1
“The Institute of Optometry is unique in being an independent self-financing charity dedicated to
the promotion of clinical excellence, research, and education in optometry.”
Roberson (1989)
TT HH EE II NN SS TT II TT UU TT EE OO FF OO PP TT OO MM EE TT RR YY
OPTOMETRY FOR CHILDREN:
SAFE PRACTICE
Prof Bruce EvansBSc (Hons) PhD FCOptom FAAO FEAOO FBCLA DipCLP DipOrth
Director of Research Institute of Optometry
Visiting Professor City University
Visiting Professor London South Bank University
Private practice Brentwood, Essex
References
Pickwell’s Binocular Vision Anomalies, 5th Edition, Elsevier, 2007
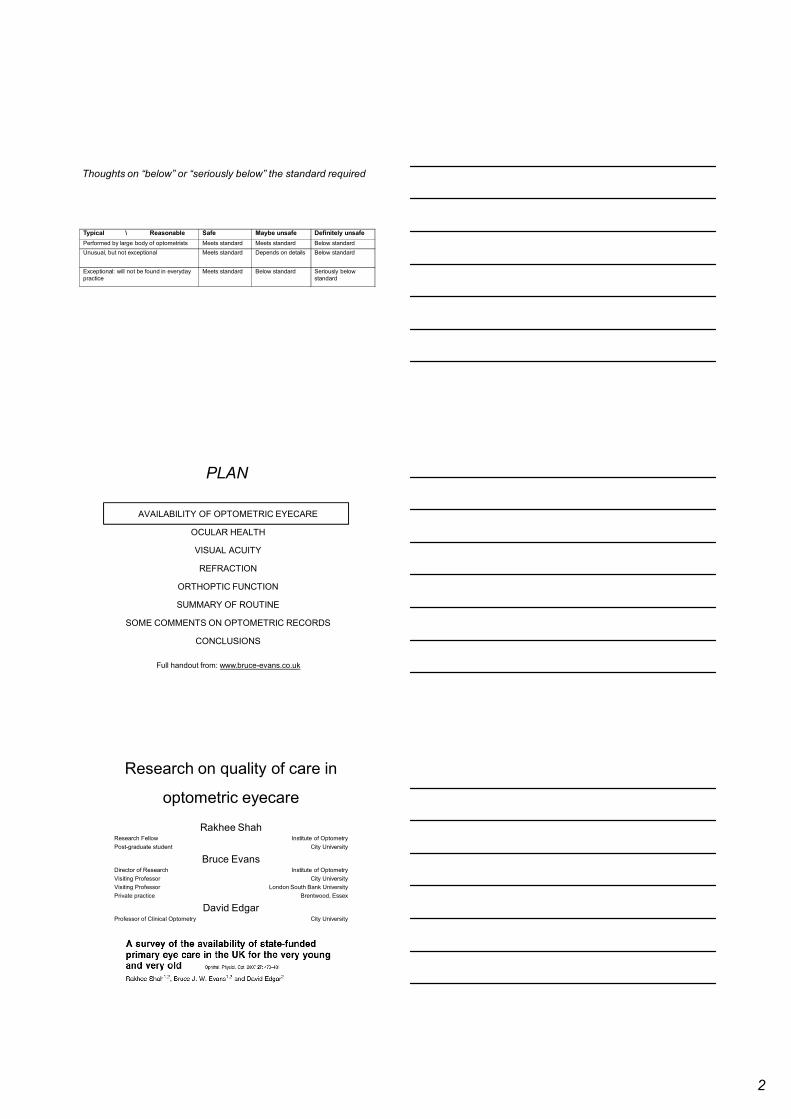
Best practice or safe practice?
