MOLECULAR GENETICS OF MYELOPROLIFERATIVE
DISORDERDSDr. A. Arun Kumar
Moderator: Dr. Mili Jain
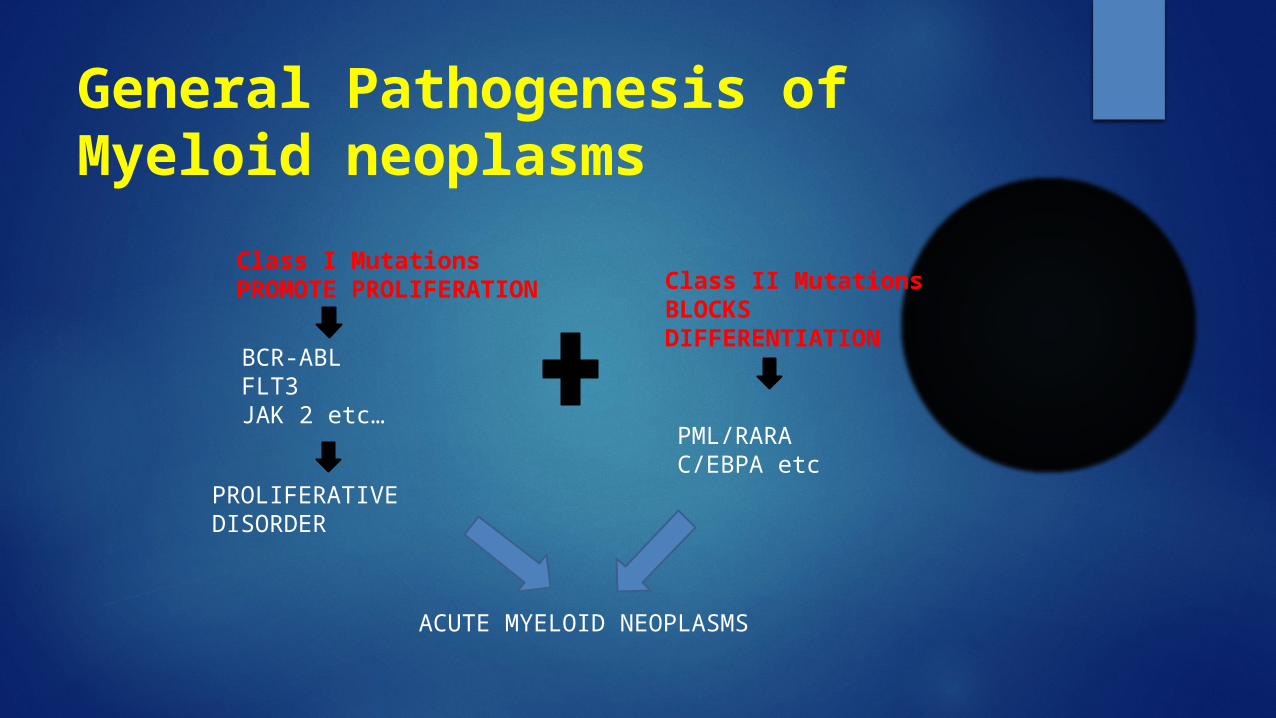
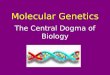
General Pathogenesis of Myeloid neoplasms
Class I MutationsPROMOTE PROLIFERATION Class II Mutations
BLOCKS DIFFERENTIATION
BCR-ABLFLT3JAK 2 etc…
PML/RARAC/EBPA etc
PROLIFERATIVE DISORDER
ACUTE MYELOID NEOPLASMS
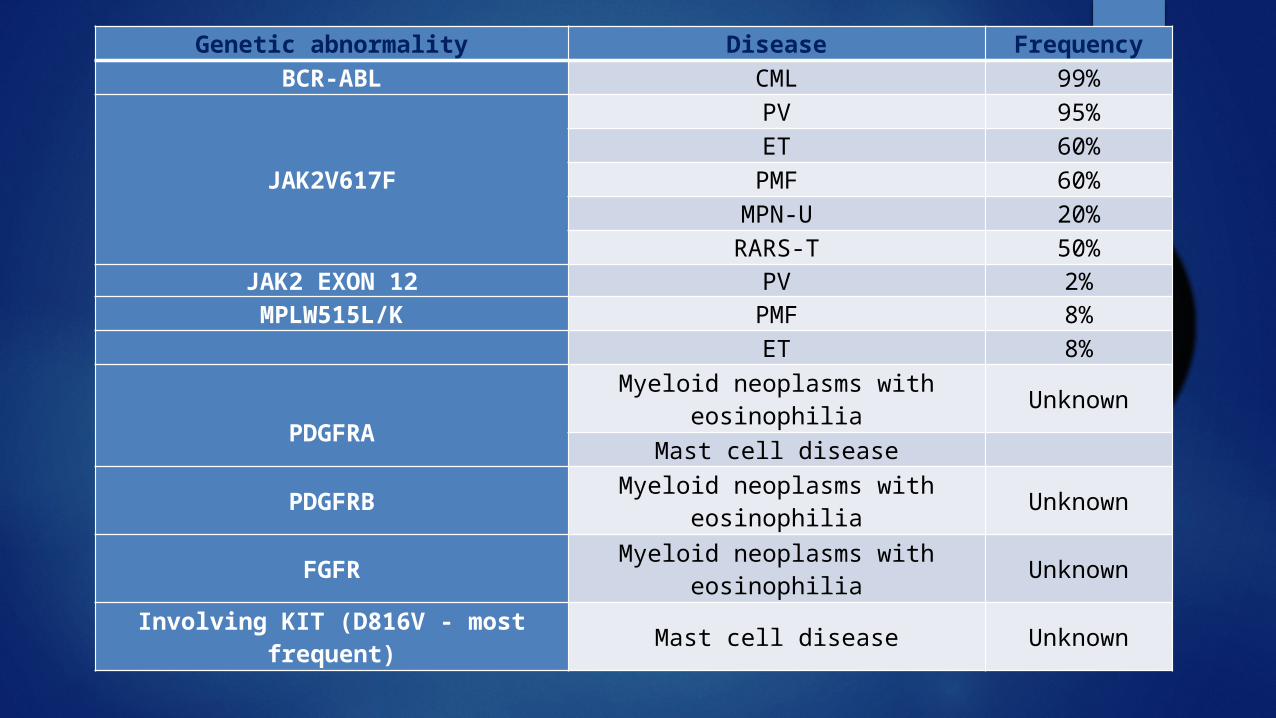
Genetic abnormality Disease FrequencyBCR-ABL CML 99%
JAK2V617F
PV 95%ET 60%
PMF 60%MPN-U 20%RARS-T 50%
JAK2 EXON 12 PV 2%MPLW515L/K PMF 8%
ET 8%
PDGFRA
Myeloid neoplasms with eosinophilia Unknown
Mast cell disease
PDGFRB Myeloid neoplasms with eosinophilia Unknown
FGFR Myeloid neoplasms with eosinophilia Unknown
Involving KIT (D816V - most frequent) Mast cell disease Unknown
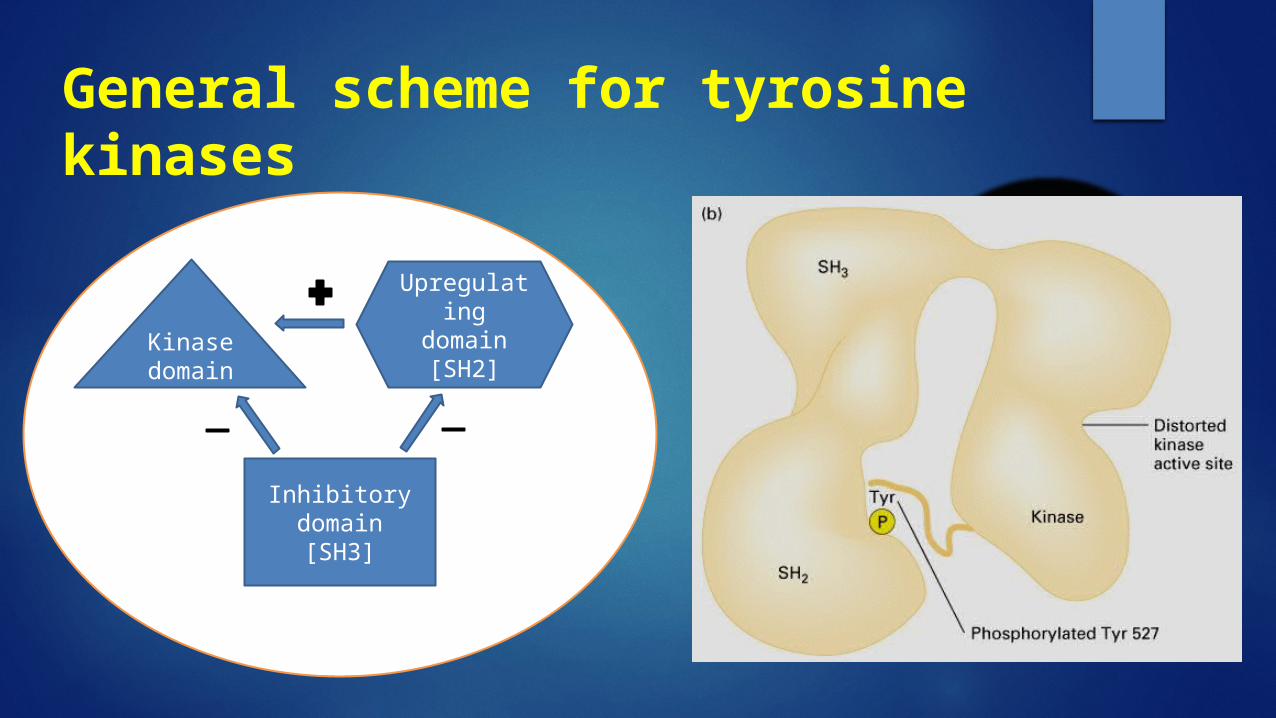
General scheme for tyrosine kinases
Kinase domain
Upregulating domain [SH2]
Inhibitory domain[SH3]
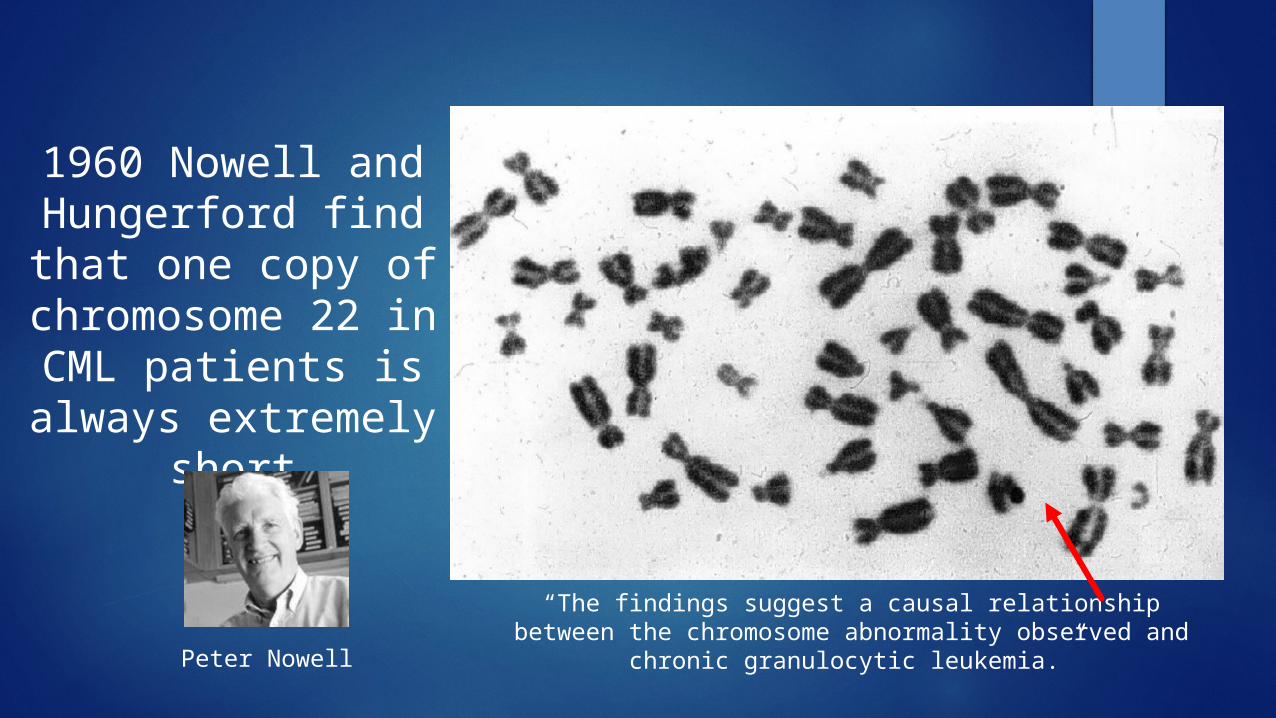
“The findings suggest a causal relationship between the chromosome abnormality observed and chronic granulocytic leukemia.”Peter Nowell
1960 Nowell and Hungerford find that
one copy of chromosome 22 in
CML patients is always extremely short
BCR-ABL
The Philadelphia chromosome - originally in Philadelphia.
