Reducing Avoidable Readmissions: The Business and Clinical Impact of Palliative Care
Susan Enguidanos, PhD, MPH
Agenda
• Introduction to & Need for Palliative Care• Evidence of Palliative Care Effectiveness
• Examples of Two Models of Palliative Care:• Inpatient (Hospital-based)• Home-based
• Palliative Care and 30-day Readmissions
• Getting Started

Introduction to Palliative Care
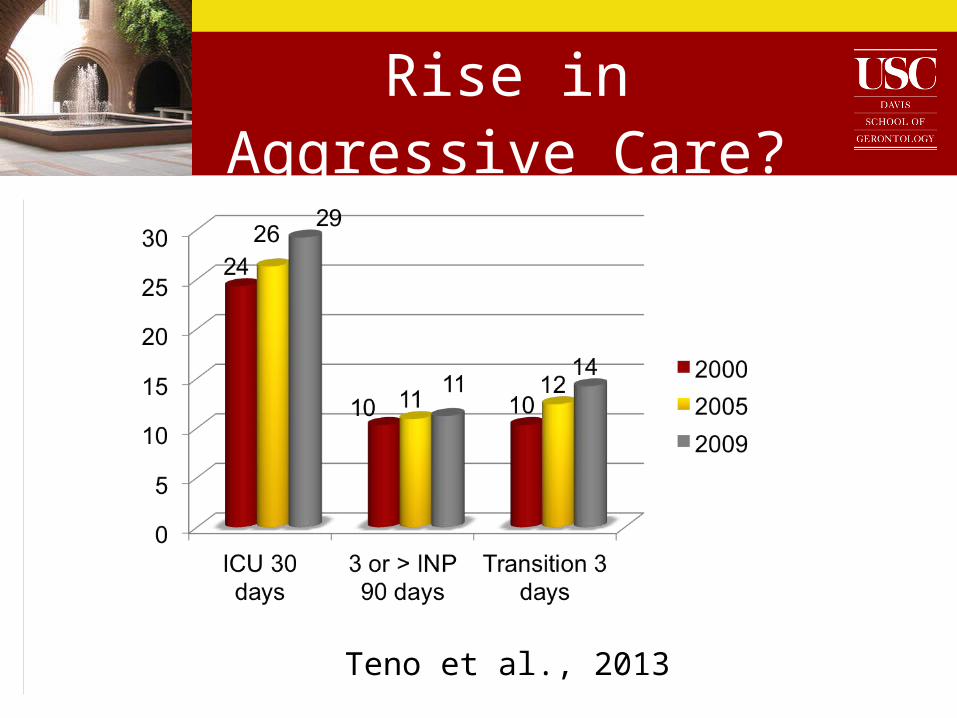
Rise in Aggressive Care?
Teno et al., 2013

65+ Medicare Beneficiaries ICU Use
(Riley & Lubitz, 2010)
Background: Patient & Family Need
Current dying experience is far from one that is desired by most Americans
• Majority of Americans prefer to die at home(Hays et al., 2001; Gallup, 2000)•33.5% die at home (2009; Teno et al., 2013)
• Patients continue to die in pain (Meier, 2006)
• 46% of Do Not Resuscitate orders written within 2 days of death
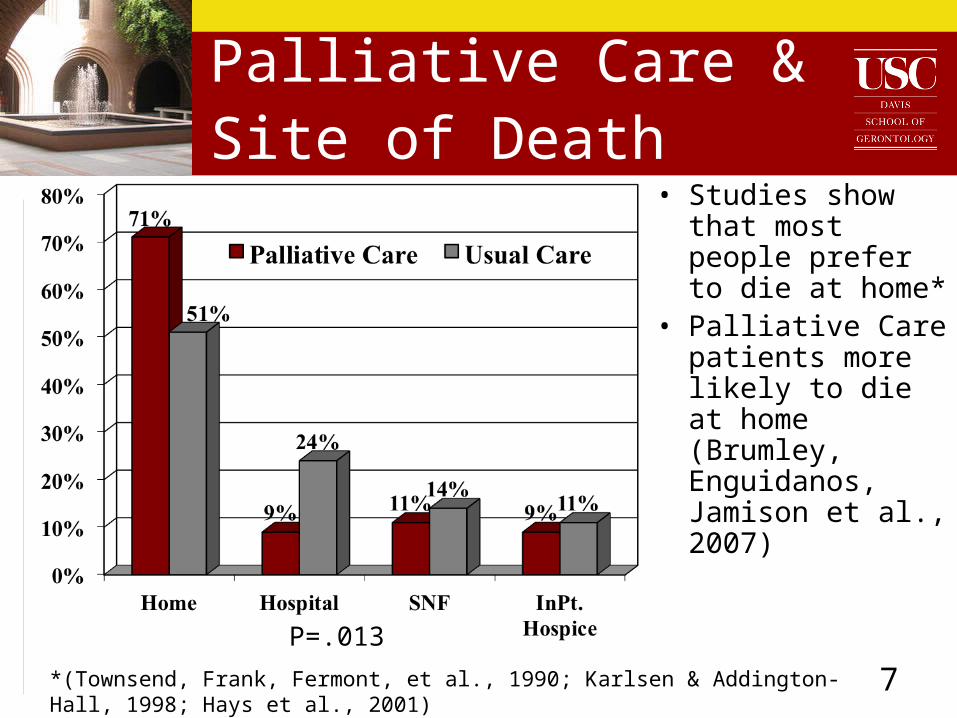
Palliative Care & Site of Death
• Studies show that most people prefer to die at home*
• Palliative Care patients more likely to die at home (Brumley, Enguidanos, Jamison et al., 2007)
*(Townsend, Frank, Fermont, et al., 1990; Karlsen & Addington-Hall, 1998; Hays et al., 2001)
P=.013
7

What is Palliative Care?
