9/27/17
1
SafeDrivingforIndividualswithLowVisionandBrainInjuryJ A SONVICE , M. S. , OTR/ L
UA BCENTERF ORLOWVI SIONREHABI LI TAT ION
ObjectivesDefinetheclinicaltermlowvision.
Identifycommondiagnosesthatlimitdrivingperformanceforindividualswithlowvision.Describehowdrivingperformanceisimpactedbyvisualdeficits.
Describetheroleofthegeneralpractitionerinsafereturntodriving.
Describetheroleofthelowvisionspecialistinsafereturntodriving.
Understandtheuseofbioptictelescopesfordriving.
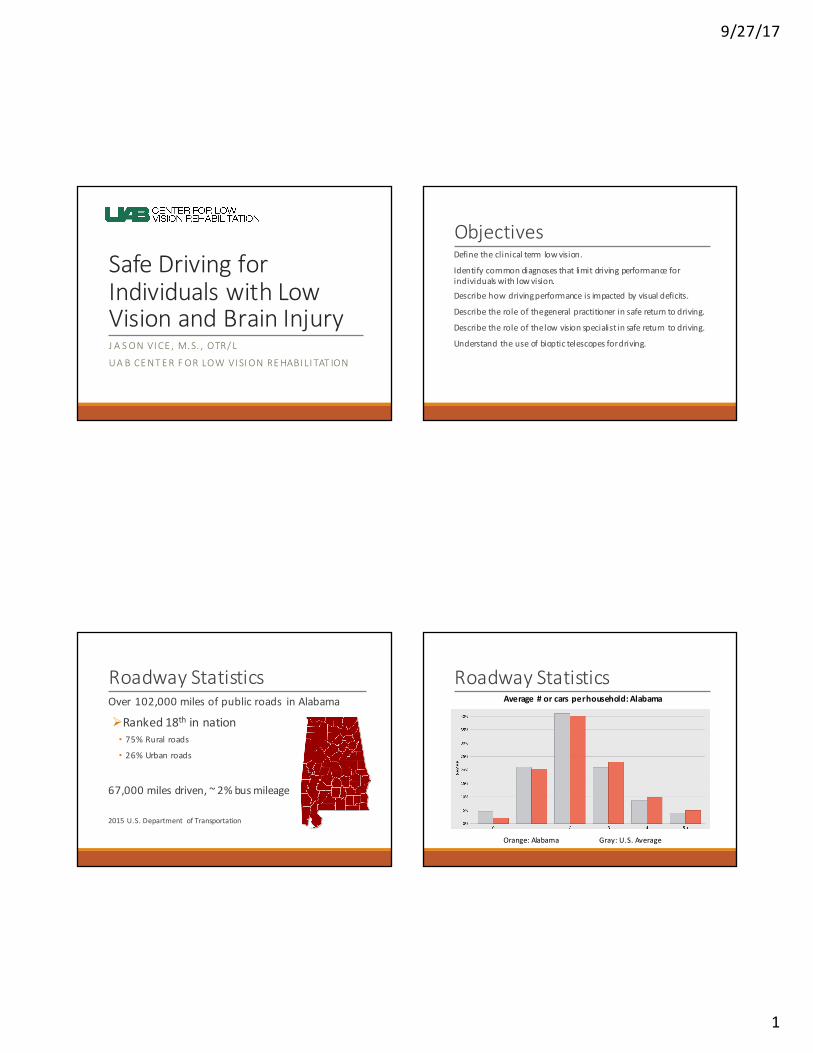
RoadwayStatisticsOver102,000milesofpublicroads inAlabama
ØRanked18th innation• 75%Ruralroads
• 26%Urbanroads
67,000milesdriven,~2%busmileage
2015U.S.Department ofTransportation
RoadwayStatisticsAverage#orcarsperhousehold:Alabama
Orange:Alabama Gray:U.S.Average