The first genetic abnormality to be associated with a human cancer.
The result of a balanced translocation between chromosomes 9 and 22.
Derivative chromosome 22 is significantly smaller Ph chromosome is present in all hematopoietic lineage
cells from patients with CML. Ph chromosome is acquired and NOT inherited
through the germline.
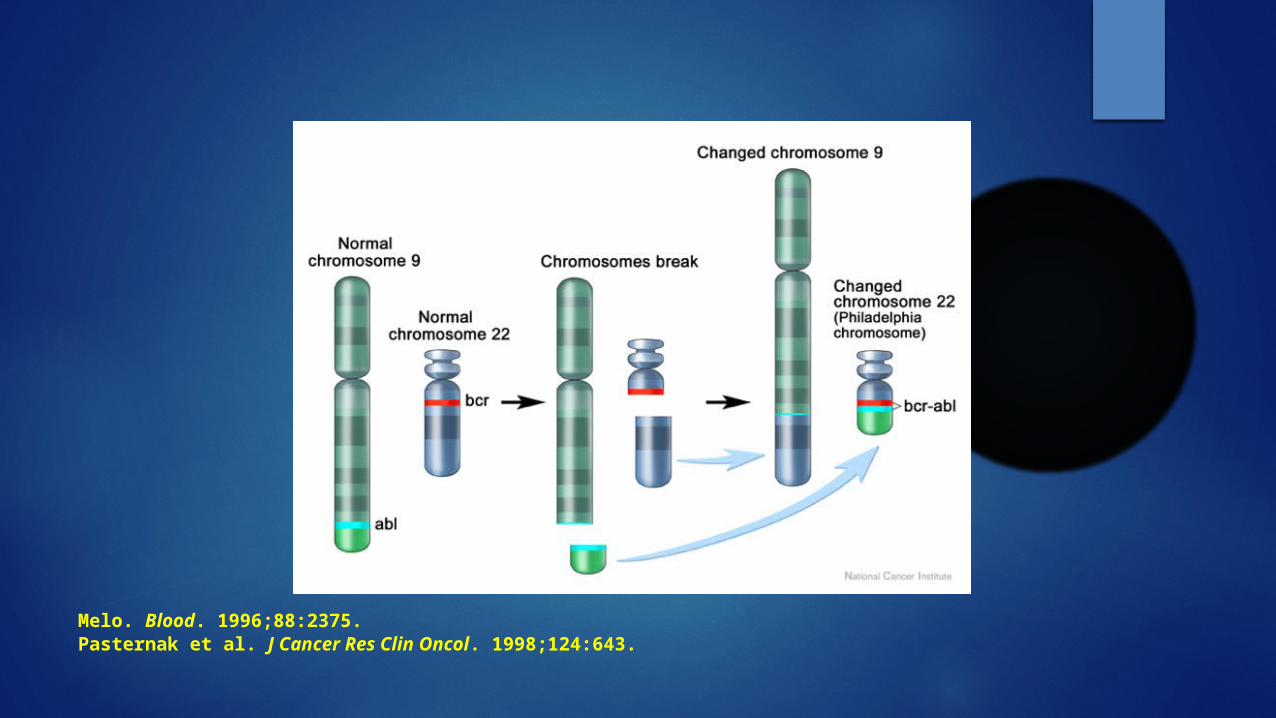
Melo. Blood. 1996;88:2375. Pasternak et al. J Cancer Res Clin Oncol. 1998;124:643.
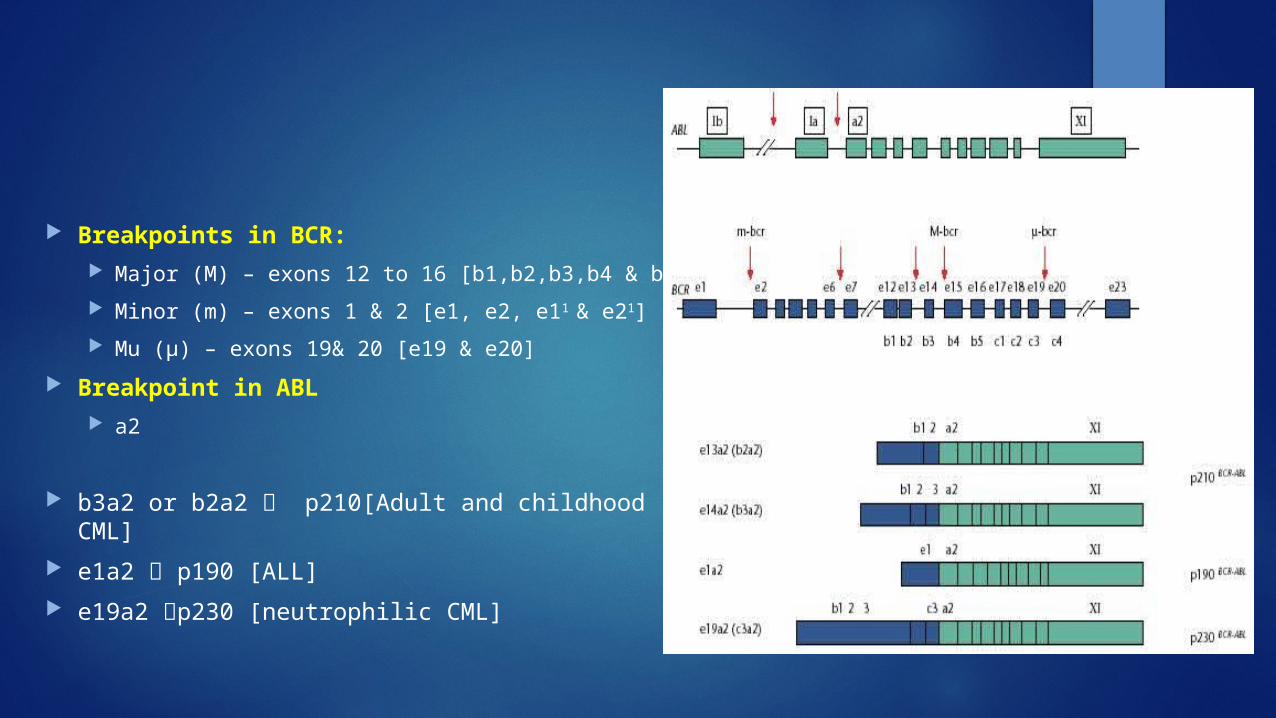
Breakpoints in BCR: Major (M) – exons 12 to 16 [b1,b2,b3,b4 & b5]
Minor (m) – exons 1 & 2 [e1, e2, e11 & e21]
Mu (μ) – exons 19& 20 [e19 & e20]
Breakpoint in ABL a2
b3a2 or b2a2 p210[Adult and childhood CML]
e1a2 p190 [ALL]
e19a2 p230 [neutrophilic CML]
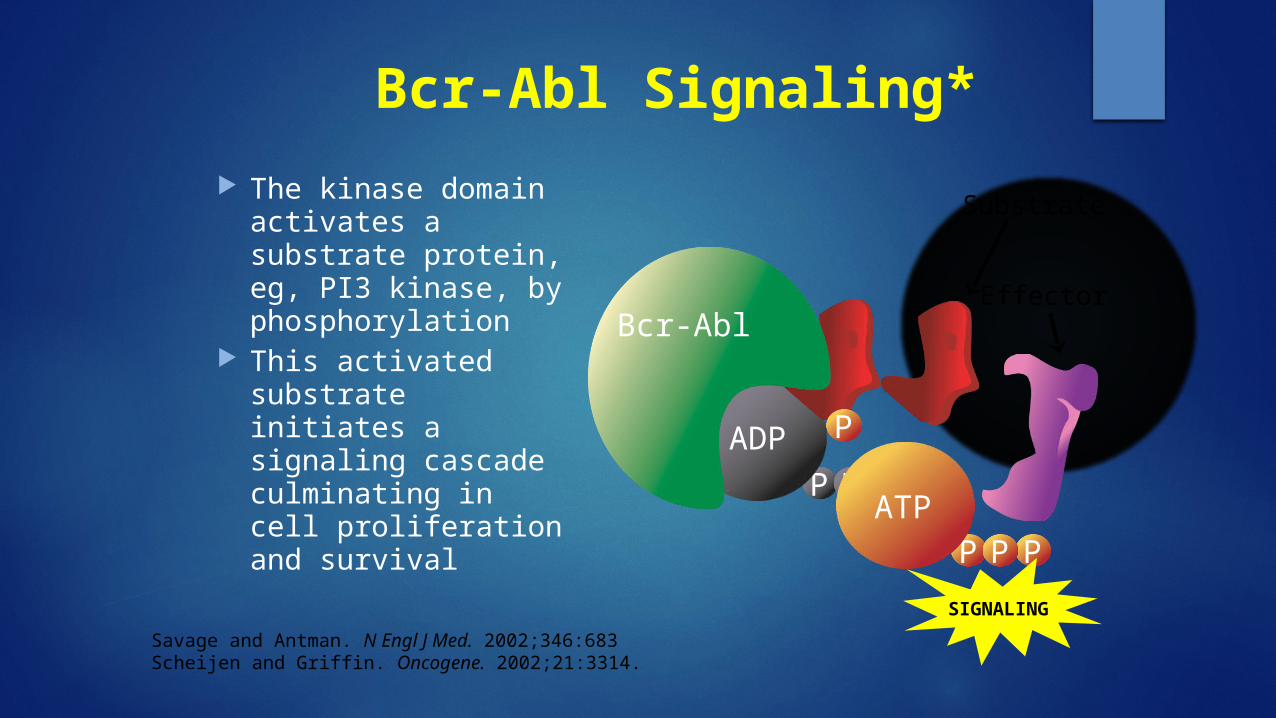
Bcr-Abl Signaling*
The kinase domain activates a substrate protein, eg, PI3 kinase, by phosphorylation
This activated substrate initiates a signaling cascade culminating in cell proliferation and survival
PP P
ADP P
P
PP PATP
SIGNALING
Bcr-Abl
Substrate
Effector
Savage and Antman. N Engl J Med. 2002;346:683Scheijen and Griffin. Oncogene. 2002;21:3314.
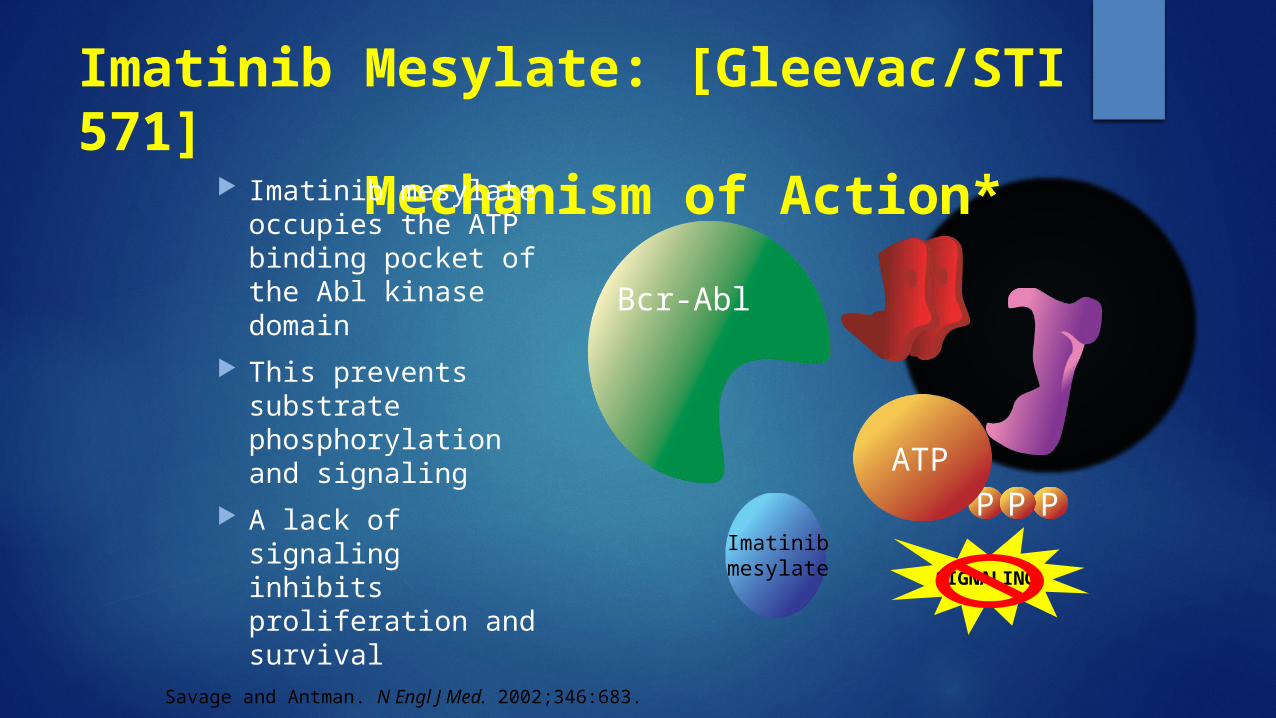
Imatinib Mesylate: [Gleevac/STI 571] Mechanism of Action* Imatinib mesylate
occupies the ATP binding pocket of the Abl kinase domain
This prevents substrate phosphorylation and signaling
A lack of signaling inhibits proliferation and survival
P
PP PATP
SIGNALING
Imatinib mesylate
Bcr-Abl
Savage and Antman. N Engl J Med. 2002;346:683.
