Phenotyping hypertensive patients Phenotyping hypertensive patients with blood and urine - with blood and urine -
inflammation, oxidative stress, fibrosis, angiogenesisinflammation, oxidative stress, fibrosis, angiogenesis
Jan Menne, Hermann Haller Department of Nephrology, Medical School Hannover

The first problem: The first problem: how translate risk factors into vascular disase ?how translate risk factors into vascular disase ?
Risk factors Clinical diseaseClinical disease
years and decadesyears and decades
Organ damage Organ damage „subclinical“„subclinical“
glucoseglucoselipidslipids
smokingsmokinghypertensionhypertension

Mechanisms of cardiovascular morbidity and mortalityMechanisms of cardiovascular morbidity and mortality
Progressive deterioration of organ function
years and decades
Sympatheticactivity
RAAS
Hypertension
DiabetesSmoking
Cholesterol
Risk factors
Clinical diseaseClinical disease

Mechanisms of cardiovascular morbidity and mortalityMechanisms of cardiovascular morbidity and mortality
Progressive deterioration of organ function
years and decades
Sympatheticactivity
RAAS
Hypertension
DiabetesSmoking
Cholesterol
Risk factors
Clinical diseaseClinical disease
Oxidative stress

Mechanisms of cardiovascular morbidity and mortalityMechanisms of cardiovascular morbidity and mortality
Progressive deterioration of organ function
years and decades
Sympatheticactivity
RAAS
Hypertension
DiabetesSmoking
Cholesterol
Risk factors
Clinical diseaseClinical disease
Oxidative stress
EC dysfunction

Mechanisms of cardiovascular morbidity and mortalityMechanisms of cardiovascular morbidity and mortality
Progressive deterioration of organ function
years and decades
Sympatheticactivity
RAAS
Hypertension
DiabetesSmoking
Cholesterol
Risk factors
Clinical diseaseClinical disease
Oxidative stress
EC dysfunction
Microinflammation

Mechanisms of cardiovascular morbidity and mortalityMechanisms of cardiovascular morbidity and mortality
Progressive deterioration of organ function
years and decades
Sympatheticactivity
RAAS
Hypertension
DiabetesSmoking
Cholesterol
Risk factors
Clinical diseaseClinical disease
Oxidative stress
EC dysfunction
Microinflammation
Hypertrophy/Fibrosis

Risk Factors for Future Cardiovascular Events
Relative Risk of Future Cardiovascular Events0
Ridker PM et al. N Engl J Med 2000;342:836-843.
Lipoprotein(a)
Homocysteine
IL-6
TC
LDL-C
sICAM-1
SAA
Apo B
TC:HDL-C
hs-CRP
hs-CRP + TC:HDL-C1.0 2.0 4.0 6.0

PREVEND Study (n = 8,592)
Blood pressure, hsCRP and microalbuminuria
Stuveling EM et al. Hypertension 2004; 43: 791

phenotyping - we are looking for patterns phenotyping - we are looking for patterns
hypertensionhypertension
OxidativeOxidativestressstress
Micro-Micro-inflammationinflammation
Hypertrophy Hypertrophy fibrosisfibrosisEC function/EC function/
AngiogensisAngiogensis

Ingenious Hypercare phenotyping platformsIngenious Hypercare phenotyping platforms
Oxidative stressOxidative stress
Micro-Micro-inflammationinflammation
Hypertrophy Hypertrophy FibrosisFibrosis
EC function/EC function/AngiogenesisAngiogenesis

Structure of the phenotyping program
patient information
Clinical assessment
clinical data
data processing and management
vascular function
blood samples
ELISAMS
UltrasoundNMRFMDSphygmocor
urine analysis
proteomics
storage

Ingenious Hypercare phenotyping platformsIngenious Hypercare phenotyping platforms
Oxidative stressOxidative stress
Micro-Micro-inflammationinflammation
Hypertrophy Hypertrophy FibrosisFibrosis
EC function/EC function/AngiogenesisAngiogenesis

Ingenious Hypercare phenotyping platformsIngenious Hypercare phenotyping platforms
Oxidative Oxidative stressstress
ADMAADMAAOPPAOPPOx-LDLOx-LDL
GlutathionperoxidaseGlutathionperoxidaseCarbonylated proteinsCarbonylated proteinsMPOMPOMalondialdehydMalondialdehyds-RAGEs-RAGE
Others others others ?Others others others ?

