2012
Occurrence Variance Report Annual Report 2012
Patient Safety & Risk Management Unit KING KHALID UNIVERSITY HOSPITAL
2 OVR Annual Report 2012
TABLE OF CONTENTS
Introduction 3
Statistical Snapshot 2012 4
Classification of Occurrences 5
Reporting Departments 6
Reporter 7
OVR Categories 8
Clinical Practice/Procedure 10
Medication 11
Family/Visitor/Watcher 12
Staff/Employee 13
Equipment/Supplies 13
Safety 14
Fire/Security 14
Behavioral 15
Patient Care 16
Recommendations 17
References 17
Appendix – OVR Form 17
3 OVR Annual Report 2012
INTRODUCTION King Khalid University Hospital attaches the greatest of importance to the safety of patients,
employees, visitors and those who access our services and facilities. It is essential that
management and staff work together positively to achieve a situation consistent with the
provision of safe, high quality services to patients, where preventable incidents can be reduced
to a minimum.
All Occurrence Variances are encouraged to be reported at KKUH and as an organization it is
important there is a common understanding of what constitutes an untoward incident.
It is essential that following any occurrence variance or adverse event, an OVR is completed
and forwarded to Quality Management Department (QMD). The report is checked for
completeness, logged, forwarded to the designated QM Coordinator, sent to the Concerned
Department where appropriate action is taken relating to the event. On completion the OVR is
returned to Quality Management Department where the designated coordinator will check the
action and provide feedback as required. It is then scanned, returned to the Reporter, and any
concerned persons/department heads. In some instances an OVR may involve two departments
and a photocopy of the original OVR is made and sent to the respective department for follow-
up.
If a particular OVR requires further investigation, this is the responsibility of the Concerned
Department. For example a policy may need to be revised or developed, a procedure reviewed,
equipment changed, resources re-allocated.
If, on receiving an OVR it is classified as a Sentinel Event it is raised to the Director of QMD
who will initiate appropriate action and/or decide on an investigation using, for example, a
Root Cause Analysis approach.
As an organization there is a need to ensure all occurrence variances are reported. The Quality
Management Department is committed to encouraging staff to be open and honest in the
formal reporting of occurrence variance and near misses. To facilitate this we need to support
a philosophy that advocates a Just Culture, where the employee reporting an occurrence
variance feels confident that he/she has the support of Leadership. The overall outcome of an
occurrence variance is to improve systems not blame individuals.
The total number of Occurrence Variance Reports can provide valuable information and guide
our organization to improve safety practices. If staff fail to report due to concerns that
reporting will result in repercussions this will impact on achieving our objectives of providing
safe, high quality care and services to our clients. We urge all staff to report all occurrence
variance and promote positive safety outcomes at our hospital.
The Quality Management Department is looking forward to launching the (electronic) e-OVR
which will become effective in January 2013.
4 OVR Annual Report 2012
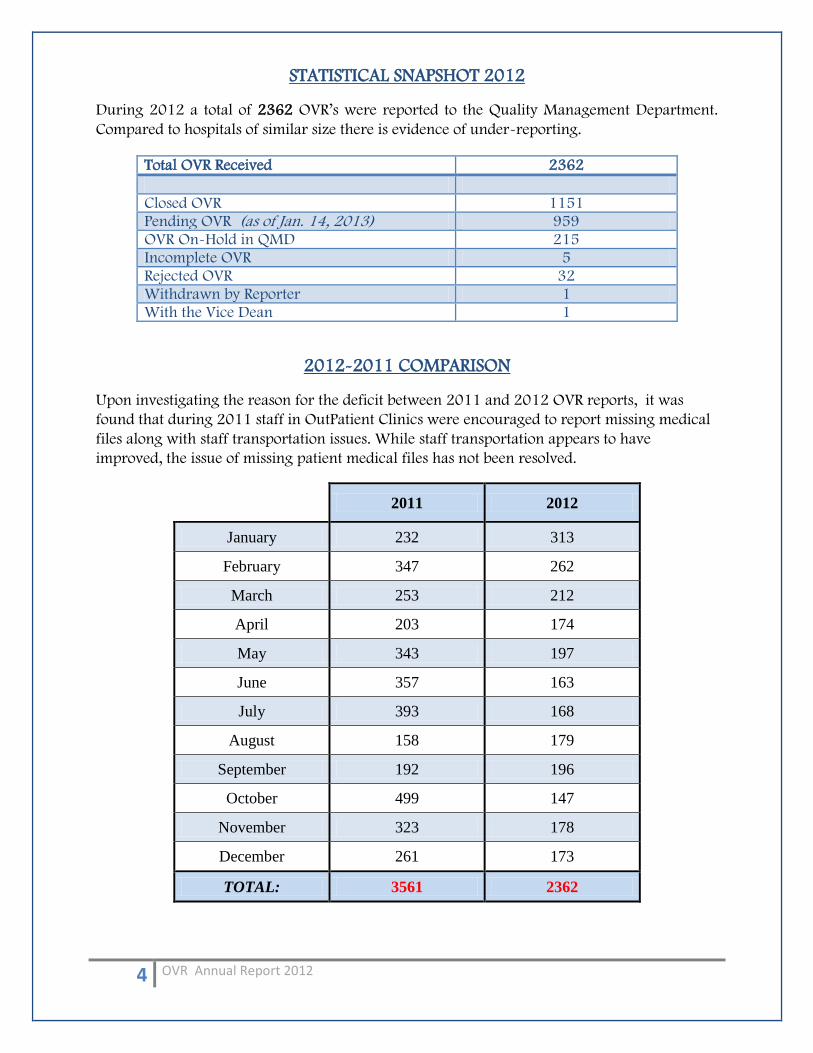
STATISTICAL SNAPSHOT 2012
During 2012 a total of 2362 OVR’s were reported to the Quality Management Department.