Average can be defined as a point
or as a rangeIf a point, then 50% of
practitioners are below average
Easiest to consider ranges
C.Optom guidelines described as
“good practice”
Presentation today describes
average (typical) range & unsafeaverage
expert
best practice
average
range
unsafe
just reasonably
competent
good
below average
but OK
unusual, may
be unsafe
best
C.Optom
guidelines
2
Thoughts on “below” or “seriously below” the standard required
Typical \ Reasonable Safe Maybe unsafe Definitely unsafe
Performed by large body of optometrists Meets standard Meets standard Below standard
Unusual, but not exceptional Meets standard Depends on details Below standard
Exceptional: will not be found in everyday
practice
Meets standard Below standard Seriously below
standard
PLAN
AVAILABILITY OF OPTOMETRIC EYECARE
OCULAR HEALTH
VISUAL ACUITY
REFRACTION
ORTHOPTIC FUNCTION
SUMMARY OF ROUTINE
SOME COMMENTS ON OPTOMETRIC RECORDS
CONCLUSIONS
Full handout from: www.bruce-evans.co.uk
Research on quality of care in
optometric eyecare
Rakhee ShahResearch Fellow Institute of Optometry
Post-graduate student City University
Bruce EvansDirector of Research Institute of Optometry
Visiting Professor City University
Visiting Professor London South Bank University
Private practice Brentwood, Essex
David EdgarProfessor of Clinical Optometry City University
3
Plan
Study 1
A telephone survey to assess the availability of
state-funded eye care in the UK
Study 2
The use of standardised patients to assess the
content of optometric eye examinations in the
UK
Study 3
The use of computerised clinical vignettes to
assess the content of optometric eye
examinations in the UK
Child scenario: questions
1. At what age do you start testing kids? My son is one year old.
2. We have a family history of "lazy eye"/"squint". Should he have an
eye test?
If answer to question 2 is YES, then proceed to 3; if no to 4,5,6.
3. Can it be done at your “opticians”?
If answer to question 3 is NO, then proceed to 4, 5, and 6.
4. At what age should he have an eye test?
