www.ebmt.org
Pediatric Hematopoietic
Stem Cell Transplantation
Geneva – 2/4/2012
Isaac Yaniv MD
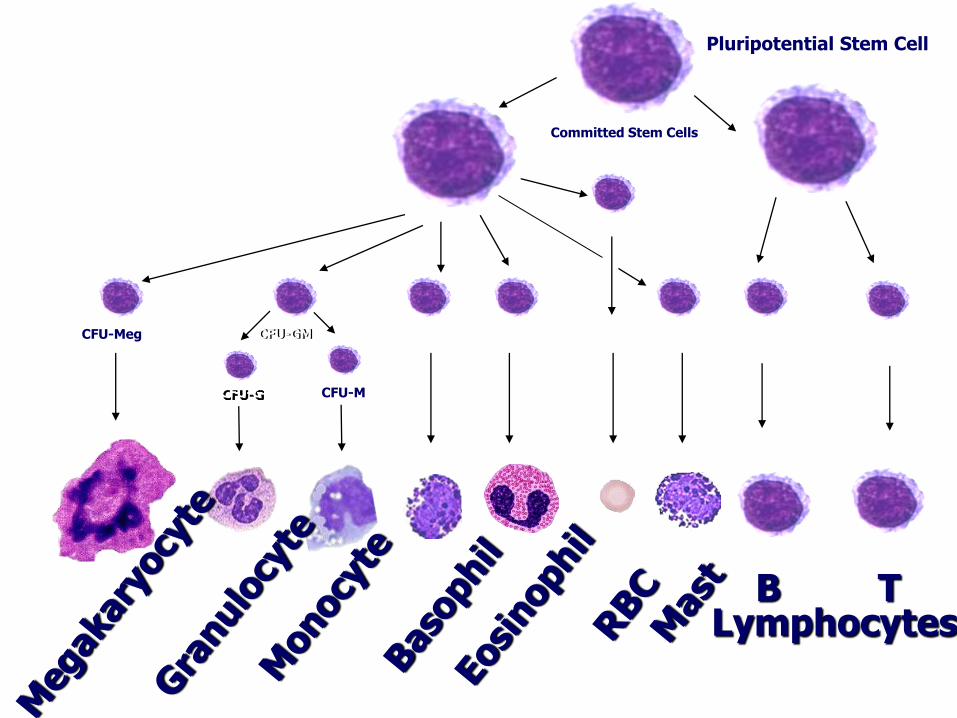
Pluripotential Stem Cell
Committed Stem Cells
CFU-Meg
Lymphocytes B T
CFU-Ba CFU-Eo CFU-E CFU-B CFU-T
BFU-E
CFU-Ms CFU-GM
CFU-G CFU-M
Which diseases are treated by
hematopoietic stem cell transplants?
• Hematologic malignancies originating in the bone marrow (leukemia
• Congenital or acquired bone marrow failure diseases
• Immune deficiency diseases (bubble children
• Other congenital genetic diseases such as Gaucher disease, thalassemia, etc
• Other malignancies
Pediatric diseases treated by SCT
• Malignant:
– ALL, AML
– CML
– MDS, Jmml
– NHL
– Hodgkin disease
– Solid tumors
• neuroblastoma
• rhabdomyosarcoma
• Ewing tumors
• Non malignant
– aplastic anaemia, pure red cell a.
– paroxysmal nocturnal hemoglobinuria
– autoimmune diseases
• Immunodeficiencies
– SCID, CID, LAD
• Hematologic defects
– Wiscott-Aldrich syndrome
– Fanconi anemia
– Blackfan-Diamond anemia
– Thalassemia
– Sickle cell disease
– Chronic granulomatous disease
– Chediak-Higashi syndrome
– Langerhans cell histiocytosis
– familial hemophagocytic lymphohistiocytosis
• Osteopetrosis
• Mucopolysaccharidoses
– Hurler, Hunter syndrome
• Lysosomal diseases
– metachromatic leukodystrophy
– adrenoleukodystrophy
– Lesch-Nyhan syndrome
Acquired Congenital
The course of SCT
• Preparation
• SC source
• Conditioning
• Toxicity: Organ, VOD, Infection,
• GVH,
• Relapse??
• Late effects
What are the dangers of SCT?
• Short-term - risk of non-relapse mortality
– Infection (fungal, viral)
– Organ failure (VOD, pneumonitis, heart)
– Acute Graft versus Host Disease
• Long term - Late effects of chemo/radio therapy
• Chronic GvHD, lungs, skin, sicca syndrome
• Infertility, 30% need Growth Hormone
• Thyroid failure, delayed puberty, premature menopause
• Cataract, 2nd Cancer, neuropsychological
SEVERE COMBINED
IMMUNODEFICIENCIES (SCID)
“the bubble boy”
• Genetic diseases due to defects in key genes
of the immune system
• More than 20 genes identified
Mild Primary Immunodeficiencies
• Common Variable Immunodeficiency
• Immunodeficiency With Hyper-IgM
• X-linked Agammaglobulinemia
• Autosomal Recessive Agammaglobulinemia
• Selective IgA Deficiency
• Chronic Granulomatous Disease
• Di George Syndrome
• Chronic Mucocutaneous Candidiasis
• Combined Immunodeficiencies
• Ataxia-telangiectasia
• IFN-gamma Deficiency
• Myeloperoxidase Deficiency
• X-linked Lymphoproliferative Disease
• Wiskott-Aldrich Syndrome
• Hyper-IgE Syndrome
• ADA Deficiency
Severe Primary Immunodeficiencies
• Wiskott-Aldrich Syndrome
• Leukocyte Adhesion Deficiency
• Combined Immunodeficiencies
• SCID
• ADA deficiency SCID
• Hyper-IgM Syndrome
• Lymphohistiocytosis
• Chediak-Higashi Syndrome
• Kostmann Disease
• X-linked Agammaglobulinemia
• Chronic Granulomatous Disease
CLINICAL SPECTRUM OF SEVERE
COMBINED IMMUNODEFICIENCIES
• Recurrent and severe infections caused by
bacteria, viruses and opportunistic organisms.
