New insights into Research and Evidence on how Investments in PMTCT and Paediatric AIDS have
contributed to Health Systems Strengthening
Rene Ekpini ESenior Adviser
UNICEF, New York
Pre-conference meeting of Health Systems Experts, HIV Researchers and Implementers
Cape Town, South Africa, 17-18 July 2009

PMTCT, best model of combination prevention and treatment
acceleration
Primary preventionPrimary
prevention
Prevention of HIV
transmission from an
HIV-infected woman to her
infant
Prevention of HIV
transmission from an
HIV-infected woman to her
infant
Care, support and treatment
for HIV-infected women,
their infants and their families
Care, support and treatment
for HIV-infected women,
their infants and their families
Prevention of unintended pregnancies
among HIV-infected
women
Prevention of unintended pregnancies
among HIV-infected
women Individuals,
families and
communities
Individuals, families
and communities

3
PMTCT and paediatric HIV care, support and treatment: an opportunity
to improve MNCH services
PMTCT and paediatric HIV care, support and treatment: an opportunity
to improve MNCH services
Reaching MDGs 4,5 and 6 requires a paradigm shift
from the rhetoric of “the good, the bad and the ugly” toward the
prospect of using scaling up of PMTCT and paediatric
HIV care, support and treatment as an opportunity
to improve maternal and child health and survival
Reaching MDGs 4,5 and 6 requires a paradigm shift
from the rhetoric of “the good, the bad and the ugly” toward the
prospect of using scaling up of PMTCT and paediatric
HIV care, support and treatment as an opportunity
to improve maternal and child health and survival Maternity of
InongoMaternity of Inongo

0 20,0
00
40,0
00
60,0
00
80,0
00
100,0
00
120,0
00
140,0
00
160,0
00
Botswana
Mozambique
Haiti
Cote d'Ivoire
Rwanda
PMTCT Total prevention Care & Treatment
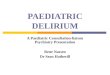
Expenditure in Care and treatment, Prevention and PMTCT in selected
countries
Source: UNAIDS 2008 Global Report
Source: UNAIDS 2008 Global Report

Building up PMTCT on weak health systems in resource-limited settings
9196
6874
60.5
43.4
0
20
40
60
80
100
120
Malawi Zambia
1+ visit 4+ visits Births with skilled attendant
Sources: 1- ANC coverage: Antenatal care in developing countries-Promise, achievements and missed opportunities – An analysis of trends, level and differentials, 1990-2001 updates 2- Skilled attendant at birth 2006
Coverage of antenatal care and skilled attendant at birth
50
65
32
47
1721
1216
0
10
20
30
40
50
60
70
Malawi Zambia
HIV T&C ARV for PMTCTInfant ARV for PMTCT CTP for infant by 2 months
Coverage of PMTCT services

From proof of principles to implementation at large scale
• Expansion of quality antenatal and delivery care
• Expansion of provider initiated HIV testing and counselling in antenatal, delivery and child health care settings
• Scaling up more efficacious ARV regimens for PMTCT, including building capacity for CD4 cell count and ART for pregnant women
• Cotrimoxazole prophylaxis for HIV-infected pregnant women, HIV-infected mothers and their infants as a standard of care

From proof of principles to implementation at large scale
• Scaling up early infant diagnosis and ART for infants
• Scaling up innovations to service delivery, including use mobile phone technology to expand EID and ART for infants
• Strengthening national M&E systems

8
2.2
25 25
19.5
17.2
0
5
10
15
20
25
30
Sd-NVP AZT/ Sd-NVP
tra
nsm
issi
on
ra
te (
%)
In PMTCT programme Outside PMTCT pg All
Current system performance (KZN province)
Attend ANC clinic 92%
Counseled and tested for HIV, CD4 75%
Get ARVs (pre- and perinatal) 50%
Adapted from Pierre Baker & Nigel RollinsAdapted from Pierre Baker & Nigel Rollins

8
2.2
25 25
11.1
6.1
0
5
10
15
20
25
30
Sd-NVP AZT/ Sd-NVP
tra
nsm
issi
on
ra
te (
%)
In PMTCT programme Outside PMTCT pg All
95% efficiency of the system (KZN province)
Attend ANC clinic 92%
Counseled and tested for HIV, CD4 95%
Get ARVs (pre- and perinatal) 95%