9/27/17
2
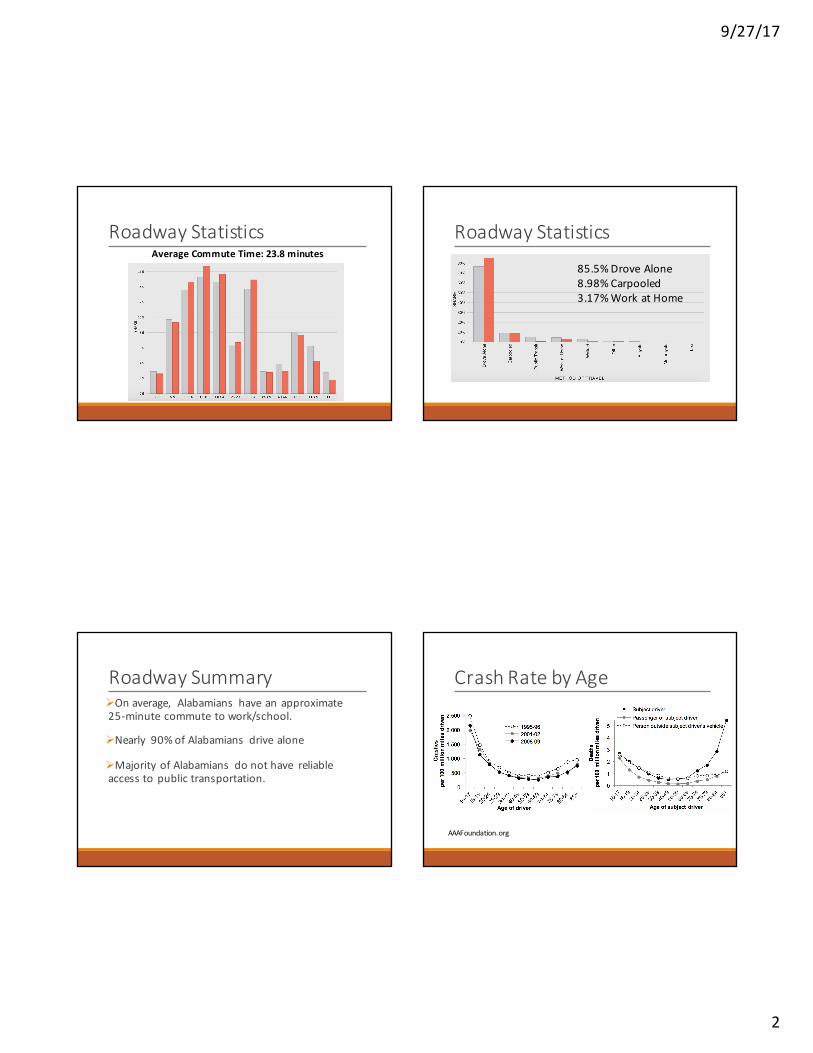
RoadwayStatisticsAverageCommuteTime:23.8minutes
RoadwayStatistics
85.5%DroveAlone8.98%Carpooled3.17%WorkatHome
RoadwaySummaryØOnaverage, Alabamians haveanapproximate 25-minutecommute towork/school.
ØNearly 90%ofAlabamians drivealone
ØMajorityofAlabamians donothave reliableaccesstopublictransportation.
CrashRatebyAge
AAAFoundation.org
9/27/17
3
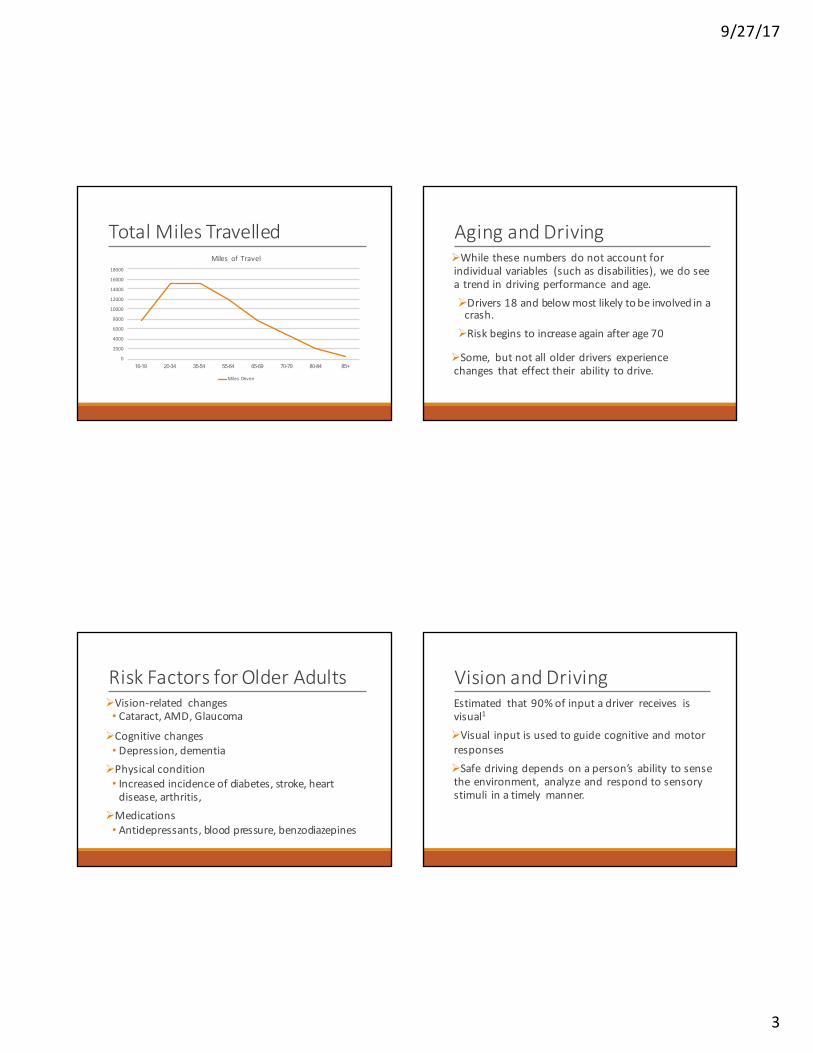
TotalMilesTravelled
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
16-19 20-34 35-54 55-64 65-69 70-79 80-84 85+
Miles ofTravel
Miles Driven
AgingandDrivingØWhile thesenumbersdonotaccountforindividualvariables (suchasdisabilities),wedoseea trendindrivingperformance andage.ØDrivers18andbelowmostlikelytobeinvolvedinacrash.
