Embed Size (px)
Citation preview

NoCVA North CarolinaPreventing Avoidable
Readmissions Collaborative
Community Engagement and
CMS Reports Preview
November 8, 2012

How to Participate Today
• Use the Hand Icon to raise your hand, your line will then be unmuted
• Submit text questions through the Questions box

Oct 22 Submit med rec and handover communication data to QDS
Oct. 22 Team completes Team Assessment Tool and submit to QDS
Nov. 1 Test an improvement in the first two areas: assessment of post hospital needs and improve teaching and patient learning
Nov. 20 Submit med rec and handover communication data to QDS
Dec. – Jan. Begin community engagement assessment and mobilize community around Care Transitions
Dec. 20 Submit med rec and handover communication data to QDS
Jan. 1 Test an improvement in the second two areas: ensuring post-hospital follow up care and timely handover communication
Jan. 10 In-person Learning Session 2
Collaborative Action PeriodTimeline

Agenda
• Hospital sharing of improvement strategy: Katherine Barmer, Carteret General Hospital
• CMS “Dry Run” Readmissions Report: Erica Preston-Roedder, Director of Quality Measurement
• Preview of Community Engagement:
Linda McNeil, CCME

Carteret General HospitalOutreach Services
Reducing unnecessary ED visits and preventable readmissions at Carteret General Hospital by
improving transitions of care and building and strengthening community partnerships

Carteret General HospitalOutreach Services
• Readmission Collaborative• Community Care Plan• The Learning Center• Stroke Transitional Care• Community Transitions Project• Telehealth

Community Care Plan
• Public/private partnership• Carolina Access Medicaid• Drive down cost and utilization while
increasing quality of care• Physician-drive, patient-centered care

Carteret General Hospital Learning Center
• DSME-ADA Recognized• Educating/empowering patients in managing
their diabetes at home• MNT patients• Group and individual therapy

Carteret General HospitalStroke Transitional Care Program
• In Hospital VisitProgram introduction/stroke education
• Home Visit48-72 hours post discharge
• Call Back ProgramAt 1 week, 1 month, 2 months, and 3 months post discharge

Carteret General HospitalStroke Transitional Care Program
Program Successes *Provider follow up within 7 days of
discharge *Post discharge monitoring *Referrals for diabetes education,
MNT, smoking cessation *Enhanced post acute assessment of
outpatient needs

Carteret General HospitalStroke Transitional Care Program
Program Successes *Patient specific medication education *Reinforcement of stroke education
utilizing teach back method *Early recognition of signs and
symptoms of stroke and initiation of action plan

Community Transitions Project • Partnership with CCME-QIO and other community
health care providers and stakeholders• Work collaboratively in a comprehensive, community-
wide effort to measurably improve the quality of care provided to Medicare beneficiaries who transition between care settings. The goal of this project is to reduce 30-day readmission rates.
• Test and measure practice innovations, share experiences, and communicate openly with CCME and other providers in the CT Program on quality improvement activities.

Carteret General Hospital Telehealth Program
• Patients with CHF or related diagnosis• Follow patients 60 days post discharge• Work with patient to monitor early signs and
symptoms of their heart failure and develop action plan
• Case management in the outpatient setting• Follow up within 7 days of discharge• Collaboration with Cardiologist/PCP

Carteret General Hospital Telehealth Program
• Exception monitoring• Empower patient to be an advocate for their
own health• Expansion

Questions?

Question
Has your team identified an improvement in each of the four key areas?
Yes
No
Yes for the first two areas only

Question
Has your team conducted a Plan-Do-Study-Act cycle?
Yes
No

Readmissions: Understanding CMS Hospital-wide readmission
reports

• CCNC Medicaid PPR readmissions reports, sent to your CCNC representative twice per year & to your Quality Director (or equivalent)o Extensive info on your Medicaid population
• CMS ‘dry-run’ reportso Excess readmissions ratioo Hospital-wide readmissions measure
So many sources for info…

• Hospital readmission reductions programo Tied to payment; ‘excess readmissions ratio’o Publicly reported: Was reported initially in FY 2013 IPPS
Final Rule, and results will be posted on HospitalCompareo CMS had a data error and has had to re-calculate HRR for
all hospitals. Corrected results have been sent.o Measure uses AMI, HF, PN patientso CMS has circulated hospital-specific reports on QualityNet.
Also, NCHA has circulated hospital-specific reports to the CFOs. Both contain similar info.
CMS Hospital Readmissions Reduction Program


• New measure• Added to Inpatient Quality Reporting (IQR) program in IPPS
final rule for FY 2013…o …so hospitals have just started reporting it to CMS
• Will be publicly reported on HospitalCompare as of 2013• I haven’t heard anything about this being tied to payment• You received your dry run report in Sept, had opportunity to
ask questions up until Oct 5. Dry run report covered 2010 discharges.
• Source for more info is QualityNet. o Navigation: claims-based measures/hospital-wide
readmission & hip/knee measures
Hospital-Wide Readmission Measure

• First, various exclusions are made• Each patient is assigned one of 5 ‘specialty
cohorts’o Surgery/gynecology, cardiorespiratory,
cardiovascular, neurology, general medicine
• Any readmission to any hospital for any reason within 30 days is counted—unless the readmission is planned.
Basics of the Methodology




Admissions to other hospitals?

To find another hospital’s Medicare ID

Questions?

• Community Self Assessment• Expectations for Action Period 2 of Collaborative• Expectations for Learning Session 2 on Jan. 10
Community Engagement

Community Engagement with CCME

Second Action Period-Community Engagement
Three tracks will run concurrently
• Track 1: Not yet engaged in community building but
beginning to implement changes within the hospital.
• Track 2: Strong engagement in improving hospital
processes but haven’t started with community building
• Track 3: High level of engagement and success in
hospital changes and community building

January meeting-community segment
• Overview of community engagement
• Breakout sessions for each track
• Panel discussion
• Toolkit with resources to complete the work

Before January 10th
Prework checklist
•Submit zip codes to define community area•Data use agreement•Complete a community self-assessment and return it to
CCME by November 20th
•Identify a community lead/partner to attend January
meeting with you

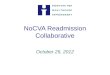
Readiness Assessment
No Activity Getting Started Complete Comments
1-a
Community and/or individual organization has identified key partners who share a piece in the continuum of care for a beneficiary discharged from a hospital (i.e. SNF, HHA, Meals on Wheels, transportation services, local community providers)
1-bCommunity care transitions team meets on a regular basis to look at the drivers of readmission
1-c
Community care transitions team has developed goals and secured a commitment from its partners to work on reducing readmissions
1-dThere is a defined leader for the Community care transitions team
Snapshot of the first items on the assessment.

www.ccmemedicare.org • (NC) 800-682-2650 • (SC) 800-922-3089
Questions?
This material was prepared by The Carolinas Center for Medical Excellence (CCME), the Medicare Quality Improvement Organization for North and South
Carolina, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The
contents presented do not necessarily reflect CMS policy. Product Number Needed

Contacts
• For more information, contact Laura Maynard, Director of Collaborative Learning at: [email protected] or 919-677-4121 or
• Dean Higgins, Project Manager at [email protected] or 919-677-4212
• Erica Preston-Roedder, Director of Quality Measurement, at [email protected] or 919-677-4125
• Linda Touvell McNeill, Care Improvement Specialist, CCME at: 919-356-3548 or [email protected]