Goal:“…to prevent and relieve suffering & to support the best possible quality of life for patients & their families, regardless of the stage of the disease or the need for other therapies.”
What Palliative Care Does:“Expands traditional disease-model medical treatments to include the goals of enhancing quality of life for patient & family, optimizing function, helping with decision making, & providing opportunities for personal growth.”
National Consensus Project for Quality Palliative Care, 2013
9
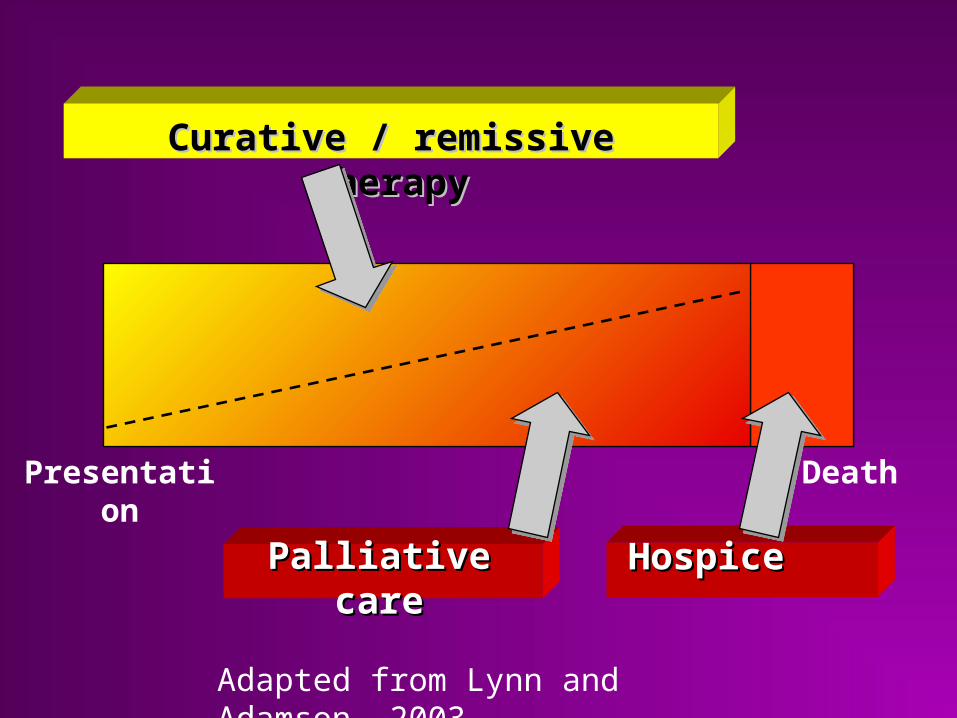
HospiceHospicePalliativePalliative carecare
Curative / remissive therapyCurative / remissive therapy
Presentation Death
Adapted from Lynn and Adamson, 2003

10
Core Components of Palliative Care
• Interdisciplinary team: MD, RN, SW, Chaplain • Physical, medical, psychological,