Compared to hospitals of similar size there is evidence of under-reporting.
2012-2011 COMPARISON
Upon investigating the reason for the deficit between 2011 and 2012 OVR reports, it was
found that during 2011 staff in OutPatient Clinics were encouraged to report missing medical
files along with staff transportation issues. While staff transportation appears to have
improved, the issue of missing patient medical files has not been resolved.
2011 2012
January 232 313
February 347 262
March 253 212
April 203 174
May 343 197
June 357 163
July 393 168
August 158 179
September 192 196
October 499 147
November 323 178
December 261 173
TOTAL: 3561 2362
Total OVR Received 2362
Closed OVR 1151 Pending OVR (as of Jan. 14, 2013) 959 OVR On-Hold in QMD 215 Incomplete OVR 5 Rejected OVR 32 Withdrawn by Reporter 1 With the Vice Dean 1

5 OVR Annual Report 2012
CLASSIFICATION OF OCCURRENCES
A Sentinel Event is defined as an unexpected occurrence involving the death or serious
physical or psychological injury, or risk thereof, including loss of limb or function, signaling
the need for immediate investigation and response.
A Major Event is defined as any occurrence which did not affect the outcome but for which a
recurrence carries a significant chance of a serious adverse outcome.
An Occurrence is defined as any event or circumstance that deviates from established
standards or care.
Near Miss is defined as any process variation which did not affect the outcome (by chance or
intervention), but for which a recurrence carries a significant chance of serious adverse
outcomes.
Sentinel Event Major Occurrence Near Miss
2012 0 51 2271 40
6 OVR Annual Report 2012
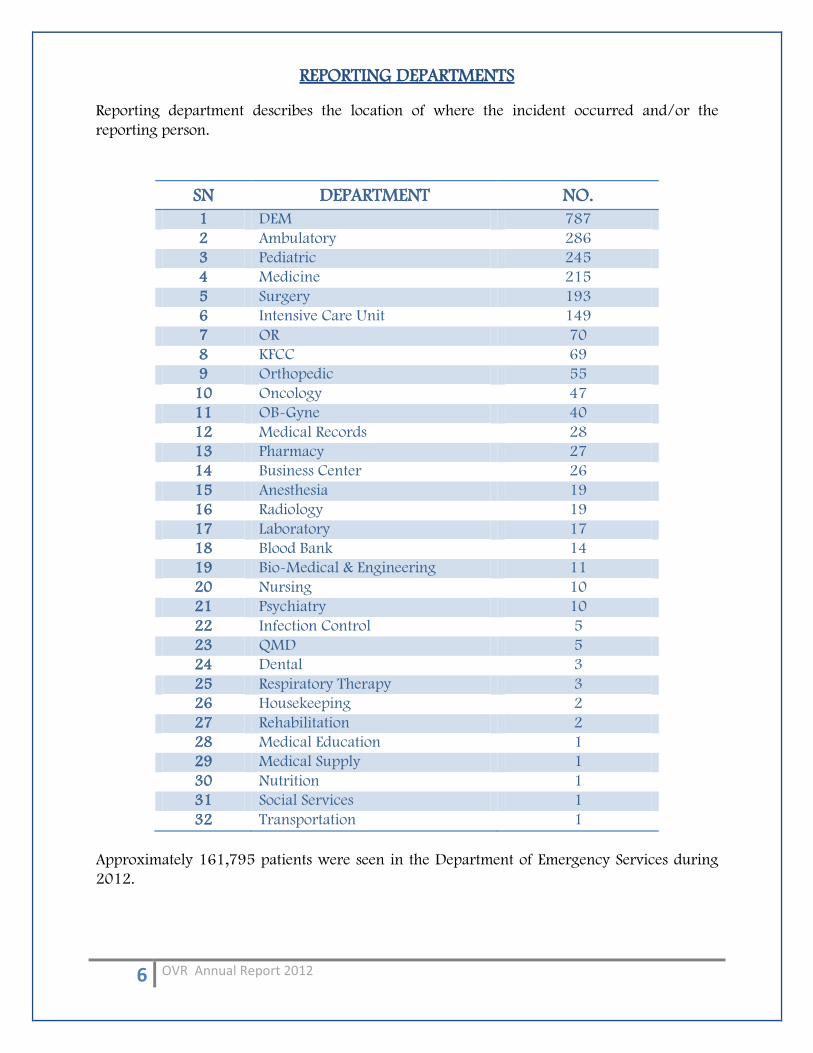
REPORTING DEPARTMENTS Reporting department describes the location of where the incident occurred and/or the
reporting person.
SN DEPARTMENT NO.
1 DEM 787
2 Ambulatory 286
3 Pediatric 245
4 Medicine 215
5 Surgery 193
6 Intensive Care Unit 149
7 OR 70
8 KFCC 69
9 Orthopedic 55
10 Oncology 47
11 OB-Gyne 40
12 Medical Records 28
13 Pharmacy 27
14 Business Center 26
15 Anesthesia 19
16 Radiology 19
17 Laboratory 17
18 Blood Bank 14
19 Bio-Medical & Engineering 11
20 Nursing 10
21 Psychiatry 10
22 Infection Control 5
23 QMD 5
24 Dental 3
25 Respiratory Therapy 3
26 Housekeeping 2
27 Rehabilitation 2
28 Medical Education 1
29 Medical Supply 1
30 Nutrition 1
31 Social Services 1
32 Transportation 1
Approximately 161,795 patients were seen in the Department of Emergency Services during
2012.

