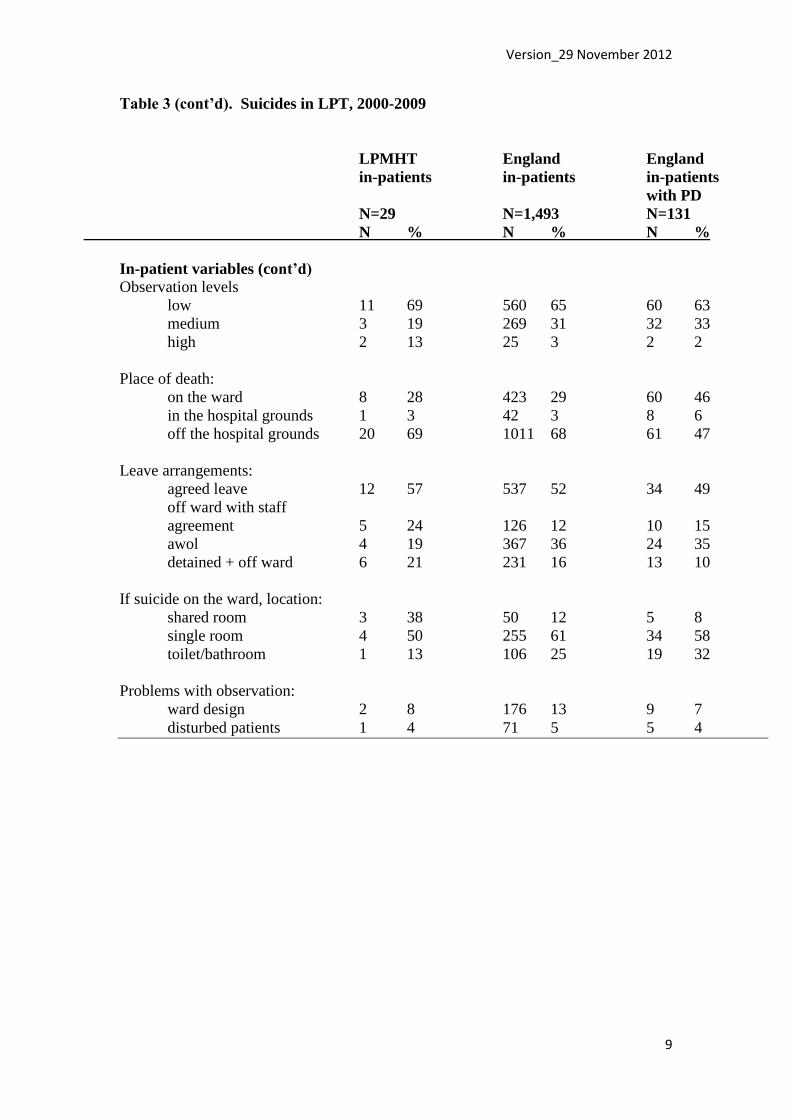
Characteristics of inpatient suicides
Table 3 presents selected characteristics of inpatient suicides occurring in LPT during
2000-09, alongside equivalent figures for inpatient suicides in England as a whole.
