1
Pancreas Cysts: An Incidental Pancreas Cysts: An Incidental Finding or Harbinger of MalignancyFinding or Harbinger of Malignancy
William R. William R. BruggeBrugge, MD, FACG, MD, FACG
Professor of MedicineProfessor of Medicine
Harvard Medical SchoolHarvard Medical School
Director, GI Director, GI EndoscopyEndoscopy UnitUnit
Massachusetts General HospitalMassachusetts General Hospital
Cysts: Early Cysts: Early NeoplasiaNeoplasia
MalignantSerous
Cyst with associated mass
Macrocystic
Microcystic
Morphology
Mucinous
Pseudocyst / InflammatoryCavity
Mucinous Cystic LesionsMucinous Cystic Lesions
Cystic lesions of the pancreas. A diagnostic and management dilemma.Pancreatology. 2008;8(3):236-51. Garcea G, Pollard CA, Berry DP, Dennison AR.
EUSEUS--guided guided FNAFNA
Linear e-scope
Color Doppler
Aspiration needle
Transgastric or transduodenal aspiration
Cytologyendoscopy
EUScytology
Mucinous Cystic Mucinous Cystic NeoplasmNeoplasm
Macrocystic lesionsMacrocystic lesions Viscous (1.8), mucoid fluidViscous (1.8), mucoid fluid Fluid analysis: CEA>200, low Fluid analysis: CEA>200, low
amylase, DNA >40ng/mlamylase, DNA >40ng/ml MucinMucin--secreting epithelial secreting epithelial
cellscells Malignant potentialMalignant potential
cytology
Histology
Cyst fluid
CEA
Types of IPMNTypes of IPMN
Side branch
Main Duct
Gross

2
Tissue Types of IPMNTissue Types of IPMN
Gastric Villous-intestinal Pancreatic-Biliary MalignantSurgery. 2010 Jan 7. Invasie carcinoma derived from the nonintestinal type intraductal papillary mucinous neoplasm of the pancreas has a poorer prognosis than that derived from the intestinal type.Sadakari Y, Ohuchida K, Nakata K, Ohtsuka T, Aishima S, Takahata S, Nakamura M, Mizumoto K, Tanaka M.
Low grade dysplasia
(adenoma)
Low grade dysplasia
(adenoma)
Moderate dysplasia
(Borderline)
Moderate dysplasia
(Borderline)
CarcinomaCarcinoma
Grading of IPMNGrading of IPMN
Chromoendoscopy of IPMNChromoendoscopy of IPMN
Brian C. Brauer MD, Norio Fukami MD and Yang K. Chen MDDirect cholangioscopy with narrow-band imaging, chromoendoscopy, and argon plasma coagulation of intraductal papillary mucinousneoplasm of the bile duct (with videos) Gastrointest Endosc. 2008 Mar;67(3):574-6.
Narrow Band Imaging
Chromoendoscopy
Types of IPMN by CT scanningTypes of IPMN by CT scanning
World J Gastroenterol. 2009 Aug 28;15(32):4037-43.Imaging features of intraductal papillary mucinous neoplasms of the pancreas in multi-detector row computed tomography.Tan L, Zhao YE, Wang DB, Wang QB, Hu J, Chen KM, Deng XX.
Benign Side-Branch Malignant main duct
MRCP of IPMNMRCP of IPMN
Waters JA, Schmidt CM, Pinchot JW, Akisik F, Howard TJ, Nakeeb A, Zyromski NJ, Lillemoe KD.CT vs MRCP: optimal classification of IPMN type and extent.J Gastrointest Surg. 2008 Jan;12(1):101-9.
Benign side branch Malignant main duct
EUS of IPMN Adenoma: type IIEUS of IPMN Adenoma: type II
Ann Surg. 2009 Apr;249(4):628-34.Intraductal papillary mucinous neoplasms of the pancreas: differentiation of malignant and benign tumors by endoscopic ultrasound findings of mural nodules. Ohno E, Hirooka Y, Itoh A, Ishigami M, Katano Y, Ohmiya N, Niwa Y, Goto H.