social & spiritual support• Patient & family education & training
• Develop plan of care• Coordinated, patient-centered care
11
• Pain & symptom management• comprehensive primary care to
manage underlying conditions
• Aggressive treatment of acute exacerbation per patient and family request
• Facilitates transfer to hospice if appropriate
Core Components of Palliative Care
12
Palliative Care Models
Hospital-based, Inpatient Palliative
Care Programs
Home-based Palliative Care
Inpatient Palliative Care (IPC)
• Consultative IPC service involves family meeting with patients/family
• Follow-up care as needed
13

Home-based Palliative Care
• Eligibility
• Diagnosis of congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), or cancer
• Life expectancy about 1 year• Primary care physician “would not be surprised” if the
patient died in the next year
• Palliative Care (PC)• Multiple home visits provided by
interdisciplinary palliative team • Access to all usual medical care services
Palliative Care vs. Hospice
Physicians not required to give a 6 month prognosis
Patients do not have to forego curative care
Palliative care physician coordinates care to prevent service fragmentation
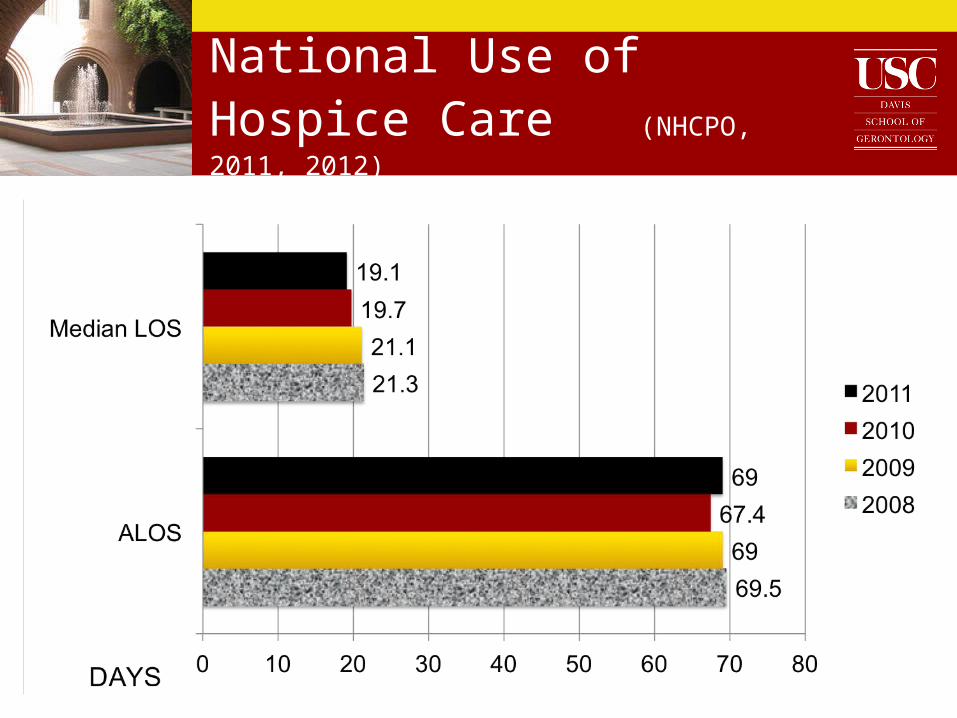
National Use of Hospice Care (NHCPO, 2011, 2012)
Clinical and Economic Impact of Palliative Care
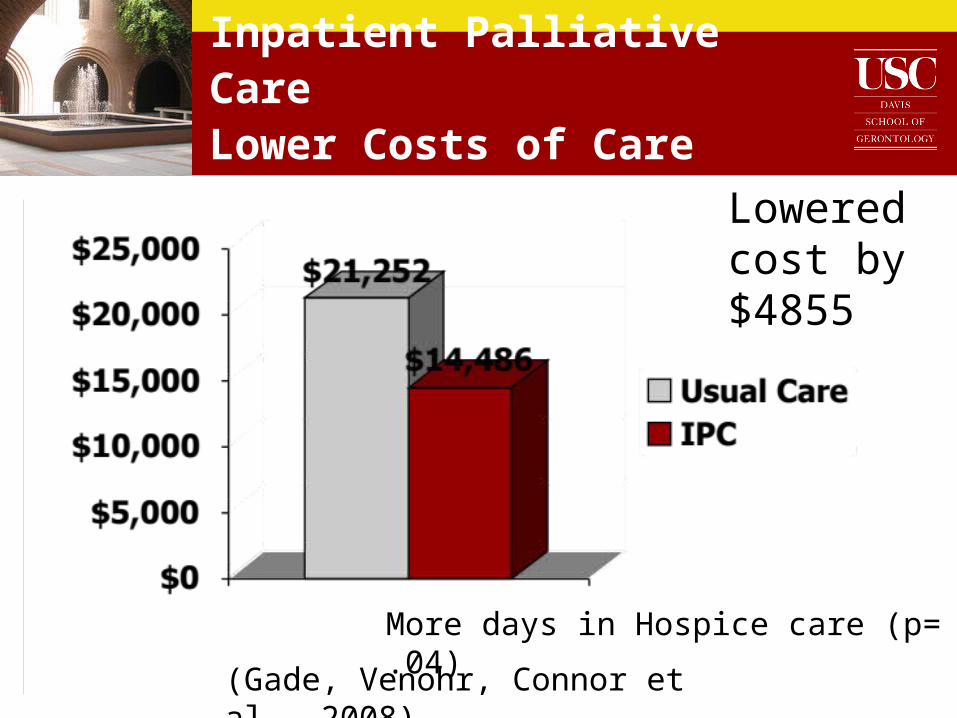
Inpatient Palliative CareLower Costs of Care
Lowered cost by $4855
(Gade, Venohr, Connor et al., 2008)
More days in Hospice care (p= .04)

Fewer ICU Admissions at Readmission (IPC)
(Gade, Venohr, Connor et al., 2008)
Other IPC Evidence(Morrison et al., 2008)
• Comparison Group Study