• Maternal GVHD.
• Failure to thrive.
• Autoimmunity and cancer.
In the absence of treatment death within the first years.
Comorbidities in Children
• Viral Infections: SCID
– Rota, Adeno, CMV
– Encephalitis, Pneumonia, Gastroenteritis
• Organ Dysfunctions:
– Cardiac dysfunction in metabolic diseases
– Encephalopathies in congenital storage diseases
– Bone infarction in Sickle Cell diseases
– Iron Overload
– Liver fibrosis in Thalassaemia
AVAILABLE TREATMENTS
• Conventional therapy
• Immunoglobulin replacement therapy
• Cytokine therapy
• Hematopoietic stem cell transplantation
• Enzyme replacement therapy
• Gene therapy – ADA SCID
– X LINKED SCID
– CGD
Stem Cell Transplantation in
Thalassemia
No immediate threat on life
With good chelation - increased survival
History of good chelation correlates with good
outcome post MSD SCT
Those who are non compliant with chelation
have also poor prognosis with SCT
Stem Cell Transplantation
in Thalassemia
The question:
Continue with a chronic disease (Thalassemia)
and daily chelation
Or
Undergo SCT (if a MSD available) and risk
10% of TRM and 25% of GVHD
Inborn Errors of Metabolism
• Inborn errors of metabolism (IEM) are a diverse group of diseases
arising from genetic defects in lysosomal enzymes or peroxisomal-
function.
• Lysosomal enzymes are hydrolytic and are stored in cellular
organelles called lysosomes.
• Peroxisomes are subcellular organelles involved in lipid metabolism.
• These diseases are characterized by devastating systemic processes
affecting neurologic and cognitive function, growth and
development, and cardiopulmonary status. Onset in infancy or early
childhood is typically accompanied by rapid deterioration and
associated with early death.
Title of the presentation - Author
Inborn Errors of Metabolism
• Timely diagnosis and immediate referral to a
“specialist in IEM” are essential steps in
management of these disorders, this includes
presentation of the patient in a multidisciplinary
team including a transplant-physician.
Inborn errors of metabolism
History
• 1969
• Fratantoni and Neufeld laid the foundation for our understanding of
transferable lysosomal enzymes by demonstrating cross-correction of
metabolic defects in co-cultures of fibroblasts from Hurler and Hunter
syndrome patients » Fratantoni JC, Hall CW, Neufeld. Proc Natl Acad Sci USA 64: 360–366.
• 1971
• correction of the deficient enzyme was demonstrated with lymphocyte
extracts or serum » Di Ferrante N et al. Proc Natl Acad Sci USA 68: 303–307.
» Knudson AF Jr et al. Proc Natl Acad Sci USA 68: 1738–1741.
History
• 1981
• The first SCT for Hurler Syndrome
» Hobbs JR, Hugh-Jones K, Barrett AJ, et al (1981) Reversal of clinical features of Hurler’s disease
and biochemical improvement after treatment by bone-marrow transplantation. Lancet 2: 709–712.
• 1984
» Krivit W et al. Bone marrow transplantation in the Maroteaux–Lamy syndrome
(mucopolysaccharidosis type VI). Biochemical and clinical status 24 months after transplantation. N
Engl J Med 311: 1606–1611.
• 1995
• More Proof of principles/success post SCT
– Repopulating donor macrophages (e.g. Kupffer cells and microglial cells) in various tissues
– Secretion and delivery of the enzyme by donor cells leads to arrest of further progression of disease –
neurodegeneration, and also the tissue storage.
– Cross reaction
» Krivit W, Henslee-Downey J, Klemperer M, et al. Survival in Hurler’s disease following bone
marrow transplantation in 84 patients. Bone Marrow Transplant 15: S182–S185.
• 2005
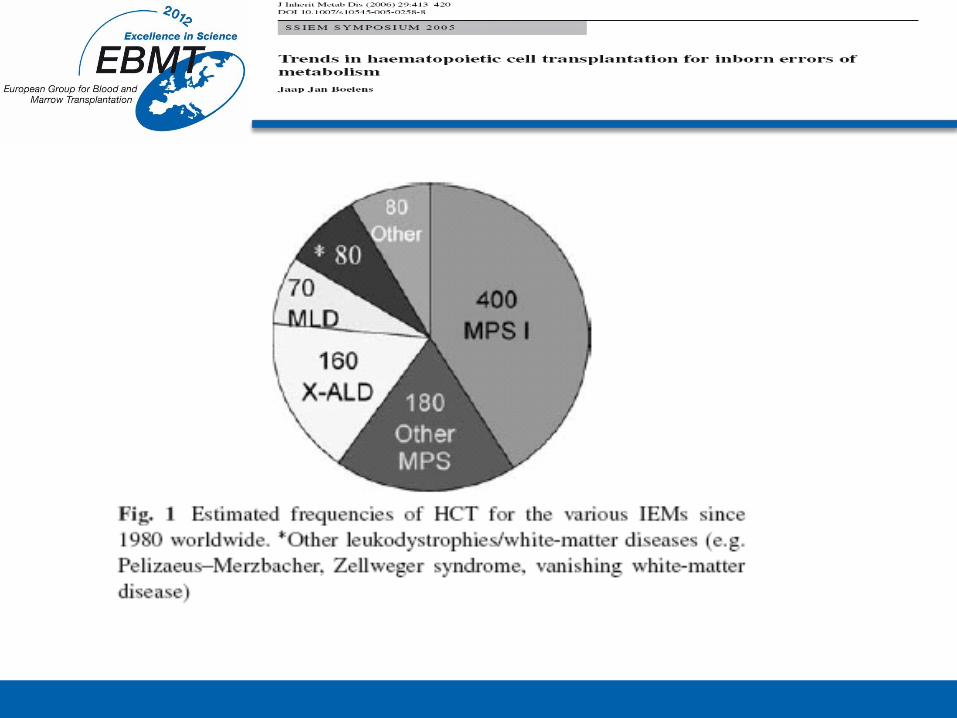
• ~950 SCTs worldwide (for more than 20 IMGD diseases)
» Rovelli AM, Steward CG (2005) . Bone Marrow Transplant 35(Supplement): S23–S26.
