
Practical management of PI therapyin Hepatitis C Paris Februari 2012
Ola Weiland Karolinska InstitutetStockholm, Sweden
New major adverse events with PIs• Exanthema for TVR
• Prolonged anemia with BOC

TelaprevirIlluminate studySherman et al2011
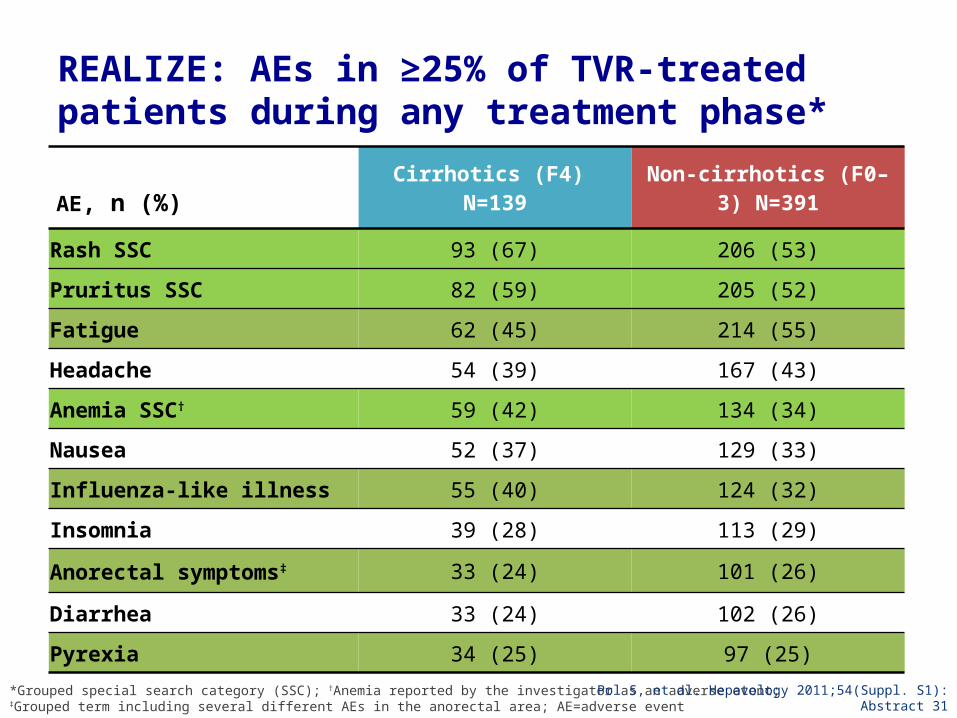
REALIZE: AEs in ≥25% of TVR-treated patients during any treatment phase*
AE, n (%)Cirrhotics (F4)
N=139 Non-cirrhotics (F0–3) N=391
Rash SSC 93 (67) 206 (53)
Pruritus SSC 82 (59) 205 (52)
Fatigue 62 (45) 214 (55)
Headache 54 (39) 167 (43)
Anemia SSC† 59 (42) 134 (34)
Nausea 52 (37) 129 (33)
Influenza-like illness 55 (40) 124 (32)
Insomnia 39 (28) 113 (29)
Anorectal symptoms‡ 33 (24) 101 (26)
Diarrhea 33 (24) 102 (26)
Pyrexia 34 (25) 97 (25)
*Grouped special search category (SSC); †Anemia reported by the investigator as an adverse event; ‡Grouped term including several different AEs in the anorectal area; AE=adverse event Pol S, et al. Hepatology 2011;54(Suppl. S1): Abstract 31
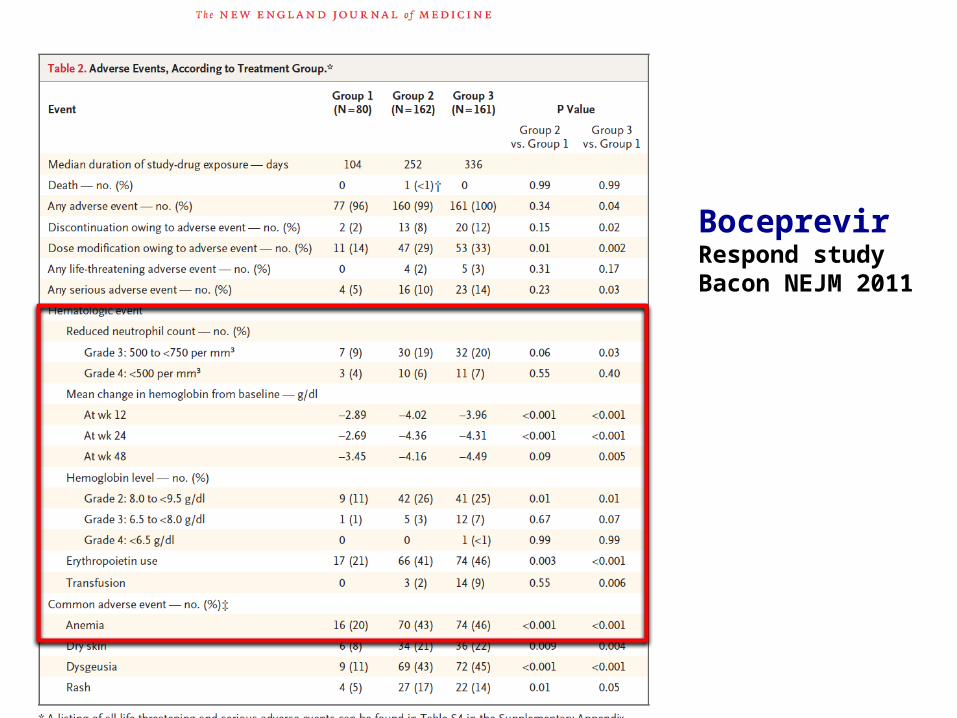
BoceprevirRespond studyBacon NEJM 2011
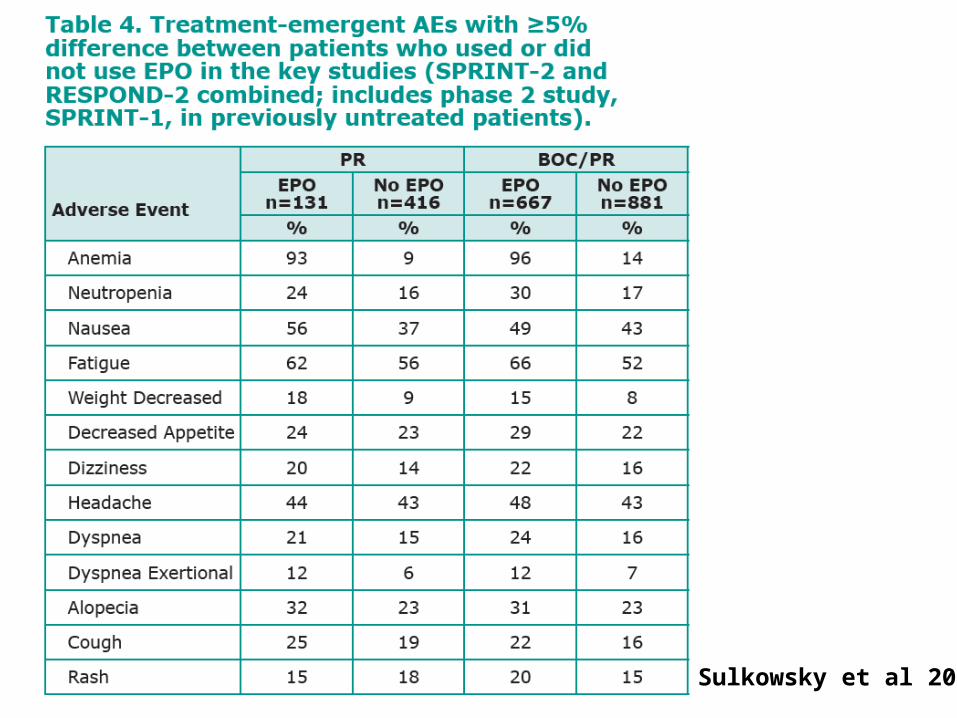
Sulkowsky et al 2011
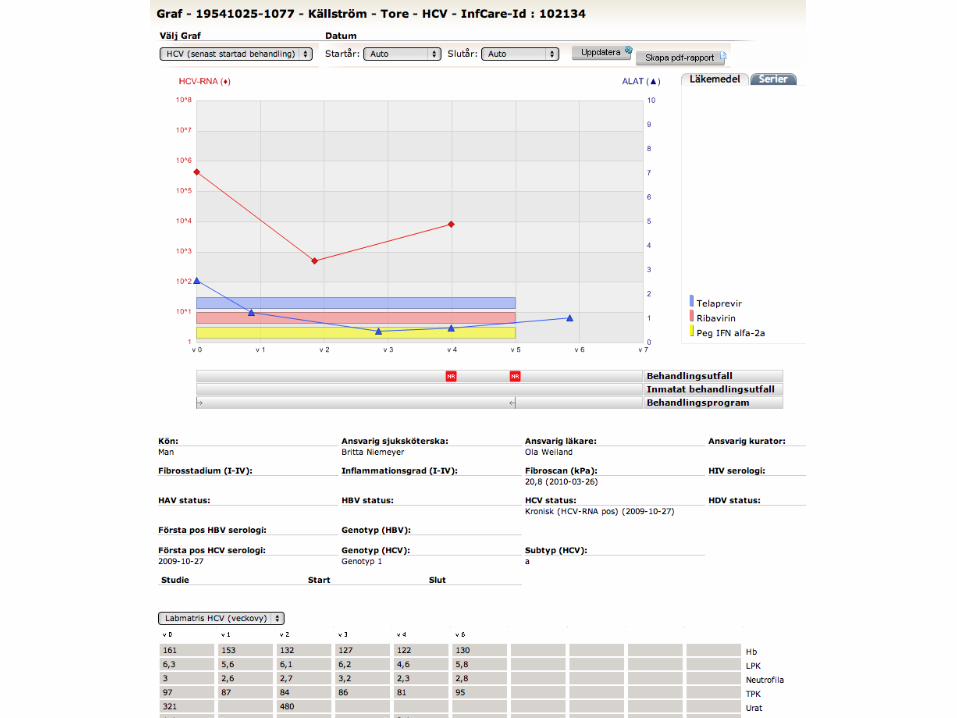
Case number 1
HCV case male born 1947
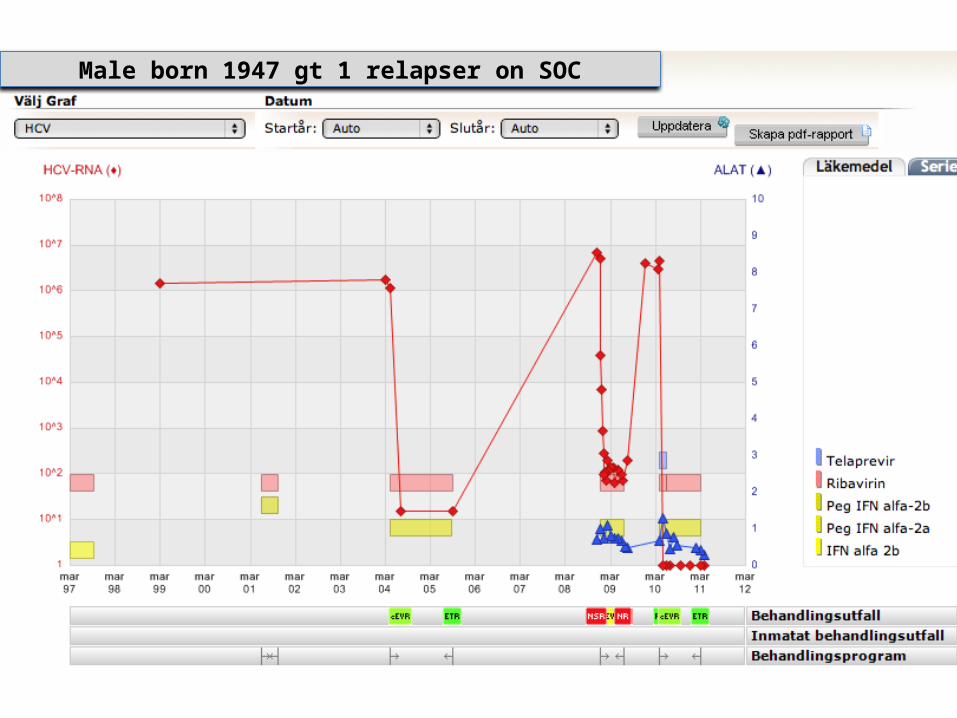
• Chronic HCV gt 1b• IFN + RBV later part of 1990is relapse after Rx• Liver biopsy 2004 stage 1-2• Peg IFN alfa 2a + RBV in REPEAT study
72 ws Rx 2005 slow response-relapse• 2005 Retinal emboli• 2006 closure of atrial atrial septal defect
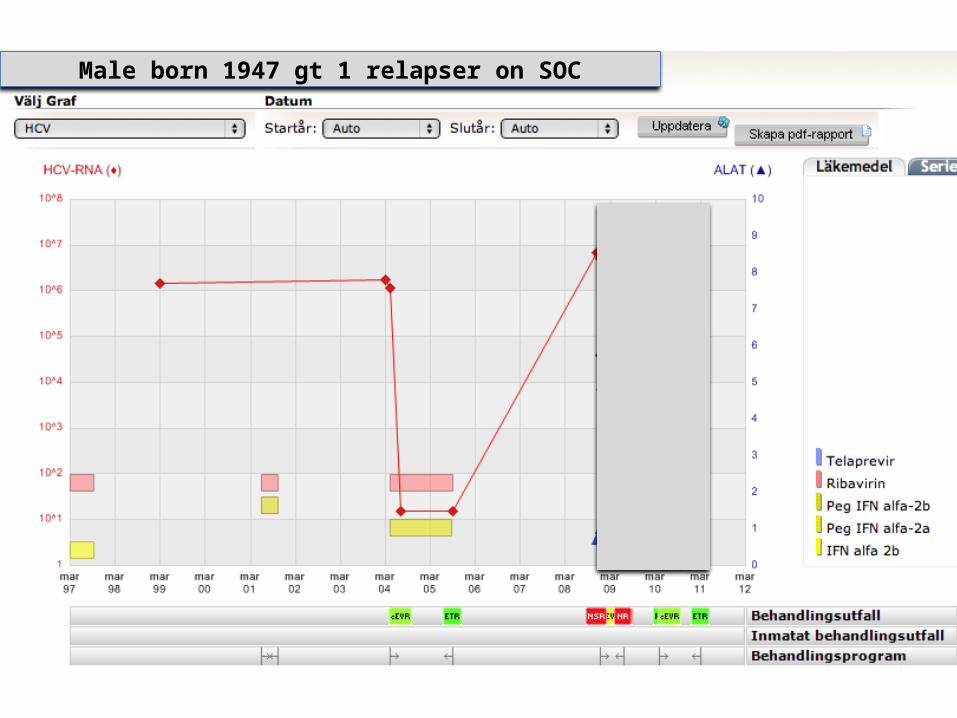
Male born 1947 gt 1 relapser on SOC
HCV case male born 1947
• Retreat with PI + peg-IFN + RBV
• Wait for better DAAs
HCV case male born 1947
• Retreatment with Telaprevir + peg-IFN alpha 2a + RBVIn the realize study startedRandomized to placebo – outcome response-relapse
• Later switched to Telaprevir + peg-IFN alpha 2a + RBV
Male born 1947 gt 1 relapser on SOC
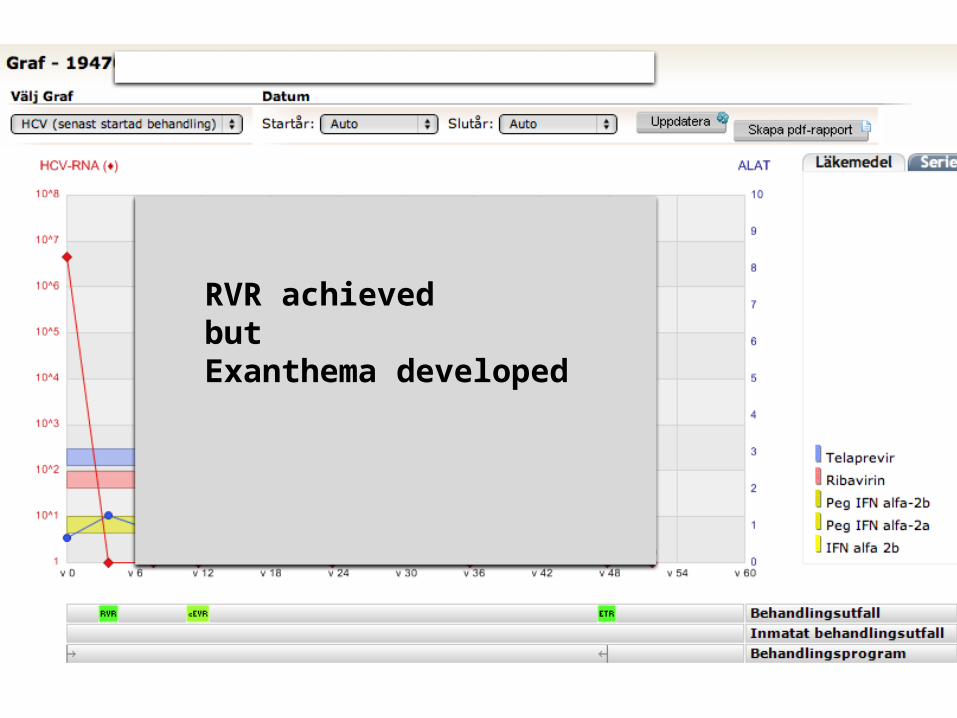
RVR achievedbutExanthema developed
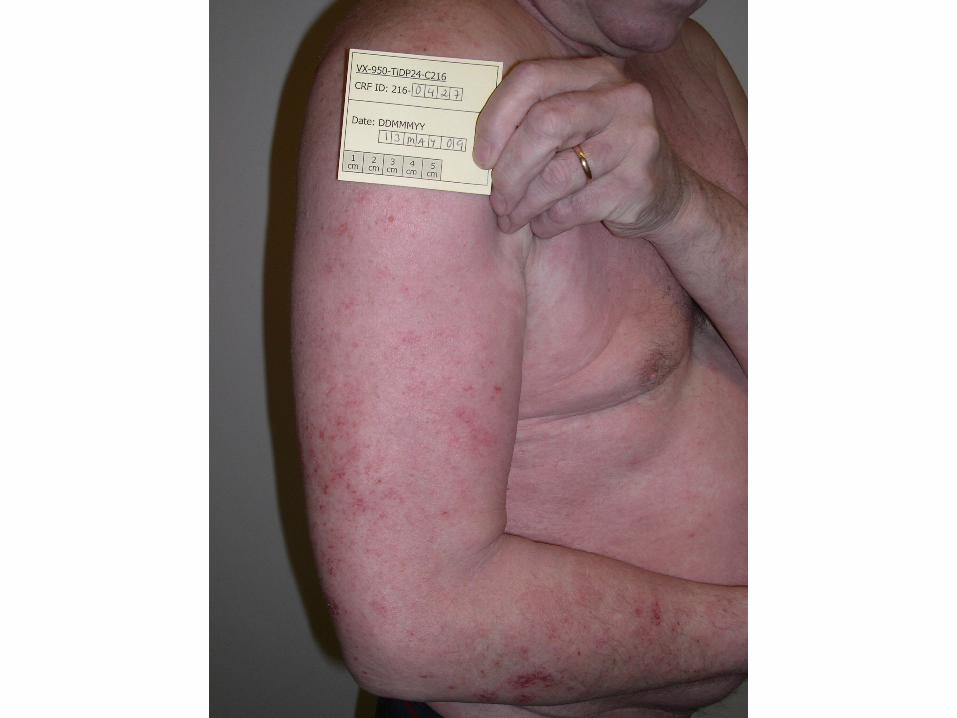

How to manage exanthema?• Stop Rx ? • Continue Rx ?
• Treat the exanthema and continue Rx ?
• Switch PI ?
How to manage exanthema?
• Initially Rx was continued • Topical-steroids were given
• Desloratadine for pruritus
Outcome of exanthema?
• Continued to progress • Week 8

What to do?
• Continue Rx with topical steroids ? • Stop TVR week 8 ?
•Other measures ?
Treatment was stopped week 8Due to exanthema and pruritus?
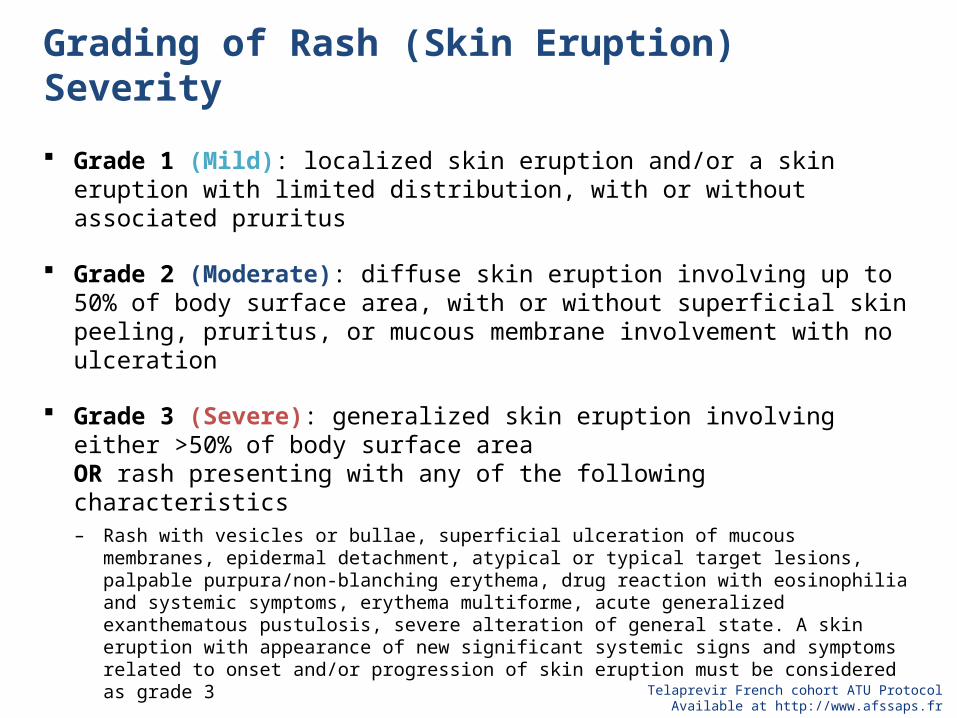
Grading of Rash (Skin Eruption) Severity
Grade 1 (Mild): localized skin eruption and/or a skin eruption with limited distribution, with or without associated pruritus