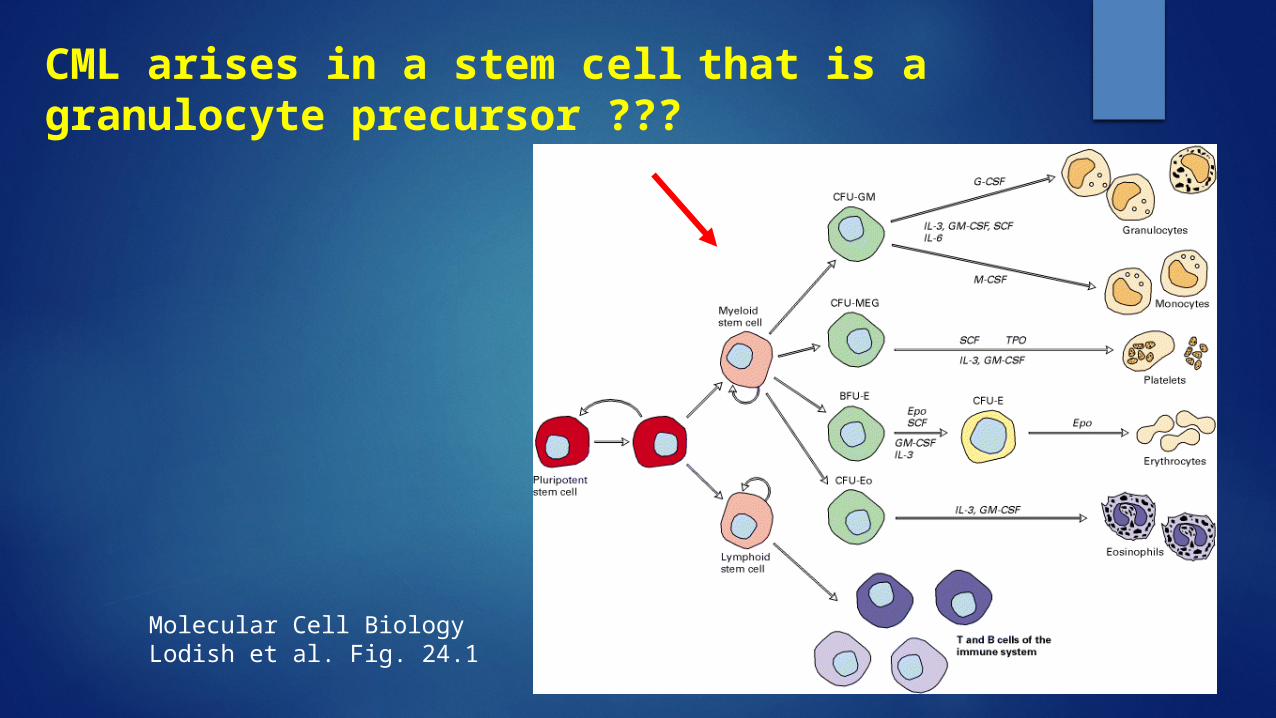
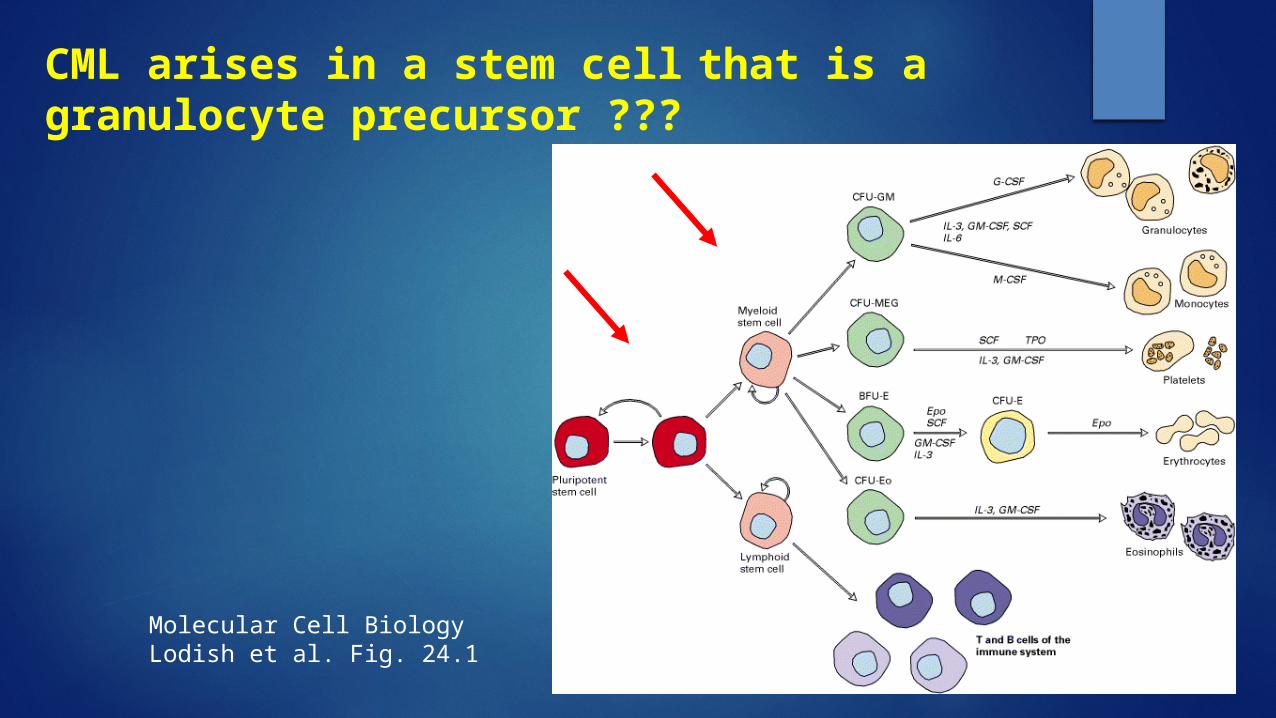
Molecular Cell BiologyLodish et al. Fig. 24.1
CML arises in a stem cell that is a granulocyte precursor ???
Leukaemogenesis
Ph chromosome is found on myeloid, monocytic, erythroid, megakaryocytic, B-cells and sometimes T-cells
Molecular Cell BiologyLodish et al. Fig. 24.1
CML arises in a stem cell that is a granulocyte precursor ???
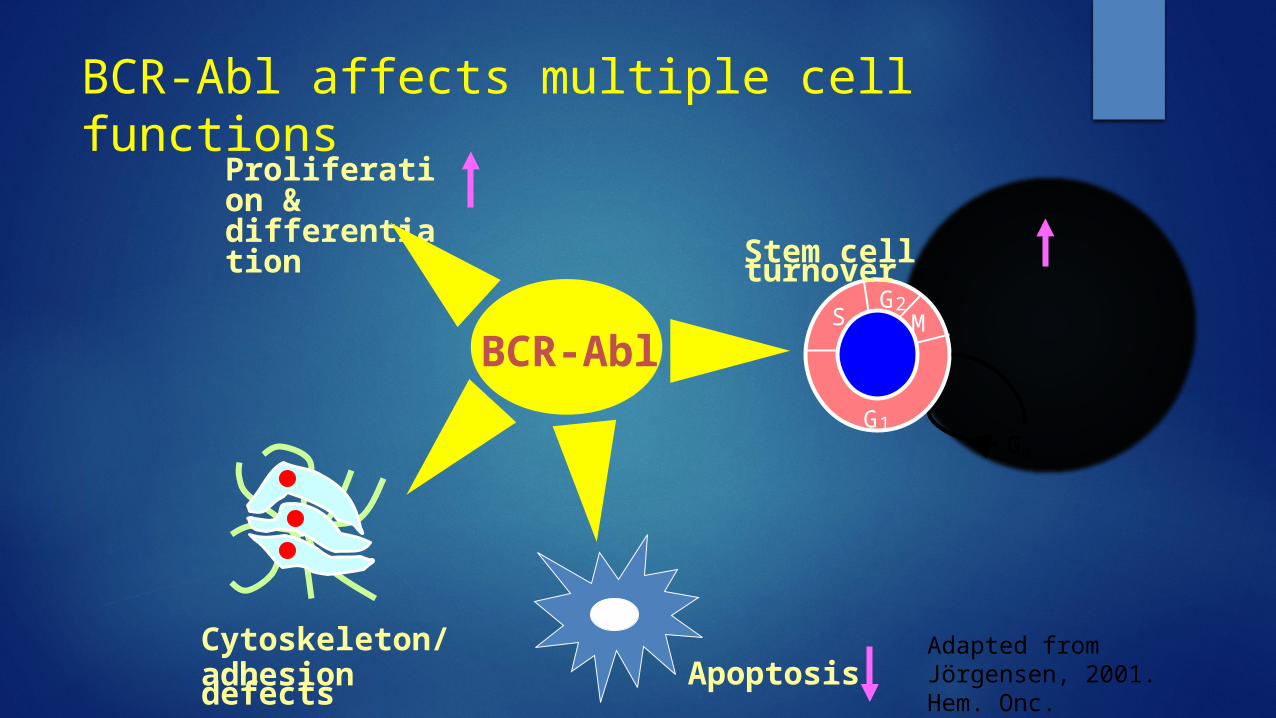
BCR-Abl
Cytoskeleton/adhesion defects
SG2
M
1GG0
Apoptosis
Stem cell turnover
Proliferation & differentiation
BCR-Abl affects multiple cell functions
Adapted from Jörgensen, 2001. Hem. Onc.