SCT- inborn error of
metabolism
• Hurler syndrome (MPS 1H)
• Gaucher disease
• Osteopetrosis
• Marteaux-Lamy syndrome (MPS VI)
• Krabbe’s disease (Infantile GLD)
• X-adrenoleukodystrophy (X-ALD)
• Late onset Globoid-cell leukodystrophy (GLD)
• Metachromatic leukodystrophy (MLD)
• Alpha-mannosidosis
• Mucolipidosis, type II (I-cell disease)
• Fucosidosis (1 case report, Vellodi et al. 1995)
Inborn Errors of Metabolism
• Metabolic correction of lysosomal storage diseases (LSD) occurs by mannose-6-phosphate receptor-mediated endocytosis of secreted enzyme and by direct transfer of enzyme from adjacent cells.
• The mechanism by which HSCT halts cerebral demyelization of the peroxisomal disorder cerebral X-linked adrenoleukodystrophy (X-ALD) is multifactorial : immunosuppression, replacement with metabolically competent cell populations leading to decreased perivascular inflammation and, metabolic correction. Migration, distribution, and growth of donor-derived metabolically-competent cells into host tissues including the central nervous system (CNS) are critical to the success of transplant.
• In Osteopetrosis, a disease due to osteoclasts dysfunction, HSCT can correct the disease by providing competent osteoclasts since the osteoclast is derived from the hemopoietic stem cell 3.
Inborn Errors of Metabolism
• Currently, BMT from an HLA-matched,
enzymatically normal related donor and UCBT are
the most common modalities of HSCT for IEM.
• In cases where damage to the central nervous system
(CNS) is present this is irreversible and therefore it
represent a contra-indication for HSCT in all
candidate diseases
Osteopetrosis
• Osteopetrosis is a genetically heterogeneous group
of osteoclast disorders.
• Transplant-toxicity in HSCT for osteopetrosis is
mainly caused by hypercalcemia, graft-failure,
pulmonary complications and veno-occlusive
disease
MPS IH
• Autosomal recessive
• Deficiency of alpha-L-iduronidase
• 1:80,000 live births
• Short life expectancy (5 years)
• Developmental delay, hydrocephalus, sleep apnea, auditory
and visual changes, cardiopulmonary dysfunction, dysostosis
multiplex, hepatosplenomegaly…..etc.
MPS IH
• Treatment
– Enzyme replacement therapy (ERT)
– Gene therapy
– SCT
• ERT and gene therapy in animal models: immunologic
complications
SCT-MPS IH
• Normalizes WC alpha-L-iduronidase.
• Extends life expectancy.
• Stabilizes intelligence.
• Prevents or stabilizes coronary disease.
• Prevents or stabilizes hydrocephalus.
• Corrects sleep apnea & hepatosplenomegaly.
• Improve cardiopulmonary and auditory.
• LITTLE benefit for the skeletal deformities.
When to perform SCT ?
• Based on
– cognitive assessment, scores for age equivalent and
IQ measuring and rate of development
– 24 months is the accepted cut off
X-ALD (Adrenoleukodystrophy)
• X-ALD is an X-linked peroxisomal disorder involving defective beta-oxidation of very long chain fatty acids (VLCFA). Cerebral X-ALD is a rapidly progressive, intensively inflammatory myelinopathy
• Disease progression results in severe disability, dementia and death over a period of months to years.
• HSCT is reserved for boys/men who have early definitive evidence of cerebral disease as determined by magnetic resonance imaging.
• In individuals presenting with clinical disease, the rapidly progressive nature of the condition precludes a successful transplant outcome in most cases.
SCT challenges
• Engraftment failure
• GVHD/TRM
• Pulmonary hemorrhage
• Long term follow up » Neuro-cognitive
» Adaptive functioning
» Quality of life
Long term follow up and
outcome measures
• Survival
• Performance scales
• Neurocognitive outcomes
• Adaptive functioning
• QOL
HSCT for IEM
• Early diagnosis and treatment have favorably
affected all children with IEM, leading to
prevention of devastating neurocognitive and
neuropsychological sequellae.