7 OVR Annual Report 2012
REPORTER Nursing staff are one of the largest employee groups and also the dominate reporting group.
REPORTER NO. Nurses 1944 Doctors 280 Technician 122 Head of Department 8 QMD 5 Housekeeping 2 Social Worker 1
PERSON INVOLVED Occurrence Variances can include any persons involved either as a pateint, employee, visitor or watcher. Patients, and those directly involved in health care are more likely to be persons involved in an occurrence variance.
PERSON INVOLVED NO. Others (see below for firther catergorisation) 904 Staff 672 Patient 666 Watcher 99 Visitor 21
OTHERS
Other involved categories include Medical Records, Medical Supplies, Biomedical and Engineering.
OTHERS – Related to No. Bed Management 181 Bio-medical & Eng’g 47 Dietary 9 Housekeeping 12 Housing 1 Infection Control 1 Information Management 12 Maintenance 110 Medical Files 297 Medical Supplies 117 Medication 23 Relatives 23 Safety & Security 42 Transportation 40
8 OVR Annual Report 2012
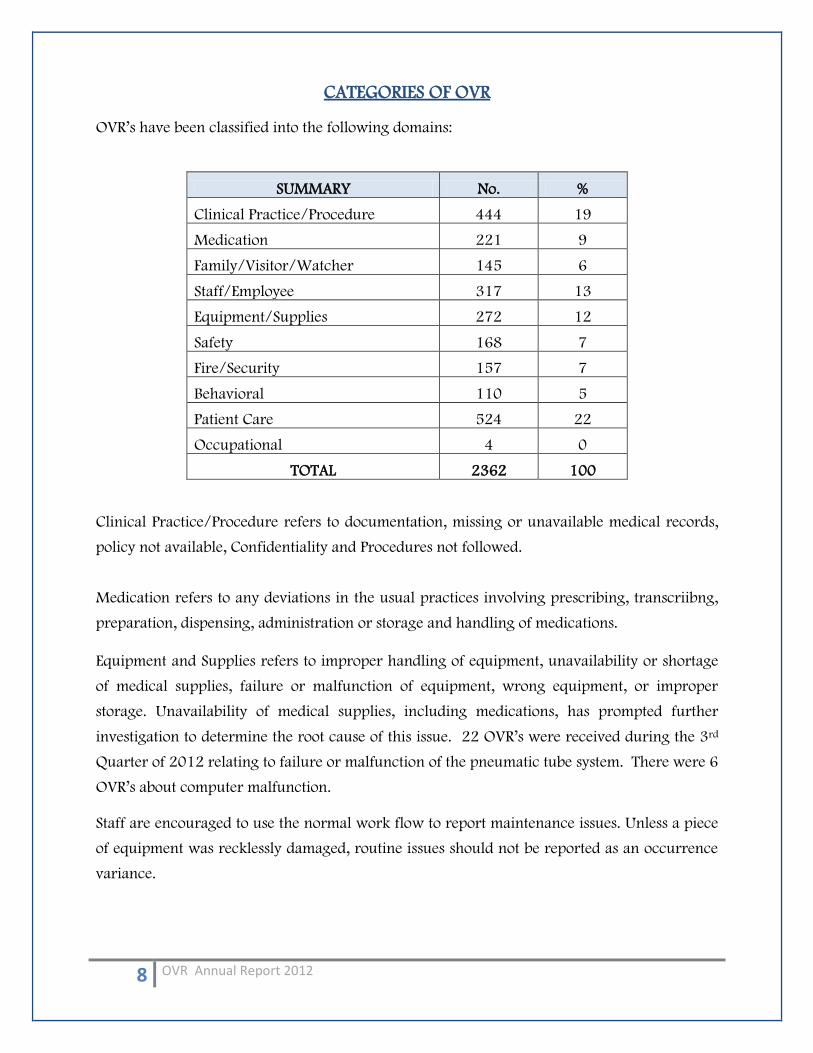
CATEGORIES OF OVR OVR’s have been classified into the following domains:
SUMMARY No. %
Clinical Practice/Procedure 444 19
Medication 221 9
Family/Visitor/Watcher 145 6
Staff/Employee 317 13
Equipment/Supplies 272 12
Safety 168 7
Fire/Security 157 7
Behavioral 110 5
Patient Care 524 22
Occupational 4 0
TOTAL 2362 100 Clinical Practice/Procedure refers to documentation, missing or unavailable medical records,
policy not available, Confidentiality and Procedures not followed.
Medication refers to any deviations in the usual practices involving prescribing, transcriibng,
preparation, dispensing, administration or storage and handling of medications.
Equipment and Supplies refers to improper handling of equipment, unavailability or shortage
of medical supplies, failure or malfunction of equipment, wrong equipment, or improper
storage. Unavailability of medical supplies, including medications, has prompted further
investigation to determine the root cause of this issue. 22 OVR’s were received during the 3rd
Quarter of 2012 relating to failure or malfunction of the pneumatic tube system. There were 6
OVR’s about computer malfunction.
Staff are encouraged to use the normal work flow to report maintenance issues. Unless a piece
of equipment was recklessly damaged, routine issues should not be reported as an occurrence
variance.
9 OVR Annual Report 2012
Occupational incidents are reported via the OVR system and usually involve the Occupational
Health department. As this is a newly established department and not fully operational, the
Infection Control department often deal with these occurrence variances. Needle stick injuries
have been the major staff related injury during 2012.
Monthly and Quarterly Occurrence Variance reports are submitted to each QMD Coordinator
responsible for their department. The quarterly report is forwarded to the respective
department. This provides the opportunity for departments to gauge their reported OVR’s on
an accumulative basis and determine an appropriate action plan. An Annual Data Base is also
reported to the Director of Qualtiy Management and Quality Management Coordinators.