5. What should I do if I see his eye turning?
6. Is there anybody you can recommend I may able to contact/visit?
If answer to question 3 is YES, then proceed to question 7.
7. Will I be paying for the consultation? How much?
Child scenario: results
At what age do you start testing kids?
Mean 3.1 years (Shah, Evans, Edgar; 2007)
[c.f., C.Optom survey (2008): 76% of optoms test younger than 3y]
We have a family history of turn. Should he have an eye
test & can it be done there?
Proportion Examine
there
Exam.
elsewhere
No exam.
Total
sample
46% 30% 24%
Non-
London
48% 31% 21%
London 36% 21% 43%
4
General discussion: ethics
NHS GOS regulations:
DoH argue that optoms cannot exclude a category of px
GOC standards of practice:
“Recognise and work within the limits of your scope of
practice, taking into account your knowledge, skills, and
experience”
Joint document on children’s eyecare by
C.Optom, R.C.Ophthalmol., BIOS:
Appropriate skills & expertise before managing any child
Those who do not spend a significant proportion of their
time in management of children discouraged from
participation in children’s eyecare
General discussion: ethics
Only 7% of children aged 0-5y visit optoms
Guggenheim & Farbrother (2005)
Many optoms may lack experience
Situation even more serious for people with
intellectual disabilities
PLAN
AVAILABILITY OF OPTOMETRIC EYECARE
OCULAR HEALTH
VISUAL ACUITY
REFRACTION
ORTHOPTIC FUNCTION
SUMMARY OF ROUTINE
SOME COMMENTS ON OPTOMETRIC RECORDS
CONCLUSIONS
Full handout from: www.bruce-evans.co.uk
5
Ocular health
Ocular pathology very rare in
children
With pre-school, optometrist
unlikely to get more than a
glimpse
Pupil reactions possibly, usually
not recorded
May see more with dilation
Limited view of retina not justification by
itself for dilation
Visual fields rarely tested in
children
Intraocular pressure almost never
tested in children
PLAN
AVAILABILITY OF OPTOMETRIC EYECARE
OCULAR HEALTH
VISUAL ACUITY
REFRACTION
ORTHOPTIC FUNCTION
SUMMARY OF ROUTINE
SOME COMMENTS ON OPTOMETRIC RECORDS