Diagnosing Chronic Myeloid Leukemia
DEMONSTRATION OF PHILADELPHIA CHROMOSOME
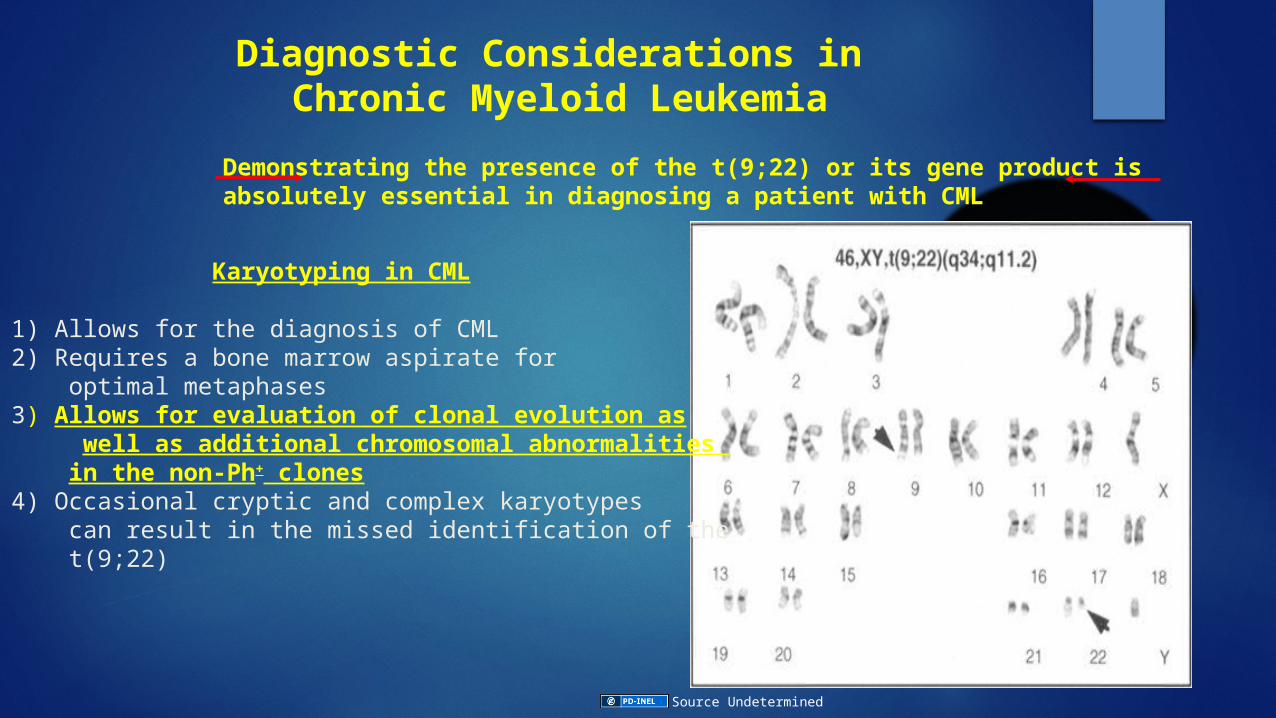
Diagnostic Considerations in Chronic Myeloid Leukemia
Karyotyping in CML
1) Allows for the diagnosis of CML2) Requires a bone marrow aspirate for optimal metaphases3) Allows for evaluation of clonal evolution as well as additional chromosomal abnormalities in the non-Ph+ clones4) Occasional cryptic and complex karyotypes can result in the missed identification of the t(9;22)
Demonstrating the presence of the t(9;22) or its gene product is absolutely essential in diagnosing a patient with CML
Source Undetermined
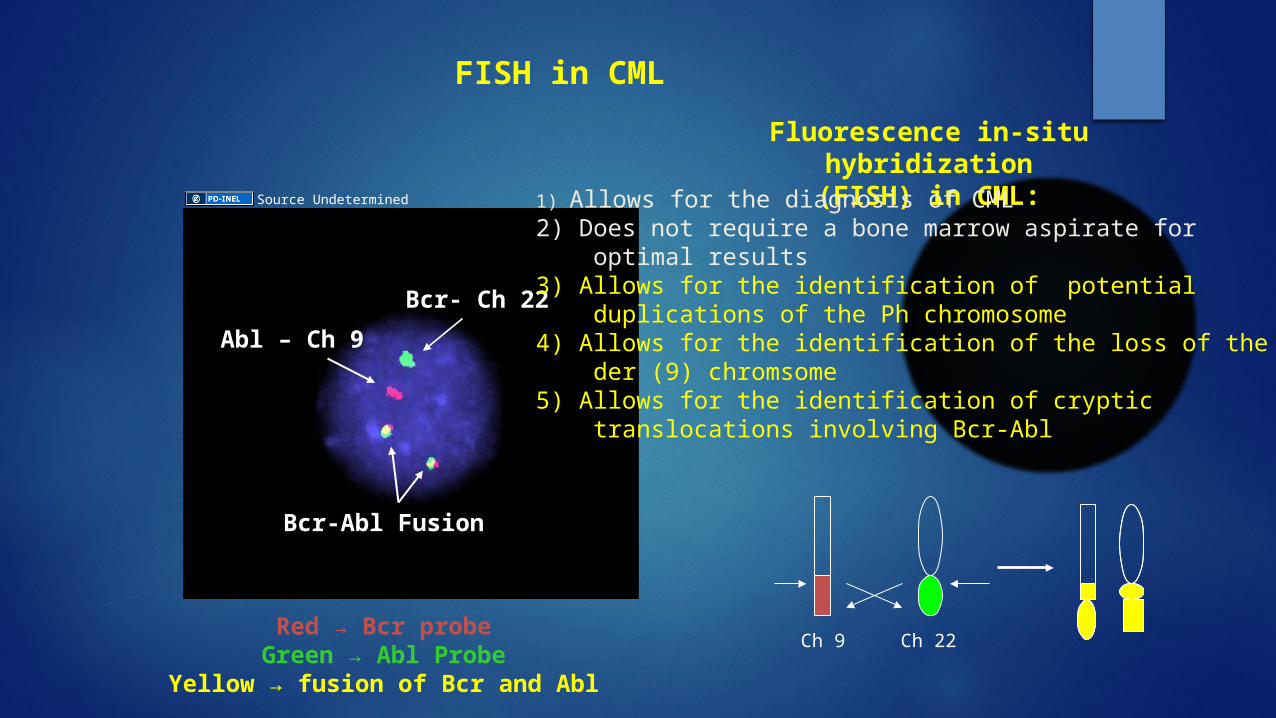
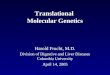
FISH in CML
Red → Bcr probeGreen → Abl Probe
Yellow → fusion of Bcr and Abl
Ch 9 Ch 22
Bcr- Ch 22
Abl – Ch 9
Bcr-Abl Fusion
Source Undetermined
Fluorescence in-situ hybridization(FISH) in CML:
1) Allows for the diagnosis of CML2) Does not require a bone marrow aspirate for optimal results3) Allows for the identification of potential duplications of the Ph chromosome 4) Allows for the identification of the loss of the der (9) chromsome5) Allows for the identification of cryptic translocations involving Bcr-Abl
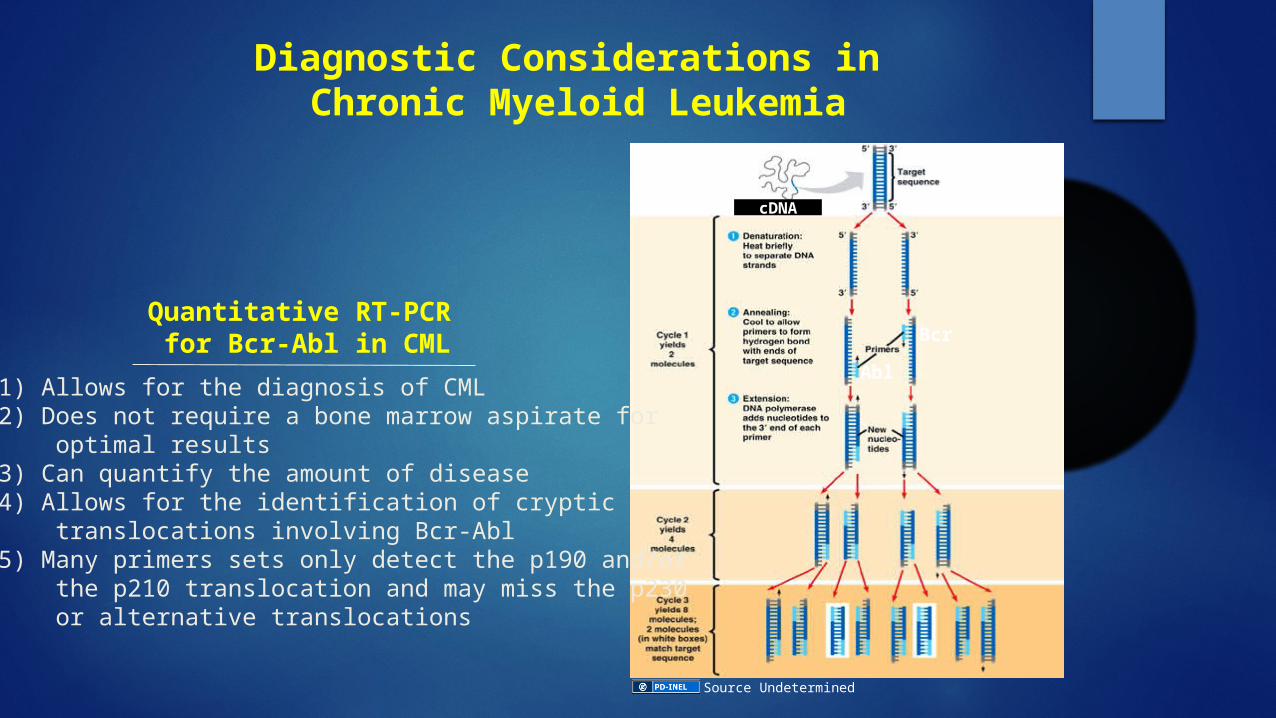
Diagnostic Considerations in Chronic Myeloid Leukemia
Bcr-Abl
Bcr
Abl
cDNA
Quantitative RT-PCR for Bcr-Abl in CML
1) Allows for the diagnosis of CML2) Does not require a bone marrow aspirate for optimal results3) Can quantify the amount of disease4) Allows for the identification of cryptic translocations involving Bcr-Abl5) Many primers sets only detect the p190 and/or the p210 translocation and may miss the p230 or alternative translocations
Source Undetermined
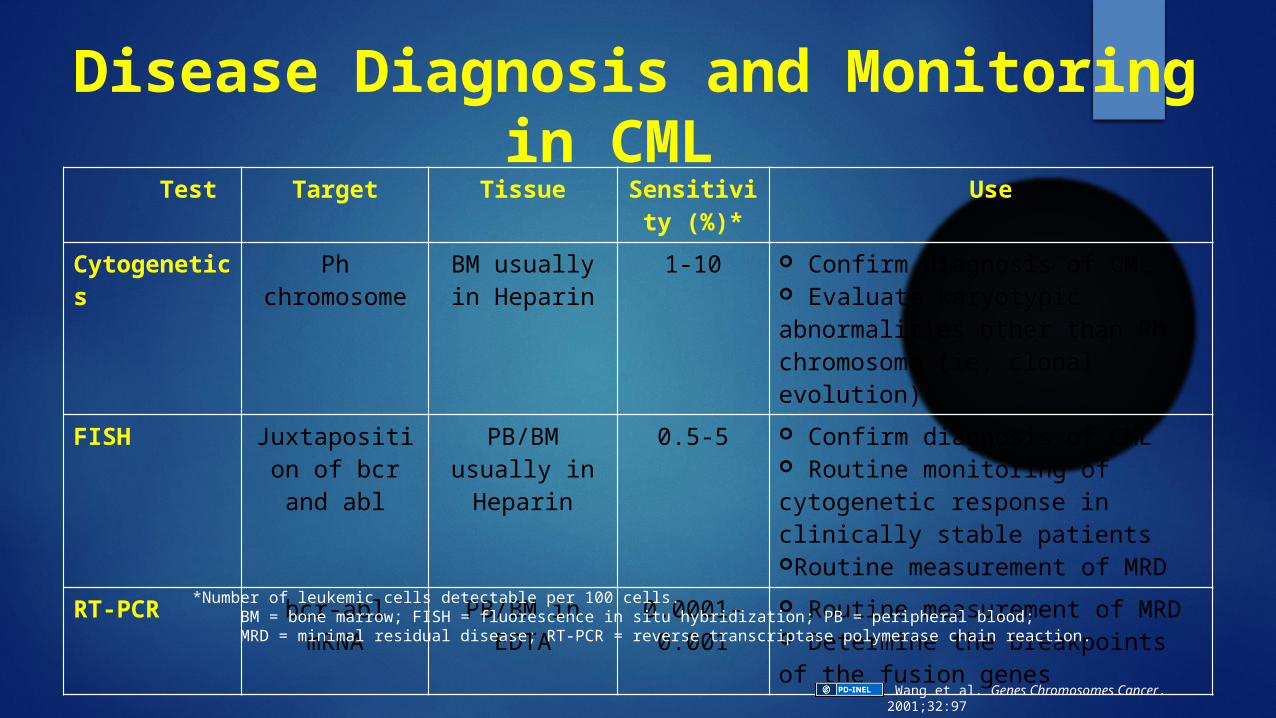
Disease Diagnosis and Monitoring in CML
Test Target Tissue Sensitivity (%)*
Use
Cytogenetics Ph chromosome BM usually in Heparin
1-10 Confirm diagnosis of CML Evaluate karyotypic abnormalities other than Ph chromosome (ie, clonal evolution)
FISH Juxtaposition of bcr and abl
PB/BM usually in Heparin
0.5-5 Confirm diagnosis of CML Routine monitoring of cytogenetic response in clinically stable patientsRoutine measurement of MRD
RT-PCR bcr-abl mRNA PB/BM in EDTA 0.0001-0.001
Routine measurement of MRD Determine the breakpoints of the fusion genes
*Number of leukemic cells detectable per 100 cells.BM = bone marrow; FISH = fluorescence in situ hybridization; PB = peripheral blood;MRD = minimal residual disease; RT-PCR = reverse transcriptase polymerase chain reaction.
