Participative
Leadership: What is it,
and why does it
matter?
Adrian Norbash, Ashley Collette, Beth Gallant-Loggie &
Heath Robson
2017 BC Health Leaders Conference –
13 October 2017

Canadian Forces Health Services Group
AGENDAAddiction and Substance Use Disorder (SUD) in the Canadian Armed Forces
Introduction
Why social connection, support and meaning/purpose matter?
What does the current addiction and SUD situation look like in the CAF (why
are we different)?
What does the prevailing culture and our relationship with the Chain of
Command look like and why?
What does our current Base Addictions and Aftercare program look like today?
What are we doing to improve the care we deliver, and how does participative
leadership factor into our design – Aftercare Improvement Initiative
Open discussion and Q&A
Canadian Forces Health Services Group
Still today…the common understanding of
addiction is wrong…and it’s hurting us all
What gets us into trouble is not what we don't know. It's what we know for
sure that just ain't so - Mark Twain
The story of Rat Park, the Vietnam War, and what it should mean for us today
Addiction must be viewed as a community and public health illness, as
opposed to a disease of individuals alone. Only when we understand this issue
properly can we expect to address it properly.
Reference: Everything you think you know about addiction is wrong - Johann
Hari. TED Talk, July 2015
Canadian Forces Health Services Group
Substances of AbuseMyths, Facts, and Implications for the CAF

Canadian Forces Health Services Group
Drugs/Drug Classes
Opioids (Narcotics)
Alcohol Cocaine/Crack/Methamphetamine
Hallucinogenics/Dissociative Drugs
Gamma Hydroxybutyrate (GHB)
Nicotine
Marijuana/ Synthetic cannabinoids
Other Synthetics