Grade 2 (Moderate): diffuse skin eruption involving up to 50% of body surface area, with or without superficial skin peeling, pruritus, or mucous membrane involvement with no ulceration
Grade 3 (Severe): generalized skin eruption involving either >50% of body surface area OR rash presenting with any of the following characteristics– Rash with vesicles or bullae, superficial ulceration of mucous membranes, epidermal detachment,
atypical or typical target lesions, palpable purpura/non-blanching erythema, drug reaction with eosinophilia and systemic symptoms, erythema multiforme, acute generalized exanthematous pustulosis, severe alteration of general state. A skin eruption with appearance of new significant systemic signs and symptoms related to onset and/or progression of skin eruption must be considered as grade 3
Grade 4 (life-threatening):
– Toxic epidermal necrolysis, Stevens-Johnson syndrome, skin eruption with generalized bullous eruption
Telaprevir French cohort ATU ProtocolAvailable at http://www.afssaps.fr
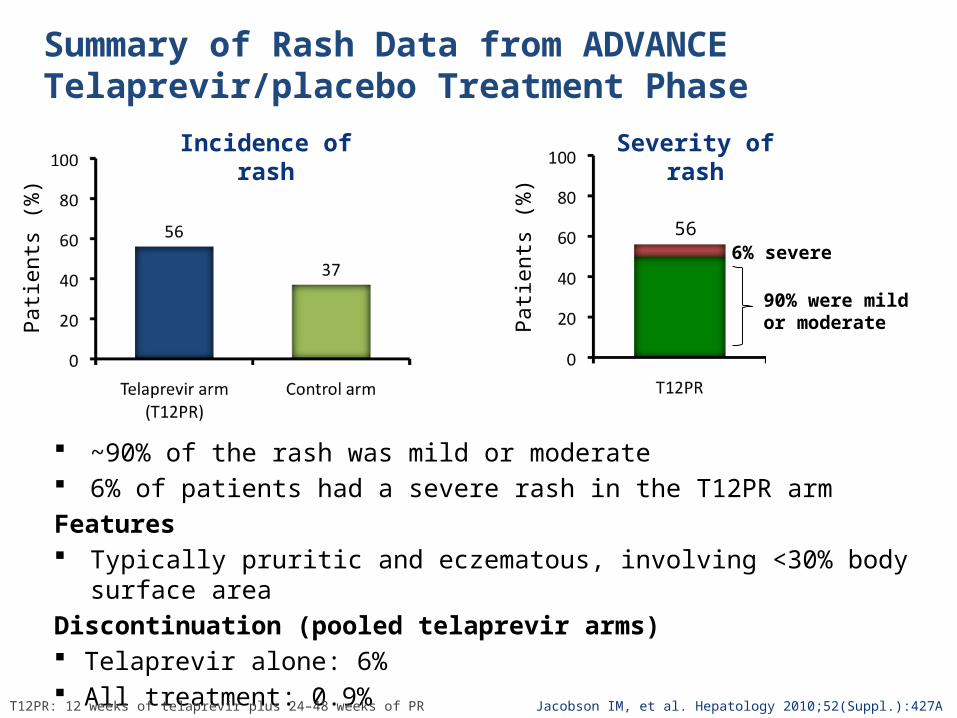
Summary of Rash Data from ADVANCE Telaprevir/placebo Treatment Phase
~90% of the rash was mild or moderate 6% of patients had a severe rash in the T12PR armFeatures Typically pruritic and eczematous, involving <30% body surface areaDiscontinuation (pooled telaprevir arms) Telaprevir alone: 6% All treatment: 0.9%
Jacobson IM, et al. Hepatology 2010;52(Suppl.):427A
Patie
nts
(%)
Patie
nts
(%)
566% severe
90% were mild or moderate
Incidence of rash Severity of rash
T12PR: 12 weeks of telaprevir plus 24–48 weeks of PR
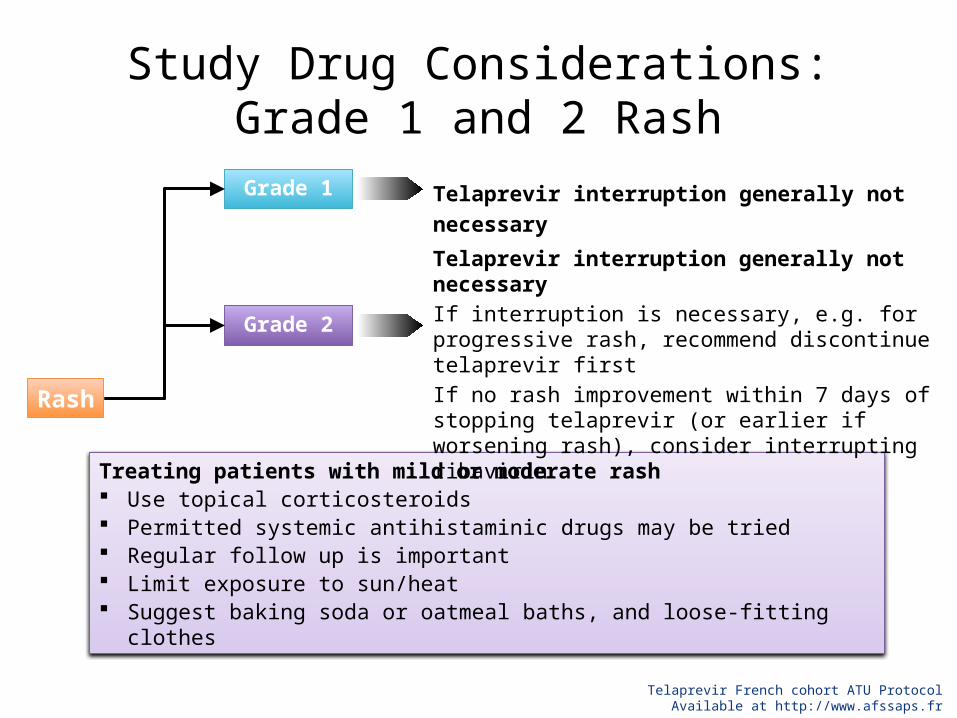
Study Drug Considerations: Grade 1 and 2 Rash
Treating patients with mild or moderate rash Use topical corticosteroids Permitted systemic antihistaminic drugs may be tried Regular follow up is important Limit exposure to sun/heat Suggest baking soda or oatmeal baths, and loose-fitting clothes
Rash
Grade 1
Grade 2
Telaprevir interruption generally not necessary
Telaprevir interruption generally not necessaryIf interruption is necessary, e.g. for progressive rash, recommend discontinue telaprevir firstIf no rash improvement within 7 days of stopping telaprevir (or earlier if worsening rash), consider interrupting ribavirin
Telaprevir French cohort ATU ProtocolAvailable at http://www.afssaps.fr
How should exanthema be treated
• Lubricants
• Topical steroiders : betamethasone – 10 days b.i.d.– 10 days q.d.– 10 every other day
• Desloratadine (Aerius®) once daily for pruritus
What SVR rate does the shortening of Telaprevir from 12 to 8 weeks Rx offer ?