3
EUS: NonEUS: Non--invasive malignancy: invasive malignancy: type IIItype III
EUS: Malignant Nodule: type IVEUS: Malignant Nodule: type IV
EUS of IPMN: nodulesEUS of IPMN: nodules
Ann Surg. 2009 Apr;249(4):628-34.Intraductal papillary mucinous neoplasms of the pancreas: differentiation of malignant and benign tumors by endoscopic ultrasound findings of mural nodules.Ohno E, Hirooka Y, Itoh A, Ishigami M, Katano Y, Ohmiya N, Niwa Y, Goto H.
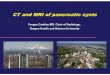
Presence of Nodules in Resected Specimens as a Function of Histologic Subtype of Br-IPMN
0
8.5
43.8
75
0
10
20
30
40
50
60
70
80
90
100
Adenoma (0/66) Boderline (4/47) Carcinoma in situ (7/16) Invasive Carcinoma(12/16)
Histologic Subtype
% S
pec
imen
s w
ith
No
du
les
BD-IPMN: histology vs. nodules
Gastroenterology. 2007 Jul;133(1):72-9; Branch-duct intraductal papillary mucinous neoplasms: observations in 145 patients who underwent resection.Rodriguez JR, Salvia R, Crippa S, Warshaw AL, Bassi C, Falconi M, Thayer SP, Lauwers GY, Pederzoli P, Fernández-Del Castillo C.
Using Nodules and Size to Predict Malignancy
Ann Surg Oncol. 2008 Jan;15(1):199-205. Treatment guidelines for branch duct type intraductal papillary mucinous neoplasms of the pancreas: when can we operate or observe?Jang JY, Kim SW, Lee SE, Yang SH, Lee KU, Lee YJ, Kim SC, Cho BH, Yu HC, Yoon DS, Lee WJ, Lee HE, Kang GH, Lee JM.
Survival: IPMNSurvival: IPMN
Thomas Schnelldorfer, MD; Michael G. Sarr, MD;;; Michael B. Farnell, MD Experience With 208 Resections for Intraductal Papillary Mucinous Neoplasm of the PancreasArch Surg. 2008 Jul;143(7):639-46;

4
MR or thin slice CT yearly No
MR or CT
1-2 cm every 6-12 mo
2-3 cm every 3-6 moStable lesion without nodules
Symptomatic, size >3 cm or
Positive high-risk stigmata
YesEUS: Mural nodulesDilated Main DuctMalignant cytology
Resect
Size <1cm Size 1-3cm Size >3cm
Monitoring of Side Branch IPMN LesionsMonitoring of Side Branch IPMN Lesions
International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas.Pancreatology. 2006;6(1-2):17-32.
Markov modeling: Management of Markov modeling: Management of pancreatic cystic lesionspancreatic cystic lesions
Gastroenterology. 2010 Feb;138(2):531-40. Asymptomatic pancreatic cystic neoplasms: maximizing survival and quality of life using Markov-based clinical nomograms.Weinberg BM, Spiegel BM, Tomlinson JS, Farrell JJ.
At 65 years old At 65 years old ……2cm cyst2cm cyst
Survival QoL
But if at 65 years old But if at 65 years old …… 3cm cyst3cm cyst
Survival QoL
Findings of the Markov ModelFindings of the Markov Model
For patients focused on overall survival, regardless of quality of life, surgery is optimal for lesions >2cm.
For patients focused on quality-adjusted survival, a 3cm threshold is more appropriate for surgery except for the extreme elderly.
Gastroenterology. 2010 Feb;138(2):531-40. Asymptomatic pancreatic cystic neoplasms: maximizing survival and quality of life using Markov-based clinical nomograms.Weinberg BM, Spiegel BM, Tomlinson JS, Farrell JJ.
Indications for Surgical Indications for Surgical ResectionResection
Recurrent pancreatitis
Main duct disease
Cystic lesion >3cm
Rising CA 19-9
Malignant cytology
J Clin Gastroenterol. 2010 May 5. Predictors of Malignant Intraductal Papillary Mucinous Neoplasm of the Pancreas.Mimura T, Masuda A, Matsumoto I, Shiomi H, Yoshida S, Sugimoto, Kutsumi H, Ku Y, Azuma T.

5
Ethanol AblationEthanol AblationEPIC TrialEPIC Trial
Prospective, randomized trial of ethanol vs saline lavage
1-3cm cystic lesion
4 patients underwent resection (histology) 42 pts
25 pts lavagedwith ethanol
12/25 resolved
17 pts lavaged with saline
0/17 resolved
ethanolsaline
EUS-guided ethanol versus saline solution lavage for pancreatic cysts: a randomized, double-blind study.DeWitt J, McGreevy K, Schmidt CM, Brugge WR.Gastrointest Endosc. 2009 Oct;70(4):710-23. Epub 2009 Jul 4.
ConclusionsConclusions
IPMN is a common malignancy Main
Side Branch
Slowly progressive
Resect: main duct disease, high risk lesions, size>3cm with nodule
Recommended