The number of cases from LPT is relatively few and it is difficult to draw definite
conclusions from formal statistical analysis. Inpatients dying by suicide at LPT tend
to be younger but not more often female or with a diagnosis of PD. They are slightly
more often detained and more often off the ward with staff agreement (though not
more often off the ward overall). Twenty-one percent of inpatients dying by suicide at
LPT had been both detained and off the ward, compared to 16% of inpatients in
Version_29 November 2012
7
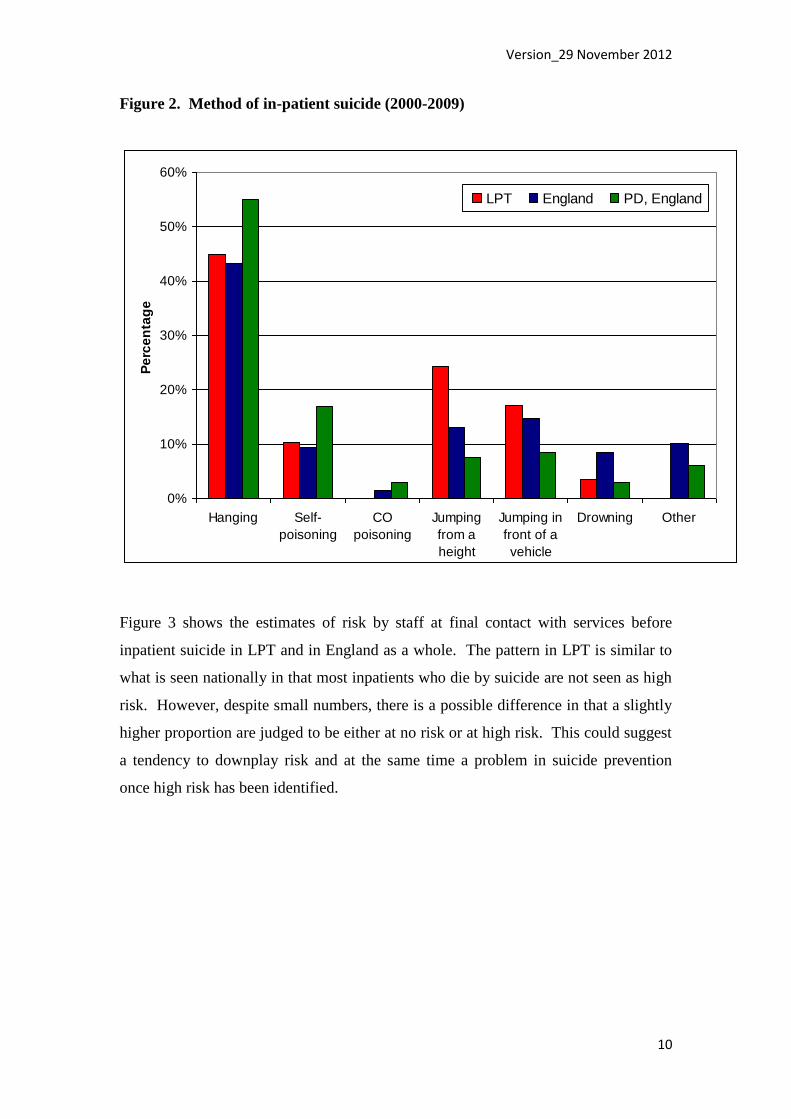
England. Method of suicide is presented in figure 2. There are more deaths by
jumping from a height, a method associated with being off the ward.
Figure 1. Number of in-patient suicides in LPT (2000-2012) and England (2000-
2010)
a)
0
1
2
3
4
5
6
7
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
Fre
qu
en
cy
LPT in-patient suicides
Note. Figures for 2010-12 are the 8 inpatient suicides notified to the NCI as part of this review.
b)
0
50
100
150
200
250
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Fre
qu
en
cy
In-patient suicides; England
Note. Figures for 2010-12 unavailable. Source: Annual Report, 2012
Version_29 November 2012
8
Table 3. Suicides in LPT, 2000-2009
LPT England England
in-patients in-patients in-patients
with PD
N=29 N=1,493 N=131
N % N % N %
Demographic features Age group
<25 3 10 116 8 26 20
25-44 18 62 663 44 74 56
45-64 8 28 535 36 28 21
65+ 0 0 179 12 3 2
Male 22 76 952 64 54 41
Clinical features Diagnosis:
Schizophrenia 14 48 460 31 -- --
Affective disorder 9 31 759 51 -- --
Alcohol dependence/misuse 2 7 28 2 -- --
Drug dependence/misuse 0 - 10 1 -- --
Personality disorder 3 10 131 9 -- --
Any secondary diagnosis 11 38 742 50 81 62
Duration of history (<12 mon.) 8 28 320 22 4 3
Duration of history (>5 yrs) 16 55 794 54 90 71
In-patient variables Weeks from admission to death:
1 1 4 201 15 14 11