CONCLUSIONS
Full handout from: www.bruce-evans.co.uk
Visual acuity: overview
Macula is poorly developed at birth
Large variation in rate of development
Results vary with different test methods
6
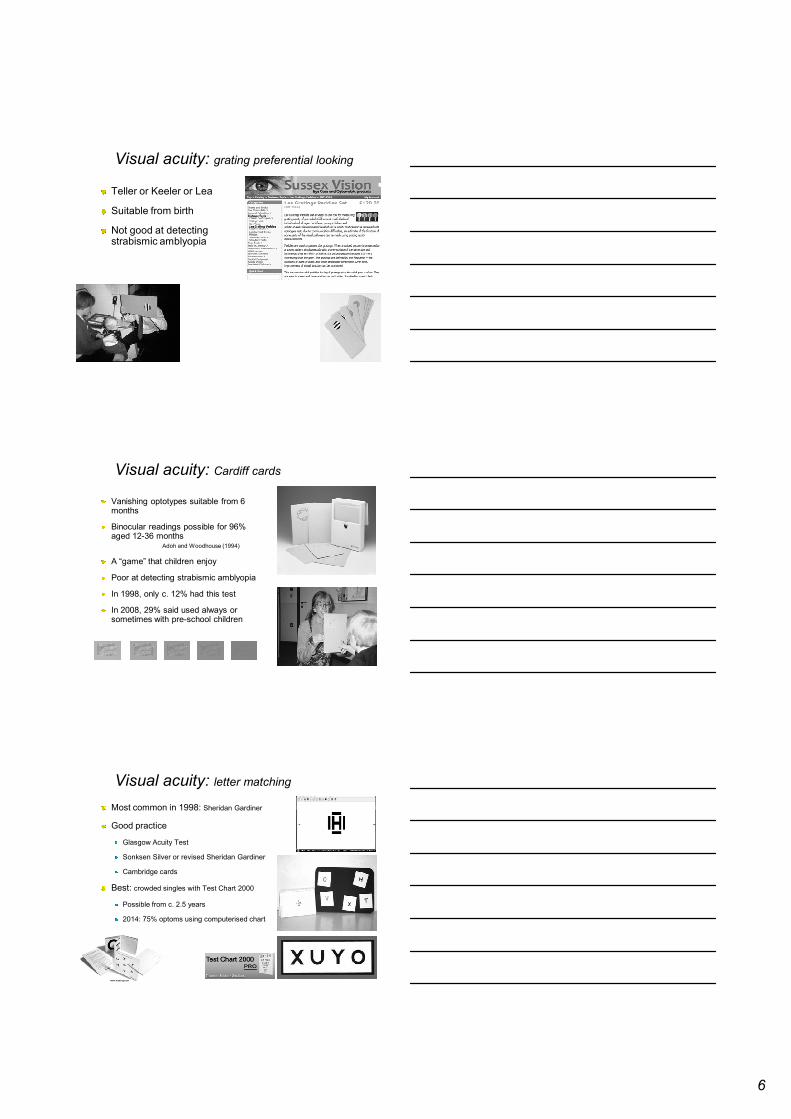
Visual acuity: grating preferential looking
Teller or Keeler or Lea
Suitable from birth
Not good at detecting strabismic amblyopia
Visual acuity: Cardiff cards
Vanishing optotypes suitable from 6 months
Binocular readings possible for 96% aged 12-36 months
Adoh and Woodhouse (1994)
A “game” that children enjoy
Poor at detecting strabismic amblyopia
In 1998, only c. 12% had this test
In 2008, 29% said used always or sometimes with pre-school children
Visual acuity: letter matching
Most common in 1998: Sheridan Gardiner
Good practice
Glasgow Acuity Test
Sonksen Silver or revised Sheridan Gardiner
Cambridge cards
Best: crowded singles with Test Chart 2000
Possible from c. 2.5 years
2014: 75% optoms using computerised chart
7
Visual acuity: near charts
Thomas the tank engine
Institute of Optometry near test chart
Many others
?child-friendly charts rarely used
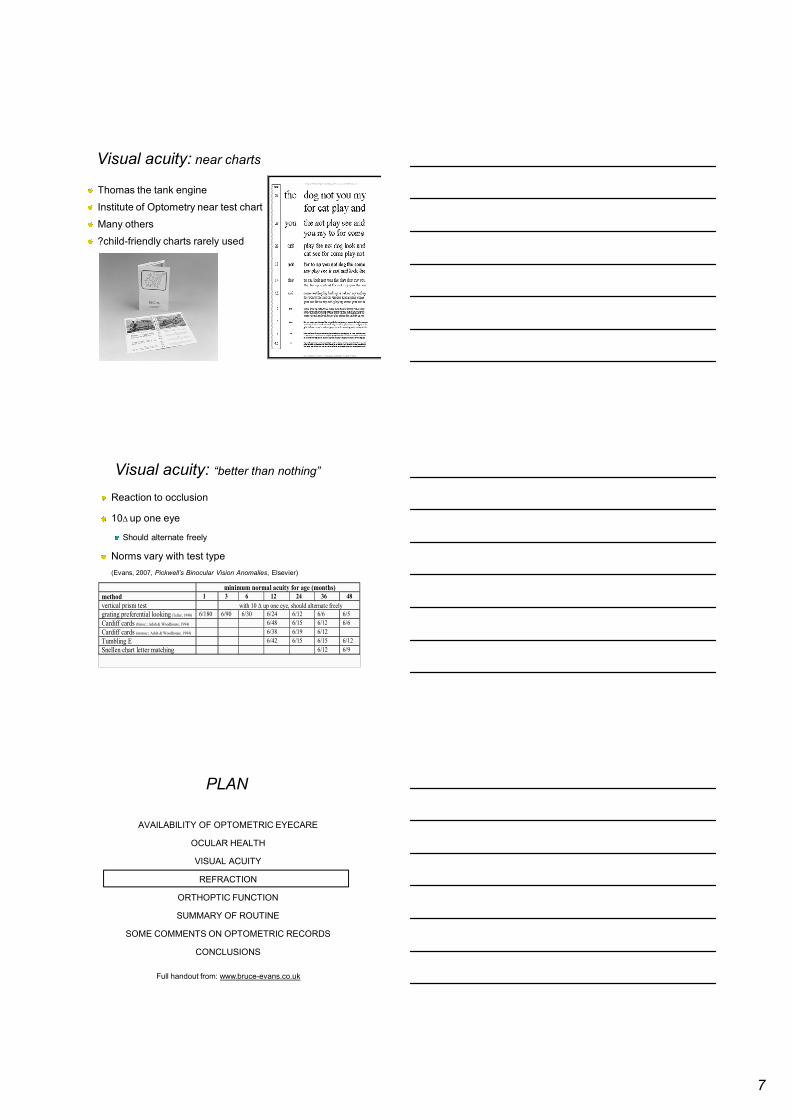
Visual acuity: “better than nothing”
Reaction to occlusion
10∆ up one eye
Should alternate freely
Norms vary with test type
(Evans, 2007, Pickwell’s Binocular Vision Anomalies, Elsevier)
minimum normal acuity for age (months)
method 1 3 6 12 24 36 48
vertical prism test with 10 ∆ up one eye, should alternate freely
grating preferential looking (Teller, 1990) 6/180 6/90 6/30 6/24 6/12 6/6 6/5
Cardiff cards (binoc.; Adoh & Woodhouse, 1994) 6/48 6/15 6/12 6/6
Cardiff cards (monoc.; Adoh & Woodhouse, 1994) 6/38 6/19 6/12
Tumbling E 6/42 6/15 6/15 6/12
Snellen chart letter matching 6/12 6/9
PLAN
AVAILABILITY OF OPTOMETRIC EYECARE
OCULAR HEALTH
VISUAL ACUITY
REFRACTION
ORTHOPTIC FUNCTION
SUMMARY OF ROUTINE
SOME COMMENTS ON OPTOMETRIC RECORDS
CONCLUSIONS
Full handout from: www.bruce-evans.co.uk
8
Refraction: Basic minimum
Are the retinoscopy reflexes
symmetrical and no large refractive
errors?