ØRiskbeginstoincreaseagainafterage70
ØSome, butnotallolderdriversexperiencechanges thateffecttheir ability todrive.
RiskFactorsforOlderAdultsØVision-related changes• Cataract,AMD,Glaucoma
ØCognitivechanges• Depression,dementia
ØPhysicalcondition• Increasedincidenceofdiabetes,stroke,heartdisease,arthritis,
ØMedications• Antidepressants,bloodpressure,benzodiazepines
VisionandDrivingEstimated that90%ofinputadriver receives isvisual1
ØVisual inputisusedtoguidecognitiveandmotorresponsesØSafedrivingdependsonaperson’sability tosensetheenvironment, analyzeand respondtosensorystimuli inatimely manner.
9/27/17
4
VisionandDrivingVisiontesting isrequired toobtain,andinmanycases,renew adriver’s license.
ØAll stateshavevisualacuityrequirements fordriving
ØVisionrequirements differ foreachstate.
StateRequirementsVision•Visualacuity– Bestcorrectedacuityofatleast20/60
•Visualfield- 110degrees(horizontal)
Physical•Seizures•Neurologicalconditions
VisionTermsVisualAcuity– clarity orsharpnessofvisionØEnablesustoseethingsclearlywhendriving
• See andreaddirectionalsignage
• Seeandrespondtotrafficandbrakelights• Readmetersondash
• Clearlyseeobjectsontheroad
9/27/17
5
VisionTermsVisualField– whatyouseeoftheworldwhenlooking inafixeddirectionØEnablesustobeawareofobjectsbothcentrallyandperipherallywhendriving
•Seeandrespondtomergingcars