2-5 10 37 433 32 40 33
6-9 5 19 230 17 24 20
10+ 11 41 498 37 45 37
Type of ward:
General psychiatry 25 89 1166 80 102 78
PICU 0 - 50 3 5 4
Secure unit 0 - 43 3 9 7
Special hospital 0 - 15 1 3 2
Rehab unit 3 11 67 5 3 2
Legal status at time of death:
informal 21 72 1108 75 93 71
detained 8 28 379 25 38 29
Version_29 November 2012
9
Table 3 (cont’d). Suicides in LPT, 2000-2009
LPMHT England England
in-patients in-patients in-patients
with PD
N=29 N=1,493 N=131
N % N % N %
In-patient variables (cont’d) Observation levels
low 11 69 560 65 60 63
medium 3 19 269 31 32 33
high 2 13 25 3 2 2
Place of death:
on the ward 8 28 423 29 60 46
in the hospital grounds 1 3 42 3 8 6
off the hospital grounds 20 69 1011 68 61 47
Leave arrangements:
agreed leave 12 57 537 52 34 49
off ward with staff
agreement 5 24 126 12 10 15
awol 4 19 367 36 24 35
detained + off ward 6 21 231 16 13 10
If suicide on the ward, location:
shared room 3 38 50 12 5 8
single room 4 50 255 61 34 58
toilet/bathroom 1 13 106 25 19 32
Problems with observation:
ward design 2 8 176 13 9 7
disturbed patients 1 4 71 5 5 4
Version_29 November 2012
10
Figure 2. Method of in-patient suicide (2000-2009)
0%
10%
20%
30%
40%
50%
60%
Hanging Self-
poisoning
CO
poisoning
Jumping
from a
height
Jumping in
front of a
vehicle
Drowning Other
Pe
rce
nta
ge
LPT England PD, England
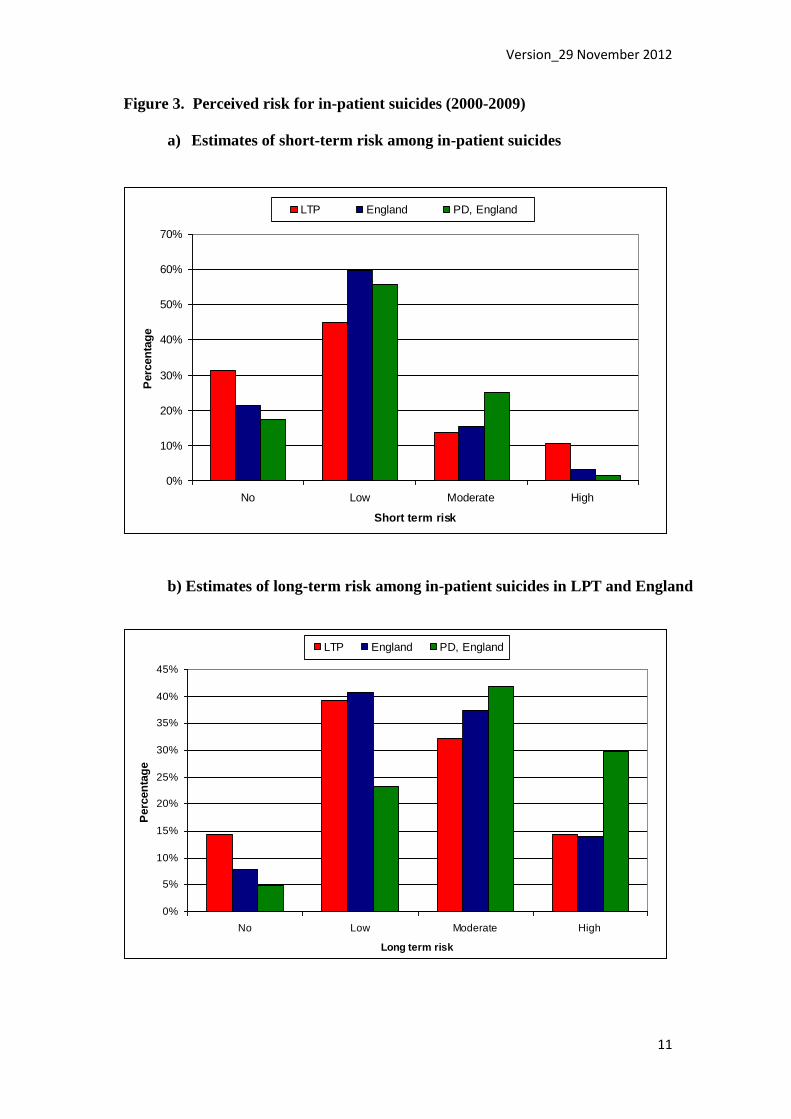
Figure 3 shows the estimates of risk by staff at final contact with services before
inpatient suicide in LPT and in England as a whole. The pattern in LPT is similar to
what is seen nationally in that most inpatients who die by suicide are not seen as high
risk. However, despite small numbers, there is a possible difference in that a slightly
higher proportion are judged to be either at no risk or at high risk. This could suggest
a tendency to downplay risk and at the same time a problem in suicide prevention
once high risk has been identified.