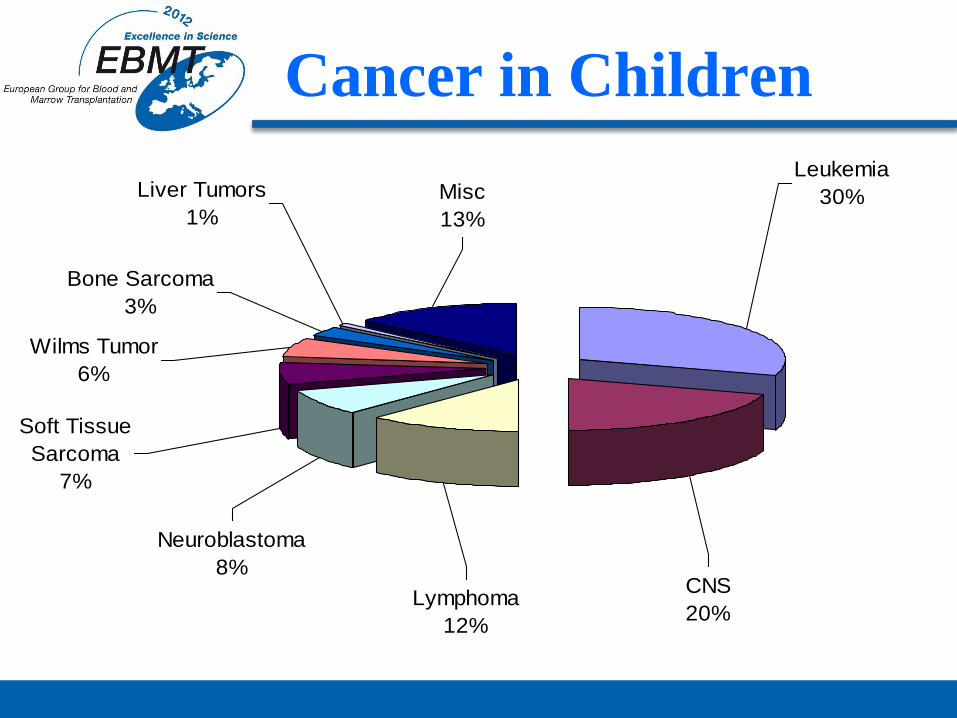
Cancer in Children
Cancer in children less than 15 years of age
Leukemia
30%Misc
13%
Liver Tumors
1%
Bone Sarcoma
3%
Wilms Tumor
6%
Soft Tissue
Sarcoma
7%
Neuroblastoma
8%
Lymphoma
12%
CNS
20%
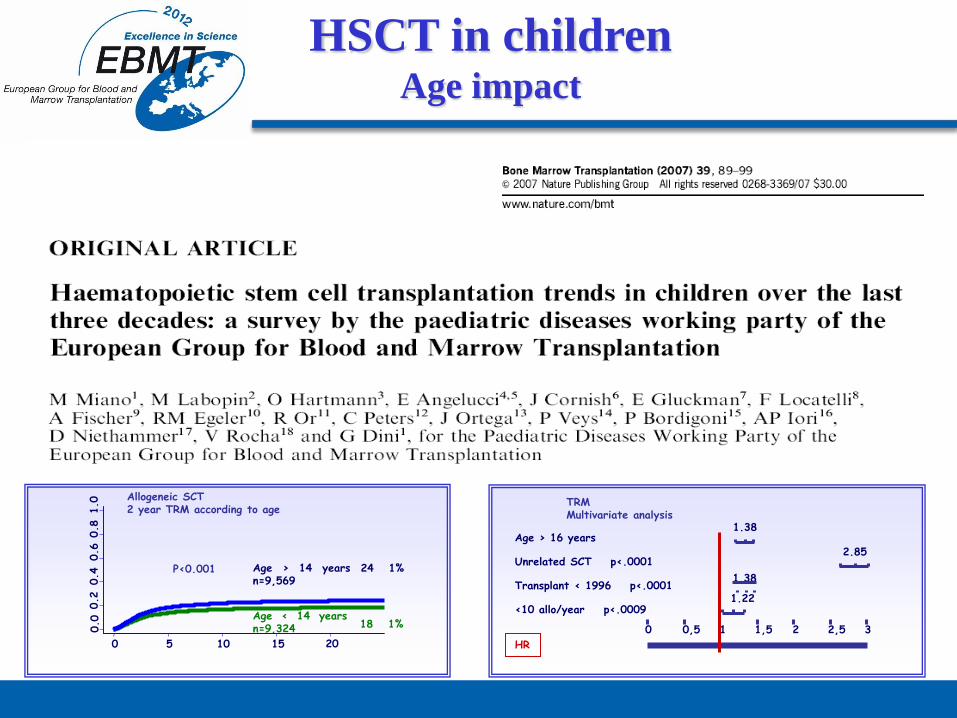
HSCT in children Age impact
Allogeneic SCT 2 year TRM according to age
Age > 14 years n=9,569
Age < 14 years n=9,324
24
1%
18
1%
P<0.001
0 5 10 15 20
TRM Multivariate analysis
Age > 16 years
Unrelated SCT p<.0001
Transplant < 1996 p<.0001
<10 allo/year p<.0009
0 0,5 1,5 2,5 1 2 3
1.38
2.85
1.38
1.22
HR
Autologous SCT
Stage IV Neuroblastoma
Relapse lymphoma
Relapse germ cell tumor
High risk Ewing
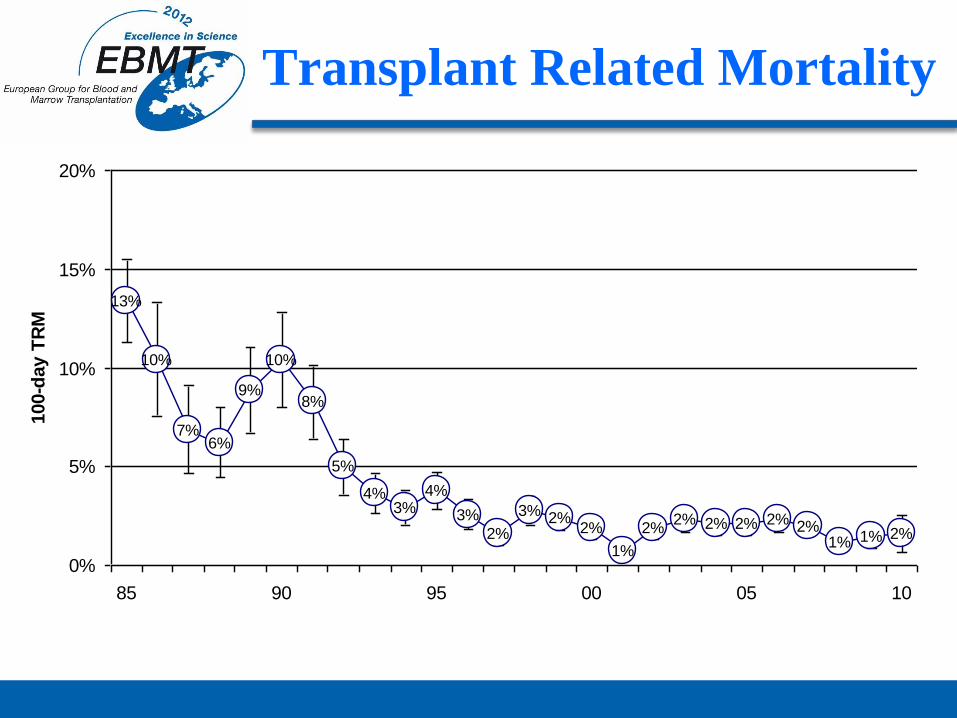
Transplant Related Mortality
13%
10%
7%6%
9%
10%
8%
5%
4%3%
4%
3%
2%
3% 2%2%
1%
2%2% 2% 2% 2% 2%
1% 1% 2%
0%
5%
10%
15%
20%
85 90 95 00 05 10
100-d
ay T
RM
Neuroblastoma
• Definition of HR patients & Eligibility for MGT
– First line • MycN amplified tumours INNS stages 2 to 4 any age
• stage 4 >18 months
– Relapse • any metastatic >18 months
• any MycN amplified without previous MAT
• European Prospective Randomised Trial: – HR-NBL1/SIOPEN
– Confirmation of superiority of BUMEL > CEM (+16% EFS & OS)
Ewing Sarcoma
• Definition of HR patients & Eligibility for MGT
– First line
• histological poor response after induction (10% viability)
• tumour volume 200ml
• primary metastatic (lungs only or other)
– Relapse
• any metastatic if no previous MGT
– Response
• CR1>PR1 5-yrs.pSU : 0.51 > 0.37
• CR2>PR2 5-yrs.pSU: 0.41 > 0.15
• Busulfan remains a promising drug to improve results in high-risk Ewing tumor patients during first line treatments
