
SEPSIS Recognition,
Treatment and Referral
Dr. Vida HamiltonNational Clinical Lead Sepsis
www.hse.ie/sepsis

Sepsis - 2
• A dysregulated immune response to infection
• Regulatedo Innate & Adaptive
• Cellular: Dendritic cells, T-cells, B-cells• PAMPs that bind TLR 2,3,4, Mannin-binding lecithin
receptors• (DAMPs)• Molecular: complement, acute phase, cytokines• Anti-viral: Interfon, local cellular immunity, apoptosis

Regulated?
• Local inflammationoVasodilation, capillary leak
• Systemic inflammationo SIRS, CARS

Bone 1996

‘Hyperinflammatory response’ Sepsis – 1
• Control inflammation – improve outcome• Multiple studies
o Steroidso Anti- TNFo Anti-IL1o Anti-IL6 o Other monoclonal antibodies
• At best – no improvement• Often – increased mortality

Drag picture to placeholder or click icon to add
NEJM

Actors• Micro-organism
o Virulenceo Innoculation doseo Multi-drug resistance
• Hosto Genetic polymorphismso Co-morbidities
• Age• Chronic health status• Immuno-modulatory medications

More pathophysiology
• Hotchkiss 2013

Dysregulated?
• Multi-organ dysfunction then failure
o Little necrosis• Apoptosis of the cellular immune system• Anti-inflammatory phase ‘ immunoparalysis’• D4 persistent lymphopenia• ‘Stimulate immune system improve
outcome’
Sepsis-3: A life threatening organ dysfunction caused by a dysregulated host
response to infection
• SOFA scoreo Respiration: PaO2/FiO2 or SaO2/FiO2o Coagulation: Plateletso Liver: Bilirubino Cardiovascular: Hypotension or vasopressoro CNS: GCSo Renal: Creatinine or urinary output
• qSOFAo RR> 22, Altered Mental status, SBP <100
1o outcome: increased specificity in predicting Mortality > 10%; ICU LOS > 3 days

The Burden
• Common
• Sepsis: 330 per 100,000 per annum• AMI: 208 per 100,000 per annum
• Mortality: 20 - 55%

The Burden in Ireland• HIPE data:
o 60% all in-hospital deaths has a sepsis or infection diagnosis
o Number of sepsis cases = 8,770o Number of bed days = 220,288
2013 2012 2011o In-hospital mortality 28.8%
31.3% 32.4%
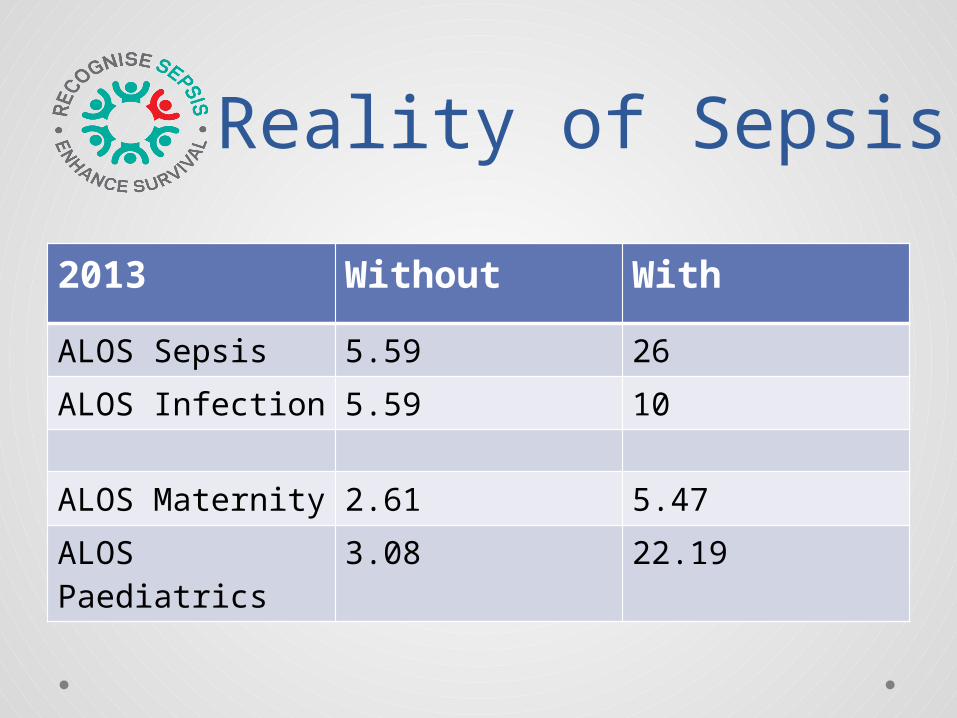
Reality of Sepsis
2013 Without With
ALOS Sepsis 5.59 26ALOS Infection 5.59 10
ALOS Maternity 2.61 5.47ALOS Paediatrics
3.08 22.19