Departmental Indicators have been developed and are being monitored by departments.
The following part of this report will focus on the high volume, high risk, error-prone OVR’s
10 OVR Annual Report 2012
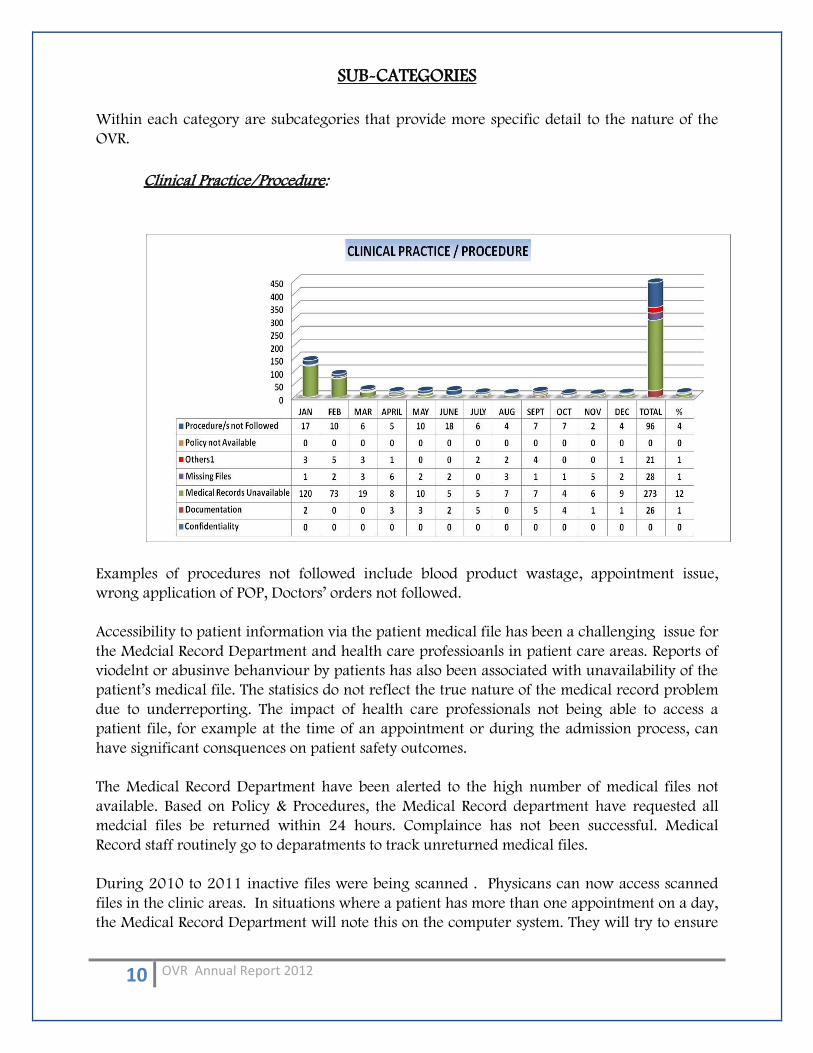
SUB-CATEGORIES
Within each category are subcategories that provide more specific detail to the nature of the
OVR.
Clinical Practice/Procedure:
Examples of procedures not followed include blood product wastage, appointment issue,
wrong application of POP, Doctors’ orders not followed.
Accessibility to patient information via the patient medical file has been a challenging issue for
the Medcial Record Department and health care professioanls in patient care areas. Reports of
viodelnt or abusinve behanviour by patients has also been associated with unavailability of the
patient’s medical file. The statisics do not reflect the true nature of the medical record problem
due to underreporting. The impact of health care professionals not being able to access a
patient file, for example at the time of an appointment or during the admission process, can
have significant consquences on patient safety outcomes.
The Medical Record Department have been alerted to the high number of medical files not
available. Based on Policy & Procedures, the Medical Record department have requested all
medcial files be returned within 24 hours. Complaince has not been successful. Medical
Record staff routinely go to deparatments to track unreturned medical files.
During 2010 to 2011 inactive files were being scanned . Physicans can now access scanned
files in the clinic areas. In situations where a patient has more than one appointment on a day,
the Medical Record Department will note this on the computer system. They will try to ensure
11 OVR Annual Report 2012
the file goes to the first appointment. It is then the responsibility of the clinic to ensure the file
is forwarded on to the next clinic.
In some clinic areas there is access to the patients medicaiton history but this is not consistent
or convenient as the access may be in a location away from the Physician/Client actual
consultation. Access to the patients medication history in the absence of an unavailable medical
file is crucial in some situaiton, for example Oncology patients receiving chemotherapy.
The operational function of the Medical Record Department requires close studying to pin
point areas for improvement. The antiquated medical filing system is also in need of a major
overhaul. The new eSiHi system should provide a great relief for all patients and health care
professionals once established. The problem is significant and urgent critical action is requied
by Leadership to reovled this issue.