Be adaptable about working distance
Hold trial lenses with infants
Fixation target is anything that will
attract their attention, ideally Test
Chart 2000
Refraction: cycloplegic
Textbook indications for cycloplegic:
Symptom of intermittent esotropia (SOT)
Sign of esophoria or esotropia
Unexplained poor visual acuity
Unexplained symptoms
Variable or suspicious Rx
When should a reasonably competent optometrist carry out a cycloplegic?
In pre-school child when esotropia or significant hypermetropia
Refer if under 3 months and needs cycloplegia
Most optometrists would probably refer if under 1 year
Refractive error: normal development
At birth +2.00 DS (SD = 2.00 DS)
very variable in first year
On average, hypermetropia decreases rapidly during the first year to a mean level of about +1.50 D at age one year
High astigmatism in first year often reduces
9
Refraction: norms
Nearly 75% of children with esotropia &/or amblyopia have a significant Rx
myopia, hypermetropia (2.00), anisometropia (1.00), astigmatism (1.50)
North American guidelines (Leat, 2011), in UK suggestions from Evans (2007, Pickwell’s Binocular Vision Anomalies, 5th edition)
age
(months)
refractive errors probably require correction if stable and:
N.B.., better prognosis if Rx is reducing and non-cyclo ret<< cyclo ret. If Rx more than half the values below then monitor
1-6 (refer) > +6.00 DS > -5.00 DS > 6.00 DC hypermetropic anisometropia > 2.50 DS/DC
6-9 > +4.00 DS > -5.00 DS > 4.50 DC hypermetropic anisometropia > 2.00 DS/DC
9-18 > +3.50 DS > -4.00 DS > 2.50 DC hypermetropic anisometropia > 1.25 DS/DC
18-36 > +2.50 DS > -2.00 DS > 1.50 DC hypermetropic anisometropia > 1.00 DS/DC
36-48 > +2.25 DS > -1.00 DS > 1.25 DC hypermetropic anisometropia > 1.00 DS/DC
PLAN
AVAILABILITY OF OPTOMETRIC EYECARE
OCULAR HEALTH
VISUAL ACUITY
REFRACTION
ORTHOPTIC FUNCTION
SUMMARY OF ROUTINE
SOME COMMENTS ON OPTOMETRIC RECORDS
CONCLUSIONS
Full handout from: www.bruce-evans.co.uk
Orthoptics: tests of alignment
Cover test: the gold standard
Should be at least attempted & recorded
Others:
Hirschberg: inaccurate 1mm = 15-20∆
Krimsky: ±14∆
Bruckner
Symmetry of red reflexes, direct ophthalmoscope at 80-100cm, dial in
correction for clear view. Darker reflex in strabismic eye
Detects strabismus, anisometropia, anisocoria or pathology
10
Orthoptics: motility
Infants don’t like having head held
Practitioner should move around
Or parent can rotate the child
Should be at least attempted in every child