Wang et al. Genes Chromosomes Cancer. 2001;32:97
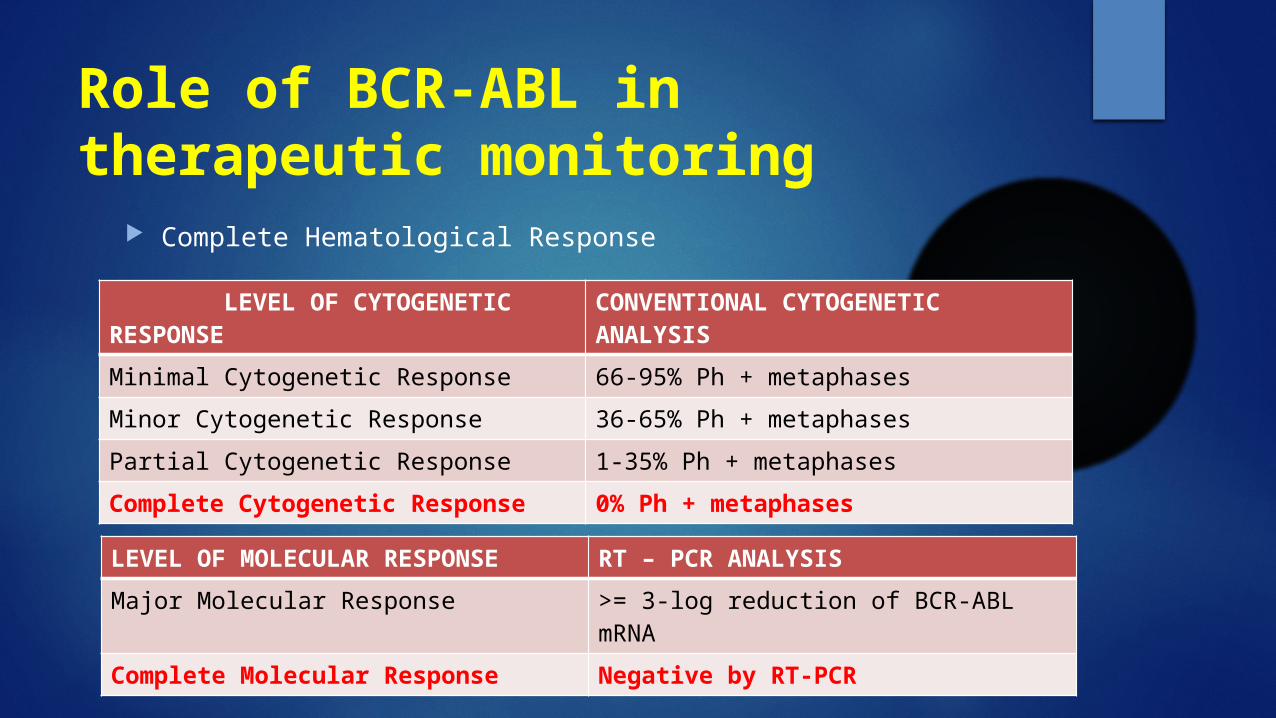
Role of BCR-ABL in therapeutic monitoring
Complete Hematological Response
LEVEL OF CYTOGENETIC RESPONSE CONVENTIONAL CYTOGENETIC ANALYSIS
Minimal Cytogenetic Response 66-95% Ph + metaphases
Minor Cytogenetic Response 36-65% Ph + metaphases
Partial Cytogenetic Response 1-35% Ph + metaphases
Complete Cytogenetic Response 0% Ph + metaphases
LEVEL OF MOLECULAR RESPONSE RT – PCR ANALYSIS
Major Molecular Response >= 3-log reduction of BCR-ABL mRNA
Complete Molecular Response Negative by RT-PCR
Therapeutic significance of BCR-ABL
Imatinib – selective Abl specific tyrosine kinase inhibitor. Binds to only the inactive conformation of Abl kinase domain
Nilotinib – selective abl inhibitor. Binds to only the inactive conformation of Abl kinase domain
Dasatinib – Src/ABL inhibitor. Binds to both active and inactive conformation of Abl kinase domain
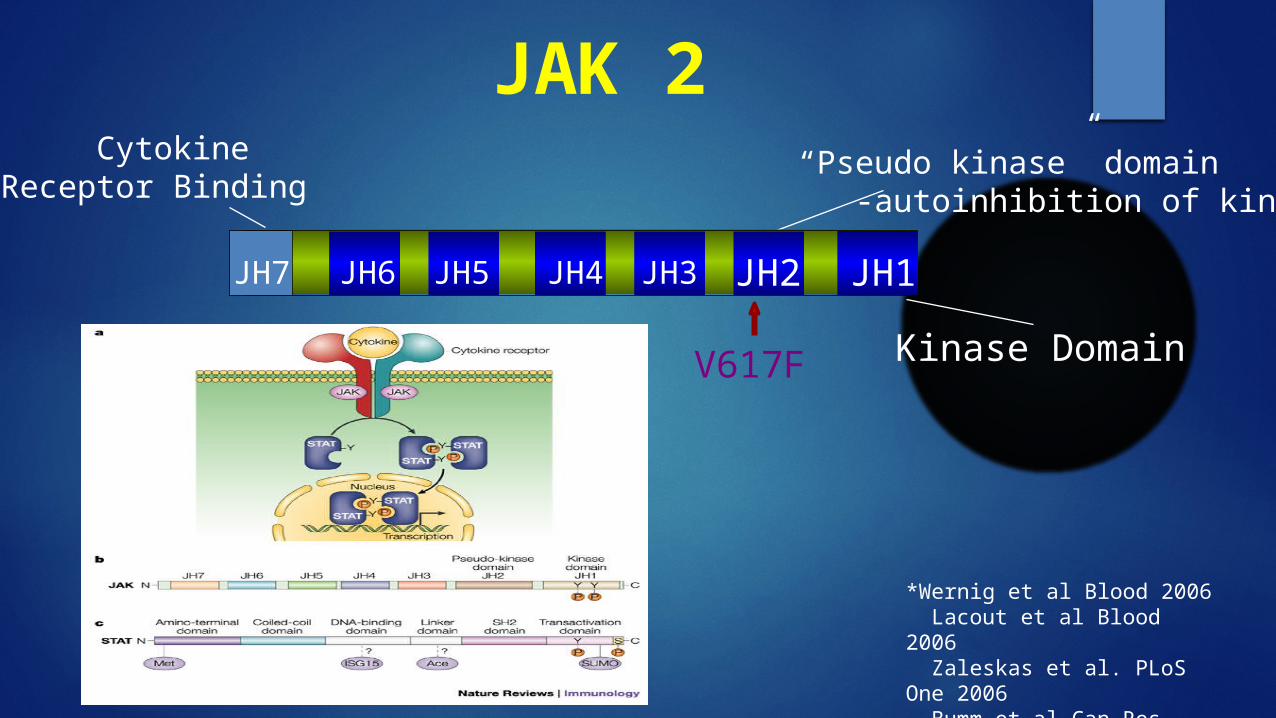
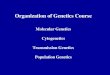
“Pseudo kinase” domain -autoinhibition of kinase
JAK 2
V617F
CytokineReceptor Binding
Kinase Domain
JH1JH2JH3JH4JH5JH6JH7
*Wernig et al Blood 2006 Lacout et al Blood 2006 Zaleskas et al. PLoS One 2006 Bumm et al Can Res 2006
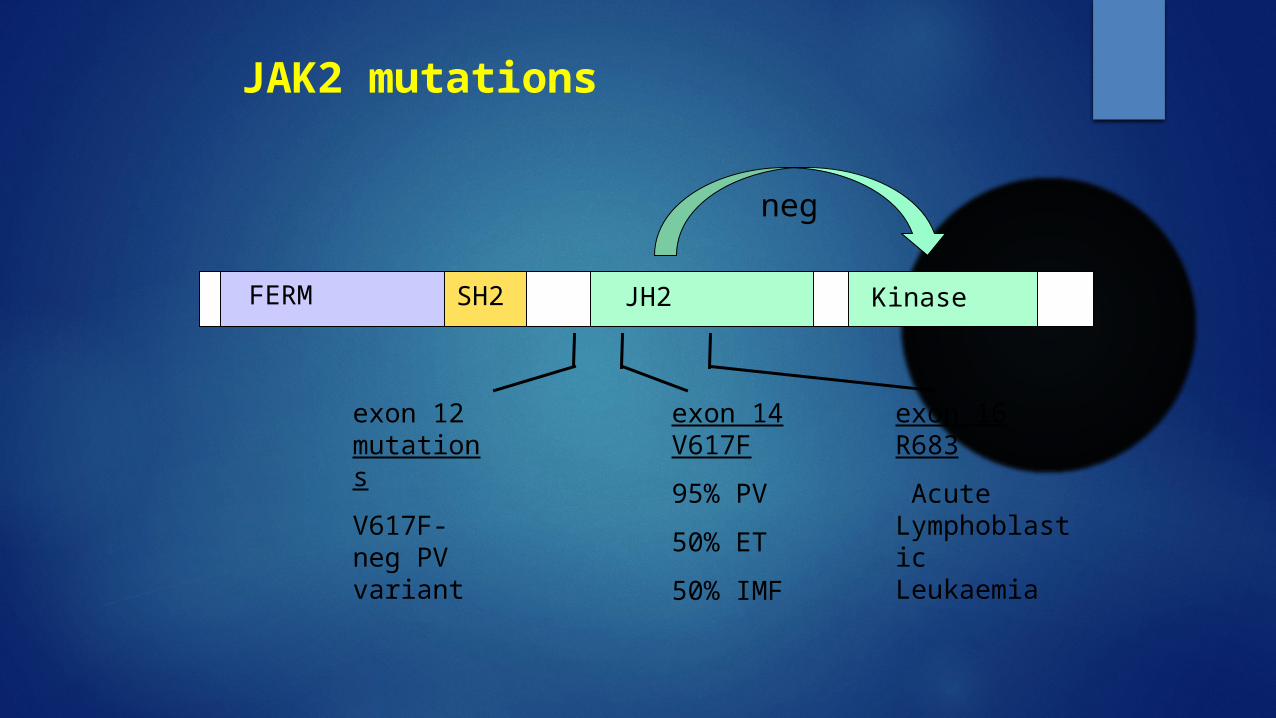
JAK2 mutations
FERM SH2 JH2 Kinase
exon 14 V617F
95% PV
50% ET
50% IMF
neg
exon 12 mutations
V617F-neg PV variant
exon 16 R683
Acute Lymphoblastic Leukaemia
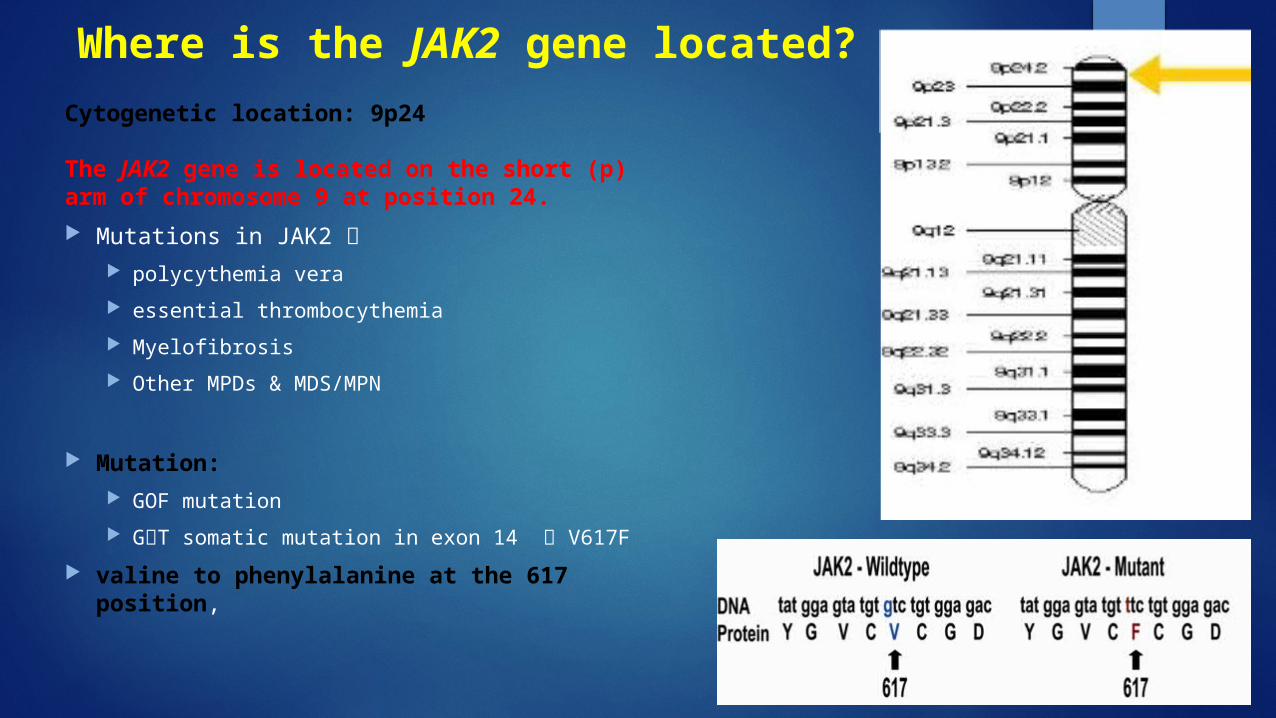
Where is the JAK2 gene located?