1. 50%
2. 55%
3. 60%
4. 69%

ADVANCE: SVR Rates in Telaprevir-treated Patients compared with PR Alone
Jacobson IM, et al. Hepatology 2010;52(Suppl.):427AT8PR: 8 weeks of telaprevir plus 24–48 weeks of PR; *p<0.0001 vs PR48
**
6% difference(95% CI: –12.5% to +0.6%)
T12PR
271/363
T8PR
250/364
PR48
158/361n/N =
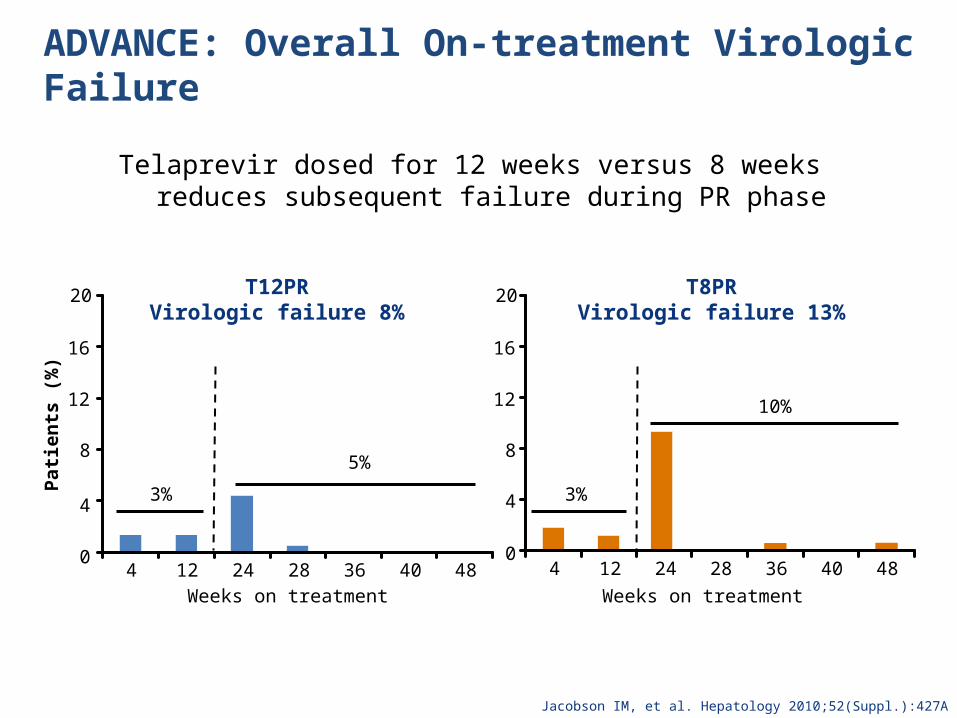
ADVANCE: Overall On-treatment Virologic Failure
Telaprevir dosed for 12 weeks versus 8 weeks reduces subsequent failure during PR phase
T12PRVirologic failure 8%
0
4
8
12
16
20
4 12 24 28 36 40 48Weeks on treatment
Patie
nts
(%)
4 12 24 28 36 40 48Weeks on treatment
T8PRVirologic failure 13%
3%
5%
3%
10%
0
4
8
12
16
20
Jacobson IM, et al. Hepatology 2010;52(Suppl.):427A
The outcome of our case?
• The exanthema vanished rapidly • Pruritus vanished rapidly
• SOC treatment was continued
• SVR was reached
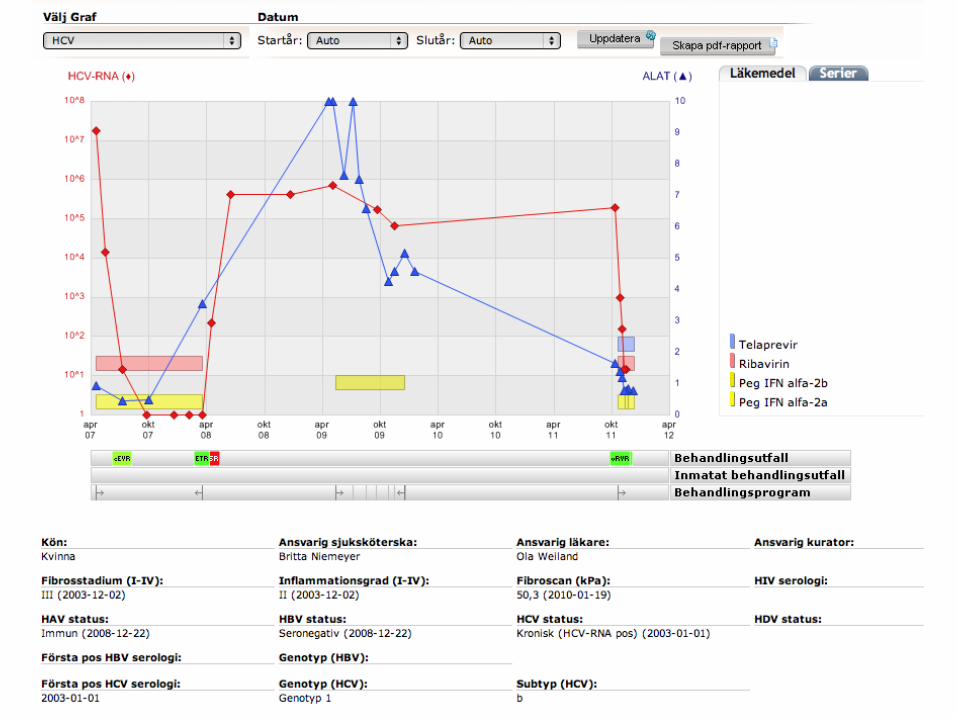
Case number 2
Case no 2 57 year old lady1• 2005 advanced HCV • HCV gt 1b• Biopsy 2003 Fibrosis stage F3, A2• Treatment with peg-IFN ribavirin
prolonged to 72 weeks - response-relapse
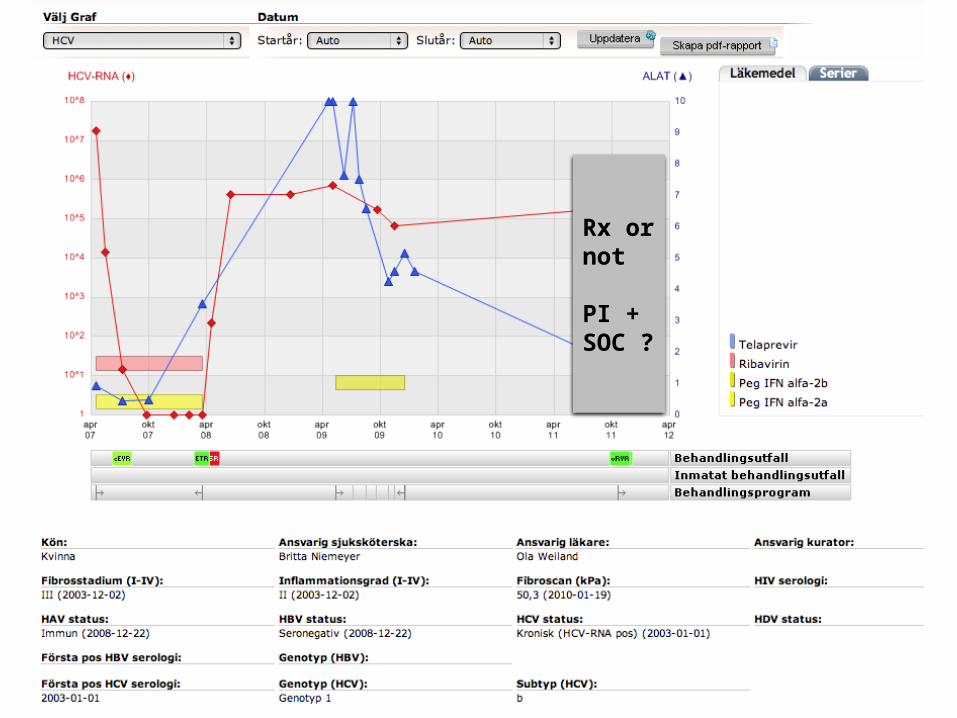
57 yr old lady2
• 2010 advanced cirrhosis• Fibroscan mean kPa 50• No focal lesion on ultrasound• No major varices• Earlier Multiforme exanthem on peg-IFN
alfa 2b but not on alfa-2a• Desired treatment
57 year old lady3
• At baseline• ALT /AST 1,63/1,52 µkat/L• Platelets 51 x 109/L• Neutrophils 2 x 109/L
57 year old lady
• Should treatment be offered ?
• Are low platelets a contraindication ?
Rx or not
PI + SOC ?
57 year old lady3
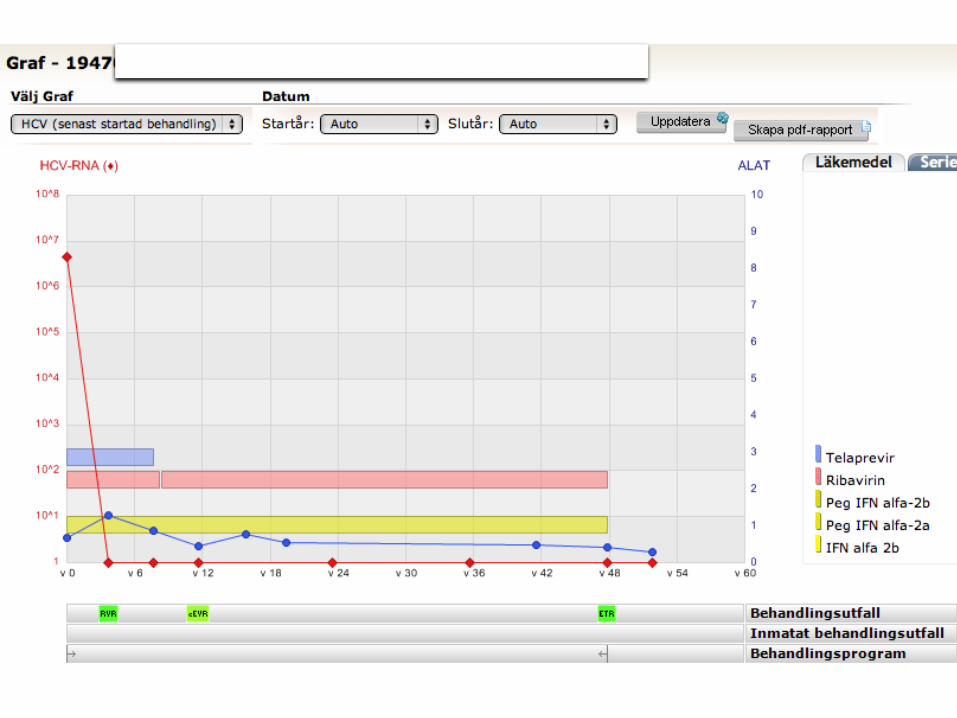
• Treatment was given• Telaprevir + peg-IFN alfa2a + ribavirin
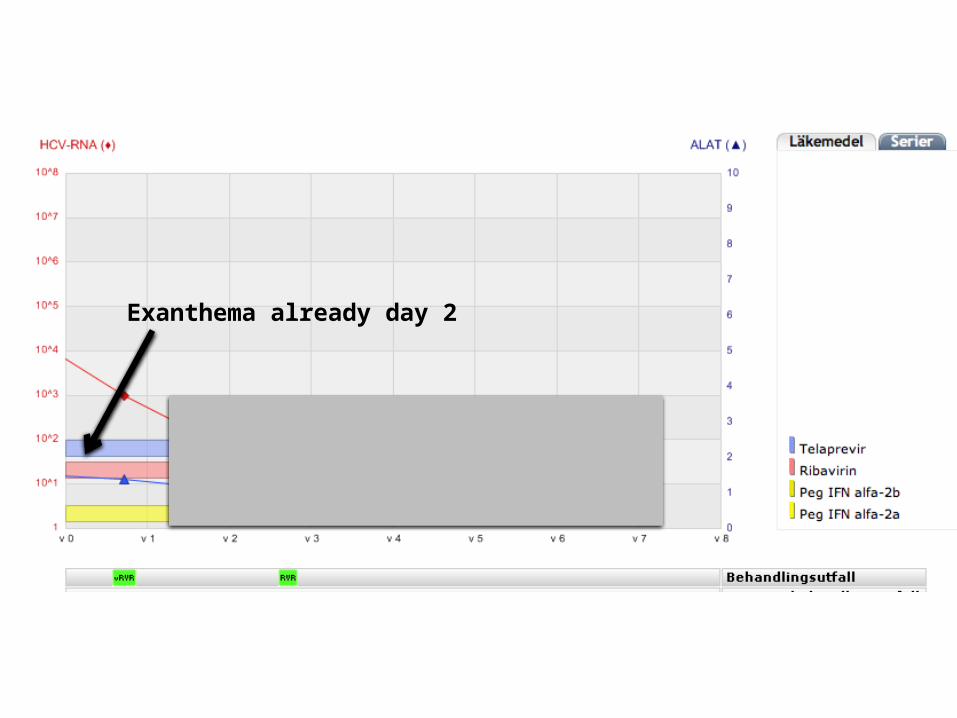
Exanthema already day 2


57 year old lady
• Stop Rx ?• Continue Rx and use exanthema plan ?• Switch PI?• Other option ?
Treatment was con-d and for the exanthema the following was given
• Lubricants
• Topical steroiders : betamethasone – 10 days b.i.d.– 10 days q.d.– 10 every other day
• Desloratadine (Aerius®) once daily for pruritus
What happened with the patient?