• EURO- EWING 99 – Investigation of BUMEL/SCT vs convent. CHT in strata R2
CNS Tumors
• Definition of HR patients & Eligibility for HDT
– Histology YES NO
• medulloblastoma • ependymoma
• PNETs • brain stem glioma
– Relapse
– Metastasis at Dx
– Additional high risk features:
• incomplete resection, age [younger than 3 or 5 years?]
• MGT Regimens of European Groups: BU-TTP [repetitive L-PAM] Vp16 / CBDCA - TTP / L-PAM Vp16 / TTP / CBDCA, BU-TTP Vp16 / TTP / CBDCA [CET] VP16 / TTP / CBDCA
Germ Cell Tumors
1. Definition of HR patients & Eligibility for MAT
• Recurrent intracranial pediatric GCT
– Recurrent malignant CNS GCT with biological remission
• non secreting: germinoma
• secreting [YST, CHC, EC] relapse rate 30%
• Recurrent extra cranial pediatric GCT
• First line pts with insufficient response to primary CHT (SIOP)
2. MGT Regimens of European Groups: Vp16 / CBDCA
Vp16 / TTP / CBDCA Vp16 / TTP
Wilms Tumor
Children with recurrent WT
ICE
Surgery (primary and metastases)
CEM / ASCR adopt to renal clearance or GFR rates 100 cc/min.173m²
adopt for kg if 12kg
Pediatric Solid Tumors
• Response Status
– Good indications: good responding first line disease (CR/VGPR/PR)
– + sensitive relapse (SR)
– Questionable: SD /MR
– No indication: RR/ NR (progression)
• No clear advantage for repetitive MGT
• No clear advantage for allogeneic SCT :
– more phase II validation needed in very high risk patients
• No TBI
• Busulphan/Melphalan MGT most promising combination in Neuroblastoma and Ewing sarcoma
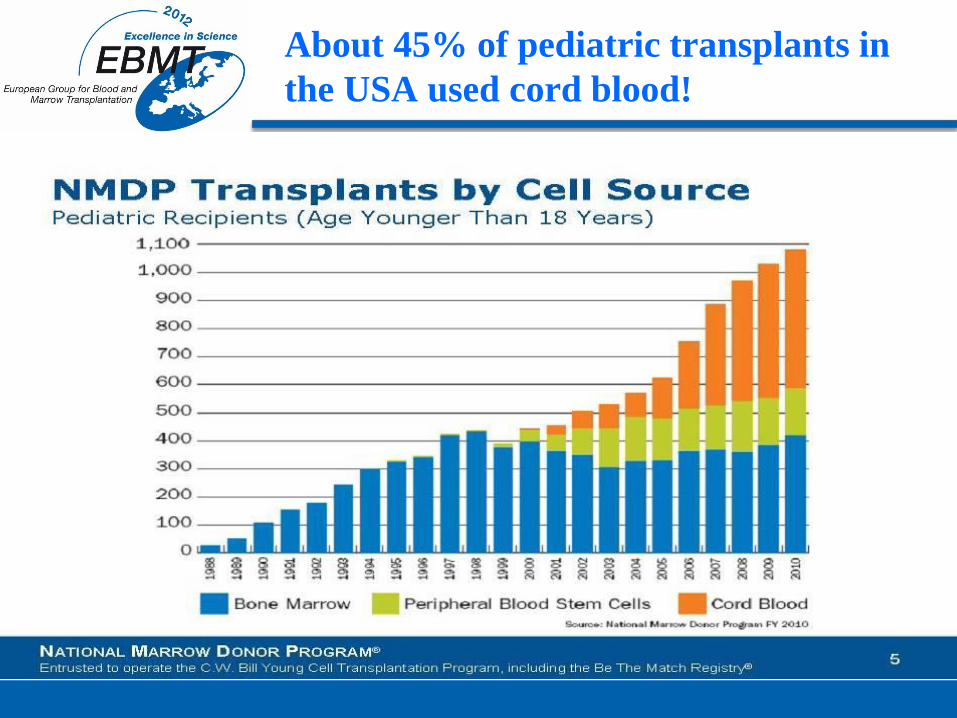
About 45% of pediatric transplants in
the USA used cord blood!