Version_29 November 2012
11
Figure 3. Perceived risk for in-patient suicides (2000-2009)
a) Estimates of short-term risk among in-patient suicides
0%
10%
20%
30%
40%
50%
60%
70%
No Low Moderate High
Short term risk
Perc
en
tag
e
LTP England PD, England
b) Estimates of long-term risk among in-patient suicides in LPT and England
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
No Low Moderate High
Long term risk
Perc
en
tag
e
LTP England PD, England
Version_29 November 2012
12
KEY THEMES FOR SUICIDE PREVENTION
The following section is based on our reading of the SUI reports and our discussions
with senior clinical and service management staff. It is an overview of the key themes
relevant to suicide prevention that these eight cases raise rather than a list of the
problems in the SUI reports themselves. These are the areas that should be
highlighted in future actions on prevention.
1. The role of specific errors
In examining patient suicides it is common to find that no single action or omission
leads directly to a death. Instead, a number of actions contribute but only because
they occur in combination. The LPT cases are unusual in that five of the eight feature
specific actions or omissions that almost certainly contributed directly to the death.
These are:
This information is withheld under Section 41 of the Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives.
It is not part of our remit to highlight individual blame. Errors are often made by the
most skilled and experienced staff and need to be understood if deaths are to be
prevented.
Clearly it is important that LPT takes steps to make errors of this kind less likely in
the future. This report considers the issues of risk recognition, observation and
communication as further themes below.
However, it is also important to assume that errors will still occur – we are dealing
with a human system. The question then for LPT is whether there are sufficient safety
nets to prevent suicides when errors happen. This is not complacency about errors. It
reflects a comprehensive approach to risk management.
2. Risk recognition
In several of the cases it seems that clear indications of suicide risk were not
recognised. For example, (This information is withheld under Section 41 of the Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individuals’ personal representatives).
Version_29 November 2012
13
Judgments of this kind, second-guessing the true intentions of people in severe
emotional disturbance, can be dangerous.
Our concern is the possibility that it is a feature of clinical practice at LPT to under-
estimate or downplay risk. This is not possible for us to say with certainty, given that
we have done no more than review SUI reports and visit the unit for one day.
However, it would be consistent with the way staff responded to clear warning signs
in some cases, the errors described above, the judgements about risk in figure 3, and
our data on being off the ward while detained. This would be a sufficiently serious
matter for the trust to take action now on the partial evidence that we have put
forward. Even so, if there was something more serious at LPT, i.e. a pervasive
problem of complacency about risk, then the number of suicides would be higher – we
have not found this.
Clinicians sometimes feel that risk is overplayed by service managers, as well as by
governments, at the expense of broader aspects of the quality of care. This is because
it can seem that a concern with risk equates to a desire for measures of physical
security (eg locked doors) and unproven assessment methods such as risk factor
checklists. Clinicians are right to be sceptical about this: risk is not a number and risk
assessment is not a checklist. Good risk management and high quality care are two
sides of the same approach. When we say that greater emphasis needs to be placed on
the recognition of risk, we are not only referring to picking up warning signs. We are
also talking about improving the therapeutic atmosphere on inpatient units, ensuring
the availability of psychological therapies that engage a patient and aim to understand
their distress, and leadership in maintaining vigilance when patients seem to be
improving.
3. Management of personality disorder
These difficulties in risk recognition are more likely to occur with patients whose
diagnosis is personality disorder, as in four of the LPT cases. Risk management,
although never easy, follows a more predictable path during the treatment of severe
depression or psychosis. Personality disorder, particularly when it is severe enough to
need admission, can follow a more turbulent process of recovery with frequent
setbacks, a less predictable response to treatment, and at times problems in the
Version_29 November 2012
14
relationship between patient and staff. Threats of self-harm may occur as part of a
pattern of challenging behaviour and can seem deliberate rather than genuinely
suicidal.
Characteristics of PD inpatients nationally who die by suicide are presented in table 3.
Compared to inpatient suicides as a whole, they tend to be younger and more often
female. They more often die on the ward and by overdose. They are seen by staff as at
higher long-term but not short-term risk (figure 3).
LPT is developing expertise in the management of personality disorder, including as
inpatients. Some of the points made above, about managing risk through improving
ward milieu, psychological therapies and leadership apply particularly to the care of
PD inpatients.