•Locateandmakelanechanges•Awarenessofpedestrianscrossing
VisionTermsContrastSensitivity – ability todistinguishlowcontrastitemsØEnablesustorecognizeobjectsfromtheirbackground
•Enhances abilitytodriveinlowlightsituations
•Recognizesidewalksandcurbsfromstreet
•Identifyobjects/potholes instreet
VisionandCrashResearchVisualAcuity - early research focusedonacuityandcrash risk.ØCorrelationsfoundbetweendecreasedacuityandcompromised binocular vision(1976,1994)
ØDatasincehasbeenveryambiguouswithweakassociations.
ØMildacuitylossdoesnotappeartoelevatecrashrisk.
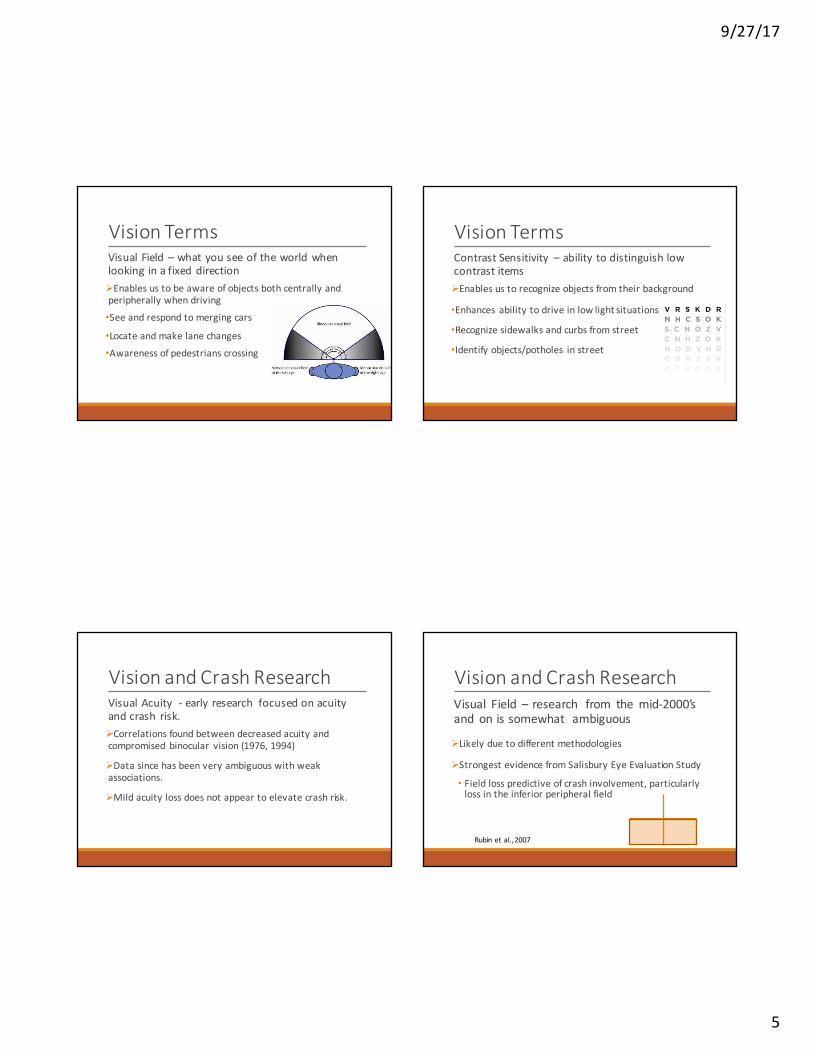
VisionandCrashResearchVisual Field – research from the mid-2000’sand onissomewhat ambiguous
ØLikelyduetodifferentmethodologies
ØStrongestevidencefromSalisburyEyeEvaluationStudy
• Fieldlosspredictiveofcrashinvolvement,particularlylossintheinferiorperipheralfield
Rubinetal. ,2007
9/27/17
6
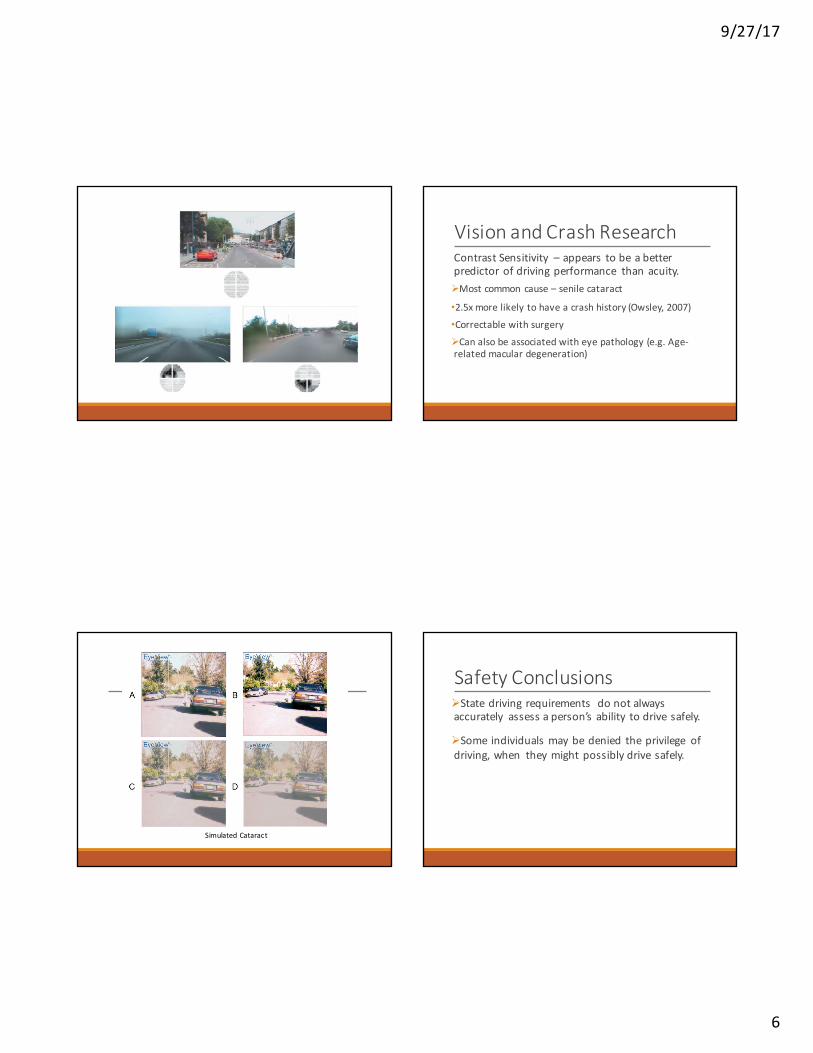
VisionandCrashResearchContrastSensitivity – appears tobeabetterpredictorofdrivingperformance thanacuity.ØMostcommon cause– senilecataract
•2.5xmorelikelytohaveacrashhistory(Owsley,2007)•CorrectablewithsurgeryØCanalsobeassociatedwitheyepathology(e.g.Age-relatedmaculardegeneration)
SimulatedCataract
SafetyConclusionsØStatedriving requirements donotalwaysaccurately assessaperson’sability todrivesafely.