• IPC patients discharged had savings of $1696 in direct costs per admission (p=.004)• $279 in direct costs per day (p<.001)
• IPC patients who died had savings of $4908 in direct costs per admission (p=.003)• $374 in direct costs per day (p<.001)

The Economic and Clinical Impact of IPC
• Mean daily costs for IPC patients
• 33% (p< .01) pre- to post-intervention
• 14.5% compared to usual care (p< .01)
• LOS 30%
• Pain by 86%
• Dyspnea by 64%
(Ciemins, Blum, Nunley, Lasher, Newman, 2007).
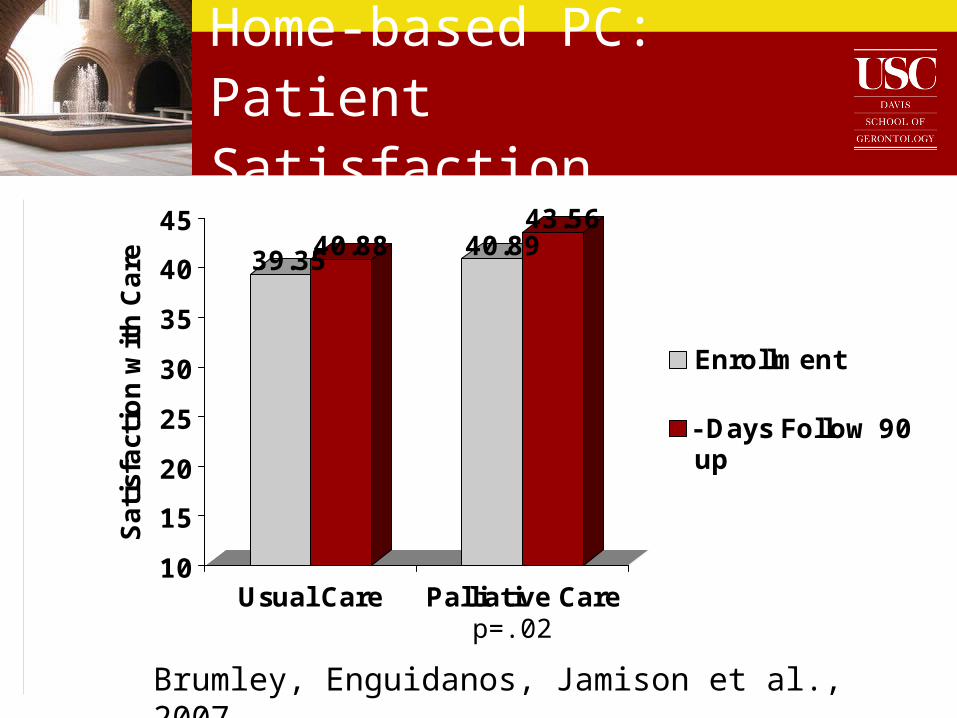
Home-based PC: Patient Satisfaction
39.3540.88 40.8943.56
10
15
20
25
30
35
40
45
Sati
sfact
ion w
ith C
are
Usual Care Palliative Care
Enrollment
-Days Follow 90up
Brumley, Enguidanos, Jamison et al., 2007
p=.02
23
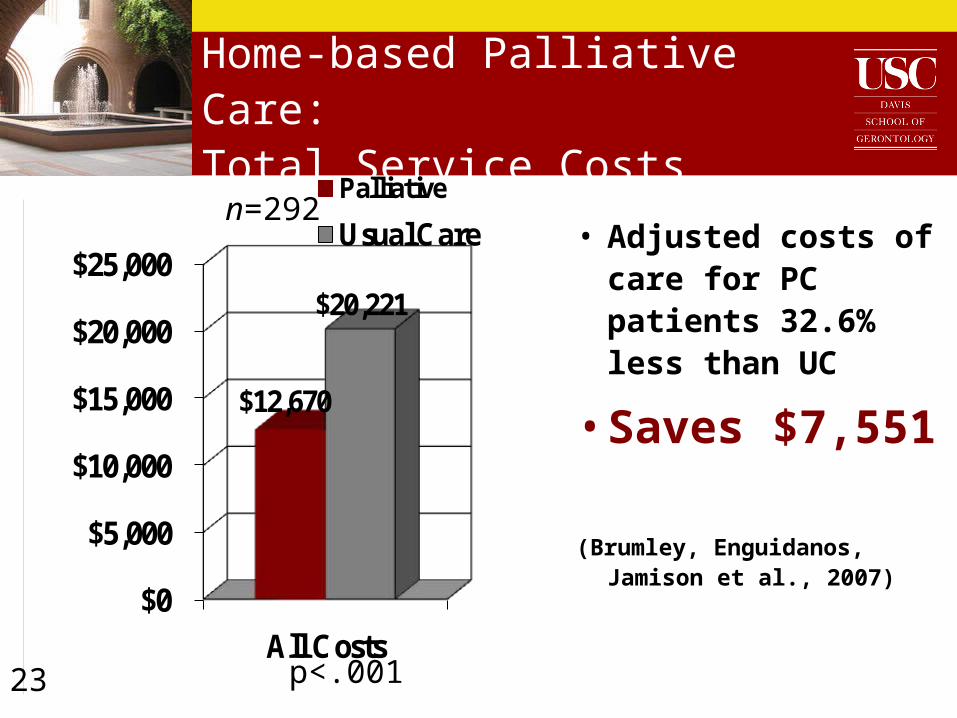
Home-based Palliative Care:Total Service Costs
$0
$5,000
$10,000
$15,000
$20,000
$25,000
All Costs
$12,670
$20,221