Canadian Forces Health Services Group
Risk of Mental Health Disorders in CAF
Higher incidence of adverse childhood events
Higher incidence of psychological trauma (e.g.
deployments)
Military factors (frequent moves, acculturation,
separation from family)
In SUDs, the military culture may play a role
Canadian Forces Health Services Group
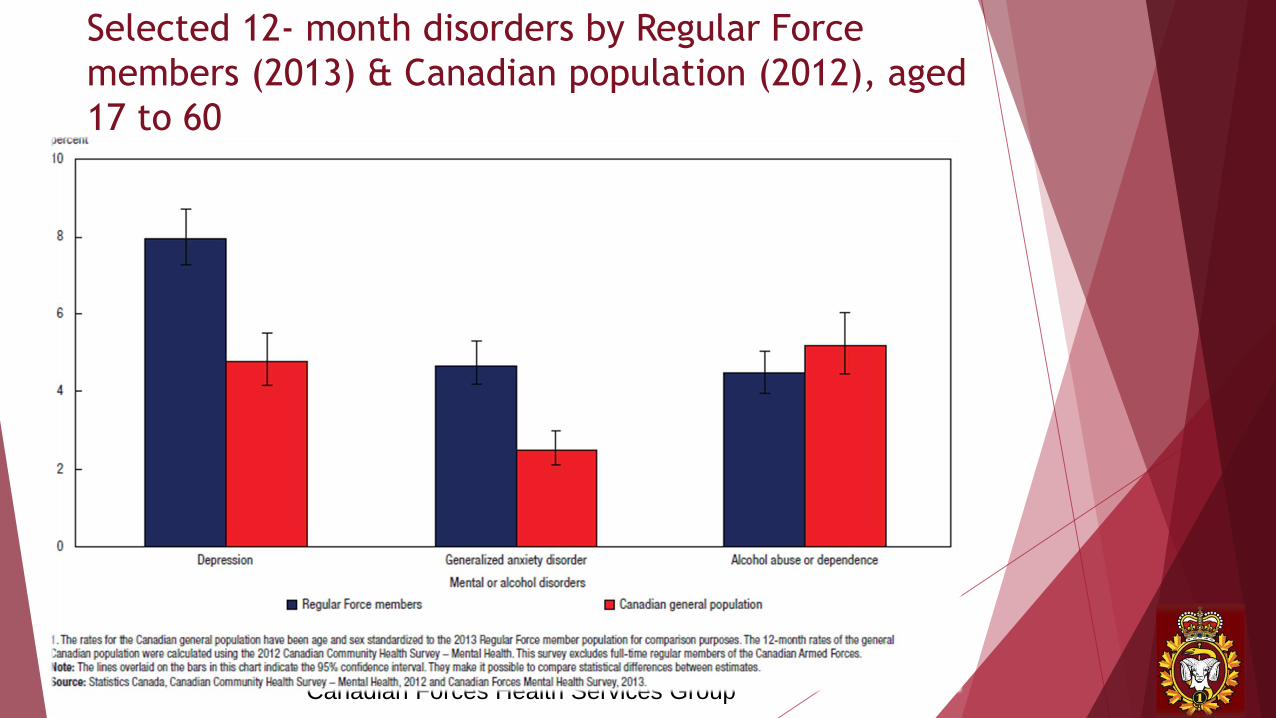
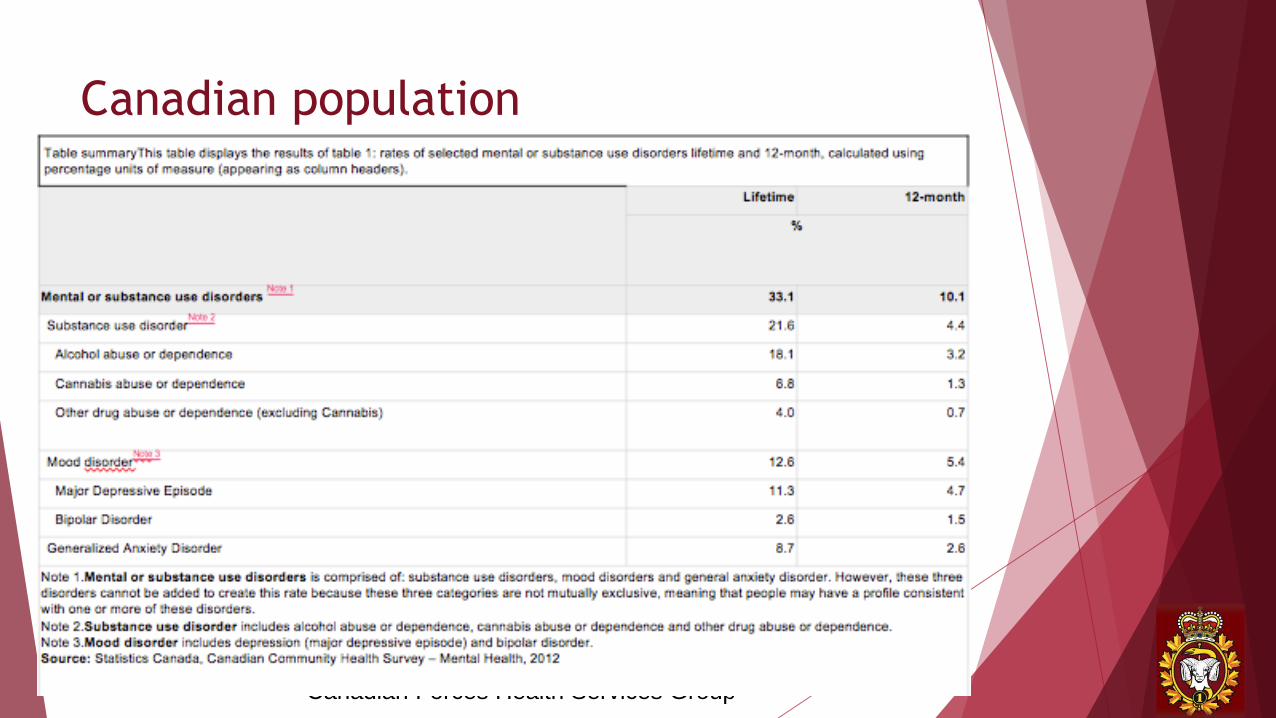
Selected 12- month disorders by Regular Force
members (2013) & Canadian population (2012), aged
17 to 60

Canadian Forces Health Services Group
Canadian Forces Health Services Group
Canadian population

Canadian Forces Health Services Group
CAF data (Stats Can 2013)
full-time regular force
members
%
Any selected mental or
alcohol disorder116.5
Major depressive episode 8.0
Post traumatic stress disorder 5.3
Generalized anxiety disorder 4.7
Panic disorder 3.4
Alcohol abuse or
dependence24.5