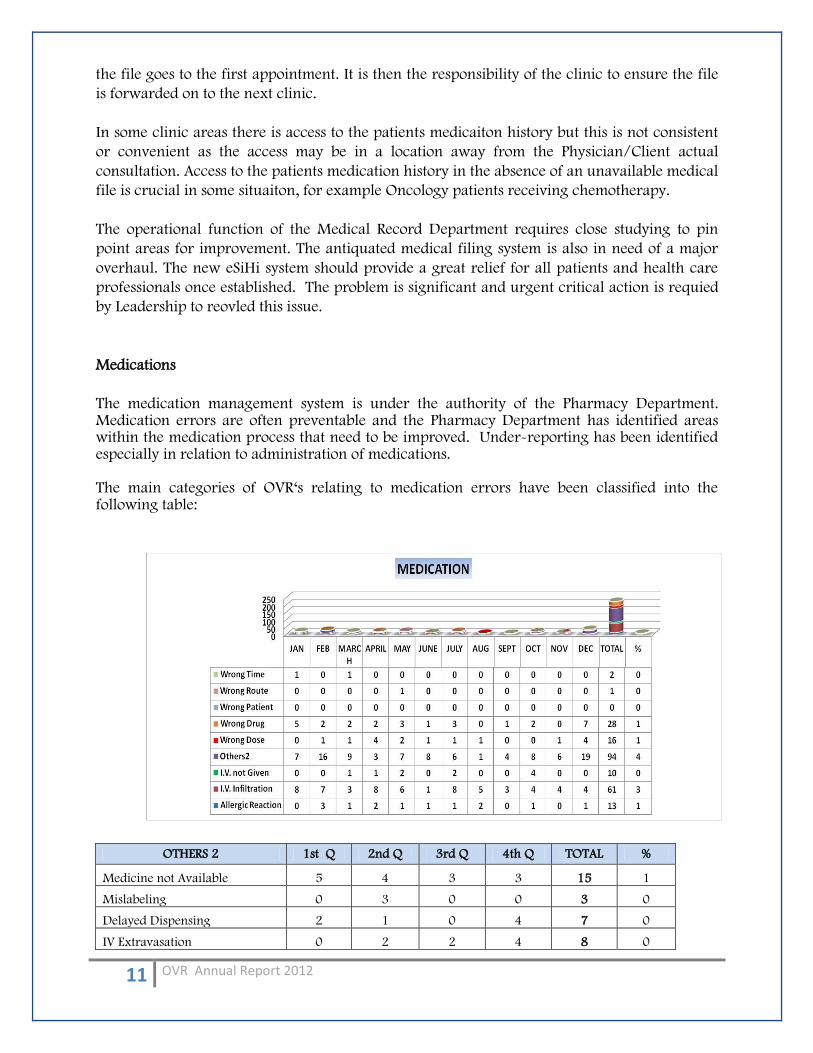
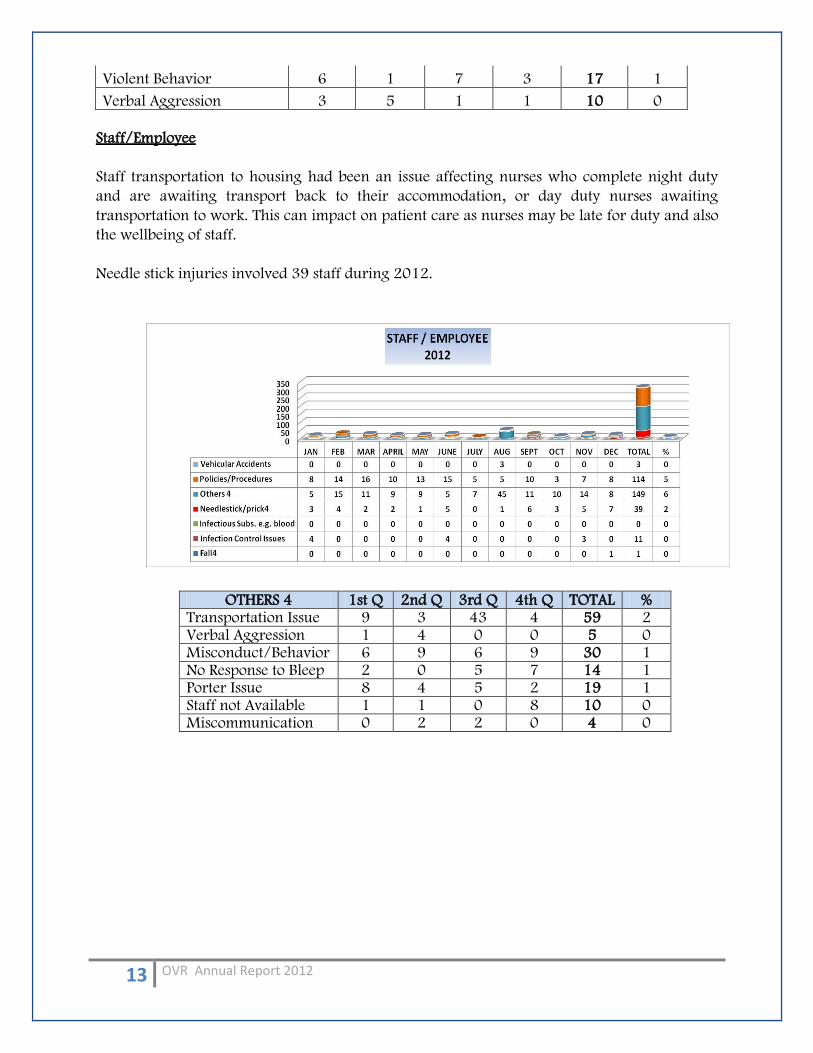
Medications
The medication management system is under the authority of the Pharmacy Department. Medication errors are often preventable and the Pharmacy Department has identified areas within the medication process that need to be improved. Under-reporting has been identified especially in relation to administration of medications. The main categories of OVR‘s relating to medication errors have been classified into the following table:
OTHERS 2 1st Q 2nd Q 3rd Q 4th Q TOTAL %
Medicine not Available 5 4 3 3 15 1
Mislabeling 0 3 0 0 3 0
Delayed Dispensing 2 1 0 4 7 0
IV Extravasation 0 2 2 4 8 0
12 OVR Annual Report 2012
Broken Narcotic Ampoule 3 2 0 1 6 0
Medicine On Hold 6 2 3 0 11 0
Unconsumed PCA 10 0 0 0 10 0
Prepared Meds not Given 0 0 0 10 10 0
The double checking process in Pharmacy has been raised as an areas of concern and staff
related issues such as Arabic literacy (cannot read English) and understaffing of pharmacists
have been identifed.