Cord Blood
• Cord blood is an excellent alternative for
someone with no suitable donor among
relatives or in the registries.
• Or when the patient’s condition does not allow
long delay until a donor is found.
• Or for directed donations.
Late effects
• Advances in SCT techniques, supportive care and increasing indications
• > resulted in significant improvement in longterm survival
• >> need for accurate diagnosis and treatment of LE
with
– Early identification of multisystem physical effects
– Comprehensive intervention and treatment
– Establishment of multidisciplinary preventive health care
Specific pediatric issues
• Age at SCT
• Growing and developing organ system
• Extended period to deal with long term
complications
• Difficult transition from pediatric to adult
medicine
Late Effects
are multifactorial and influenced by
• Genetic disposition
• developmental stage and psychosocial background
• Underlying disease and co-morbidities
• Exposure to chemo / radiotherapy prior to SCT
• Conditioning regimens (TBI….)
• Early complications and their therapy
– Organ toxicity
– Infections
– Immune dysregulation and immune deficiency
– GVHD and immunosuppressive therapy
Potential LE
• Endocrinopathies
• Musculoskeletal disorders
• Pulmonary function disorders
• Cardiovascular complications
• GI and hepatic sequellae
• Renal dysfunctions
• Occular abnormalities
• Oral and dental complications
• Hearing problems
• Skin problems/ alopecia
• Immunological dysfunctions
• Neurolgical and cognitive consequences
• Psychosocial sequellae
• Secondary malignancies
CNS
Risk factors:
younger age at SCT,
TBI, cranial irradiation,
Bu, Thio, Mel, MTX,
cGVHD, longterm steroid therapy
Clinical manifestations:
Leukoencephalopathy, cerebral atrophy, demineralizing microangiopathy, peripheral polyneuropathy
Fatigue, headache, epilepsy, ataxia, psychomotor retardation, limited age appropriate daily activities, neurocognitive deficits (diminished IQ, ↓ of executive functions and processing)
Be aware of coexisting hearing or eye problems
Broad overlap, often subtle onset
Behavioral problems
less interaction in an age-appropriate fashion, difficulties forming friendships,
social skills
social integration
Educational problems
Schooling problems with the need of special education
assistance (math, reading..)
High unemployment rate
Psychological problems
anxiety or depression,
excessive mood swings
loss of positive self-image
Psychosocial sequelae
Ototoxicity
Risk factors:
CY, Thiotepa,
Cis-and Carboplatin pre SCT
TBI, cranial irradiation
school problems and cognitive deficits may be due to coexisting hearing loss
Eye
Risk factors:
TBI, cranial irradiation, Bu, longterm
steroidtherapy
Clinical manifestations:
cataract (late onset, med. 8 years)
Sicca syndrome
Microvascular retinopathy (CSA!) children often don‘t communicate dry eye symptoms; photophobia may be the first or only symptom
Oral and dental
Risk factors:
young age at SCT, TBI and cranial irradiation, GVHD, poor hygienic status
Clinical manifestations:
Dental caries, enamel hypoplasia
Microdontia, arrested root development
Malocclusions
Salivary dysfunction, chronic mucositis
orthodontic treatment with fixed braces should only be applied after healing of mucositis
children rarely communicate dry mouth symptoms,
excessive drinking during eating and malnutrition may be only symptom
Pulmonary
Risk factors:
TBI, chest irradiation, Bu, MTX,
GVHD, IgG/ IgA deficiency,
recurrent infections
Clinical manifestations:
Obstructive and (less) restrictive
respiratory dysfunction
BO
BOOP
Lung function test in young children needs a pediatric experienced pulmonologist and serial testing
Cardiovascular
Risk factors:
Anthracycline treatment >250-300 mg/m2, Cyclophosphamide >150mg/kg,
TBI and chest irradiation, iron overload
Clinical manifestations:
arrhythmia, cardiomyopathy, pericardial and valvular disease, congestive cardiac failure,
often subtle onset, may increase over time
Estrogen deficiency and metabolic syndrome may predispose to increasing cardiac LE
Renal
Risk factors:
TBI, local irradiation,
Cisplatin, Carboplatin pre SCT
long term anti bacterial and viral therapy
Clinical manifestations:
tubular and glomerular toxicity,
thrombotic microangiopathy,
nephrotic syndrome
GI and hepatic
Risk factors:
TBI and local irradiation,
GVHD
Iron overload
chronic infection (viral, bacterial)
Clinical manifestations:
dysphagia, pain, irritable bowel syndrome, malnutrition,
hyperbilirubinemia, chronic hepatitis