Palliative
Usual Care • Adjusted costs of care for PC patients 32.6% less than UC
• Saves $7,551
(Brumley, Enguidanos, Jamison et al., 2007)
p<.001
n=292
Brumley, Enguidanos, Jamison et al., 2007
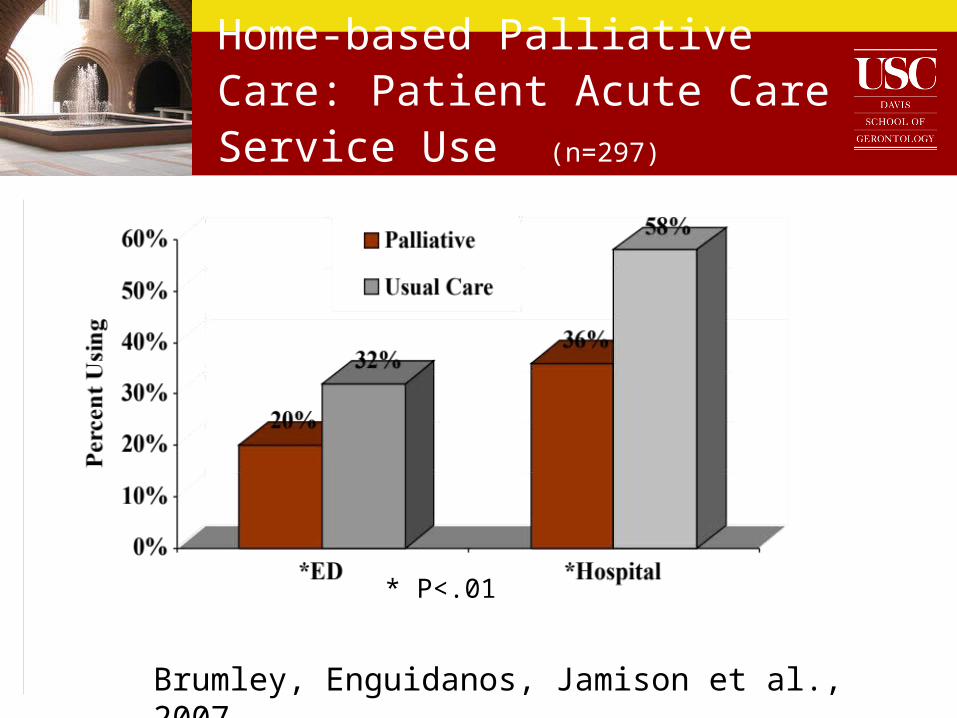
Home-based Palliative Care: Patient Acute Care Service Use (n=297)
* P<.01
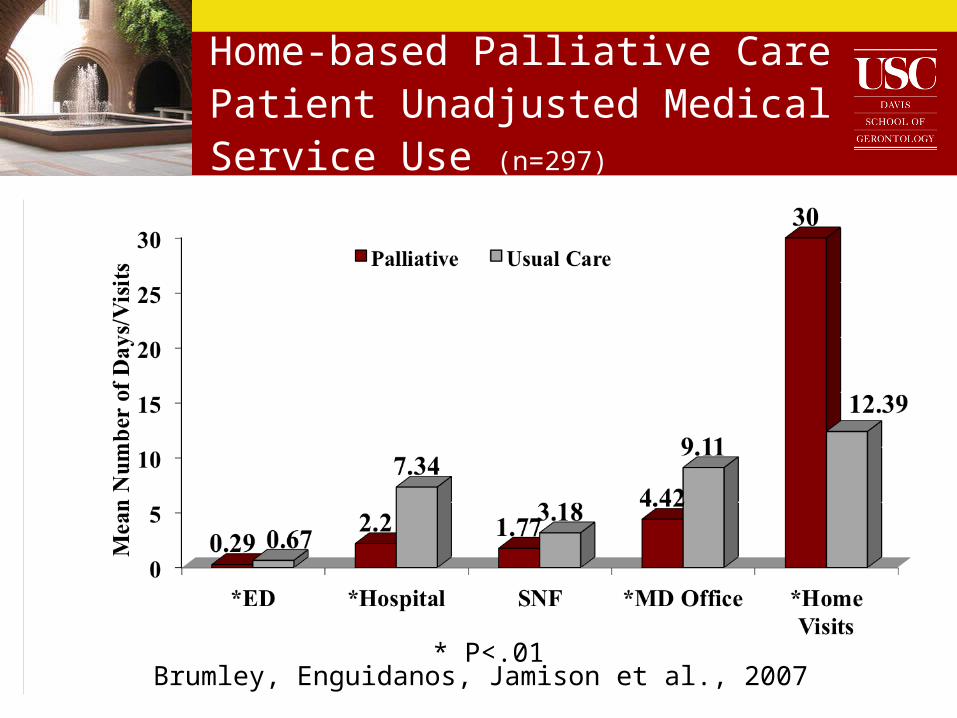
Home-based Palliative Care Patient Unadjusted Medical Service Use (n=297)
* P<.01Brumley, Enguidanos, Jamison et al., 2007
30-Day Readmission among Seriously Ill Older Adults: Why Do They Come Back?
Readmission Rates among IPC Patients• Among IPC patients discharged, overall
readmission rate = 10%
• Overall hospital readmission = 15%
• Reduced readmission by 1/3
Enguidanos, Vesper, & Lorenz (2012). 30 day readmissions among Seriously Ill Older Adults. Journal of Palliative Medicine, 1-6.