ØSome individualsmaybedenied theprivilege ofdriving,when theymightpossiblydrivesafely.
9/27/17
7
LowVisionLowvisionisavisionlosssosevere,thatitcannotbefullycorrectedbyglassesorsurgery.ØVisualacuityis20/70orpoorerinthebetterseeing eye
•Means aperson with 20/70 vision who is20 feet fromeyechartcannotseewhataperson with unimpaired (20/20)vision cansee from70 feetaway
LowVision- FunctionallyLowvisionisuncorrectablevision lossthatinterferes witheveryday activities.
“Notenoughvisiontodowhatyouneed todo”• Varies fromperson toperson
LowVisionvs.LegalBlindness”LegalBlindness”– definitionestablishedbythegovernment asacutofftodetermine disabilitybenefits.
ØArbitrarynumber(20/200orlessinbetterseeingeyeoravisualfieldof20degreesorless)
CommonConditionsCausingLowVisioninOlderAdults
•Age-related macular degeneration (AMD)•Glaucoma•Diabetic Retinopathy•Stroke

9/27/17
8
AMDProblemwith the retina
•Macula isdamaged
•Losecentral vision,butperipheral visionremainsintact
•2types:
Dryandwet (DAMD,WAMD)
GlaucomaProblemwith theopticnerve•Usuallywhen fluidbuildsupinfrontoftheeye. Putspressureonopticnerve.•Loseperipheral vision,butcanprogress tocentral
•“Silent thief”oftengoesunnoticed
DiabeticRetinopathyProblemwithbloodvesselsofretina, associatedwithdiabetes•Highbloodsugarcausesdamage tobloodvessels,causingthem toleak, closeorgrowabnormally.•Canstealvisioncompletely
StrokeProblemwithvisualpathways inthebrain
•Symptomsdependonwhichpartofthebrainwasaffected.• Doublevision• Lightsensitivity• Hemianopsia
9/27/17
9
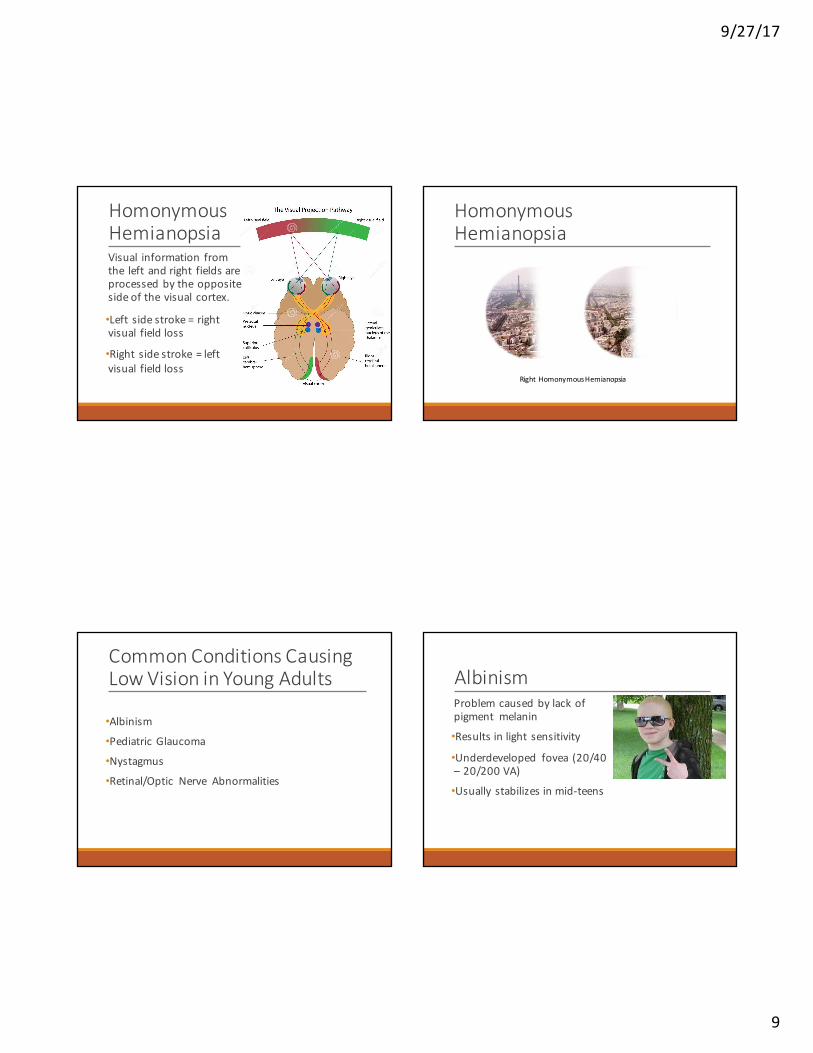
HomonymousHemianopsiaVisual information fromthe leftandright fieldsareprocessedbytheoppositesideofthevisual cortex.