• The exanthema vanished rapidly
• Pruritus vanished rapidly
• Tripel therapy was continued
• RVR was achieved

Anemia during PI treatment
• Management
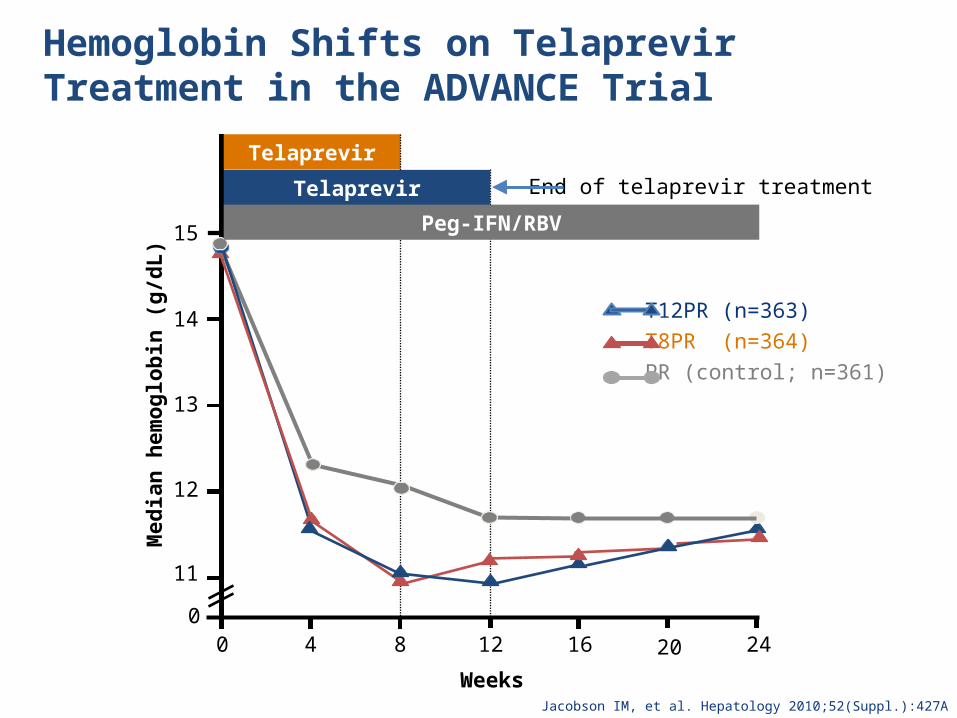
Hemoglobin Shifts on Telaprevir Treatment in the ADVANCE Trial
Jacobson IM, et al. Hepatology 2010;52(Suppl.):427A
0
Med
ian
hem
oglo
bin
(g/d
L)
Weeks
0
11
12
13
14
15
4 8 12 16 20 24
Telaprevir
T12PR (n=363)T8PR (n=364) PR (control; n=361)
Telaprevir End of telaprevir treatment
Peg-IFN/RBV
Sulkowsky et al 2011
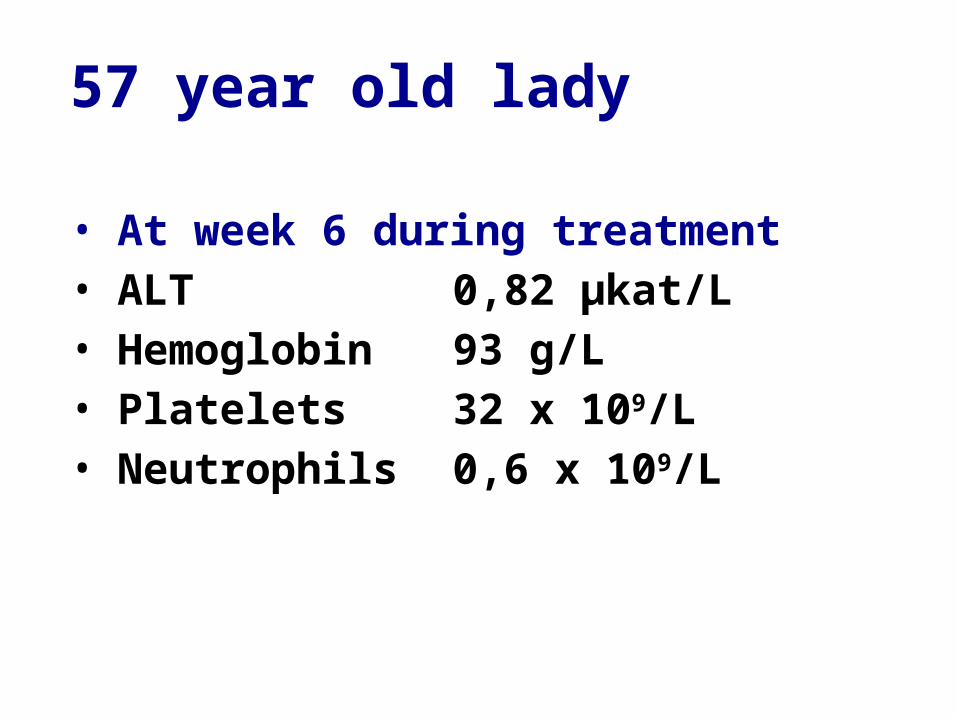
57 year old lady
• At week 6 during treatment• ALT 0,82 µkat/L• Hemoglobin 93 g/L• Platelets 32 x 109/L• Neutrophils 0,6 x 109/L
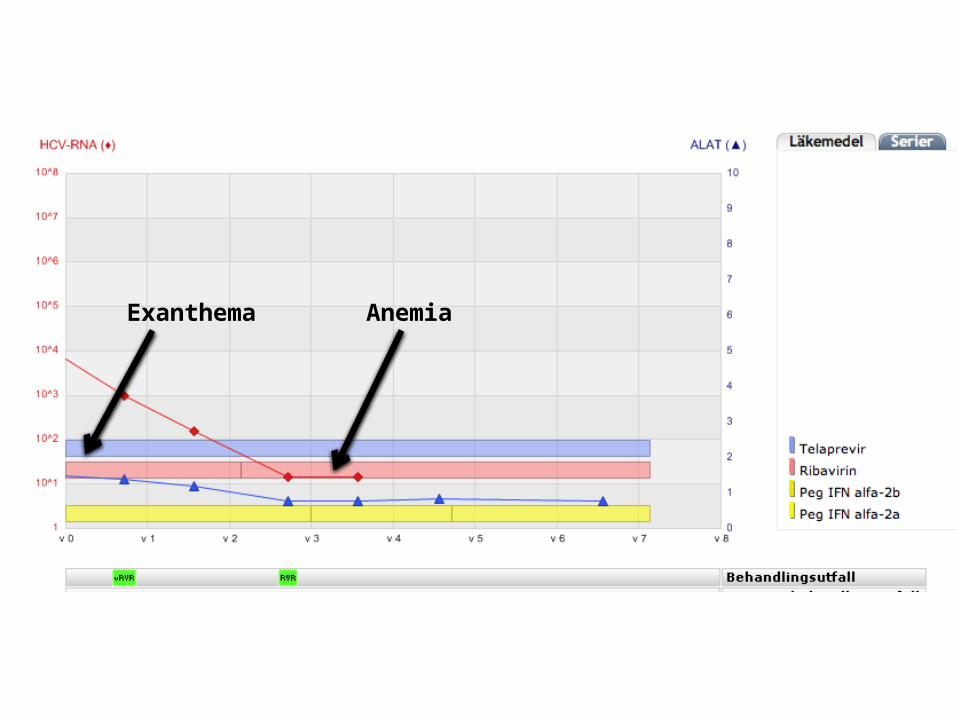
Exanthema Anemia
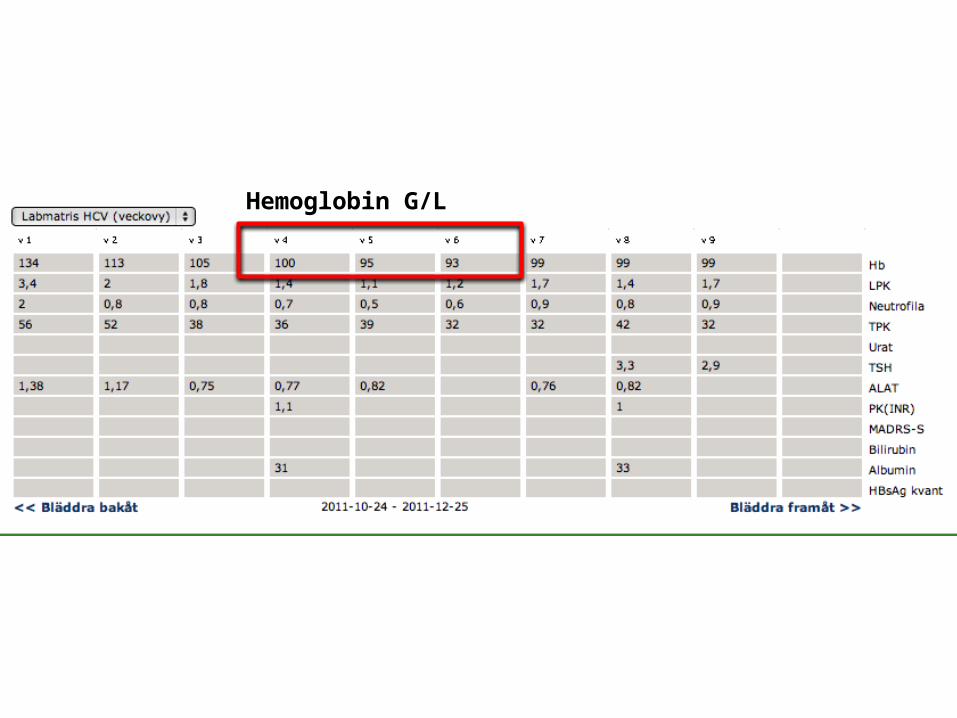
Hemoglobin G/L

Hemoglobin G/L
Ribavirin dose was reduced and Rx continued
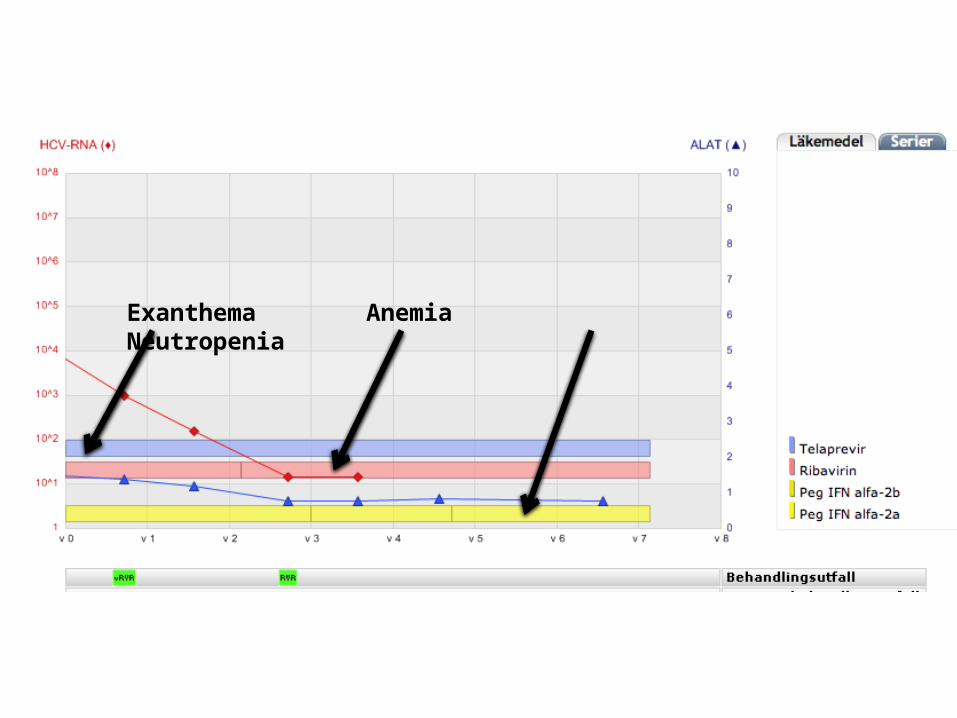
Exanthema AnemiaNeutropenia
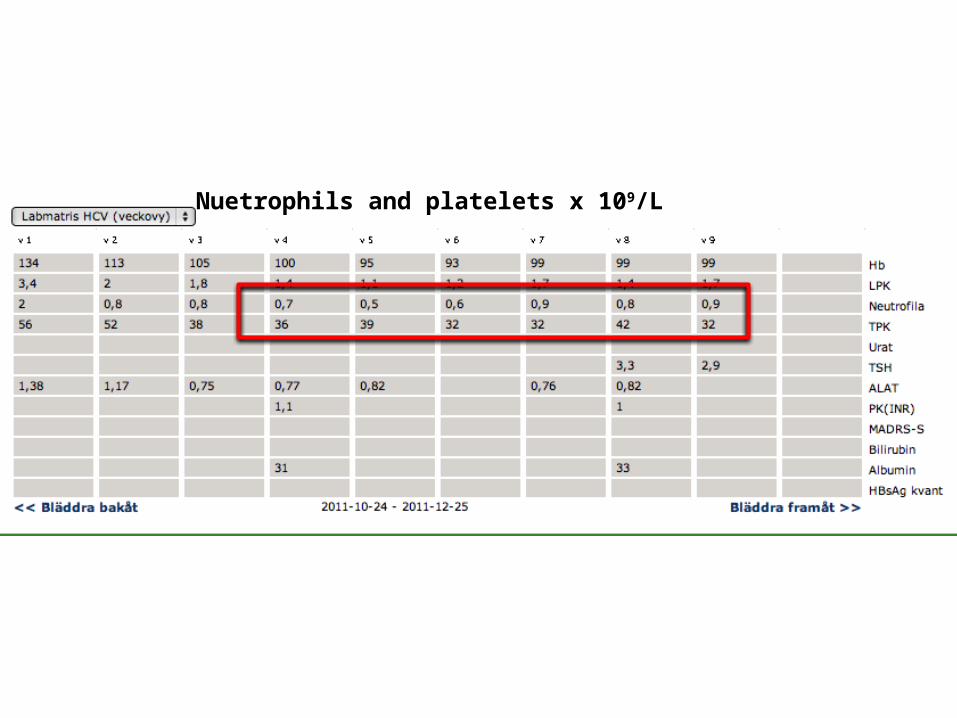
Nuetrophils and platelets x 109/L
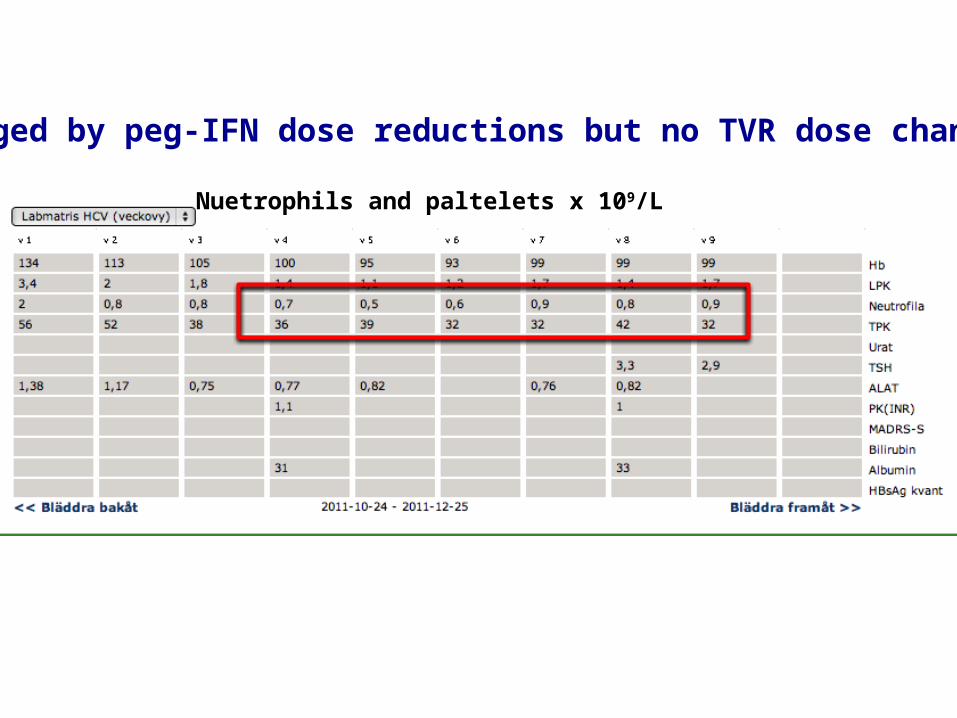
Nuetrophils and paltelets x 109/L
Managed by peg-IFN dose reductions but no TVR dose change


Effect of Anemia on Efficacy in Treatment-naïve Patients who Received Telaprevir
Patients with anemia Patients without anemia
T12PR24
149/196
T12PR
267/361
T12PR48
118/165
PR
46/92
T12PR24
206/269
T12PR
384/524
T12PR48
178/255
PR
108/262n/N=
SVR
(%)
Pooled analysis: ADVANCE and ILLUMINATE Phase III studies
Sulkowski MS, et al. J Hepatol 2011;54(Suppl.):S195
Sulkowsky et al 2011
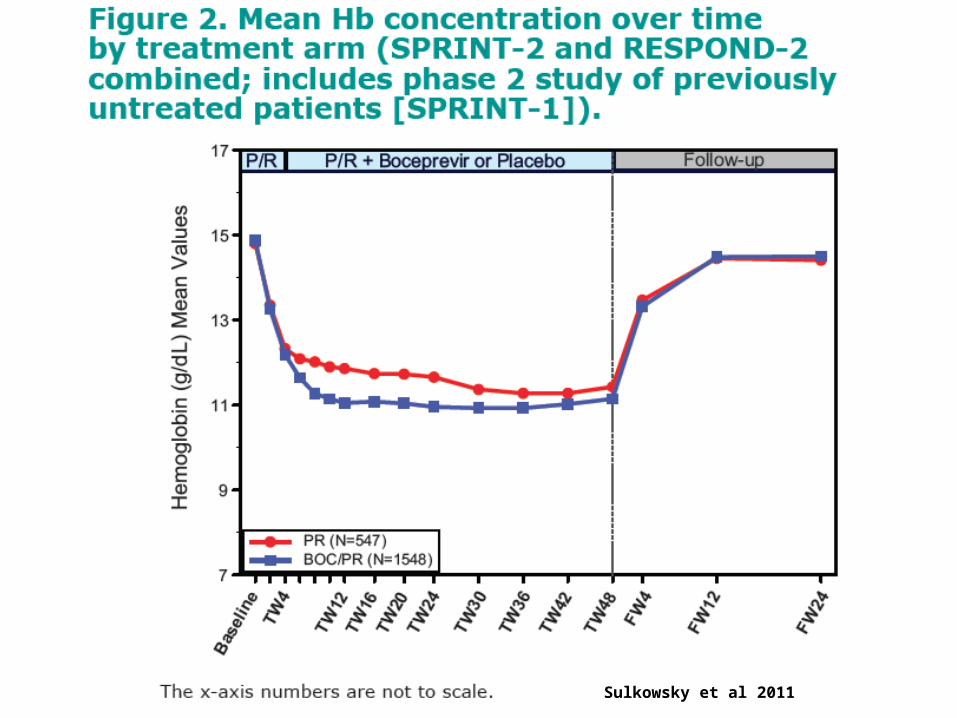
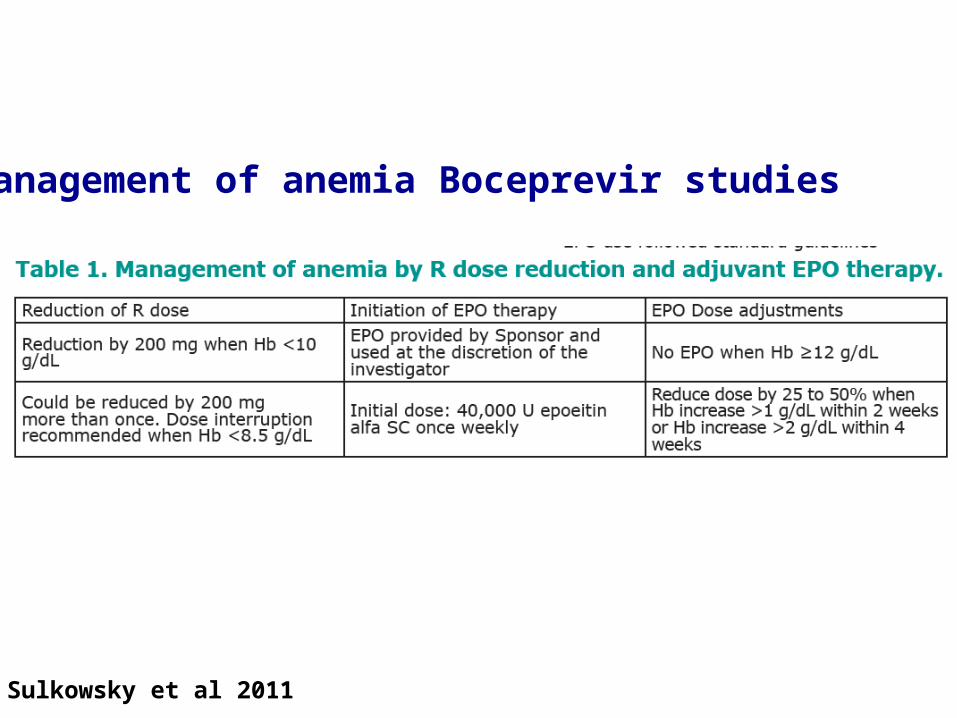
Management of anemia Boceprevir studies
Sulkowsky et al 2011
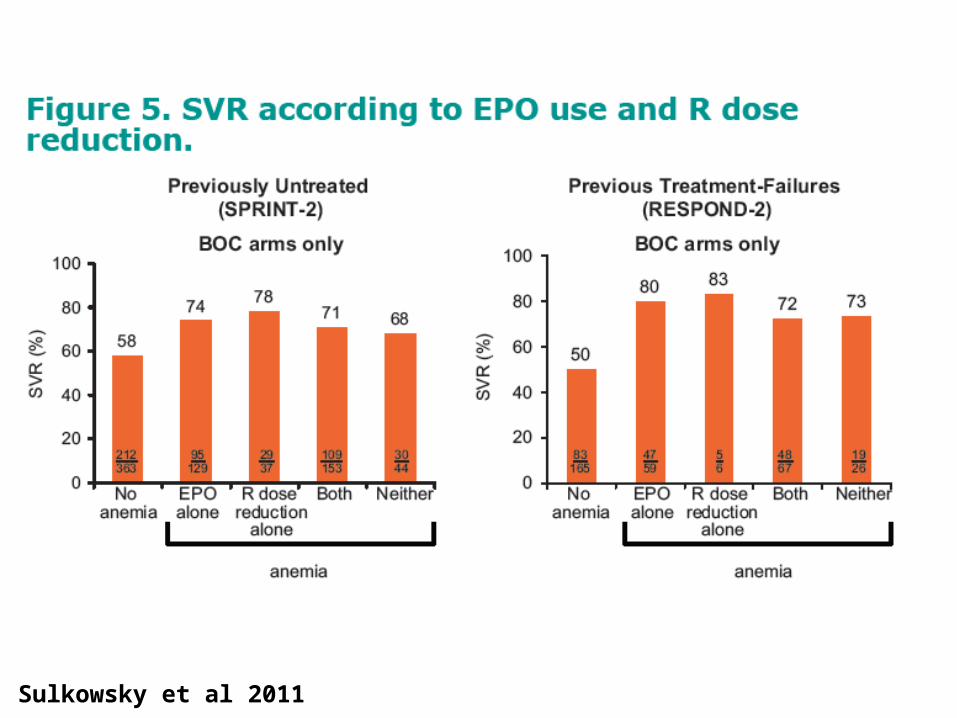
Sulkowsky et al 2011
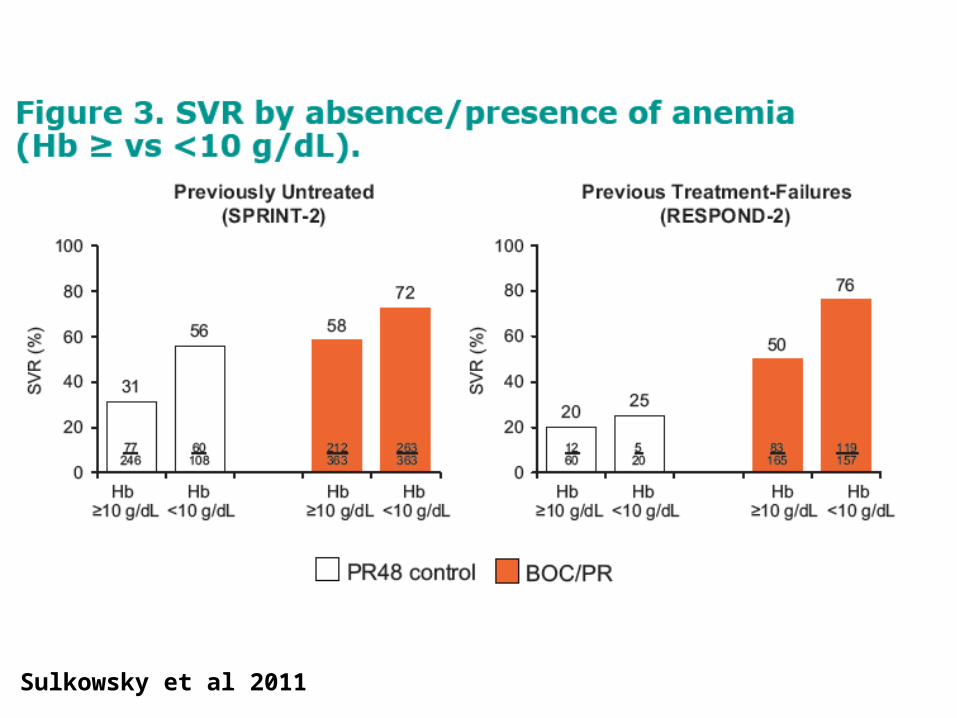
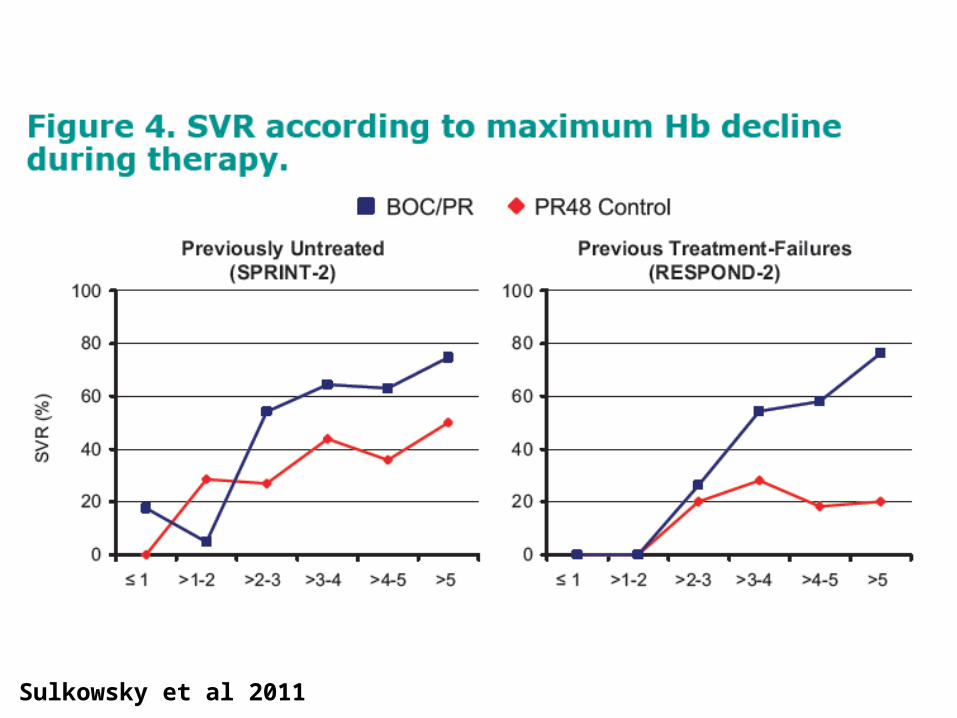
Sulkowsky et al 2011
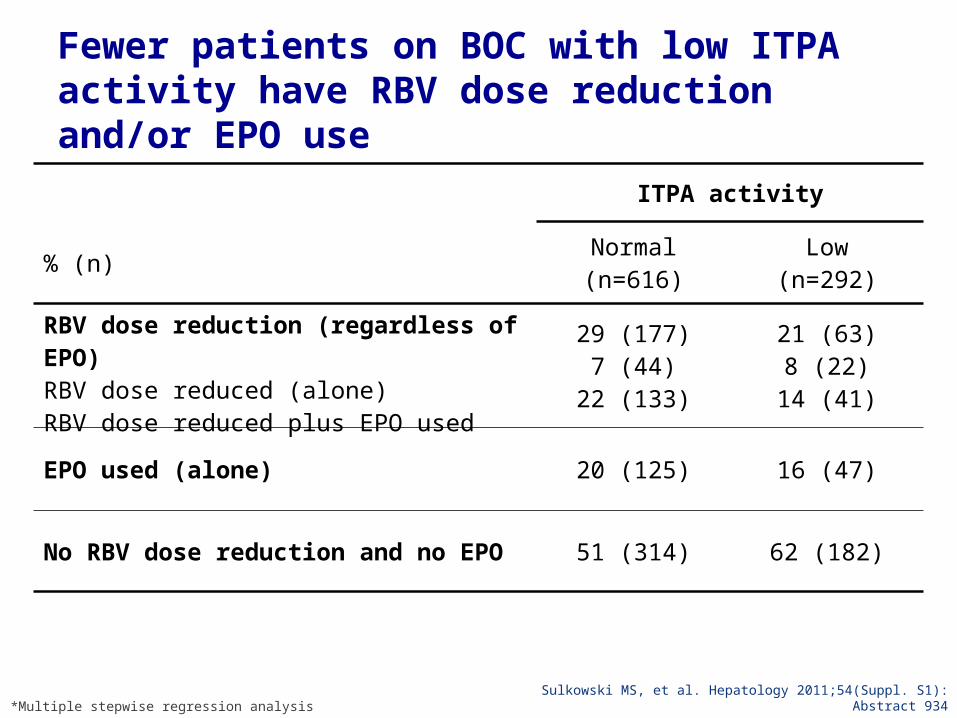
Fewer patients on BOC with low ITPA activity have RBV dose reduction and/or EPO use
Sulkowski MS, et al. Hepatology 2011;54(Suppl. S1): Abstract 934*Multiple stepwise regression analysis
ITPA activity
% (n)Normal(n=616)
Low(n=292)
RBV dose reduction (regardless of EPO)RBV dose reduced (alone)RBV dose reduced plus EPO used
29 (177)7 (44)
22 (133)
21 (63)8 (22)
14 (41)
EPO used (alone) 20 (125) 16 (47)
No RBV dose reduction and no EPO 51 (314) 62 (182)
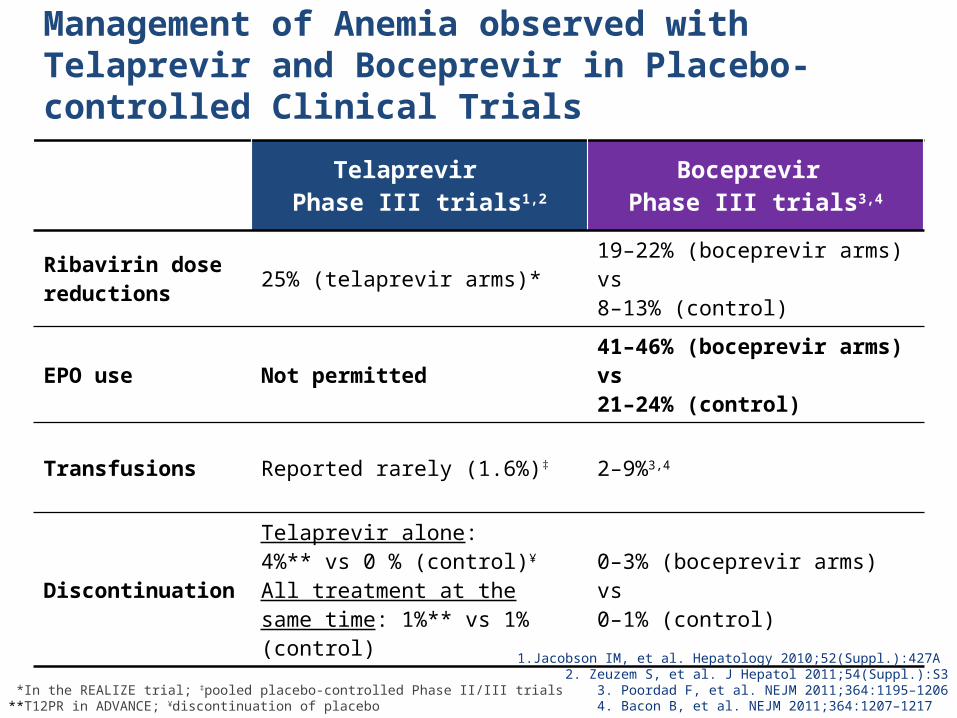