Age standardised hospital discharge rate for medical septic shock, 2005 - 2012

Age standardised hospital discharge rate for surgical septic shock, 2005 - 2012
Costs
• 25,000 euro per acute presentation
• Chronic health burden for survivorsoAnxiety, depression, post-traumatic
stress oMusculo-skeletal, immune suppressiono Shortened life expectancy

Iwashyna et al: Long-term cognitive impairment & functional disability among survivors of severe sepsis. JAMA, 2010.
Cognitive impairment

Issues
• 90% of cases with poor outcome in the Australian sepsis database, inadequate recognition was found to be the most common feature

An Irish Report
• The categorisation of the severity of a patients illness
• The early detection of that deterioration• The use of a standardised and structured
communication tool such as ISBAR• Early medical review that is prompted by
evidence based trigger points• A definite escalation plan that is monitored and
audited on a regular basis

National Sepsis Guidelines
• Aim for decrease in in-hospital mortality by 20% for severe sepsis
• Care pathway for every patient diagnosed with sepsis in Ireland
• Recognition, Resuscitation, Referral• Education, audit

SIRS•Infectious & non infectious causes•Clinical response arising from a non specific insult
Sepsis•SIRS plus•Presumed or confirmed infection
Severe Sepsis•Sepsis plus•Sepsis-induced organ dysfunction or tissue hypoperfusion
Septic Shock•Sepsis-induced hypo-perfusion or hypotension persisting despite 30 mls/kg fluid rescusitation
Diagnostic criteria for sepsis

SIRS Criteria• T > 38.3, < 36• HR > 90• RR > 20• WCC > 12, < 4• BSL > 7.7 mmol/l in non-diabetic• Altered mental status
Common mistake - 1• Other inflammatory parameters
o CRP, PCT• Organ dysfunction parameters
o Hypoxia, Oliguria, Creatinine, Coag, Platelet, Bilirubin, Ileus
• Tissue perfusion parameterso Mottling, capillary refill, lactate
• Haemodynamic variableso BP <90, MAP < 70, SBP > 40mmHg from
baseline

Sources of sepsis• Respiratory 38%• Urinary tract 21%• Intra-abdominal 16.5%• CRBSI 2.3%• Device 1.3%• CNS 0.8%• Others 11.3%

Give 3 Take 31.OXYGEN: Titrate O2 to saturations of 94 -98% or 88-92% in chronic lung disease.
1. CULTURES: Take blood cultures before giving antimicrobials (if no significant delay i.e. >45 minutes) and consider source control.
2. FLUIDS: Start IV fluid resuscitation if evidence of hypovolaemia. 500ml bolus of isotonic crystalloid over 15mins & give up to 30ml/kg, reassessing for signs of hypovolaemia, euvolaemia, or fluid overload.
2.BLOODS: Check point of care lactate & full blood count. Other tests and investigations as per history and examination.
3. ANTIMICROBIALS: Give IV antimicrobials according to local antimicrobial guidelines.
3. URINE OUTPUT: Assess urine output and consider urinary catheterisation for accurate measurement in patients with severe sepsis/septic shock.
Sepsis screening• Early recognition• 2% of all ED referrals are due to sepsis • NSW audit of NEWS: sepsis is the cause of
30% of triggered reviews• UK: NEWS > 5; 52% sepsis

ED vs In-patientED Ward
• Community acquired
• Less co-morbidities• Generalised
training• Mortality 20%
• Hospital acquired• Co-morbidities• Second – Hit• Specialist training• Mortality ???
Higher

Prompt treatment• Sepsis is a time-dependent medical
emergency
• Mortality increases by 7.6% for each hour delay to appropriate antibiotics (Kumar CCM 2006)

Early antibiotics are goodAuthor N Setting Median
time (mins)
Odds ratio for death
GaieskiCCM 2010; 38;1045-53
261 ED, USA(shock)
119 0.30(1st hour vs all times)
DanielsEmerg Med J 2010; doi:10.1136
567 Whole hospital, UK
121 0.62(1st hour vs all times)
KumarCCM 2006; 34(6): 1589-1596
2154 ED, Canada(shock)
360 0.59(1st 3 hours vs delayed)
AppelboamCCM 2010; 14(Suppl 1):50
375 Whole hospital, UK
240 0.74(1st 3 hours vs delayed)
LevyCCM 2010; 38(2): 1-8
15022 Multi-centre 0.86(1st 3 hours vs delayed)



Management of sepsis in adult in-patient


Start Smart• 9-fold increase in mortality with
inappropriate antibiotics• Independent risk factors
o COPDo Immunocompromisedo Chronic dialysis