Canadian Forces Health Services Group
Treatment for alcohol – DAOD 5019-7
The Chain of command is responsible for ensuring that a CAF member who is believed to be displaying unacceptable alcohol-related conduct or performance is referred to a CAF medical care provider for assessment. A DAOD 5019-7A: Medical Referral and Certification
Only a CAF medical care provider or a CF addictions counsellor may assess, recommend treatment for, and treat alcohol abuse or alcohol dependence.
A CAF medical care provider shall fully describe and explain to the CO, by appropriate means, any medical employment limitations (MELs) assigned to the CAF member and any time required away from the workplace for medical reasons.
Canadian Forces Health Services Group
Considerations in Safety-Sensitive
occupations
Drug use likely and foreseeably impairs cognitive
function
Intoxication is consistently associated with an
increased vehicle crash risk
Most pronounced in high cognitive demand positions

Medical Employment Limitations (MELs)
No flying (pilot)
No operating commercial transport
No driving in line of duties, incl. emergency driving
No training in, or use of firearms (handguns and/or long guns)
No operational duties
No shift work
No night work
No task where incapacitation is a danger to self or others
No situation where the employee may be involved in confrontation
No duties where employee is expected to respond to emergencies
In summary: No decision-critical duties & No safety sensitive
duties
Canadian Forces Health Services Group
Criteria for retention…for now
The involvement constitutes a first time established involvement with drugs
Limited to personal use or possession for personal use
Did not take place on duty and did not create an immediate danger to operational readiness, security or safety
Unlikely repeat unauthorized use
Conduct and performance otherwise satisfactory and capacity for leadership has not been compromised
Canadian Forces Health Services Group
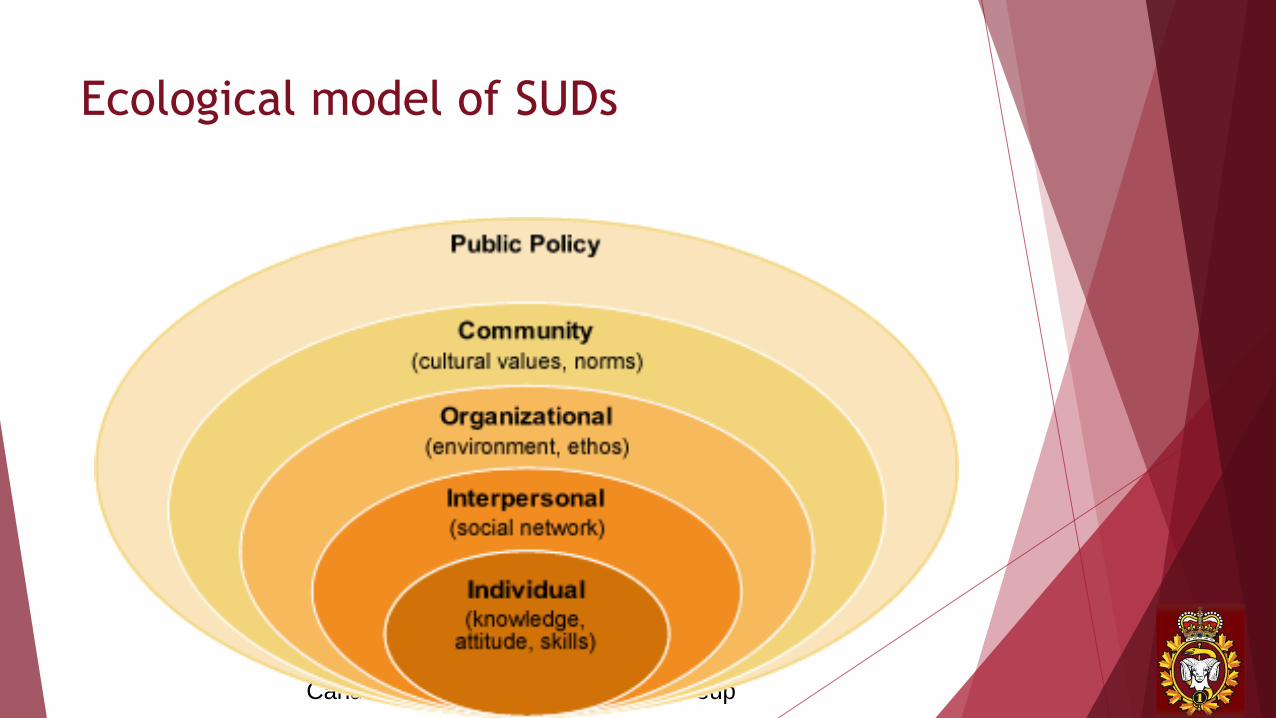
Ecological model of SUDs
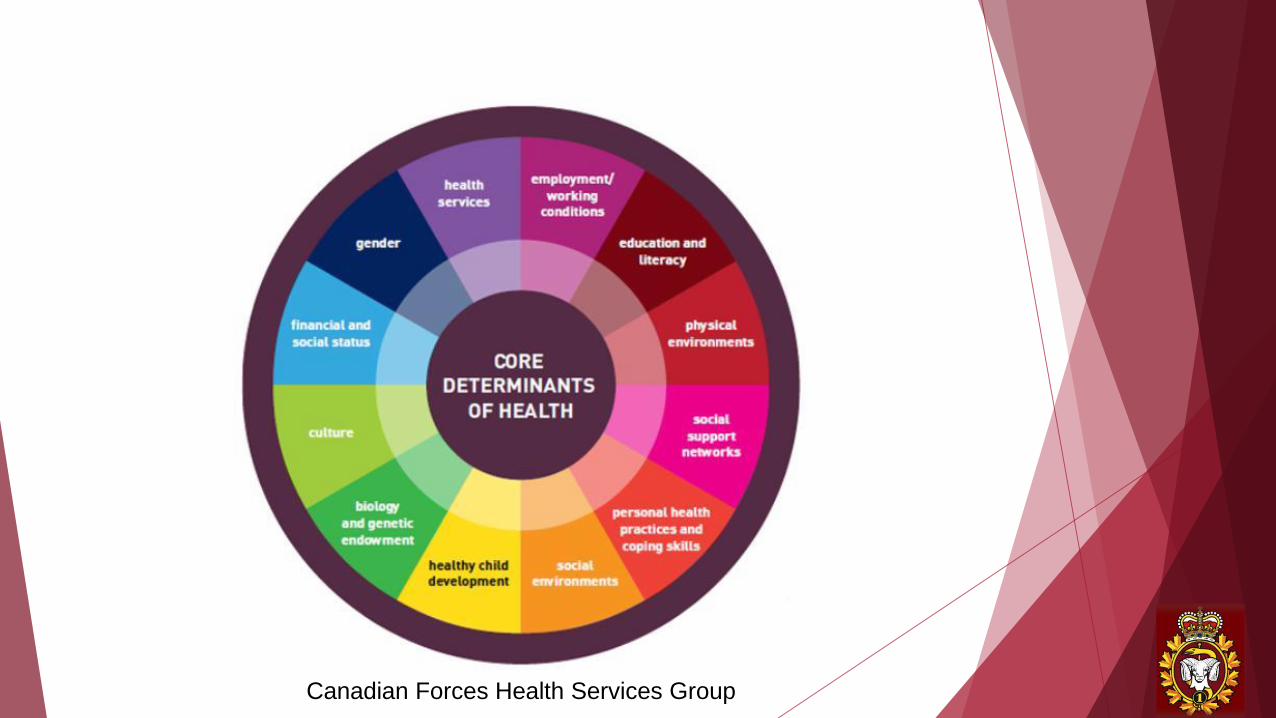
Canadian Forces Health Services Group
Canadian Forces Health Services Group
Ecological factors
CAF culture related to addiction
Stigma of mental health treatment – where we were and
where we are now
Influence of chain of command in recovery
Closing the circle of care - where we are going
Canadian Forces Health Services Group
Aftercare group
Mandated program for members who complete a
residential treatment program
Attendance: 6 months – 1 year
2 hour sessions, 2x/week
Considered a medical appointment
Not 12 step, but aligned with principles
Uses CBT, MI, strengths based and psycho-education
approach