Cytogenetic location: 9p24
The JAK2 gene is located on the short (p) arm of chromosome 9 at position 24.
Mutations in JAK2
polycythemia vera
essential thrombocythemia
Myelofibrosis
Other MPDs & MDS/MPN
Mutation:
GOF mutation
GT somatic mutation in exon 14 V617F
valine to phenylalanine at the 617 position,
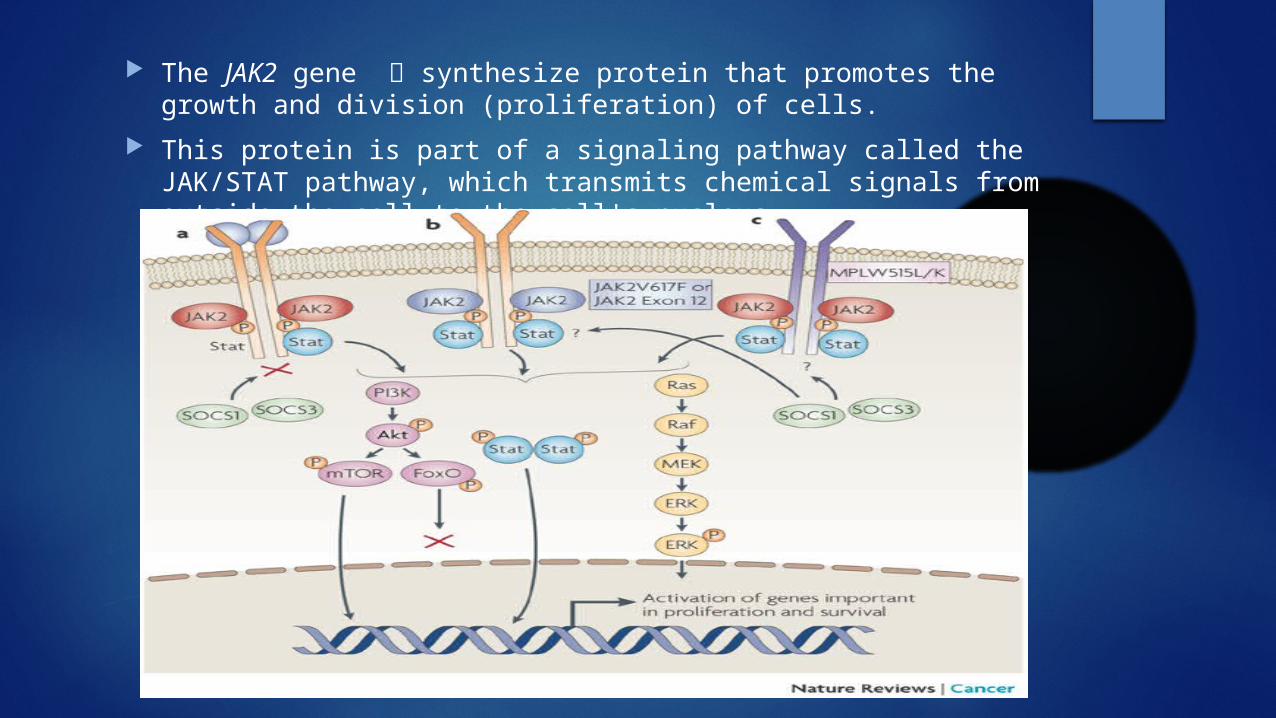
The JAK2 gene synthesize protein that promotes the growth and division (proliferation) of cells.
This protein is part of a signaling pathway called the JAK/STAT pathway, which transmits chemical signals from outside the cell to the cell's nucleus.
JAK 2 Mutations
Polycythemia Vera
Essential Thrombocytosis
Primary Myelofibrosis
Myelodysplastic syndromes
AML
MDS/MPN aCML
CMML
RARS-T
????????? Why is the same mutation occurring in the same
gene (V617F in JAK 2 gene) cause PV in some patients and ET or PMF in others ????
Why do some ET patients progress to PMF while others progress to PV ????
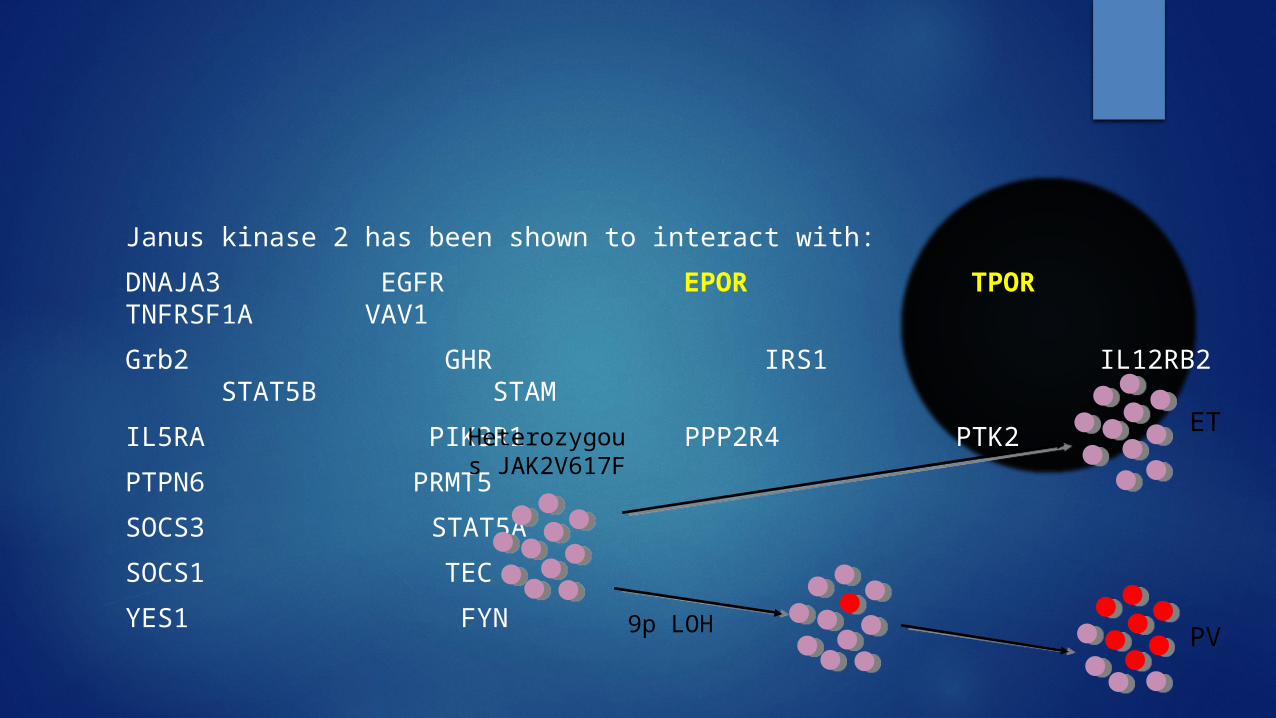
Janus kinase 2 has been shown to interact with:
DNAJA3 EGFR EPOR TPOR TNFRSF1A VAV1
Grb2 GHR IRS1 IL12RB2 STAT5B STAM
IL5RA PIK3R1 PPP2R4 PTK2
PTPN6 PRMT5
SOCS3 STAT5A
SOCS1 TEC
YES1 FYN
Heterozygous JAK2V617F