•Left sidestroke= rightvisual fieldloss
•Right sidestroke=leftvisual fieldloss
HomonymousHemianopsia
RightHomonymousHemianopsia
CommonConditionsCausingLowVisioninYoungAdults
•Albinism•PediatricGlaucoma
•Nystagmus
•Retinal/Optic Nerve Abnormalities
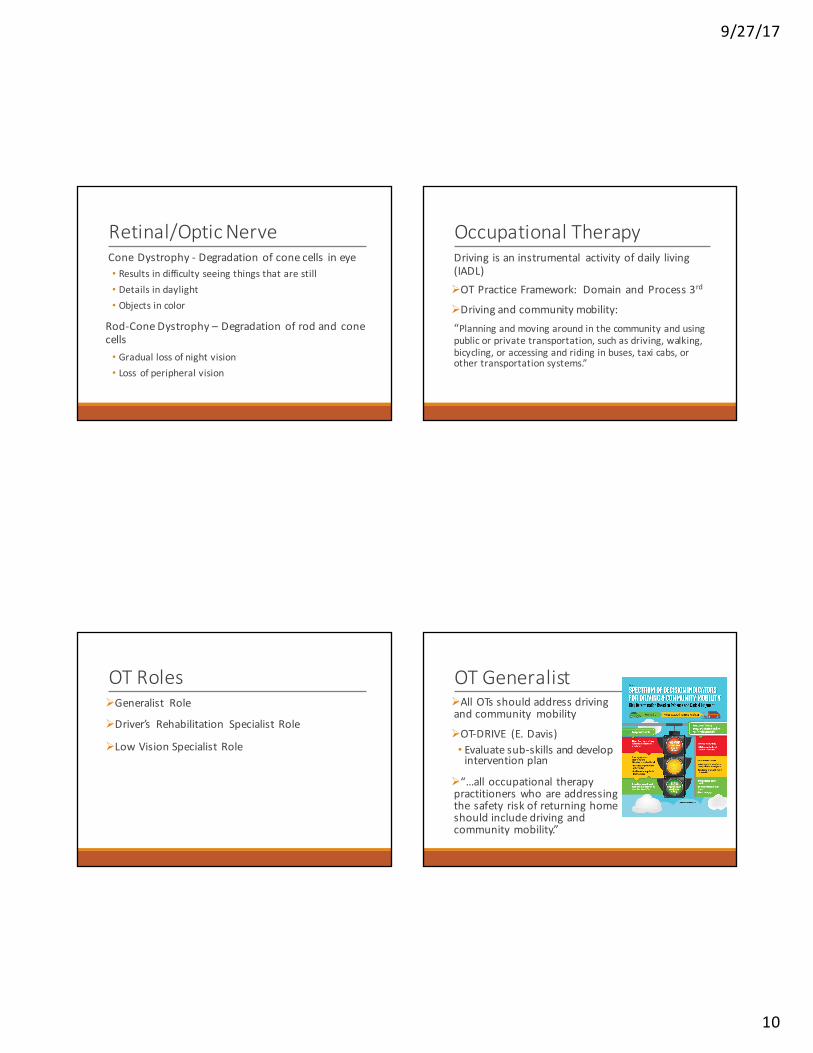
AlbinismProblemcausedbylackofpigment melanin
•Resultsinlight sensitivity
•Underdeveloped fovea (20/40– 20/200VA)
•Usually stabilizesinmid-teens
9/27/17
10
Retinal/OpticNerveConeDystrophy- Degradationofconecells ineye• Resultsindifficultyseeingthingsthatarestill• Detailsindaylight• Objectsincolor
Rod-ConeDystrophy– Degradationofrodandconecells• Graduallossofnightvision• Loss ofperipheralvision
OccupationalTherapyDriving isaninstrumental activityofdaily living(IADL)ØOTPracticeFramework: DomainandProcess3rd
ØDrivingandcommunitymobility:“Planningandmovingaroundinthecommunityandusingpublicorprivatetransportation,suchasdriving,walking,bicycling,oraccessingandridinginbuses,taxicabs,orothertransportationsystems.”