Canadian Forces Health Services Group
Changes to Aftercare
Increased attendance – up to 20 members
Counsellors facilitate, members participate
Emphasis on peer support approach
Canadian Forces Health Services Group
So what are we doing?
Focus of our Aftercare Improvement Initiative
Engage, Educate, Enable (Patient, CoC, Family, Ourselves)
Change the culture through respectful two way dialogue
(ambitious, we know…but so necessary)
Strengthen social support & connection (Circle of Care) and
grow/influence recovery capital for our patients
Define and commit to purpose for each participant -
together
Study outcomes and share knowledge to improve
Aftercare programs CAF-wide
Canadian Forces Health Services Group
How is the project designed, and why?
Purposeful lack of control in the process and the precision of hypotheses
Redesigning and reimagining the care team. Who cares, cares.
Series of group facilitation exercises, focus groups, individual goal-setting, two-way sharing (two-eyed seeing)
Three proxy measures of success
Does level of participation increase, and incidence of withdrawal decrease (discussed adverse events/relapse, but decided to leave out of definition of success due to empowerment model)?
Do the CoC and unit support staff have the knowledge and tools to be proactive and positive actors in their member’s recovery?
Have the participants defined success from their perspective, and are they making meaningful steps in that direction?

Canadian Forces Health Services Group
How is the project designed, and why?
Designed around three central themes
Engage, Educate and Enable all stakeholders, including
ourselves
Empower the patients and those in their Circle of Care
employing two way sharing
Create a climate where those suffering from addiction
are encouraged and supported in accessing care, and
once there, makes keeping them enrolled in (and
attending) Aftercare a priority - for the patient, the
CoC, and the family alike.
Canadian Forces Health Services Group
How are we fostering participative
leadership?
Clarity of expectations and effort (Mission, Vision, Values)
Finding a spark – why should anybody care?
Drawing on the principles of Relationship Based Care and Team
Based Leadership (next slides)
Diluting power, diluting control (Mission Command)
Slow and simple wins the race
Timing is everything…and our Stars are presently aligned
Sharing responsibility and accountability for success
Being curious…and comfortable with discomfort

Canadian Forces Health Services Group
Relationship Based Care
What is Relationship Based Care in our context?
Clear focus on the strengthening of relationships
Role modelling the behaviour we want to see in our patients, our
colleagues (also our patient’s CoC), and our communities at large
Transforming our practice by returning us to what we see as our
basic purpose: caring for and connecting with other human beings

Canadian Forces Health Services Group
Relationship-based Care: A Model for Transforming Practice - Mary
Koloroutis, 2004

Canadian Forces Health Services Group
What does Helen think?
https://scienceforwork.com/blog/psychological-safety/

Canadian Forces Health Services Group
Team based leadership principles
What are our conditions for success?
A clear, achievable and laudable vision to link with team
objectives
A focus from management on building, helping and
supporting teams to do what they can do themselves
An effort to align team member’s needs with the
organization’s mission and vision
A staunch commitment to empowering and engaging team
members through trust and support (psychological safety)
Clarity of roles and expectations with clear and respectful
communication…always (R+A+A)
Canadian Forces Health Services Group