9p LOH
ET
PV
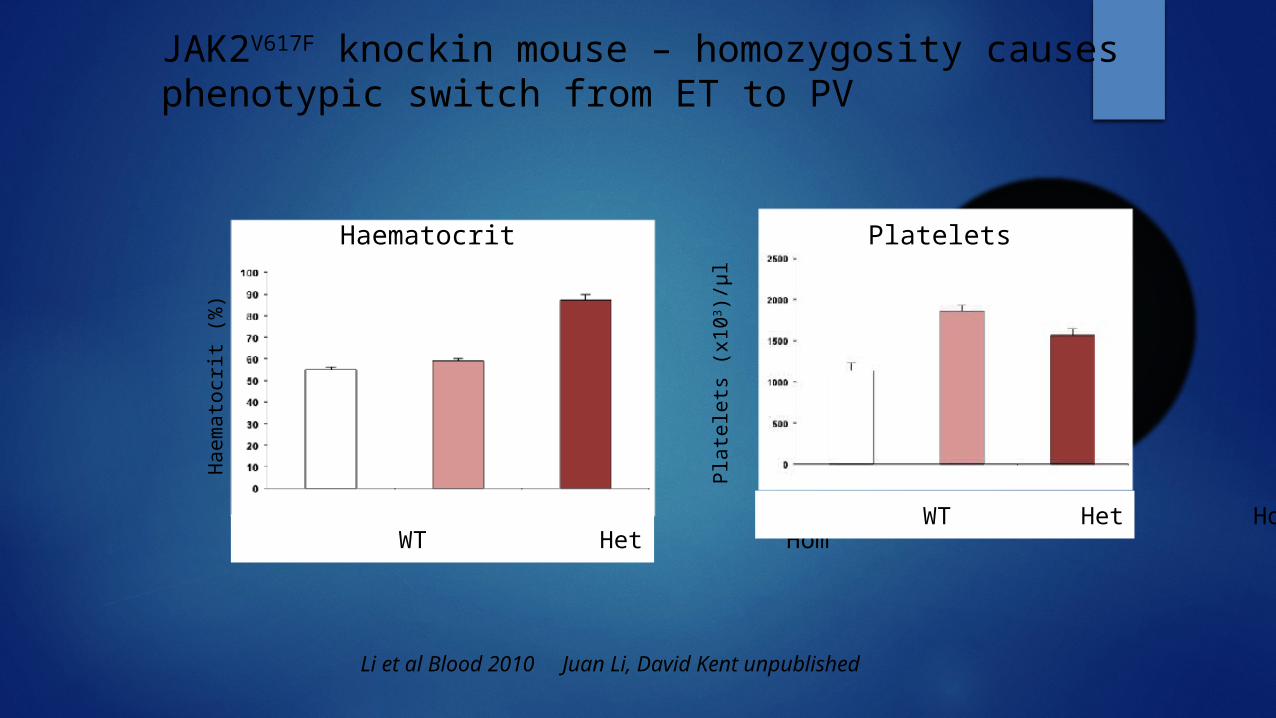
JAK2V617F knockin mouse – homozygosity causes phenotypic switch from ET to PV
Li et al Blood 2010 Juan Li, David Kent unpublished
Pla
tele
ts (
x10
3 )/µ
l
Ha
em
ato
crit
(%)
WT Het Hom WT Het Hom
Haematocrit Platelets
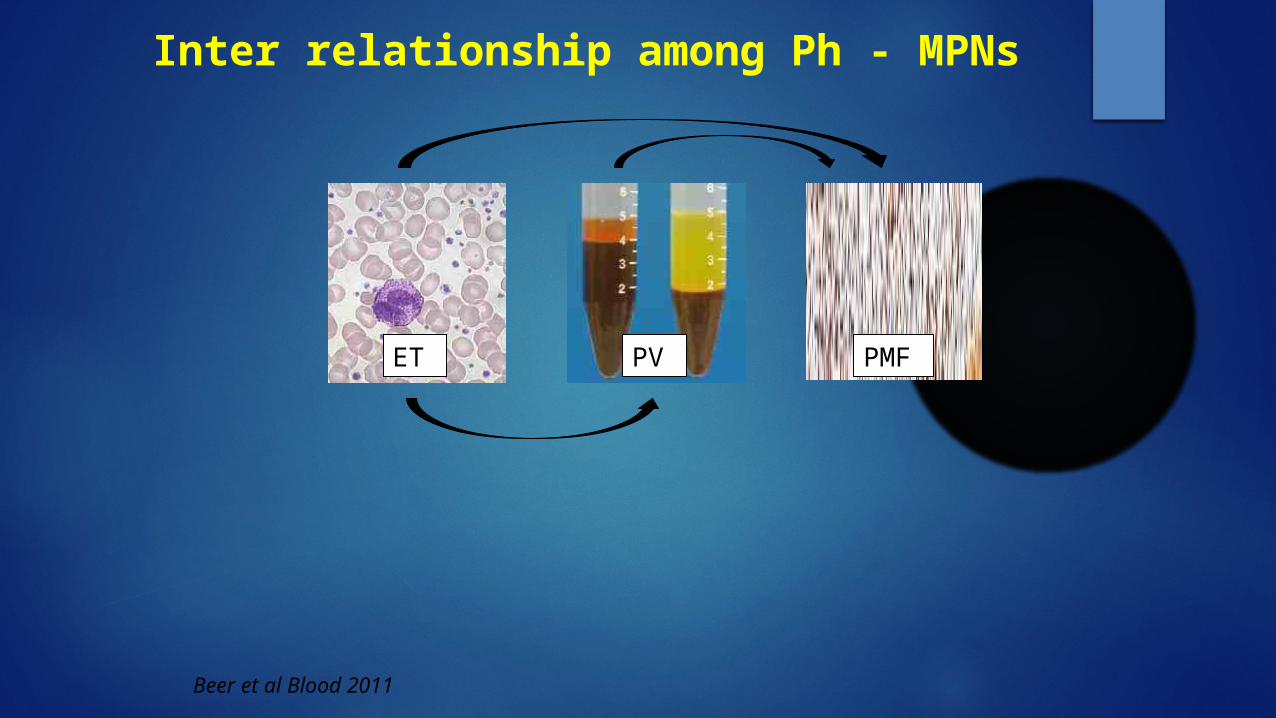
Inter relationship among Ph - MPNs
ET PV PMF
Beer et al Blood 2011
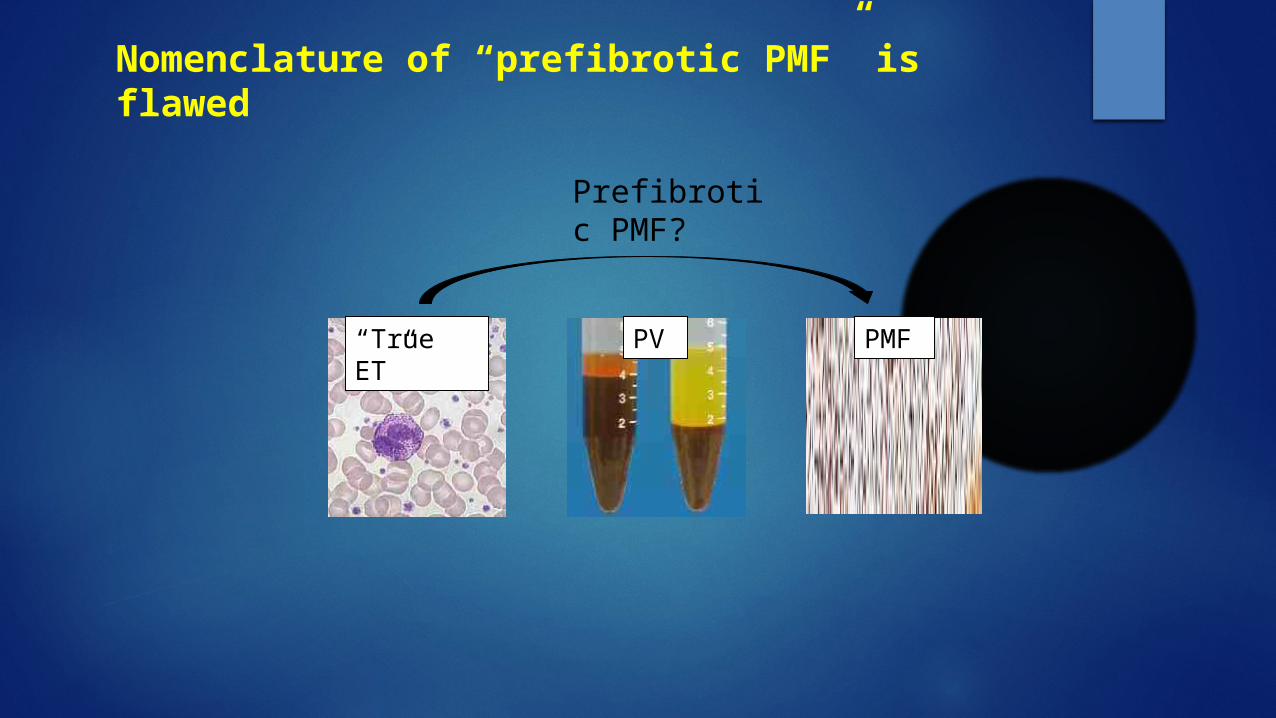
Nomenclature of “prefibrotic PMF” is flawed
“True ET”
PV PMF
Prefibrotic PMF?
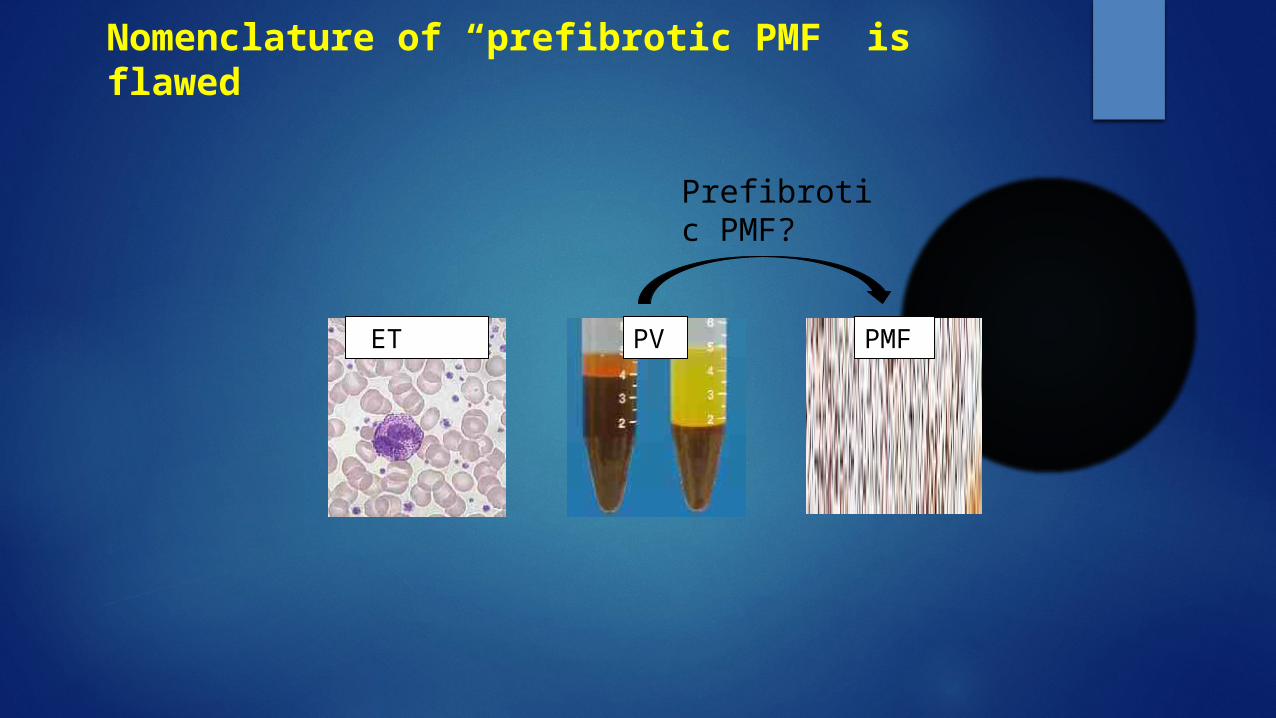
Nomenclature of “prefibrotic PMF” is flawed
ET PV PMF
Prefibrotic PMF?
Nomenclature of “prefibrotic PMF” is flawed
ET PV PMF
Prepolycythaemic PV?
JAK2V617F negative MPN• JAK2V617F-negative PV
- JAK2 exon 12 mutations- loss of function mutations in LNK, negative regulator of
JAK2*
• JAK2V617F-negative ET/PMF- MPL mutations in 10%- LNK mutations in <5%
• Somatic mutations have not been identified in few MPN patients
* Oh et al Blood 2010
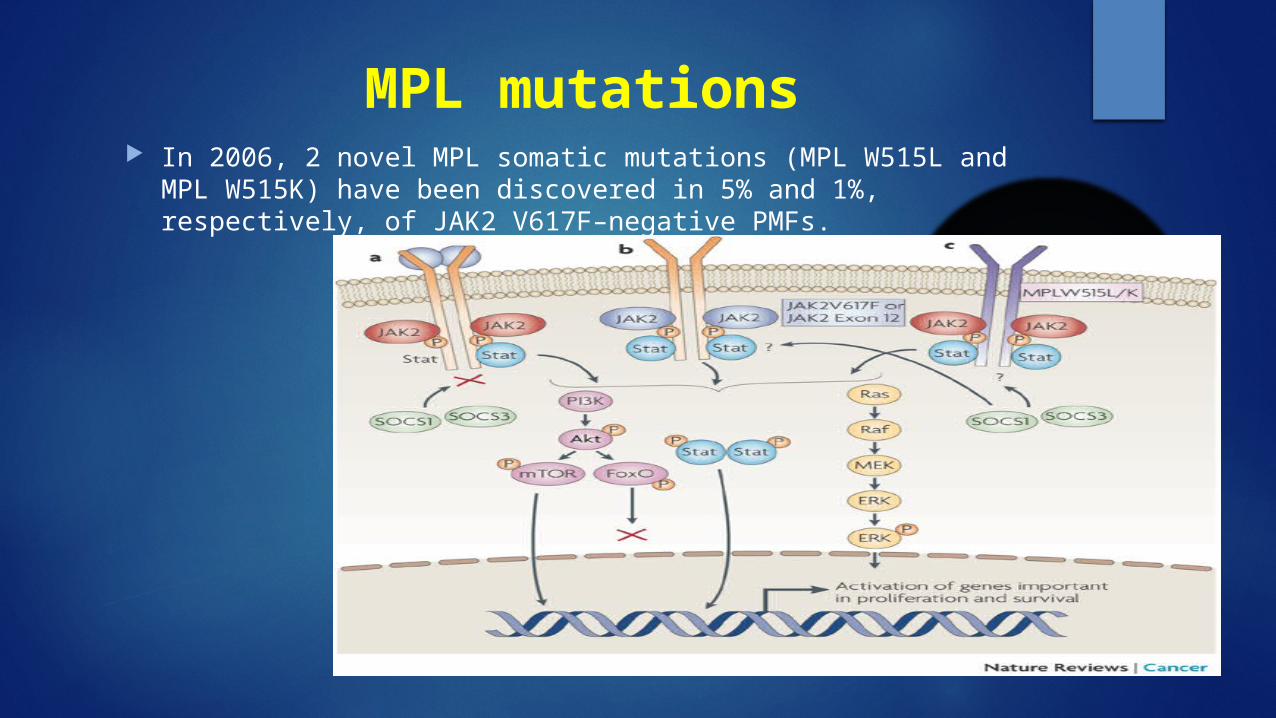
MPL mutations In 2006, 2 novel MPL somatic mutations (MPL W515L and MPL W515K) have
been discovered in 5% and 1%, respectively, of JAK2 V617F–negative PMFs.