Often carried out but only recorded if abnormal
Orthoptics: motor fusion
Base out prism test
Have child fixate a detailed picture
Can measure in older children with prism
bar
Motor fusion assessment in young children
is good practice/best practice
age (months) test response
0-3 20 ∆ out unlikely to make any response
by 6 20 ∆ out should be overcome
Evans (2007) Pickwell’s Binocular Vision Anomalies, 5th edition
Orthoptics: sensory fusion & stereo
Good practice is to test stereo-acuity in pre-school children
It is questionable whether a failure to do so falls below the standard
of a reasonably competent optometrist
More likely to do so if child has other risk factors for strabismus
70% of optoms say they always test in pre-school children
(C.Optom, 2008)
The test used is
matter of personal
preference
11
Orthoptics: stereotest norms
Generally, different tests give different results
So, test should be named or obvious (e.g., only test)
age test response
0-3 mo. any unlikely to make any response
6-18 mo. Lang 1 observe patient’s eyes: may see fixations indicating sees pictures
18-24 mo. Lang 1 or 2 should fixate and may point at pictures
> 24 mo. Lang 1 or 2 should be able to point and name pictures
≥ 24 mo. Randot (shapes) if sees shapes on random dot background indicates no strabismus
≥ 24 mo. Randot (animals) should be able to see all animals
3-5 yrs. Randot (circles) 70"
> 5 yrs. Randot (circles) 40" or better
3.5 yrs. Titmus 3000” (Romano et al., 1975)
5 yrs. Titmus 140” (Romano et al., 1975)
6 yrs. Titmus 80” (Romano et al., 1975)
7 yrs. Titmus 60” (Romano et al., 1975)
9 yrs. Titmus 40” (Romano et al., 1975)
3-5 yrs. Frisby 250"
3-5 yrs. TNO 120"
Orthoptics: treating amblyopia
Main causes of amblyopia are strabismus
(squint) and/or anisometropia (one eye
more long-sighted than other)
Treated by (a) glasses and usually (80%)
also (b) patch
Treatment widely believed to be less
effective over 7y
Actually, only applies to strabismic amblyopia
C. Optom survey (1998):
75% of optoms treat anisometropic amblyopia
25% treat strabismic amblyopia (75% refer)
Unclear if just spectacles or patch too
PLAN
AVAILABILITY OF OPTOMETRIC EYECARE
OCULAR HEALTH
VISUAL ACUITY
REFRACTION
ORTHOPTIC FUNCTION
SUMMARY OF ROUTINE
SOME COMMENTS ON OPTOMETRIC RECORDS
CONCLUSIONS
Full handout from: www.bruce-evans.co.uk
12
Paediatrics: routine for 0-1.5 yr
attempt ophthalmoscopy
attempt visual acuity
reaction to occlusion, vertical prism, PL
test binocularity
corneal reflexes, cover test, motility, (Lang, 10∆ out)