Skeletal disorders
Risk factors:
older age at SCT,
TBI, local irradiation,
GVHD,
long term steroid therapy
malnutrition, catabolism,
loss of muscle mass, physical inactivity
hypogonadism
Clinical manifestations:
osteopenia, osteoporosis
avascular necrosis (AVN)
Endocrine LE
• Thyroid dysfunction
• Gonadal dysfunction
• Adrenal dysfunction
• Growth retardation
Thyroid dysfunction
Most common endocrine LE
Risk Factors:
TBI, cranial irradiation, Bu, age < 10yrs at SCT, cGVHD
Clinical manifestations:
• Hypothyroidism: fT4 ▼,TSH▲
• Compensated hypothyroidism: ▲ TSH, ft4 normal
• Euthyroid sick syndrome: fT3 and fT4 ▼, TSH normal
• Autoimmune - thyroiditis: thyroid Ab
Growth
Risk factors:
TBI, cranial RT, HD-Chemotherapy before SCT
Long-term steroidtherapy
Multifactorial:
• Hypothyroidism, hypogonadism
• Peripheral lesions of cartilage, bones and epiphyseal growth plate
• Malnutrition
• Genetic disposition
• GH-deficiency
• Not always correlation between GH-deficiency and growth retardation

Pubertal developement
• development of secondary sexual characteristics,
changes in fat distribution, skeletal and somatic growth, psychologic changes
• needs a delicate balance of function of hypothalamus, pituitary gland and sexual hormone secretion
Risk factors:
SCT during puberty ,TBI, cranial RT, Bu, cGVHD
• Compensated hypogonadism with spontanous puberty
• Delayed puberty, amenorrhea and infertility
• In young adults premature menopause
•
Risk of osteoporosis and cardiovascular complications
• Germinal epithelium is more vulnerable than Leydig cells with testosterone production
• Mostly normal puberty with reduced spermatogenesis
Metabolic Syndrome
Risk factors:
TBI, long term steroids, cGVHD, obesity, physical inactivity,
Family history
Clinical manifestations:
• Central obesity
• Insulin-resistence, Glucose intolerance,
• ↑ increased risk of diabetes typ II
• Dyslipidemia, potential steatosis hepatis
• Hypertension
Immunological dysfunction
Risk factors:
delayed immune reconstitution, RIC ?, mixed chimerism, cGVHD, chronic viral infections
poor T-cell function
disturbed B-cell homeostasis, impaired specific antibody production
IgA and IgG subclass deficiency
Functional hyposplenism in cGVHD
Clinical manifestations:
increased risk of infections especially encapsulated bacteria (e.g. pneumococci)
auto/ alloimmune phenomena (e.g. autoimmune thyroiditis)
→ revaccination!!!
Secondary malignancies
Incidence continues to increase with prolonged follow-up
Risk factors:
TBI and local irradiation, HD-chemotherapy prior to SCT, less data about longterm FU after RIC;
longterm immunosuppression and extensive cGVHD, younger age at SCT,
Increased risk : 4-11 fold compared to general population
Predominantly:
post-transplant lymphoproliferative disorder (PTLD) (in the first year),
lymphoma
secondary MDS and AML
solid cancers with a longer latency period (up to 15-20 yrs post SCT)
skin, oropharyngeal (squamous cell carcinoma), brain,
thyroid and breast cancer
higher risk for sec. malignancies due to underlying disease: Fanconi Anemia
Prevention
• Primary prevention
– RIC?
– Avoidance of TBI and additional irradiation
– Timepoint of SCT in non malignant diseases
• Secondary prevention
– Early diagnosis and treatment
– Enhanced rehabilitation
– SCT-outpatient and LE-clinics
– Adolescent medicine
– longitudinal data collection within studies
Preventive strategies
• Long term follow up
– Functional status, symptom review
– symptom burden (patient assessment), QOL
– Specific screening
• Encourage patients to self-examination (skin, breast..)
• Establishment of preventive health care
• Patient counseling : „life style „ guidance – Good nutrition, regular exercise..
• Avoidance of high-risk behaviors – Unnecessary exposure to sunlight (esp. among pat. with history of radiation)
– Smoking
– Alcohol, drugs
– Obesity
The difference..
The pediatric age group has relevance to many aspects of
oncology, from basic biology through health services and
treatment to psycho-oncology.
Some cancers that affect young people have worse
outcomes than others: leukemia, brain tumors, epithelial
cancers and Sarcomas
Tumor biology and clinical outcome for a given tumor vary
in different age groups, thus suggesting tailored
approaches according to patient’s age
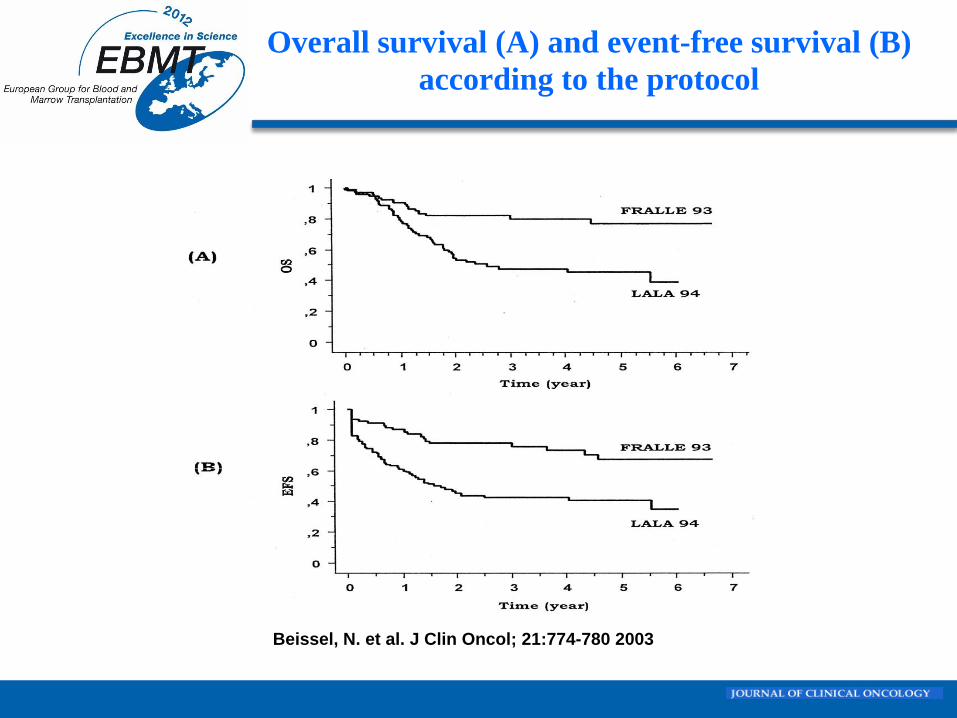
Beissel, N. et al. J Clin Oncol; 21:774-780 2003
Overall survival (A) and event-free survival (B)
according to the protocol
Specific issues..