Canadian Forces Health Services Group
The Unhealthy Workplace
Problem
Person
Union
Supervisor
Co-worker
Doctor Family
Friends
Covering Up
Excuses
Ignore
Ineffectiveness
Denial
Justify
Avoidance Mistrust
Unfairness
Low Morale
Sabotaging
Health Problems
Stress
Mistakes
High Absenteeism
Low Trust
PoorAttitudes
Accidents
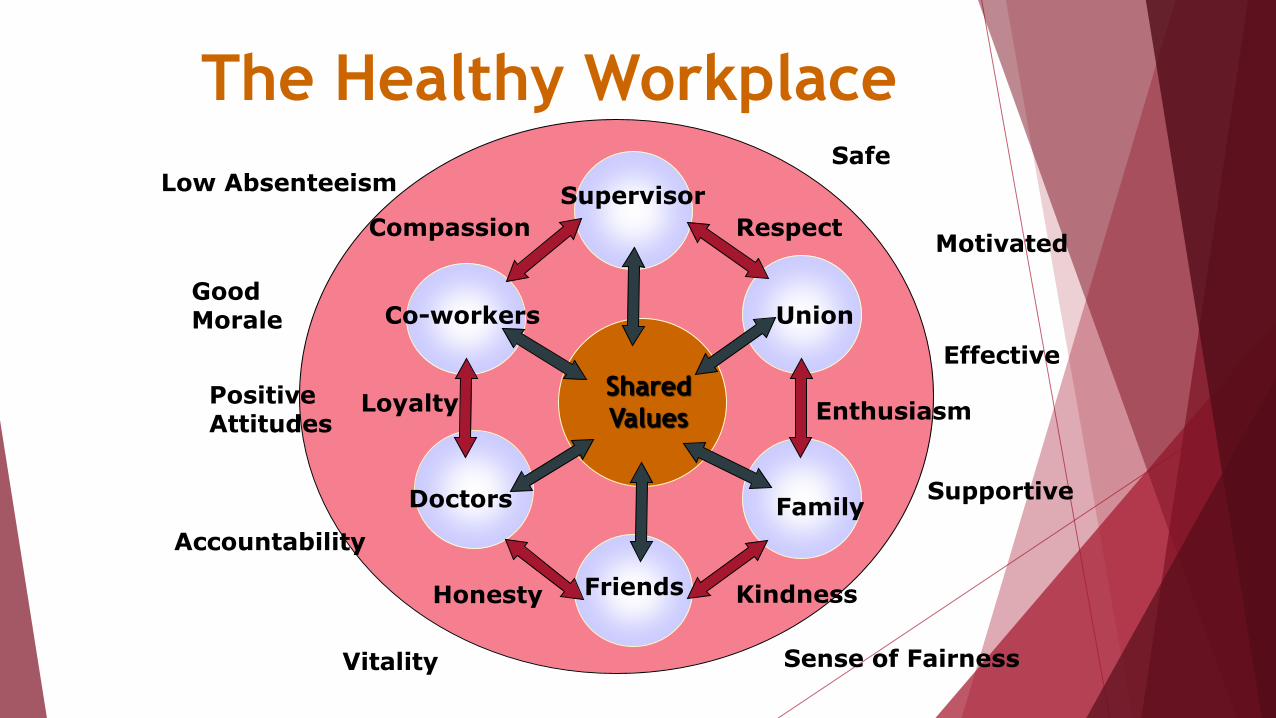
The Healthy Workplace
Supervisor
Union
Family
Friends
Doctors
Co-workers
Shared
Values
Respect
Enthusiasm
Kindness
Compassion
Loyalty
Honesty
Safe
Motivated
Effective
Supportive
Sense of FairnessVitality
Accountability
Low Absenteeism
Good Morale
PositiveAttitudes

Canadian Forces Health Services Group
Care Quality Commission– State of Care
http://www.cqc.org.uk/publications/major-report/state-care

Canadian Forces Health Services Group

Canadian Forces Health Services Group
Work done to date
Logic Model and Value Stream Mapping with all parties
Mental Health Forum focused on addiction & recovery
Baseline data collected for last 24 months
Level of participation and withdrawal rate
Baseline survey for patients
Baseline survey for the CoC and Unit support staff prior to
the MH Forum to measure impact

Canadian Forces Health Services Group
Mental Health Forum – 28 September 2017
Canadian Forces Health Services Group
Canadian Forces Health Services Group
What’s next?
Project will end October, 2018
Present findings to colleagues at CIMVHR 2018 in Regina,
SK
Share design and lessons learned with national Addictions
cell
Create an agreed upon design framework in conjunction
with the CoC/Army for successful Aftercare programs and
implement CAF-wide.
Canadian Forces Health Services Group
So then, what is participative leadership
exactly?
Never underestimate the power of ideas – Robert Evans. An
Undisciplined Economist. 2016.
The Journey of a thousand miles….

Canadian Forces Health Services Group
References
Everything you think you know about addiction is wrong - Johann Hari. TED Talk, July 2015
Creative Healthcare Management. 2003. Leading an Empowered Organization: Participant Manual. Minneapolis, Minnesota.
Relationship-based Care: A Model for Transforming Practice - Mary Koloroutis, 2004
Guarding Minds @ Work. 2012 Centre for Applied Research in Mental Health and Addiction (CARMHA)
On the way home: Family centered academic aftercare services. University of Nebraska – Lincoln Center for Child and family well-being
State of Care 2016/2017. Care Quality Commission. UK
Five questions about psychological safety answered. Science for work, October 2017

Canadian Forces Health Services Group
Open Discussion and Q&A
Recommended