Six building blocks of health systems
• Strong leadership and governance
• Good health-financing system
• Responsive health care force
• Effective, safe, and high-quality health
services
• Equitable access to essential medical
products,
vaccines, and technologies
• Well-functioning health information system
• Strong leadership and governance
• Good health-financing system
• Responsive health care force
• Effective, safe, and high-quality health
services
• Equitable access to essential medical
products,
vaccines, and technologies
• Well-functioning health information system

How investments in PMTCT and paediatric AIDS have contributed to
health systems strengthening
How investments in PMTCT and paediatric AIDS have contributed to
health systems strengthening

Inducing improved governance and policy changes
• Strong political leadership and commitment to ensure that health system goals of access, equity, efficiency and improvement in outcomes are achieved
• Promotion of innovative policies on: - Provider initiated HIV testing and counselling
- access to treatment for women and children
- Abolition of user fees for antenatal and delivery care in some countries
• Revision of the content of the basic package of antenatal and postnatal care to integrate HIV-related services
• Induction of changes in resource allocation including innovative approaches such as performance-based financing

Strengthening programme management, coordination, and
monitoring and evaluation
• Harmonization and alignment of programmes (SRH, Nutrition, MNCH, HIV) and partners through integrated coordination bodies and mechanisms
• Revision/adaptation of national indicators in line with global guidelines, development of M&E tools, and human capacity building for data management, analysis and use
• Setting up mechanisms for information sharing and referrals, including notification of HIV information on child and maternal health cards
• Growing support to impact evaluation and operational research

Addressing shortage in human resources and improving working
conditions • Innovative approaches to addressing insufficient skilled human resources to sustain
expansion of services:
- Task shifting and sharing
- Engagement of PLWH
• Improvement of infrastructure and equipment, optimizing working conditions, and improve efficient delivery of services:
- Rehabilitation and equipment of ANC, delivery care, laboratory and pharmacy facilities
- Reorganization of service delivery mechanisms
• Engagement of civil society, PLWH, male partners and communities (lay counselors, peer support groups, Mother2Mother, post-test clubs)

0
10
20
30
40
50
60
70
80
90
nutritionduring
pregnancy
Familyplanning
Preventionof STIs
Measurefoetal
heart rate
Partographever filled
in
Checkuterine
retraction
Perc
enta
ge
Before PMTCT After PMTCT
Individual counsellingIndividual counselling
Quality of antenatal and delivery care before and after the implementation of
PMTCT; Cote d’Ivoire
Therese Delvaux et al.Therese Delvaux et al.

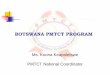
Impact of PMTCT on institutional deliveries in Rwanda – HIV-positive
women
69%
72%
80%
87%
89%
31%
28%
20%
13%
11%
0% 20% 40% 60% 80% 100%
2004 (N= 412)
2005 (N=499)
2006 (N=966)
2007 (N=1,053)
2008 (N=1,253)
At health facility Home
Bangendanye, L; Price, J.E.; Micomyiza E.; Shumbusho F.; Wesson Bangendanye, L; Price, J.E.; Micomyiza E.; Shumbusho F.; Wesson
In the general population 45% of women delivered at HF (IDHS 2007-08)
In the general population 45% of women delivered at HF (IDHS 2007-08)

25
30
35
21
28
35
12
23
32
34
37
24
28 27
24
21
2826
15
2019
17
2625
HIV-negative
HIV-positive
Proportion of married women age 15-49 with unmet need for contraception,
according to HIV serostatus, selected DHS surveys 2003-2007

The way forward The way forward

Closing the gaps toward virtual elimination of paediatric HIV
infection
1.Closing the funding gaps through resource mobilization and allocation and more efficient use of available resources
2.Closing the gap in access to the best available science for all by scaling up more efficacious ARV regimens for PMTCT, early diagnosis and ART for infants and children
3.Closing the gap in access and equity for the majority of women and children in need through decentralisation and scaling up of innovation to service delivery

Closing the gaps toward virtual elimination of paediatric HIV
infection
4. Closing the gap between health-based approach and communities through engagement of individuals, families and communities
5. Closing the gap with the future by building capacity and setting up appropriate fiscal policies and operational mechanisms to ensure sustainability
6. Closing the knowledge gap through promotion and support to impact evaluation and operational research to inform advocacy, policies and programming

Two Worlds, Two Realities One Hope
Two Worlds, Two Realities One Hope

Before
Rutobwe H.C. Maternity
After
Recommended