Gap in pharmacologic data on cytotoxics in childhood,
adolescence and young adulthood
Differences in anthropometric measures, body
composition, size, and maturity of organs, hormonal
status, directly influence the disposition and clearance
of drugs, the susceptibility to treatment morbidity
A child is not a “small adult” and does not become an
adult on a given birthday or at a given weight
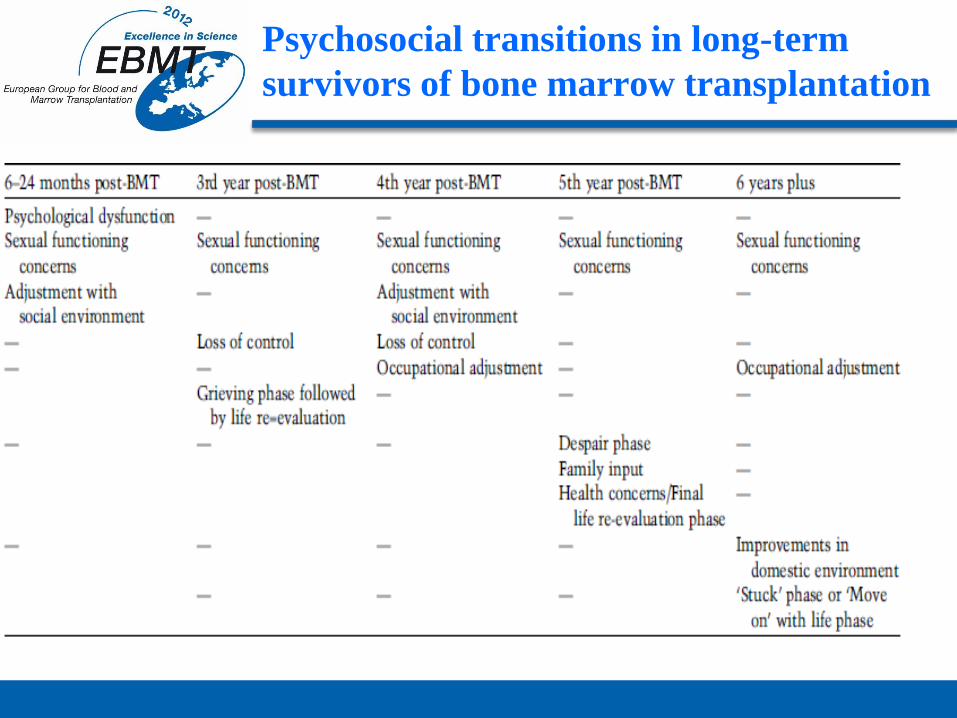
Psychosocial transitions in long-term
survivors of bone marrow transplantation
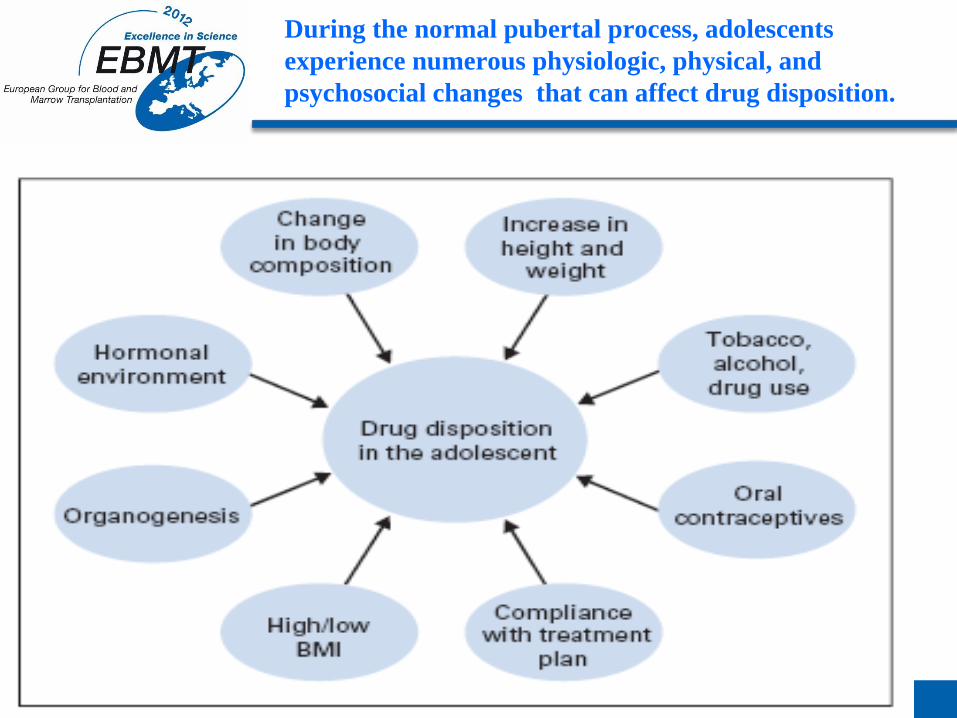
During the normal pubertal process, adolescents
experience numerous physiologic, physical, and
psychosocial changes that can affect drug disposition.
Major factors to be considered..
● Epidemiology of congenital diseases and cancer in the pediatric
population
● Biology and genetics of common pediatric diseases
● Treatment regimens specific to children
● Physiology and host biology across the age range (radiation and
chemotherapy dosing and toxicity and development of age-related co
morbidities)
● Psychosocial and neurocognitive development across the pediatric age
range
● Biomedical consequences of treatment (acute adverse and late effects)
● Fertility preservation options
Recommended

