Zoccali et al. Lancet 358:2113-7, 2001
Fatal and non fatal Fatal and non fatal cardiovascular eventscardiovascular events
1.01.0
.9.9
.8.8
.7.7
.6.6
.5.5
46.746.740.040.033.333.326.726.720.020.013.313.36.76.700
TimeTime(months)(months)
All cause mortalityAll cause mortality
46.746.740.040.033.333.326.726.720.020.013.313.36.76.700
1.01.0
.9.9
.8.8
.7.7
.6.6
.5.5
TimeTime(months)(months)
Cumulative Cumulative survivalsurvival
<50<50thth percentile percentile
5050thth –75th percentile –75th percentile
>75th percentile>75th percentile
<50<50thth percentile percentile
5050thth –75th percentile –75th percentile
>75th percentile>75th percentile
* * Fully adjusted for traditional and non Fully adjusted for traditional and non traditional risk factorstraditional risk factors
* * Fully adjusted for traditional and non Fully adjusted for traditional and non traditional risk factorstraditional risk factors
ADMA and cardiovascular mortality

Ingenious Hypercare phenotyping platformsIngenious Hypercare phenotyping platforms
Micro-Micro-inflammationinflammation
C-reactive proteinC-reactive proteinSerum amyloid ASerum amyloid AFibrinogenFibrinogenIL-6IL-6IL-6 STIL-6 STIL-12IL-12TNF-aTNF-aMCP-1MCP-1s-ICAMs-ICAMCD 40CD 40s-VCAMs-VCAM
gluPAI ?gluPAI ?Others others others ?Others others others ?
LeukocytesLeukocytesAlbuminAlbumin

Ingenious Hypercare phenotyping platformsIngenious Hypercare phenotyping platforms
EC function/EC function/AngiogenesisAngiogenesis vWFvWF
circulating damaged ECcirculating damaged ECMicroparticlesMicroparticlesEPCsEPCs
VEGFVEGFs-flt-1s-flt-1angiopoietin-1, -2angiopoietin-1, -2
uPA/s-uPA-R ?uPA/s-uPA-R ?

Endothelial cell
Basement membrane
Tie2 controls endothelial activation
Ang-1Ang-1
Ang-2Ang-2(Weibel-Palade-(Weibel-Palade-
bodies)bodies)
Disassembley of
adherence junctions
E-selectin, ICAM-1, VCAM-1
Survival
Tie2Tie2RezeptorRezeptor
Stimulation (e.g. Immune complex)
Maintenance

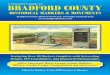
(A) CKD Patienten (HD, PD, und NTx zusammen, n=117) (B) HD Patienten (n=61) (C) PD Patienten (n=24) und (D) NTx Patienten (n=32)
Coronary angiography
Doppler ultrasound
PAOD [Fontaine]
CHD (1 VD)
CHD (2 VD)
CHD (3 VD)
Stadium I
Stadium IIa
Stadium IIb
Stadium III
Stadium IV
mild
moderate
severe
+1
+2
+3
+2
+3
+4
+5
+1
+3
+1
+2
min points 00
max points 1111
Circulating Ang-2 correlates with atherosclerotic burden
Kümpers P, David S, Hellpap J, Horn R, Leitolf H, Haller H, Kielstein JT.Angiopoietin 2 and Cardiovascular Disease in Dialysis and Kidney Transplantation.Am J Kidney Dis. 2009 Mar 4. [Epub ahead of print]

Circulating Ang-2 levels are higher in hypertensive patients
Kümpers P, David S, Hellpap J, Horn R, Leitolf H, Haller H, Kielstein JT.Angiopoietin 2 and Cardiovascular Disease in Dialysis and Kidney Transplantation.Am J Kidney Dis. 2009 Mar 4. [Epub ahead of print]

Ingenious Hypercare phenotyping platformsIngenious Hypercare phenotyping platforms
TGF-bTGF-bOsteopontinOsteopontinCTGFCTGFMMPMMPAdiponectinAdiponectinFGFsFGFs
gluPAI ?gluPAI ?Others others others ?Others others others ?
Hypertrophy Hypertrophy FibrosisFibrosis

Effects of treatment is important to knowEffects of treatment is important to know
30
40
Baseline 6 weeks 12 weeks
p < 0.05
p < 0.001
A
plas
ma
OP
N (
ng
/ml)
Angiopoetin -2 Osteopontin

no phenotyping without well characterized no phenotyping without well characterized patients and families !patients and families !
hypertensionhypertension
OxidativeOxidativestressstress
Micro-Micro-inflammationinflammation
Hypertrophy Hypertrophy fibrosisfibrosisEC function/EC function/
AngiogensisAngiogensis
Recommended