Management of Anemia observed with Telaprevir and Boceprevir in Placebo-controlled Clinical Trials
Telaprevir Phase III trials1,2
Boceprevir Phase III trials3,4
Ribavirin dose reductions 25% (telaprevir arms)* 19–22% (boceprevir arms) vs
8–13% (control)
EPO use Not permitted 41–46% (boceprevir arms) vs 21–24% (control)
Transfusions Reported rarely (1.6%)‡ 2–9%3,4
DiscontinuationTelaprevir alone: 4%** vs 0 % (control)¥
All treatment at the same time: 1%** vs 1% (control)
0–3% (boceprevir arms) vs 0–1% (control)
1.Jacobson IM, et al. Hepatology 2010;52(Suppl.):427A 2. Zeuzem S, et al. J Hepatol 2011;54(Suppl.):S33. Poordad F, et al. NEJM 2011;364:1195–12064. Bacon B, et al. NEJM 2011;364:1207–1217
*In the REALIZE trial; ‡pooled placebo-controlled Phase II/III trials**T12PR in ADVANCE; ¥discontinuation of placebo


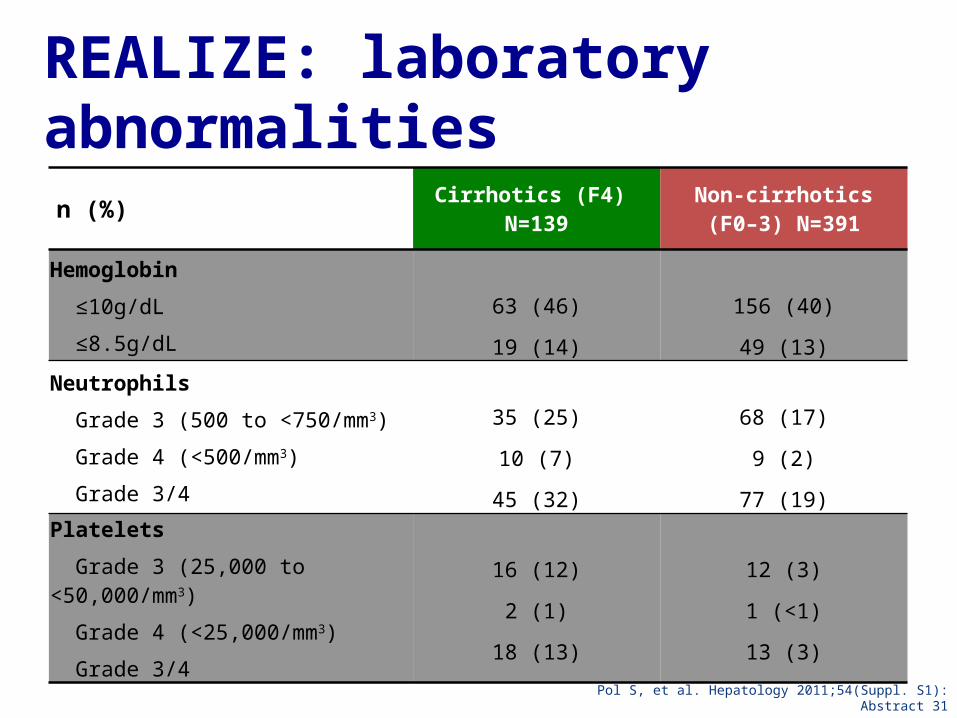
REALIZE: laboratory abnormalities
n (%) Cirrhotics (F4) N=139
Non-cirrhotics (F0–3) N=391
Hemoglobin
≤10g/dL
≤8.5g/dL
63 (46)
19 (14)
156 (40)
49 (13)Neutrophils
Grade 3 (500 to <750/mm3)
Grade 4 (<500/mm3)
Grade 3/4
35 (25)
10 (7)
45 (32)
68 (17)
9 (2)
77 (19)Platelets
Grade 3 (25,000 to <50,000/mm3)
Grade 4 (<25,000/mm3)
Grade 3/4
16 (12)
2 (1)
18 (13)
12 (3)
1 (<1)
13 (3)
Pol S, et al. Hepatology 2011;54(Suppl. S1): Abstract 31
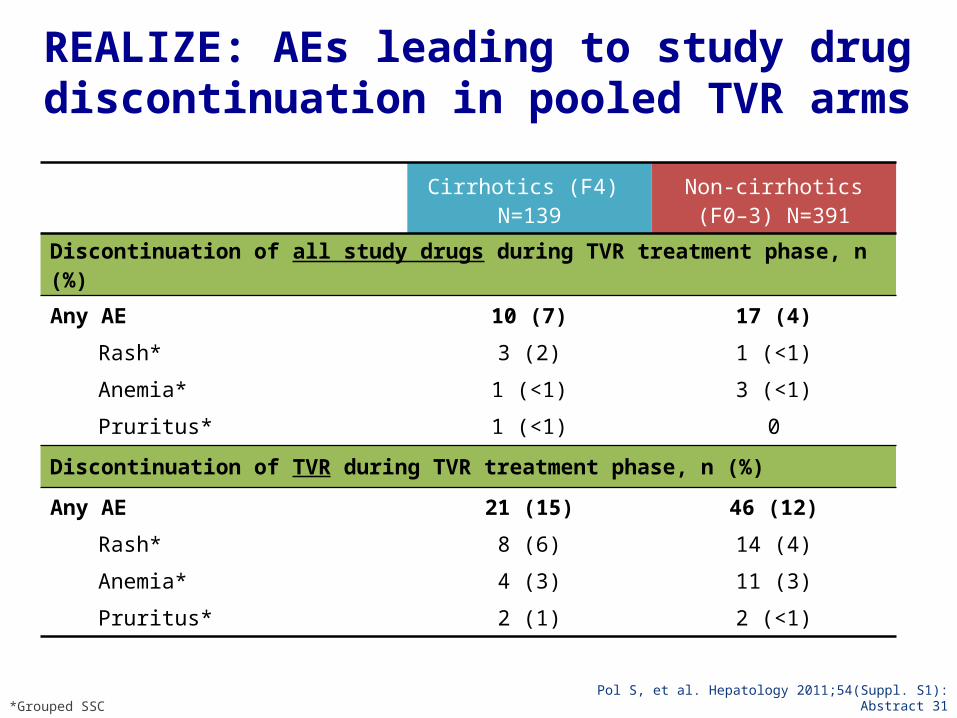
REALIZE: AEs leading to study drug discontinuation in pooled TVR arms
Cirrhotics (F4) N=139
Non-cirrhotics (F0–3) N=391
Discontinuation of all study drugs during TVR treatment phase, n (%)
Any AERash*Anemia*Pruritus*
10 (7)3 (2)
1 (<1)1 (<1)
17 (4)1 (<1)3 (<1)
0
Discontinuation of TVR during TVR treatment phase, n (%)
Any AERash*Anemia*Pruritus*
21 (15)8 (6)4 (3)2 (1)
46 (12)14 (4)11 (3)2 (<1)
Pol S, et al. Hepatology 2011;54(Suppl. S1): Abstract 31*Grouped SSC
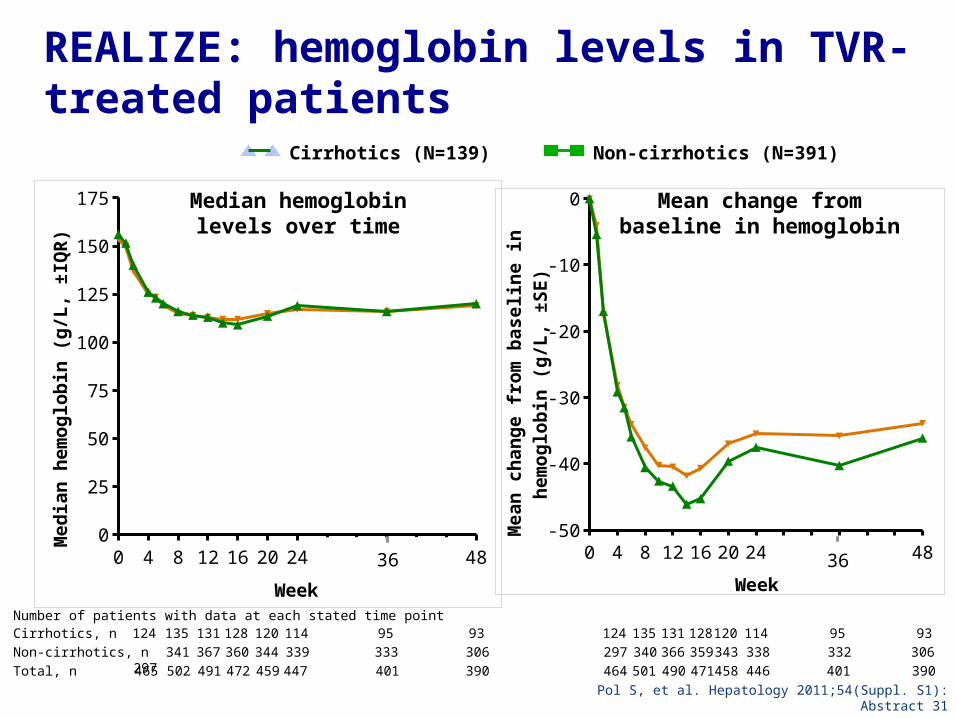
REALIZE: hemoglobin levels in TVR-treated patients
0 4 8 12 16 20 24 28 32 36 40 44 480
25
50
75
100
125
150
175
Week
Me
dia
n h
em
og
lob
in (
g/L
, ±IQ
R)
0 4 8 12 16 20 24 28 32 36 40 44 48-50
-40
-30
-20
-10
0
Week
Me
an
ch
an
ge
fro
m b
as
elin
e in
h
em
og
lob
in (
g/L
, ±S
E)
Median hemoglobin levels over time
Mean change from baseline in hemoglobin
Cirrhotics, n 124 135 131 128 120 114 95 93 124 135 131 128 120 114 95 93Non-cirrhotics, n 341 367 360 344 339 333 306 297 340 366 359 343 338 332 306 297Total, n 465 502 491 472 459 447 401 390 464 501 490 471 458 446 401 390