OTRolesØGeneralist Role
ØDriver’s Rehabilitation SpecialistRole
ØLowVisionSpecialistRole
OTGeneralistØAllOTsshouldaddressdrivingandcommunity mobility
ØOT-DRIVE (E.Davis)• Evaluatesub-skillsanddevelopinterventionplan
Ø“…alloccupational therapypractitionerswhoareaddressingthesafety riskofreturninghomeshouldincludedrivingandcommunitymobility.”

9/27/17
11
OTGeneralistØRefer toother team members asnecessaryØHaveknowledge ofanddevelop relationshipswithdriver rehabilitation specialists inthecommunityØKnowwhen torefer foracomprehensiveassessment
ØCounselondrivingcessationandtrainonalternative transportation
OTGeneralistEvaluationofSub-SkillsShouldbecompleted aspartofoccupationalperformanceassessment• Drivinghistory• Accidentsornearmisses• Whatkindofcardotheydrive• Useofalternativetransportation• Self-restriction• Wheredoyoudrive?
OTGeneralistEvaluationofSub-SkillsAdditionalassessmentshouldbecompleted dependingondiagnosisorcomplaints•Vision-related dxordecrease infunctionalperformance thatcouldbevisionrelated LeaNumbersLowContrastTest
OTGeneralistIntervention Planning•Client-centered goals that address drivingsub-skills
•Consider alternative transportation•Consider referral tolow vision specialist, ifappropriate•Consider driving cessation

9/27/17
12
DrivingCessation•Typicallya lastresort•Knowstate rules regarding reporting• Alabamamayactiftheyperceivethepersonisunsafe(denyinglicenseorrestricting)• Alicenseddoctorrequestthedriverberetestedorhavelicenserevoked.
•Beready toassistinfindingalternativetransportation.The inability todrivecanlimitoccupationalperformance.
DriverRehabilitationSpecialistHasspecialized trainingbeyondOTschool,includingcertification (CDRS).ØDetermineifapersonisatriskorcancontinuetodrivesafely
ØCompletesacomprehensive drivingevaluation• Step1:Verifypersonmeetsstaterequirements• Step2:Clinicalevaluation• Step3:On-roadevaluation
DriverRehabilitationSpecialistClinicEvaluation•Priortoon-roadevaluation
•Gathermedical/socialhistory•Determinelevelofpre-requisiteskills•Determineneedforadaptiveequipment
•Lookforredflags• Sensory/cognitive function
•Gatherinformationfromfamily
DriverRehabilitationSpecialistOn-RoadEvaluation•Completedininstructor’svehicle
•Essentialtodeterminefunctionalimpactof visiondeficitsandabilitytouseadaptiveequipmentoradaptivestrategies
•Applicationofcognitivestrategiesbehindthewheel:• Decisionmaking• Routeplanning• Judgment

9/27/17
13
LowVisionSpecialistOccupationalTherapist workswithclientbyreferral(typicallyophthalmologistoroptometrist) todevelopaplanofcare thataddressesclientgoals.
ØOftenassessmentofperformance skillsfordriving
ØTraining intheuseofadaptive equipment
Mayormaynothavespecialty certification (SCLV)
LowVisionSpecialistClinicalevaluation typically includes:•Medical/social history•Motorskills• Cognitive function• Sensory function• Acuity,fields,contrast,color(ifnotprovidedbyreferringphysician)
• Functionalmobility status
LowVisionSpecialistDynavision•Simulates visualfield
•Allowsobjects tobedisplayedinperiphery toassessreactiontime.
•Canincludedistractorstosimulatedividedattentiontasks.
•Usedtoteach visualscanning
LowVisionSpecialistUsefulFieldofView (UFOV)•Computer-basedassessmentofprocessingspeedandattention
•Considerable research tosupportscoresbelowanidentified threshold increasescrashrisk.
9/27/17
14
LowVisionSpecialistTrails MakingTestA&B
•Neuropsychological testofvisualattentionandtaskswitching.
•Providesinfoonvisual searchspeed, scanning,andexecutivefunction
LowVisionSpecialistSaintLouisUniversityMentalStatus(SLUMS)•Brieforal/written screening tool•Fordetecting mildcognitiveimpairment anddementia
•Memory-lossoftenfirstpresentswithdecreased way-finding.