retinoscopy
Paediatrics: routine for 1.5-4 yrs
ophthalmoscopy
visual acuity
reaction to occlusion, vertical prism, Cardiff cards, letter or picture matching
cover test, motility, stereo-test
maybe 20∆ out
retinoscopy
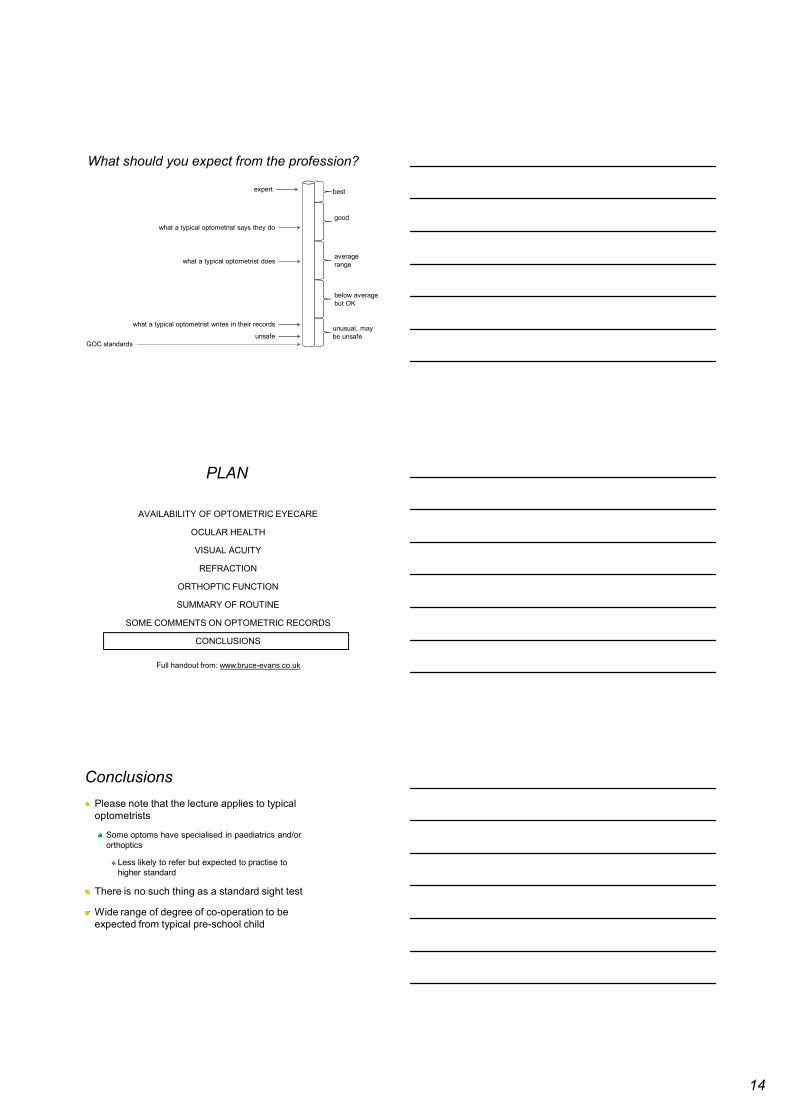
Re-exam intervalsDocument below from Optical Confederation is often taken literally
BUT: “each patient should be considered individually and a recall interval
recommended - which may be longer or shorter than the intervals in the
Memorandum - depending on the patient’s clinical needs”
13
PLAN
AVAILABILITY OF OPTOMETRIC EYECARE
OCULAR HEALTH
VISUAL ACUITY
REFRACTION
ORTHOPTIC FUNCTION
SUMMARY OF ROUTINE
SOME COMMENTS ON OPTOMETRIC RECORDS
CONCLUSIONS
Full handout from: www.bruce-evans.co.uk
Clinical records are an imperfect description
of the content of eye examinations
Rakhee ShahResearch Fellow Institute of Optometry
Post-graduate student City University
Bruce EvansDirector of Research Institute of Optometry
Visiting Professor City University
Visiting Professor London South Bank University
Private practice Brentwood, Essex
David EdgarProfessor of Clinical Optometry City University
Record abstraction: examples
46-65% of optometrists don’t record retinoscopy
Up to 18% of optometrists under-record motility,
but up to 16% can over-record this!
3-10% under-record visual fields
18-27% under-record biomicroscopy
14
What should you expect from the profession?
what a typical optometrist says they do
expert
average
range
unsafeGOC standards
good
below average
but OK
unusual, may
be unsafe
best
what a typical optometrist does
what a typical optometrist writes in their records
PLAN
AVAILABILITY OF OPTOMETRIC EYECARE
OCULAR HEALTH
VISUAL ACUITY
REFRACTION
ORTHOPTIC FUNCTION
SUMMARY OF ROUTINE
SOME COMMENTS ON OPTOMETRIC RECORDS
CONCLUSIONS
Full handout from: www.bruce-evans.co.uk
Conclusions
Please note that the lecture applies to typical
optometrists
Some optoms have specialised in paediatrics and/or
orthoptics
� Less likely to refer but expected to practise to
higher standard
There is no such thing as a standard sight test
Wide range of degree of co-operation to be
expected from typical pre-school child
15
GOC standards of practice
8.2.6 must record “Consent obtained for any examination”
Is all the profession guilty of misconduct?
“We find comfort
among those who
agree with us –
growth among those
who don’t.”
Frank A. Clark
Full handout of slides from www.bruce-evans.co.uk
Recommended