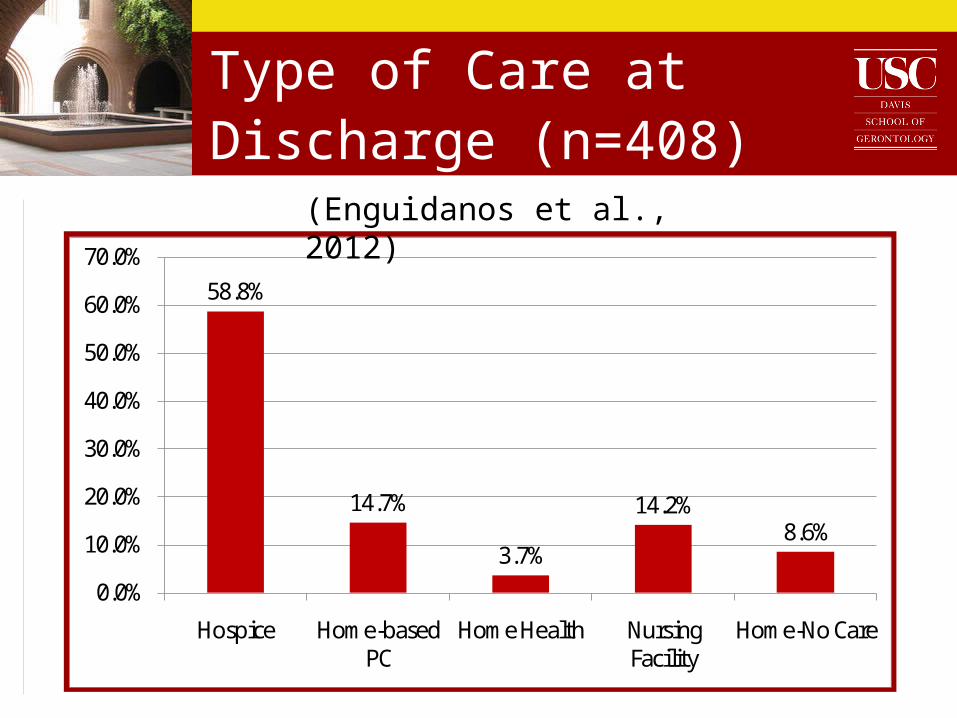
Type of Care at Discharge (n=408)
58.8%
14.7%
3.7%
14.2%8.6%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
Hospice Home-based PC
Home Health Nursing Facility
Home-No Care
(Enguidanos et al., 2012)
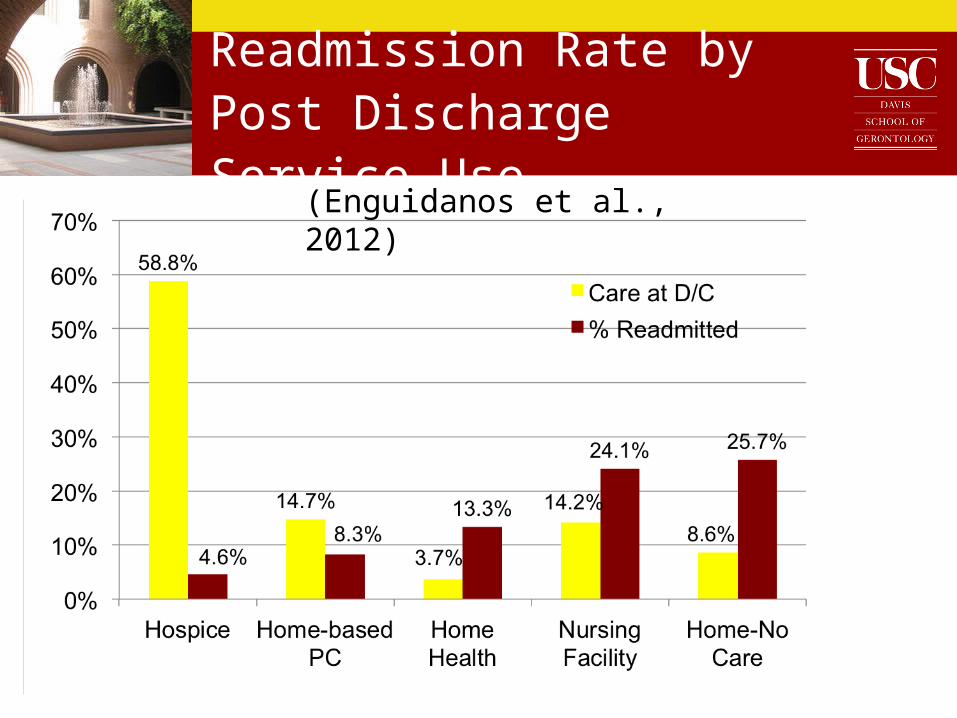
Readmission Rate by Post Discharge Service Use
(Enguidanos et al., 2012)
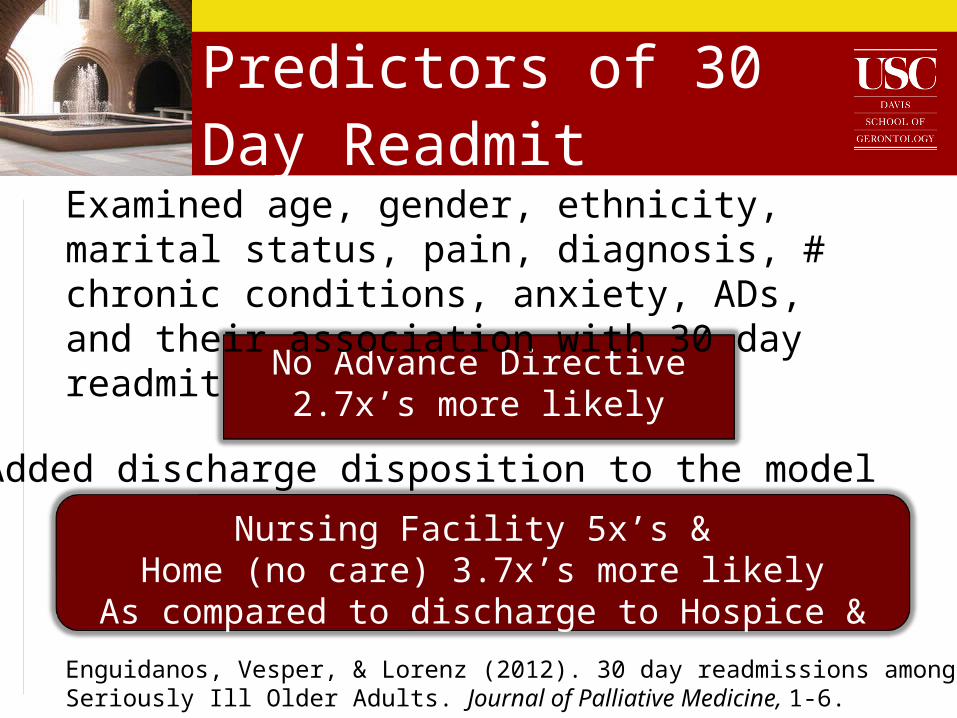
Predictors of 30 Day Readmit
No Advance Directive2.7x’s more likely
Nursing Facility 5x’s & Home (no care) 3.7x’s more likely
As compared to discharge to Hospice & HBPC
Enguidanos, Vesper, & Lorenz (2012). 30 day readmissions among Seriously Ill Older Adults. Journal of Palliative Medicine, 1-6.
Examined age, gender, ethnicity, marital status, pain, diagnosis, # chronic conditions, anxiety, ADs, and their association with 30 day readmit
Added discharge disposition to the model
Interviews with Seriously Ill 30-Day Readmits (n=10)
CHF & Cancer Patients
Three themes identified:
1. Lack of Support & Purpose
2. Rehospitalization as appropriate care
3. Lack of access to care/information

Theme: Lack of Support & Purpose
• Lack of support & purpose• Living alone and lack of support
• “I wasn’t cooking for myself, I wasn’t doing anything…I just wasn’t eating”
• “It’s just a matter of me …motivating me”
• “If there was something I could look forward to…”
Theme: Appropriate Care
• Hospital care most appropriate for medical condition and treatment preferences
“ I get to retaining the fluids again and then right back to where we were [hospital]”
• Preference for aggressive care
“ I ain’t going nowhere, and I’m fighting”

Theme: Lack of access to care/information
• “I should be comfortable. I shouldn’t have to go, ‘Oh, I got pain I need pain meds.’ I shouldn’t be going after pain medication…I was told I should come back to the ER to get my pain medicine.”