36 36
Number of patients with data at each stated time point
Pol S, et al. Hepatology 2011;54(Suppl. S1): Abstract 31
Cirrhotics (N=139) Non-cirrhotics (N=391)
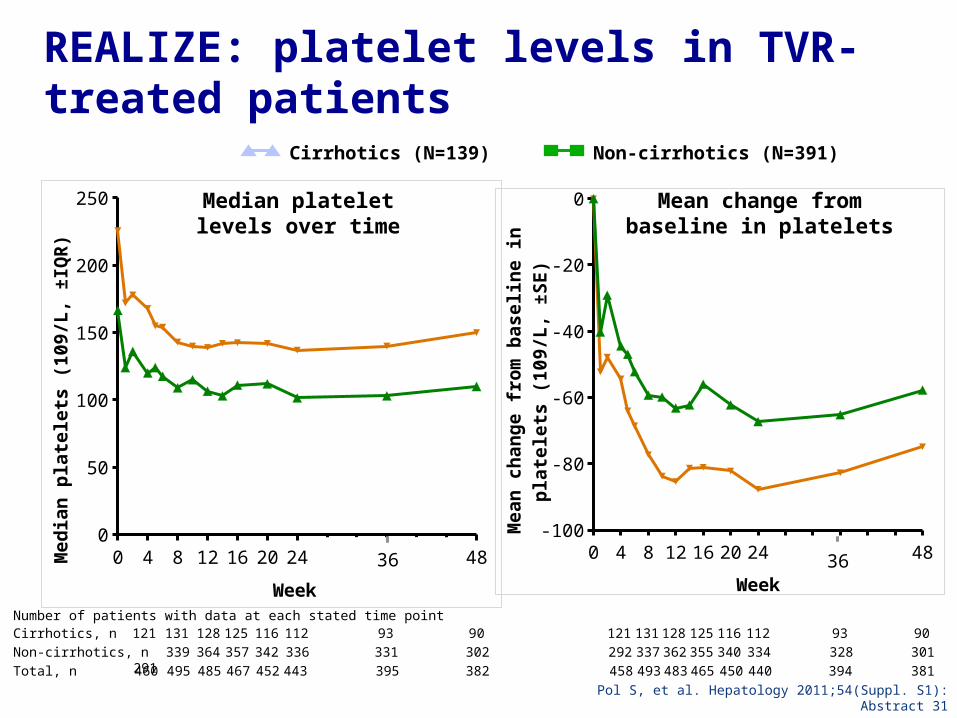
REALIZE: platelet levels in TVR-treated patients
0 4 8 12 16 20 24 28 32 36 40 44 480
50
100
150
200
250
Week
Me
dia
n p
late
lets
(1
09
/L, ±
IQR
)
0 4 8 12 16 20 24 28 32 36 40 44 48-100
-80
-60
-40
-20
0
Week
Me
an
ch
an
ge
fro
m b
as
elin
e in
p
late
lets
(1
09
/L, ±
SE
)
Median platelet levels over time
Mean change from baseline in platelets
Cirrhotics, n 121 131 128 125 116 112 93 90 121 131 128 125 116 112 93 90Non-cirrhotics, n 339 364 357 342 336 331 302 292 337 362 355 340 334 328 301 291Total, n 460 495 485 467 452 443 395 382 458 493 483 465 450 440 394 381
36 36
Number of patients with data at each stated time point
Pol S, et al. Hepatology 2011;54(Suppl. S1): Abstract 31
Cirrhotics (N=139) Non-cirrhotics (N=391)
Case no 3
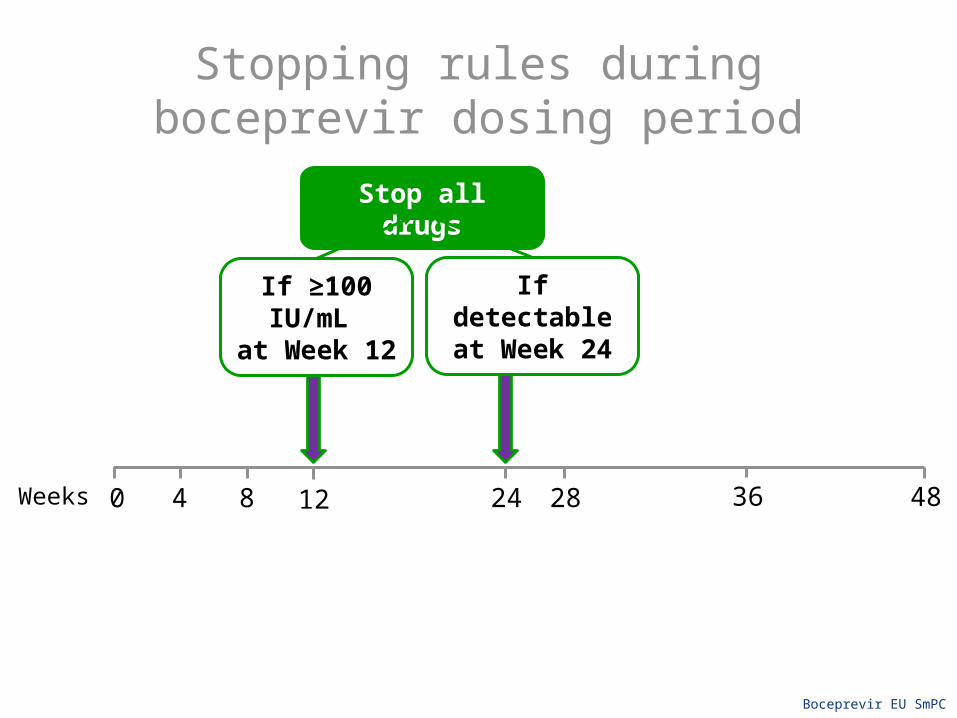
Stopping rules during boceprevir dosing period
0 48Weeks 284 8 24 3612
If ≥100 IU/mL at Week 12
If detectable at Week 24
Stop all drugs
Boceprevir EU SmPC
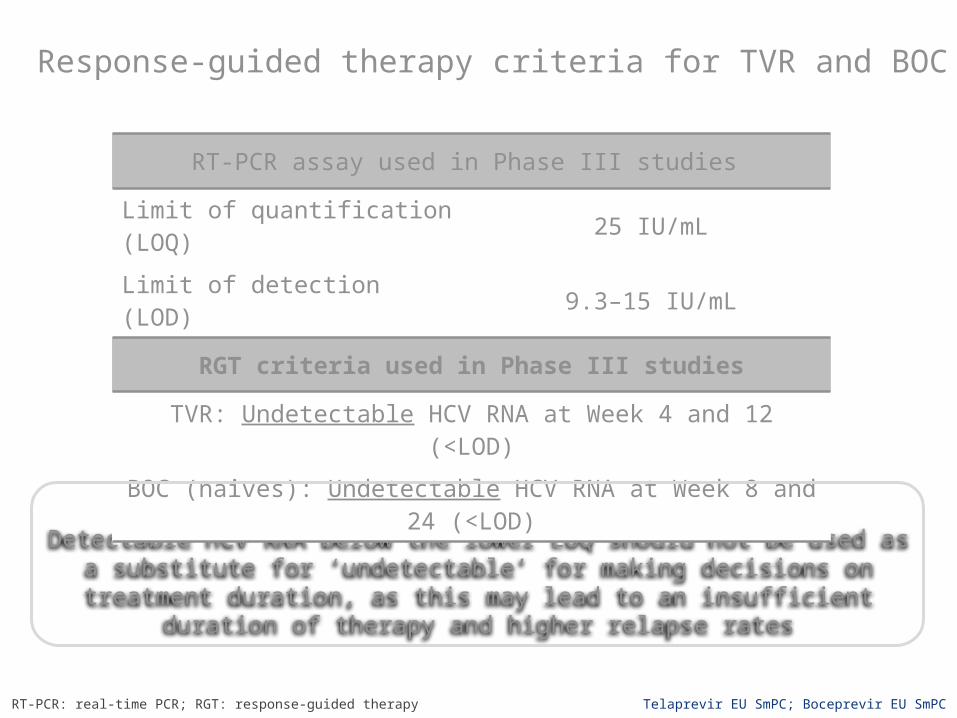
Response-guided therapy criteria for TVR and BOC
TVR SmPC:Detectable HCV RNA below the lower LOQ should not be used as a substitute for ‘undetectable’ for making decisions on treatment duration, as this may lead to an
insufficient duration of therapy and higher relapse rates
RT-PCR assay used in Phase III studies
Limit of quantification (LOQ) 25 IU/mL
Limit of detection (LOD) 9.3–15 IU/mL
RGT criteria used in Phase III studies
TVR: Undetectable HCV RNA at Week 4 and 12 (<LOD)
BOC (naives): Undetectable HCV RNA at Week 8 and 24 (<LOD)
RT-PCR: real-time PCR; RGT: response-guided therapy Telaprevir EU SmPC; Boceprevir EU SmPC
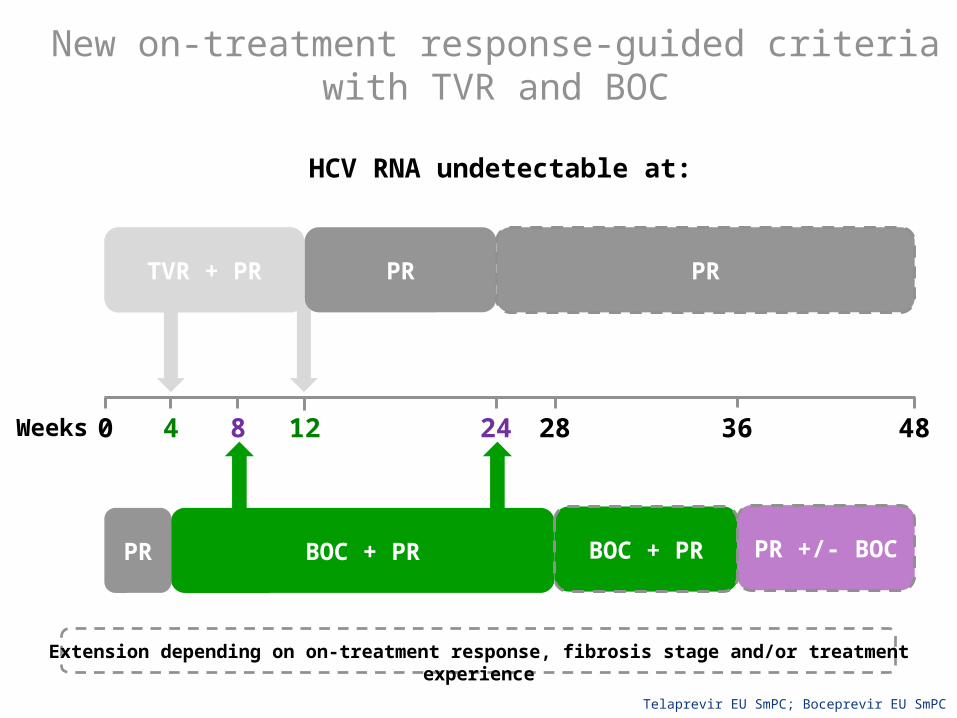
New on-treatment response-guided criteria with TVR and BOC
Telaprevir EU SmPC; Boceprevir EU SmPC
TVR + PR
0 48Weeks 284 8 24 3612
BOC + PR BOC + PR PR +/- BOCPR
PR PR
Extension depending on on-treatment response, fibrosis stage and/or treatment experience
HCV RNA undetectable at:
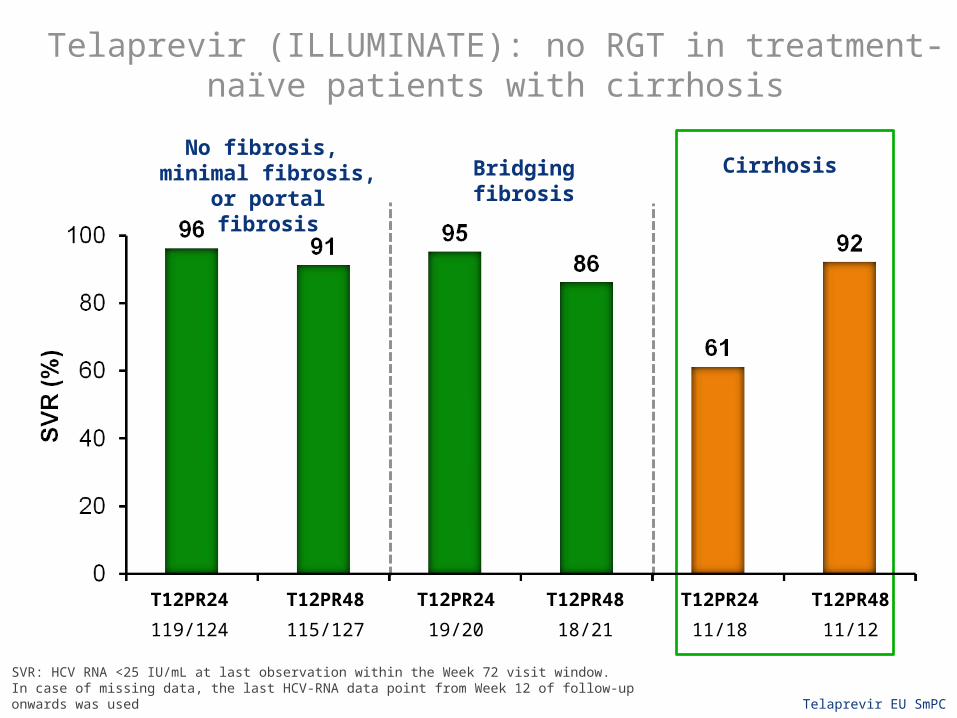
Telaprevir (ILLUMINATE): no RGT in treatment-naïve patients with cirrhosis
22%n=118
T12PR48
115/127
T12PR24