Medication availability is linked to actual medications on hand in the medical supply
department. The Inventory system for medication and a re-ordering process are examples of
areas for improvement. The purchasing process from vendors also may need to be considered
and establishment of secure contracts where supply is minimally an issue.
Broken Drill Bits
Previouysly there were few occurences relating to this issue but during 2012 a total of 11
broken drill bits were reported. This matter has been raised to the Director of Quality
Management.
OTHERS 1st Q 2nd Q 3rd Q 4th Q TOTAL
Broken Drill Bit 4 0 4 3 11
Family/Visitor/Watcher:
Unauthorised Watchers are often additional persons staying with the patient without
authorisation. On many occassions there is no transportation available to take the person
home. The Patient Relations Officer is usually called and gives approval for the person to
remain for the night. This however poses spacial problems and is not in accordance to hospital
policy.
Accommodation is not available within the hospital. Accommodation can be arranged via the
Social Work department but are usually reserved for out of town families who have a
hosptialised patient. It is also not possible for a unchaperoned female to travel alone.
OTHERS 3 1st Q 2nd Q 3rd Q 4th Q TOTAL %
Refused to take patient home 8 2 0 0 10 0
Unauthorized Watcher 30 17 14 9 70 3
13 OVR Annual Report 2012
Violent Behavior 6 1 7 3 17 1
Verbal Aggression 3 5 1 1 10 0
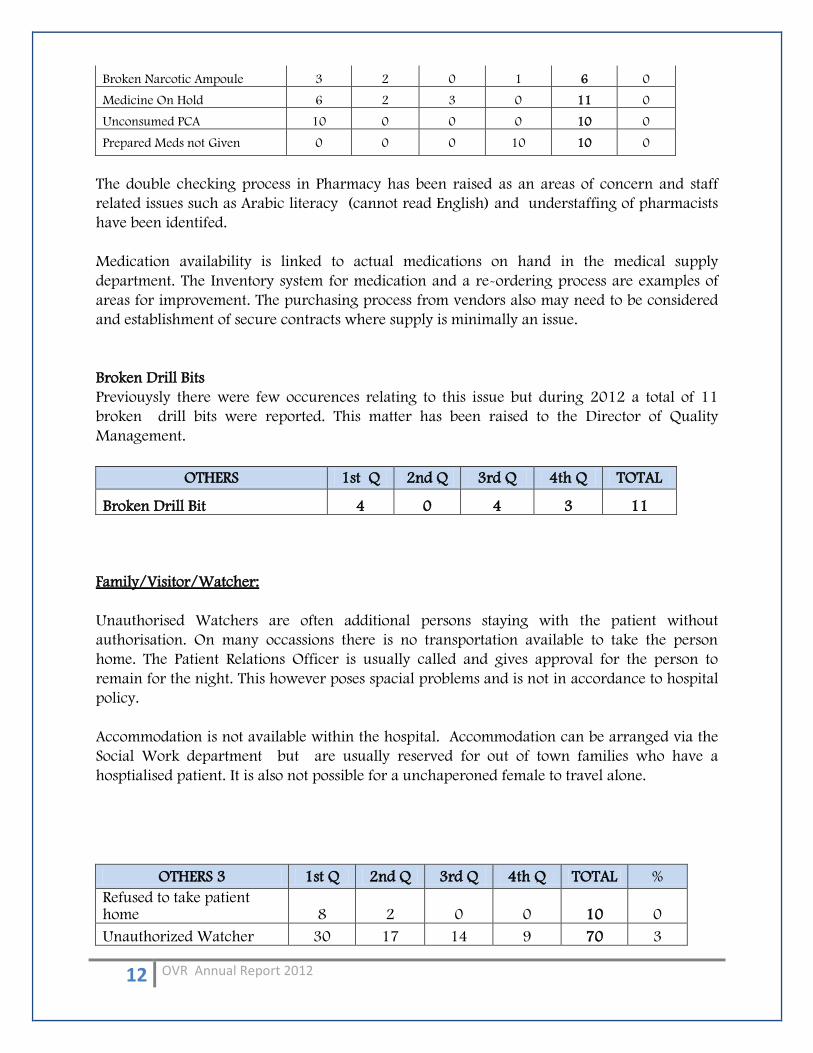
Staff/Employee
Staff transportation to housing had been an issue affecting nurses who complete night duty
and are awaiting transport back to their accommodation, or day duty nurses awaiting
transportation to work. This can impact on patient care as nurses may be late for duty and also
the wellbeing of staff.
Needle stick injuries involved 39 staff during 2012.