• “Sometimes I have questions”
• “I could have REALLY used a
hospital bed”
• Inability to physically transport spouse
to specialist appt
Discussion
• Limited access to holistic care• Enrollment in hospice and palliative care have
clear benefits, but problems getting there• Late referrals to hospice• Limited number of home-based palliative care• Most IPC referrals are late in the disease
trajectory• Too late to change the course of care or
improve quality
Discussion
• Lack of continuity problematic:
• Quality of life• Most people prefer to die at home.
Late transfers increase odds of death in hospital (Gonzalo, 2011).
• Care may not be consistent with wishes.
Getting Started
Building a Palliative Care Program
1. Making the Case for Palliative Care
2. Designing a Palliative Care Program
3. Financing a Palliative Care Program
4. Implementing a Palliative Care Program
5. Measuring Quality & Impact of Palliative Care Programs
Source: Center to Advance Palliative Carewww.capc.org

Making the Case:Benefits to Hospitals
• Lower costs for hospitals and payers• A systematic approach to caring for outlier
patients• Flexible programs support the primary care
physician• Meeting JCAHO Accreditation Standards• Easing burdens on staff and increasing staff
retention• Meeting the needs of an aging population
Source: Center to Advance Palliative Care
Components Needed for Success
• Strong Support from AdministrationGather internal/external evidence
• Program ChampionID within or locate (eg, AAHPM Membership)
• Palliative Care Training and MentoringCAPC, national leaders (eg, von Gunten)
• ClarityClearly identified goals/mission
• VisibilityCase finding, presentations, etc.
Source: Davis, Jamison, Brumley, & Enguidanos, 2006
Recommended

