119/124
No fibrosis, minimal fibrosis, or portal fibrosis
Bridging fibrosis Cirrhosis
T12PR24
19/20
T12PR48
18/21
T12PR24
11/18
T12PR48
11/12
Telaprevir EU SmPCSVR: HCV RNA <25 IU/mL at last observation within the Week 72 visit window. In case of missing data, the last HCV-RNA data point from Week 12 of follow-up onwards was used

ADVANCE and ILLUMINATE (telaprevir): eligibility for shorter treatment duration
Series10
20
40
60
80
100
9
70
8
63
Patie
nts
with
und
etec
tabl
e H
CV R
NA
(%)
Week 4 (RVR) Weeks 4 and 12 (eRVR)
Patients eligible to receive 24 weeks
of treatment in total
PR48
34/361
T12PR
635/903
T12PR
565/903
PR48
29/361n/N=
Adapted from Sherman KE, et al. CROI 2011. Abstract 957
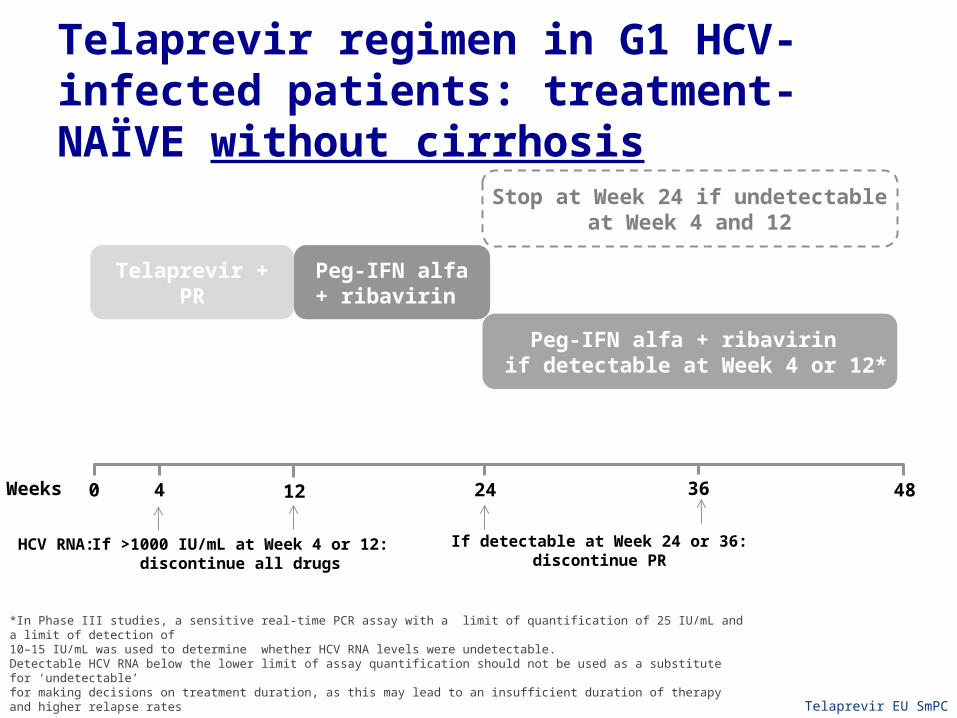
Telaprevir regimen in G1 HCV-infected patients: treatment-NAÏVE without cirrhosis
*In Phase III studies, a sensitive real-time PCR assay with a limit of quantification of 25 IU/mL and a limit of detection of 10–15 IU/mL was used to determine whether HCV RNA levels were undetectable.Detectable HCV RNA below the lower limit of assay quantification should not be used as a substitute for ‘undetectable’for making decisions on treatment duration, as this may lead to an insufficient duration of therapy and higher relapse rates Telaprevir EU SmPC
Peg-IFN alfa + ribavirin if detectable at Week 4 or 12*
Peg-IFN alfa + ribavirin
Stop at Week 24 if undetectable at Week 4 and 12
Telaprevir + PR
If >1000 IU/mL at Week 4 or 12:discontinue all drugs
If detectable at Week 24 or 36:discontinue PR
HCV RNA:
0 48Weeks 4 24 3612
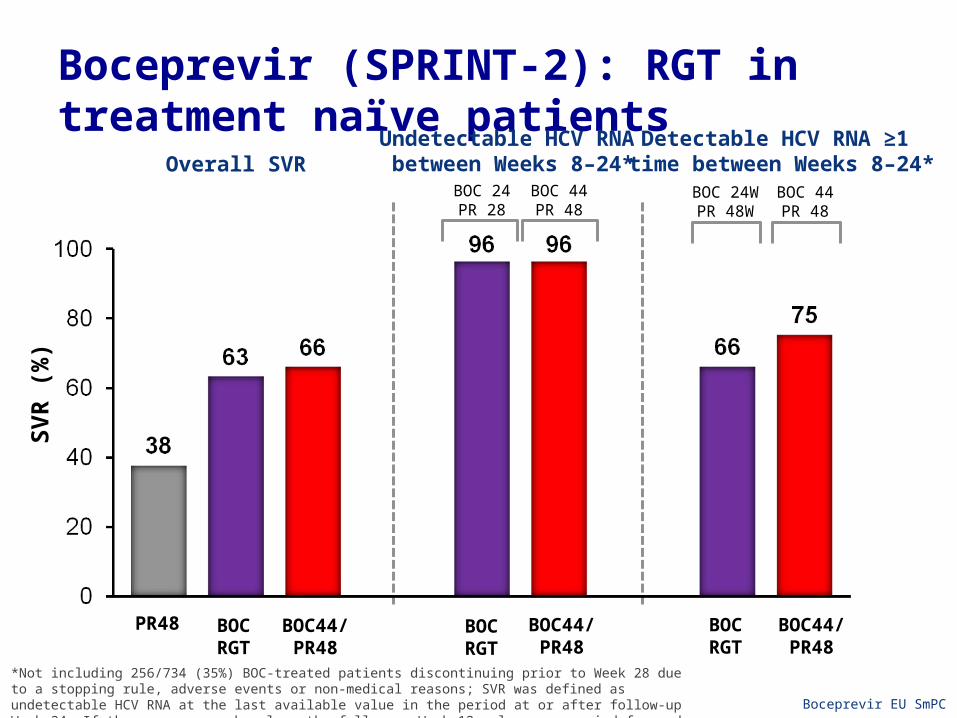
Boceprevir (SPRINT-2): RGT in treatment naïve patients
SVR
(%)
BOC44/PR48
Undetectable HCV RNA between Weeks 8–24*
Detectable HCV RNA ≥1 time between Weeks 8–24*
BOC44/PR48
BOCRGT
*Not including 256/734 (35%) BOC-treated patients discontinuing prior to Week 28 due to a stopping rule, adverse events or non-medical reasons; SVR was defined as undetectable HCV RNA at the last available value in the period at or after follow-up Week 24. If there was no such value, the follow-up Week 12 value was carried forward Boceprevir EU SmPC
BOC 24PR 28
Overall SVR
156/162
BOCRGT
155/161 45/68 55/73
BOC 24WPR 48W
BOC 44PR 48
BOC 44PR 48
BOC44/PR48
BOCRGT
PR48
137/363 233/368 242/366
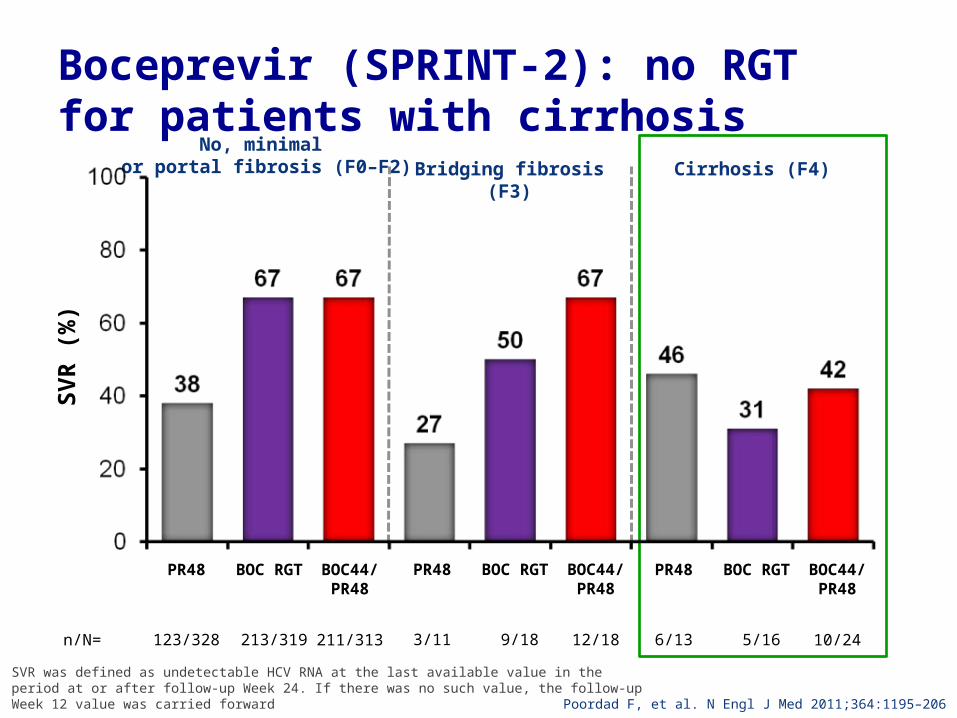
Boceprevir (SPRINT-2): no RGT for patients with cirrhosis