OTHERS 4 1st Q 2nd Q 3rd Q 4th Q TOTAL % Transportation Issue 9 3 43 4 59 2 Verbal Aggression 1 4 0 0 5 0 Misconduct/Behavior 6 9 6 9 30 1 No Response to Bleep 2 0 5 7 14 1 Porter Issue 8 4 5 2 19 1 Staff not Available 1 1 0 8 10 0 Miscommunication 0 2 2 0 4 0
14 OVR Annual Report 2012
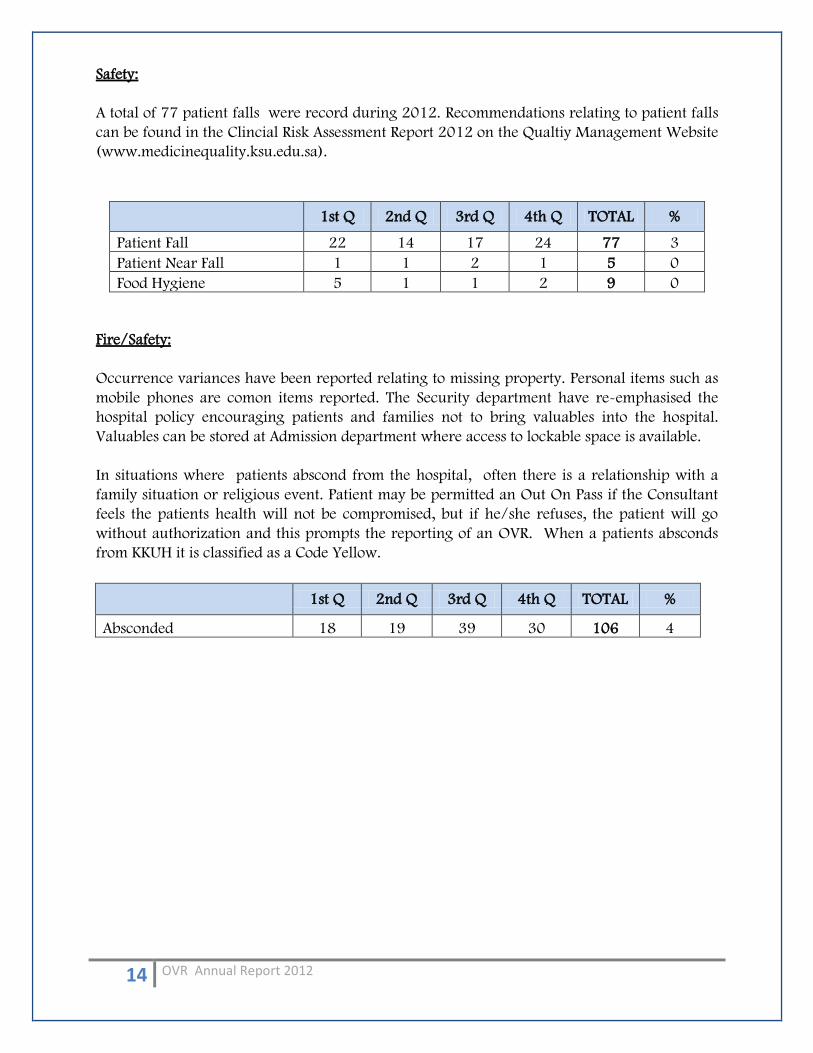
Safety:
A total of 77 patient falls were record during 2012. Recommendations relating to patient falls
can be found in the Clincial Risk Assessment Report 2012 on the Qualtiy Management Website
(www.medicinequality.ksu.edu.sa).
1st Q 2nd Q 3rd Q 4th Q TOTAL %
Patient Fall 22 14 17 24 77 3
Patient Near Fall 1 1 2 1 5 0
Food Hygiene 5 1 1 2 9 0
Fire/Safety:
Occurrence variances have been reported relating to missing property. Personal items such as
mobile phones are comon items reported. The Security department have re-emphasised the
hospital policy encouraging patients and families not to bring valuables into the hospital.
Valuables can be stored at Admission department where access to lockable space is available.
In situations where patients abscond from the hospital, often there is a relationship with a
family situation or religious event. Patient may be permitted an Out On Pass if the Consultant
feels the patients health will not be compromised, but if he/she refuses, the patient will go
without authorization and this prompts the reporting of an OVR. When a patients absconds
from KKUH it is classified as a Code Yellow.
1st Q 2nd Q 3rd Q 4th Q TOTAL %
Absconded 18 19 39 30 106 4
15 OVR Annual Report 2012
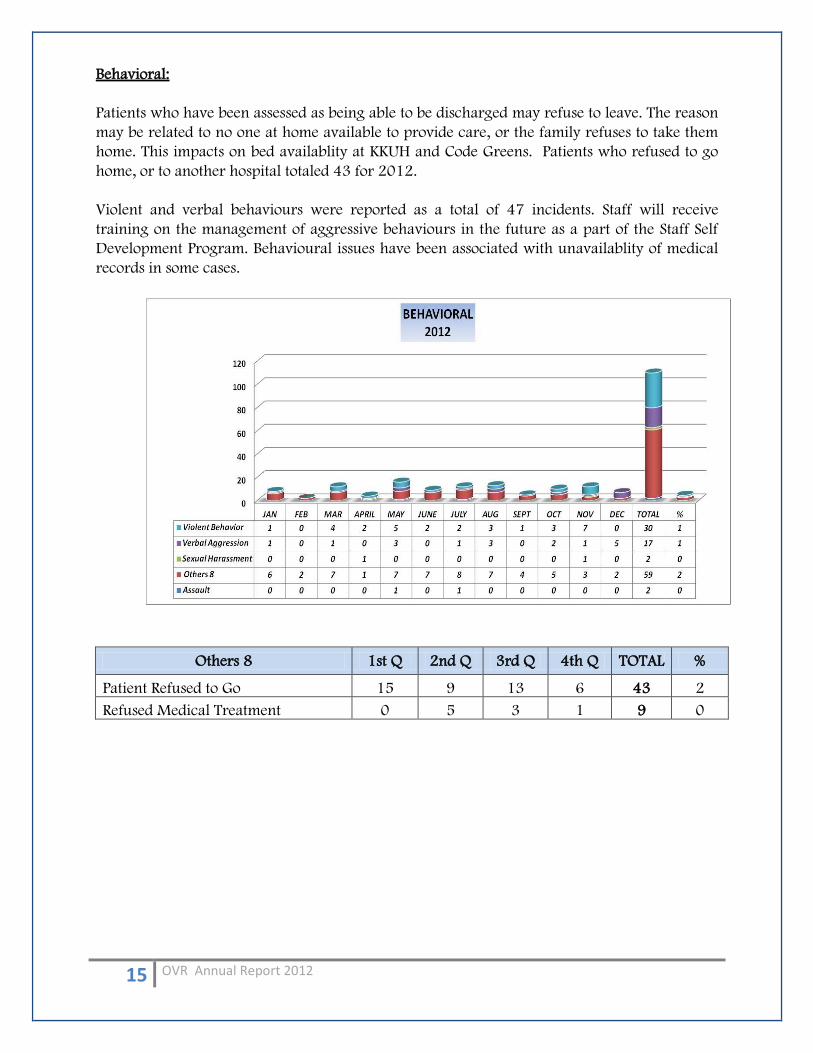
Behavioral:
Patients who have been assessed as being able to be discharged may refuse to leave. The reason
may be related to no one at home available to provide care, or the family refuses to take them
home. This impacts on bed availablity at KKUH and Code Greens. Patients who refused to go
home, or to another hospital totaled 43 for 2012.