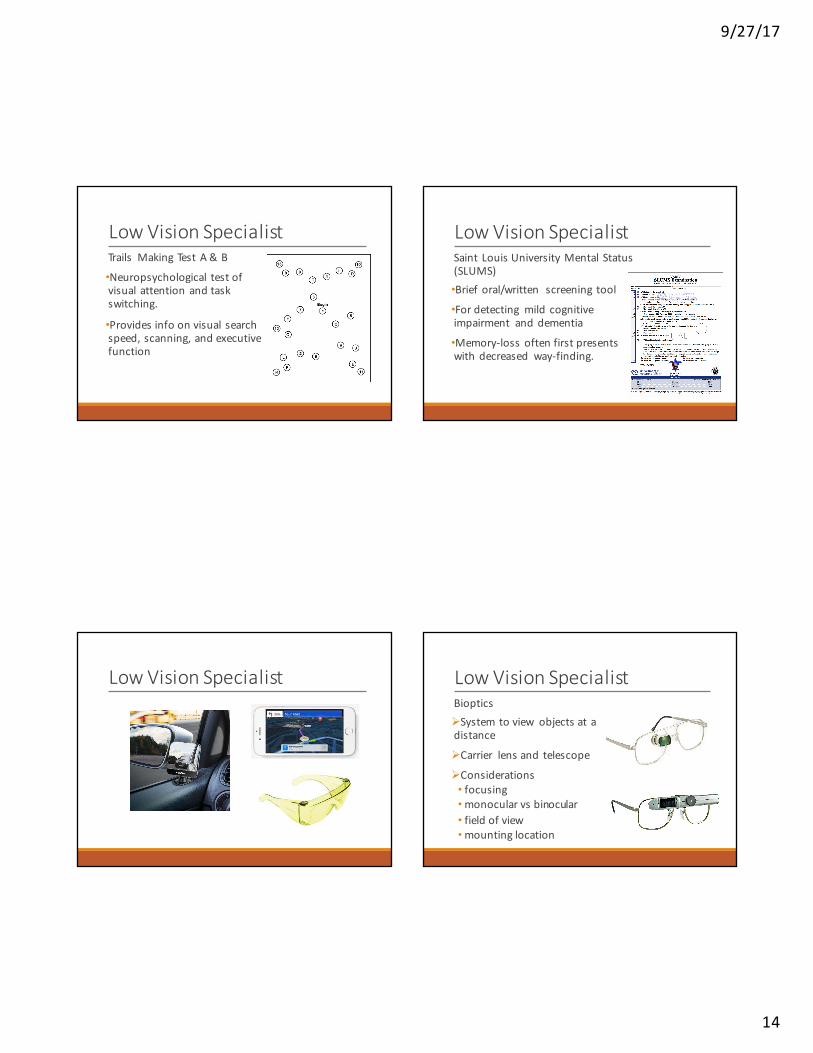
LowVisionSpecialist LowVisionSpecialistBiopticsØSystemtoview objectsatadistance
ØCarrier lensand telescope
ØConsiderations• focusing•monocularvsbinocular• fieldofview•mountinglocation

9/27/17
15
1. Interstatesignagetonormalviewer
2. ViewthroughGalileanbioptic(simulated)
3. ViewthroughKeplerianbioptic(simulated)
Bioptics StepsforBiopticDriving1. Individualisdeterminedbyanophthalmologistor
optometrist tomeet visionrequirements ofstate• Alabama this mustbeat least20/60 orbetterusing bioptic• 110degree field ofview
2. Individualisfittedforpreferred/appropriate device• Precise eyemeasurements takenbyoptometrist
3. Device isorderedandadjustedforproper fitwhen dispensed
4. Trainingbyanoccupationaltherapist toensure accuratetechniquesandspeed forspottingwithdevice
5. Around30hoursofon-roadtrainingwithCDRSbeforetakingdrivingexam
LowVisionSpecialistØProvidessoundclinical judgement onphysical,sensoryandcognitiveappropriateness forreturn todriving.
ØALWAYS refer toadriving rehabspecialist toassesstheclient functionallybehind thewheel!
WhentoRefer•Clienthasaknowndiagnosis thatcouldimpactdriving•Client ishaving repeated accidentswhile drivingorperforming functionalmobility•Counselclientnottodriveuntil referred forevaluation (visiondoctor)
•Pre-driver screen, suchasOT-DRIVE orOT-DORA

9/27/17
16
HowtoRefer•Bestpractice istoreferdirectly to lowvisiondoctor(ophthalmologist/optometrist)
•Canaskphysiciantoreferdirectly tolowvisionOTwithcertaindefinitive diagnoses• Example- homonymous hemianopsia
•Clientcannotbe receiving other formsofOTconcurrently foroutpatient services
LocationsUABCenterforLowVision
Rehabilitation
•Birmingham,AL
•LowvisionoptometristandOT
•DawnDeCarlo,OD–ClinicDirector
•(205)488-0736
•(205)488-0746(fax)
CommunityServicesforVisionRehabilitation
•Mobile,AL
•MD,optometrist,OT
•JoeFontenot,MD–MedicalDirector
•(251)476-4744
•(251)476-4741
Questions
Recommended