SVR
(%)
PR48
123/328
BOC44/PR48
211/313n/N=
No, minimal or portal fibrosis (F0–F2)
BOC RGT
213/319
Poordad F, et al. N Engl J Med 2011;364:1195–206
Cirrhosis (F4)Bridging fibrosis (F3)
PR48
3/11
BOC44/PR48
12/18
BOC RGT
9/18
PR48
6/13
BOC44/PR48
10/24
BOC RGT
5/16
SVR was defined as undetectable HCV RNA at the last available value in the period at or after follow-up Week 24. If there was no such value, the follow-up Week 12 value was carried forward

Boceprevir regimen in G1 HCV-infected patients: treatment-NAÏVE without cirrhosis
PRlead-in
BOC + PR
0 48Weeks 284 8 24
BOC + PR
36
PR*
If detectable at Week 8 but undetectable at Week 24:
12
HCV RNA
*This regimen has only been tested in patients who have failed previous therapy who were late responders Boceprevir EU SmPC
Assess for RGT criterion
If ≥100 IU/mLdiscontinue all
drugs
If detectablediscontinue all
drugs
Stop treatment at Week 28 if undetectable at Week 8 and 24
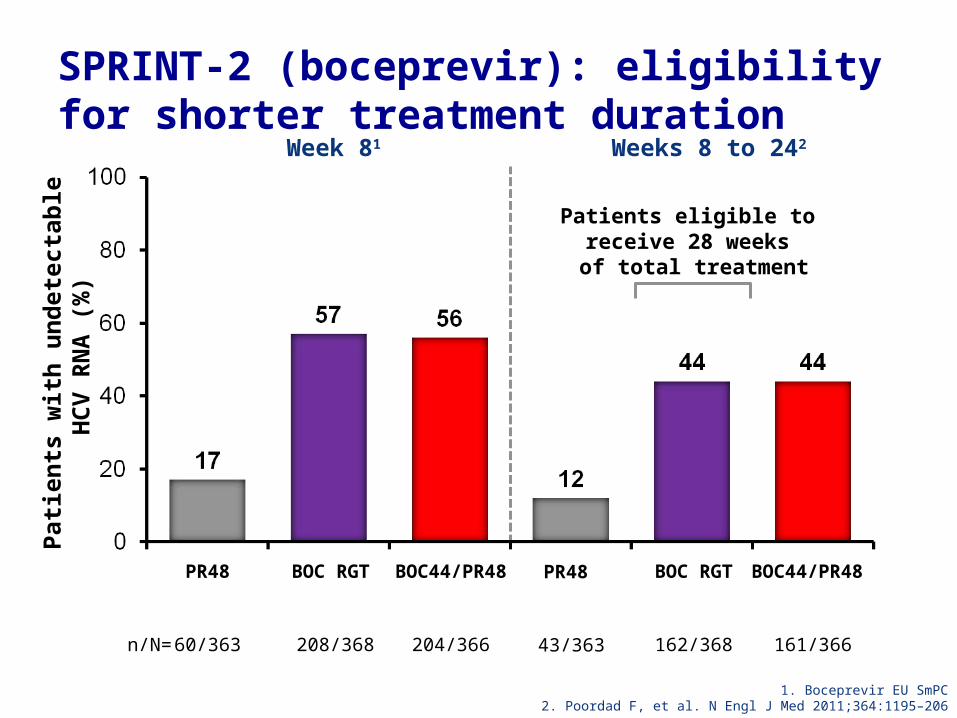
SPRINT-2 (boceprevir): eligibility for shorter treatment duration
Patie
nts
with
und
etec
tabl
e H
CV R
NA
(%)
PR48
60/363
BOC44/PR48
204/366n/N=
Week 81 Weeks 8 to 242
BOC RGT
208/368
BOC44/PR48
161/366
BOC RGT
162/368
Patients eligible to receive 28 weeks of total treatment
1. Boceprevir EU SmPC2. Poordad F, et al. N Engl J Med 2011;364:1195–206
PR48
43/363
4840 12 3624
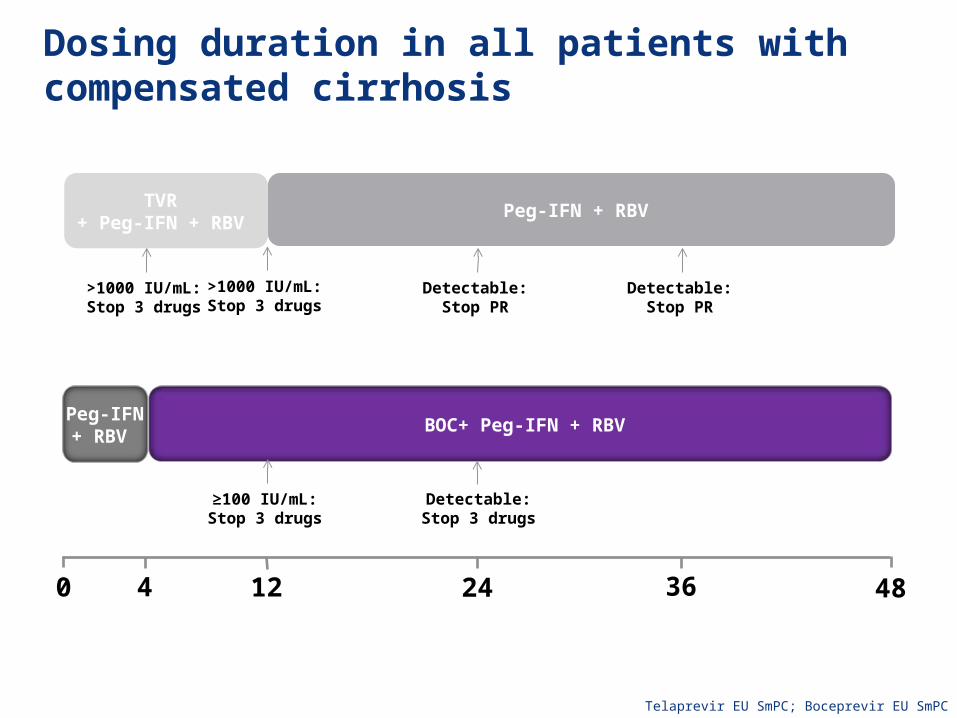
Dosing duration in all patients with compensated cirrhosis
BOC+ Peg-IFN + RBVPeg-IFN + RBV
≥100 IU/mL:Stop 3 drugs
Detectable:Stop 3 drugs
TVR + Peg-IFN + RBV
Peg-IFN + RBV
>1000 IU/mL:Stop 3 drugs
>1000 IU/mL:Stop 3 drugs
Detectable:Stop PR
Detectable:Stop PR
Telaprevir EU SmPC; Boceprevir EU SmPC

HCV RNA levels in patients who met the >1000 IU/mL HCV RNA Week 4 futility rule
Treatment-naïve patients (n=15)
Treatment-experienced patients (n=11)
108
107
106
105
104
103
102
100 4 6 8 12102
Weeks on treatment
HCV
RN
A (IU
/mL)
108
107
106
105
104
103
102
100 4 6 8 12102
Weeks on treatment
HCV
RN
A (IU
/mL)
Adda N, et al. HepDART 2011; Abstract 45
This year has brought a paradigm shift to gt 1 treatmentAddition of a 1st gen protease inhibitor to SOC
-Achieves 30 % higher SVR in naïve HCV genotype 1 patients-Offers shorter treatment for a majority
Thanks

Good Luck with the treatment of your HCV patients 2012
Recommended

