Violent and verbal behaviours were reported as a total of 47 incidents. Staff will receive
training on the management of aggressive behaviours in the future as a part of the Staff Self
Development Program. Behavioural issues have been associated with unavailablity of medical
records in some cases.
Others 8 1st Q 2nd Q 3rd Q 4th Q TOTAL %
Patient Refused to Go 15 9 13 6 43 2
Refused Medical Treatment 0 5 3 1 9 0
16 OVR Annual Report 2012
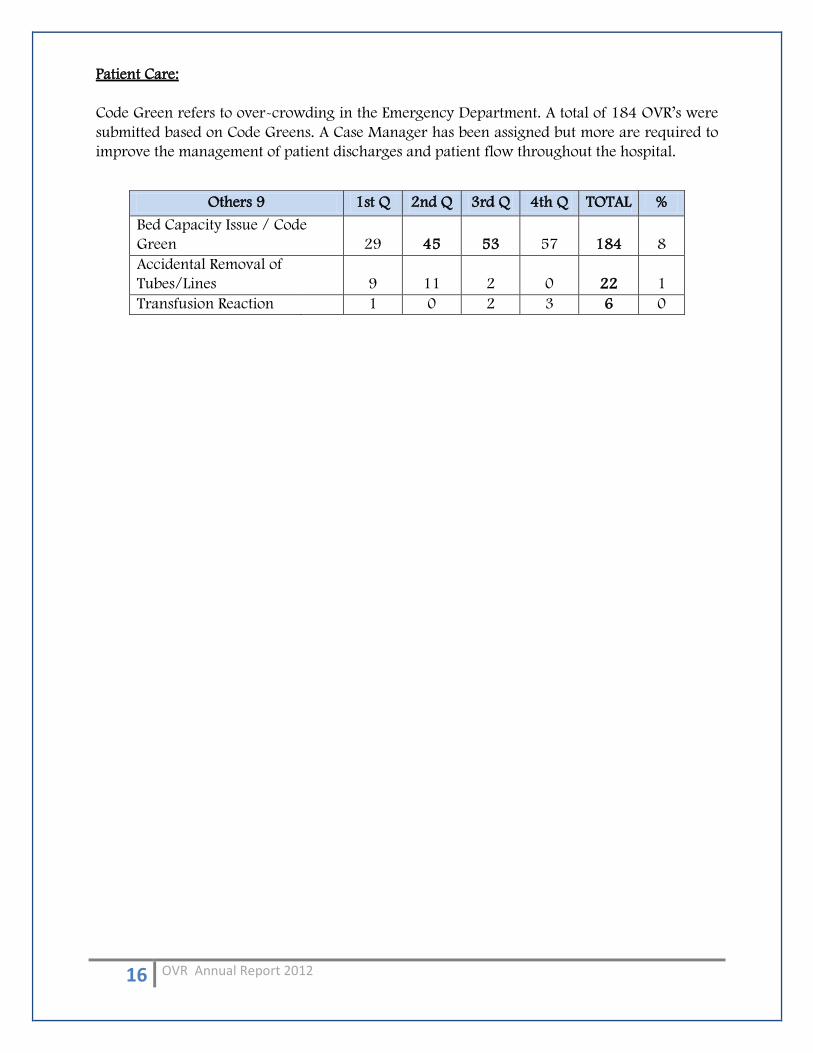
Patient Care:
Code Green refers to over-crowding in the Emergency Department. A total of 184 OVR’s were
submitted based on Code Greens. A Case Manager has been assigned but more are required to
improve the management of patient discharges and patient flow throughout the hospital.
Others 9 1st Q 2nd Q 3rd Q 4th Q TOTAL %
Bed Capacity Issue / Code
Green 29 45 53 57 184 8
Accidental Removal of
Tubes/Lines 9 11 2 0 22 1
Transfusion Reaction 1 0 2 3 6 0
17 OVR Annual Report 2012
RECOMMENDATIONS
It is essential that Senior Management consider the major issues affecting our hospital and put
in place strategies to facilate improvement. Each department is also encouraged to develop
quality improvement plans as applicable.
Currently we do not grade occurrance variances based on a risk matrix and future plans
include establishing a risk management process integrated into the OVR system.
A full copy of the Annual 2012 Occurrence Variance Report is available from QMD.
Please contact QMD if you would like to discuss this report further.
References
Occurrence Variance Report (OVR) Quality Management Department, King Khalid University Hospital: For the Period Oct. 2011-Oct. 2012.

18 OVR Annual Report 2012
Recommended