Then Focus• Daily patient review
o Investigationso Culture results
• Five optionso Continue current antimicrobialo Change antimicrobialo Change iv to oralo Stop o OPAT

Trzeciak, S et al. Int Care Med 2007; 33(6):870-7. n-=1177
Risk stratification


Figure 3. Mean hospital mortality among patients with decreased lactate within 8 hours of index test, stratified by total fluid received in increments of 7.5 ml/kg based on medication administration record.
Annals ATS, 2013http://www.atsjournals.org/doi/abs/10.1513/AnnalsATS.201304-099OC
Fluid resuscitation and Mortality


Cultures – common mistake 2

Compliance with sepsis 6
• Reduces the relative risk of death by 46.6%
• 1 additional life saved for every 5 care episodes
• Mortality reduced from 44% to 20%o Daniels et al, Emergency medicine journal 2011

Compliance with Sepsis 6R Daniels UK Sepsis Trust 2011

Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-150
10
20
30
40
50
60
70
80
90
100
Inital Sepsis Bundle
Serum lactate within 3 Hrs Blood Culture before AntibioticsAntibiotic Compliance Fluids for hypotension or elevated lactate
Perc
ent
in C
ompl
ianc
e
Severe sepsis audit – SSC

Fluid resuscitation trialsAntibioticmins
Pre-randomisation(mls/kg)
EGDT Usual Care
ProtocolStandardCare
Mort28-day(60 day in ProCESS)UC/EGDT
Mort90 day
UC/EGDT
ProCESS
76 30 2.8+/- 1.9
2.3+/- 1.9
3.3+/- 1.7
18.9/21/18.2
33.7/31.9/30.8
ARISE 70 34 1.96+/-1.4
1.7+/-1.4
14.8/15.9
18.6/18.8
ProMise
70 2 litres 2.0 +/- 1.0
1.78+/- 1.0
24.5/24.8
29.2/29.5

Impress Sept 2014
MortalityUS 24%
Europe 28%
Bundle compliant 20%
Non-bundle compliant 30% p=0.026

HIPE: Diagnosis of Sepsis, Severe Sepsis
or Septic Shock in 2015
DiagnosisNumber of Inpatients
Number of Deaths
Crude Mortality
Rate
Sepsis 9239 1756 19.0%
Severe Sepsis 111 38 34.2%
Septic Shock 509 217 42.6%
Total 9859 2011 20.4%

HIPE: Inpatients with a Diagnosis of Sepsis, Severe Sepsis or Septic Shock in 2015
Diagnosis Admission to CritNumber of Inpatients
Number of Deaths
Crude Mortality Rate
Sepsis
Yes 2542 680 26.8%
No 6697 1076 16.1%
Total 9239 1756 19.0%
Severe Sepsis
Yes 73 29 39.7%
No 38 9 23.7%
Total 111 38 34.2%
Septic Shock
Yes 372 153 41.1%
No 137 64 46.7%
Total 509 217 42.6%
Total Sepsis, Severe Sepsis & Septic Shock
Yes 2987 862 28.9%
No 6872 1149 16.7%
Total 9859 2011 20.4%

0-14 Years
15-34 Years
35-44 Years
45-54 Years
55-64 Years
65-74 Years
75-84 Years
85+ Years
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
50.0%
Hospital Inpatient Enquiry: Crude Mortality for Inpatients with a Diagnosis of Sepsis & Admission to Critical Care, by Age Group,
2015
Mor
talit
y R
ate

OECD Health Care Quality IndicatorsNational Healthcare Quality Reporting
System March 2015
Number per annum
Mortality Change in Mortality 2004 - 2013
AMI 6125 6.4% 40%
H. Stroke 1456 26%
I. Stroke 4485 10% 13.6%
Sepsis 9859 20.4% ?
Reassess• Is your patient responding to treatment?• After an initial response have they deteriorated
again?• Are they having a prolonged static period?• Don’t forget recent travel, seasonal outbreaks,
risk factors for MDRs
Barriers to implementation
• Lack of awareness, Lack of agreement• Lack of self-efficacy
o Perception – Reality gap, o Educationo Audit

Audit• HIPE Metadatasheet
o Mortalityo ICU admissiono Median LOS
• Compliance (> 95% form in chart)o All ED patients admitted with sepsiso All NEWS > 4 with infection
Summary
• Recognise, Resuscitate, Refer• Sepsis 6 in the 1st hour• Risk stratify and document• Review

Thank youwww.hse.ie/sepsis
Recommended









![Microsoft PowerPoint - Sepsis SMI [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/554b9094b4c90574668b55a5/microsoft-powerpoint-sepsis-smi-compatibility-mode.jpg)