4. Specific issues
In addition to these overall themes, there are specific areas of practice that need to be
improved to enhance safety. These are:
a) Ligature points
During our visit, it was clear that room doors could still be used for the attachment of
ligatures such as sheets and towels – this method featured in the cases we reviewed.
b) Communicating risk
In some cases there were lapses in passing on information important to the
management of risk. This was most obvious in case 6, in which sheets were handed
back to a patient who had previously used sheets as a ligature, and in case 8 (This information is withheld under Section 41 of the Freedom of Information Act 2000, as disclosure would result in an actionable breach of confidence by the deceased individual’s personal representative) There is a recurring theme that
the degree of risk is not clearly agreed, understood or communicated between staff.
c) Escort, observation and leave
A number of the cases featured lapses of escort or observation protocols. In others,
staff agreed to ward leave for patients who were being held under MH Act powers. It
can be difficult to get the balance right during recovery between helping a patient take
steps towards returning home and ensuring that they are protected from the stresses

Version_29 November 2012
15
they may return to. However, it is important that staff are aware that periods of
apparent recovery, when restrictions are being relaxed in preparation for discharge,
are generally the times of highest risk, and that trust protocols lead to rigorous care
planning at these times.
RECOMMENDATIONS
We have identified a number of unchecked errors, a possible clinical tendency to
under-estimate risk and a need to tighten procedures and protocols in the care of
inpatients. We think LPT are to be commended for their willingness to further
investigate and learn lessons from the inpatient suicide deaths that occurred during
2010-2012, in order to change the way in which services are delivered. We
understand that the trust is already removing potential ligature points from existing
wards following our visit on 23 October, and making changes to the design of the
ward currently being built. The staff we have met are all experienced and
conscientious - their expertise should provide the foundation for improving the risk
management culture at LPT.
1. Preventing errors and providing safety nets
The SUI reports and this review set out ways in which the errors that occurred in five
of the cases could in future be prevented. In addition we recommend that LPT should
consider what safety net measures are needed to prevent the consequences of such
errors if they recur. It would be a serious matter if a future death followed an identical
error. The question for LPT is whether the same errors would now be contained – if
not, new safety mechanisms are needed.
For example, decisions on medical transfer following overdose could be
countersigned by a senior clinician rather than left to junior or ward staff. Counting
the presence of patients on the ward could be double-checked, including by the key
nurse for each patient.
2. Risk recognition
We believe that the skill and experience of LPT senior clinical staff are a key resource
in overcoming a possible culture of under-estimating or downplaying risk. We
recommend that:
Version_29 November 2012
16
senior staff should meet to agree the practice and training needs of all ward staff in
the recognition and management of risk, based on the content of this report and
our seminar on 29 November;
they should pay particular attention to how ward staff respond to suicidal actions,
how to assess risk for patients going off the ward or on leave, how to conduct
observation and escort protocols, and how to achieve a therapeutic ward milieu;
and,
senior staff should set an example in risk recognition, ensuring that less
experienced staff are sufficiently vigilant.
3. Personality disorder
Most of these measures to improve risk recognition are required in particular for
personality disorder patients; protocols and training should reflect this. In developing
expertise in the care of people with PD, the trust should:
ensure that there is adequate inpatient provision of therapies used to treat PD;
that the PD service is a resource to general wards; and,
that there is sufficient support for all staff who are engaged in the care of this
demanding patient group.
4. Ligature points
Each ward should conduct a further review of potential ligature points. We suggest
that senior staff from one ward review the physical risks on another ward.
5. Protocols and procedures
The trust should strengthen formal procedures for:
recording and communicating risk among ward staff;
assessing risk as part of care planning before leave is agreed for detained patients;
carrying out observations and confirming the presence of patients on the ward;
and,
confirming the hand over of patients under escort.
Version_29 November 2012
17
In strengthening these procedures and making them more formal, LPT should
introduce cross-checking protocols and ensure that senior staff oversee these.
REFERENCE
National Confidential Inquiry into Suicide and Homicide by People with Mental Illness,
Annual Report, 2012,
(http://www.medicine.manchester.ac.uk/cmhr/centreforsuicideprevention/nci/reports/a
nnual_report_2012.pdf)
Recommended









![Psychopathic Suicides [solo cello]](https://img.pdfslide.us/doc/110x75/577cdb691a28ab9e78a81e65/psychopathic-suicides-solo-cello.jpg)