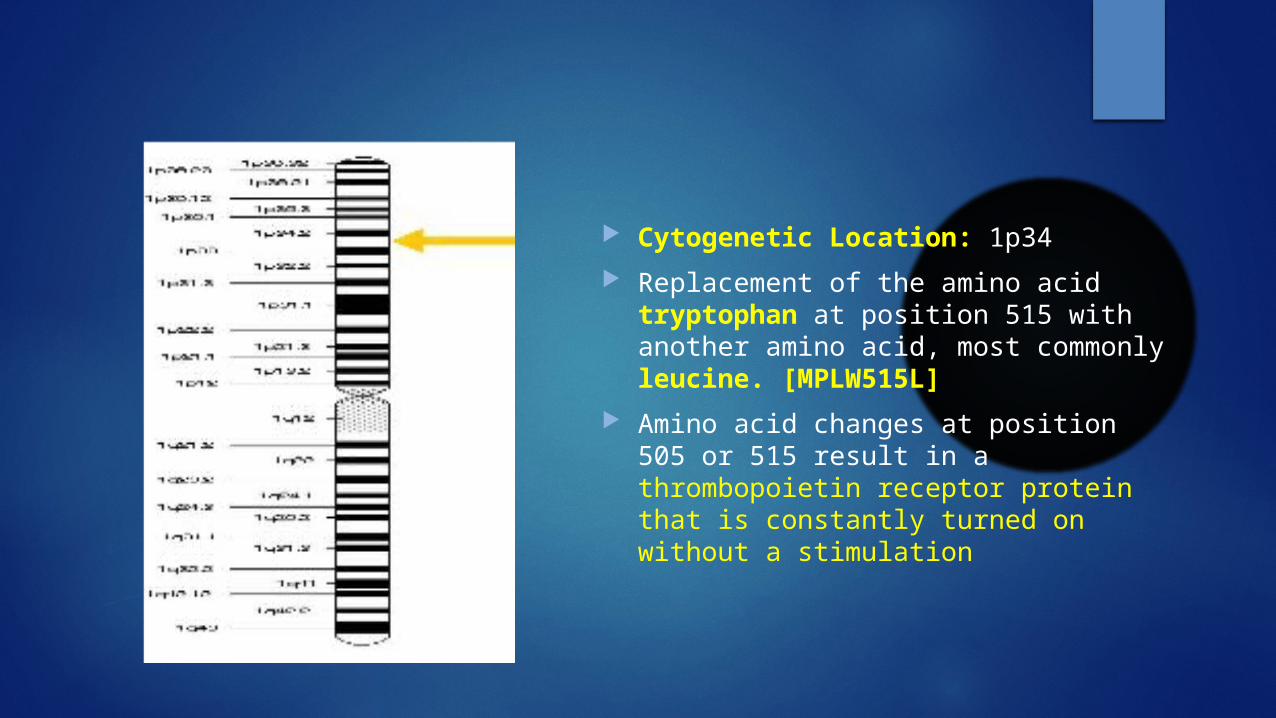
Cytogenetic Location: 1p34
Replacement of the amino acid tryptophan at position 515 with another amino acid, most commonly leucine. [MPLW515L]
Amino acid changes at position 505 or 515 result in a thrombopoietin receptor protein that is constantly turned on without a stimulation
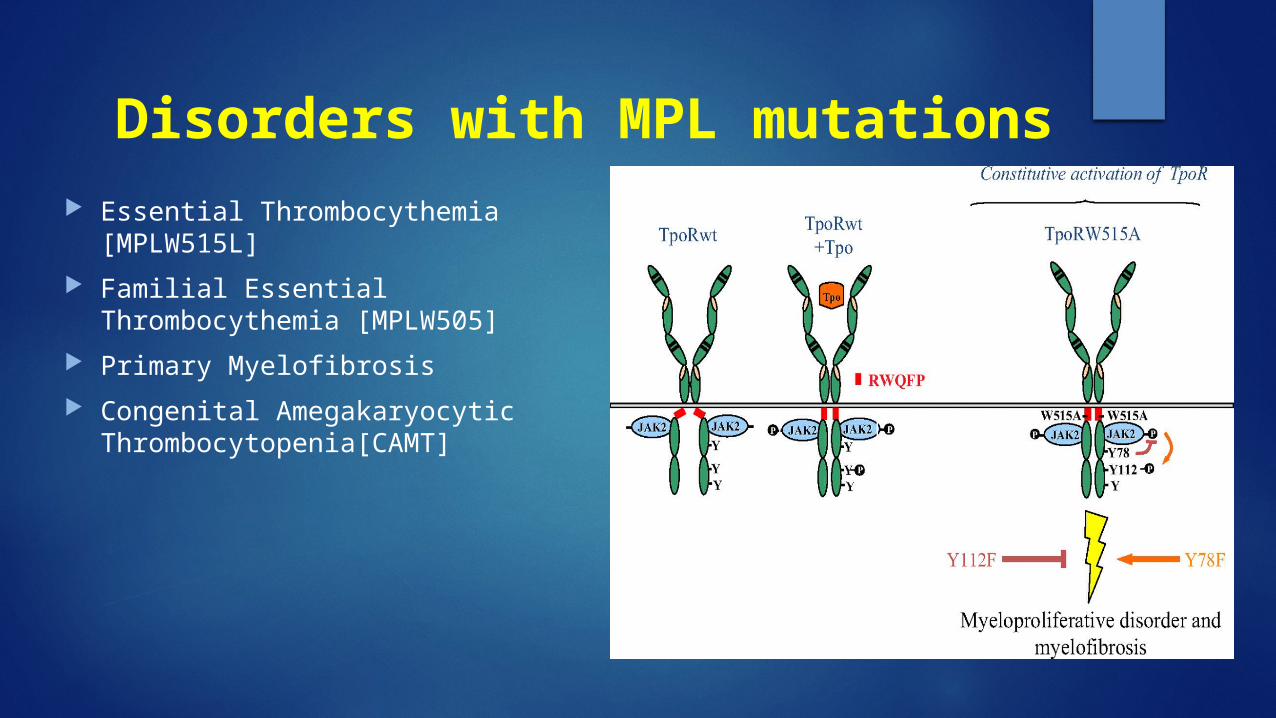
Disorders with MPL mutations Essential Thrombocythemia [MPLW515L]
Familial Essential Thrombocythemia [MPLW505]
Primary Myelofibrosis
Congenital Amegakaryocytic Thrombocytopenia[CAMT]
Kit/SCFR pathwayThe KIT protein/SCFR cell membrane of certain cell types
stem cell factor, attaches (binds) to it.
This binding turns on (activates) the KIT protein
activates tyrosine kinases
Phosphorylation
proliferation.
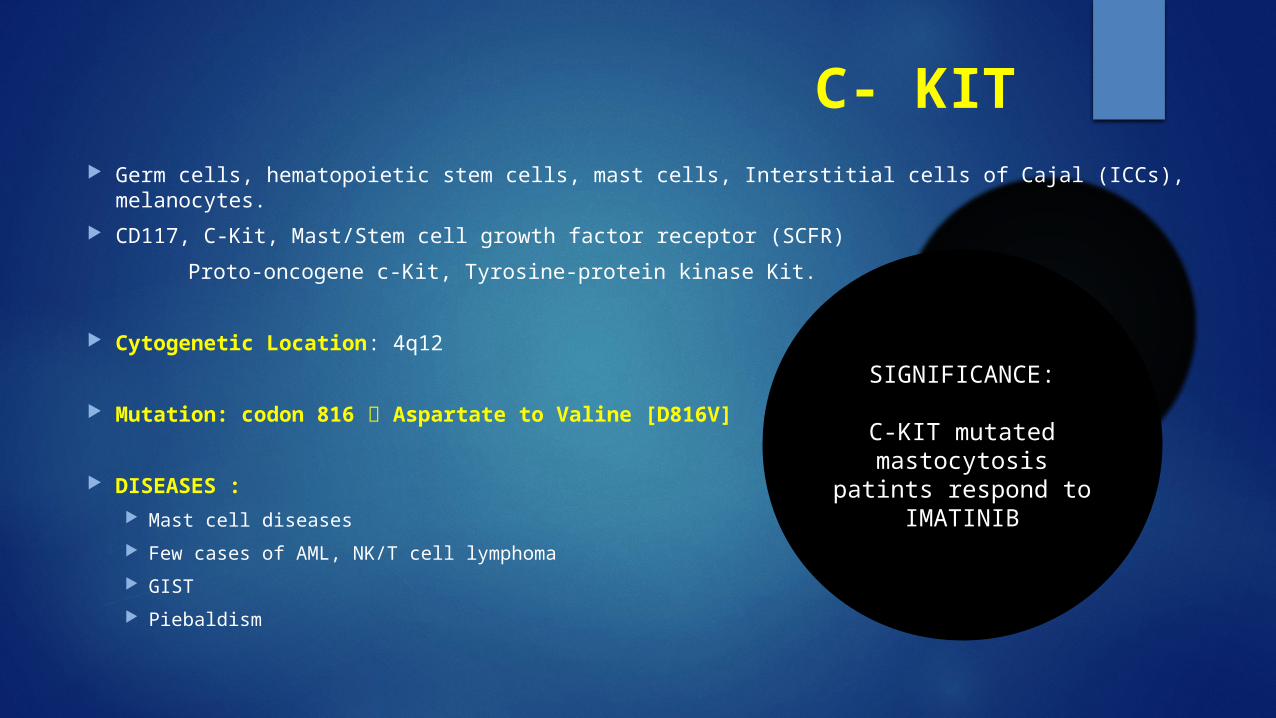
C- KIT Germ cells, hematopoietic stem cells, mast cells, Interstitial cells of Cajal (ICCs), melanocytes.
CD117, C-Kit, Mast/Stem cell growth factor receptor (SCFR)
Proto-oncogene c-Kit, Tyrosine-protein kinase Kit.
Cytogenetic Location: 4q12
Mutation: codon 816 Aspartate to Valine [D816V]
DISEASES : Mast cell diseases
Few cases of AML, NK/T cell lymphoma
GIST
Piebaldism
SIGNIFICANCE:
C-KIT mutated mastocytosis patints respond to IMATINIB
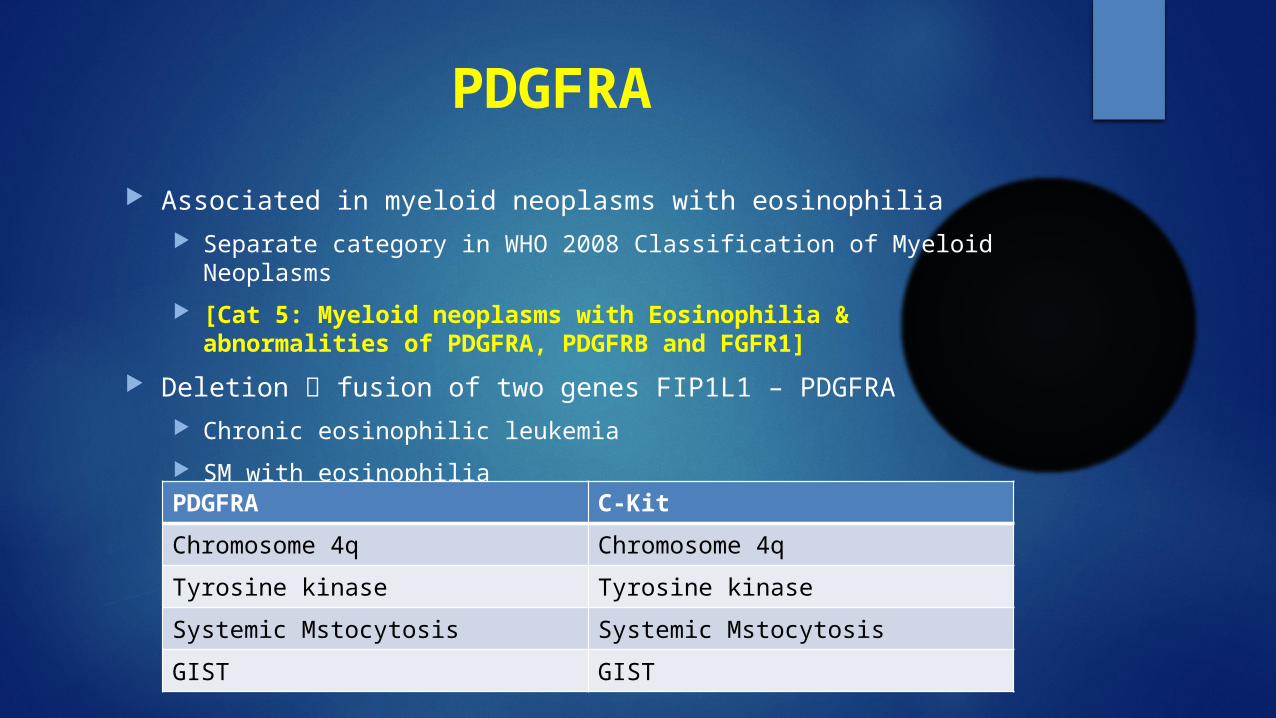
PDGFRA
Associated in myeloid neoplasms with eosinophilia Separate category in WHO 2008 Classification of Myeloid Neoplasms
[Cat 5: Myeloid neoplasms with Eosinophilia & abnormalities of PDGFRA, PDGFRB and FGFR1]
Deletion fusion of two genes FIP1L1 – PDGFRA Chronic eosinophilic leukemia
SM with eosinophilia
PDGFRA C-Kit
Chromosome 4q Chromosome 4q
Tyrosine kinase Tyrosine kinase
Systemic Mstocytosis Systemic Mstocytosis
GIST GIST
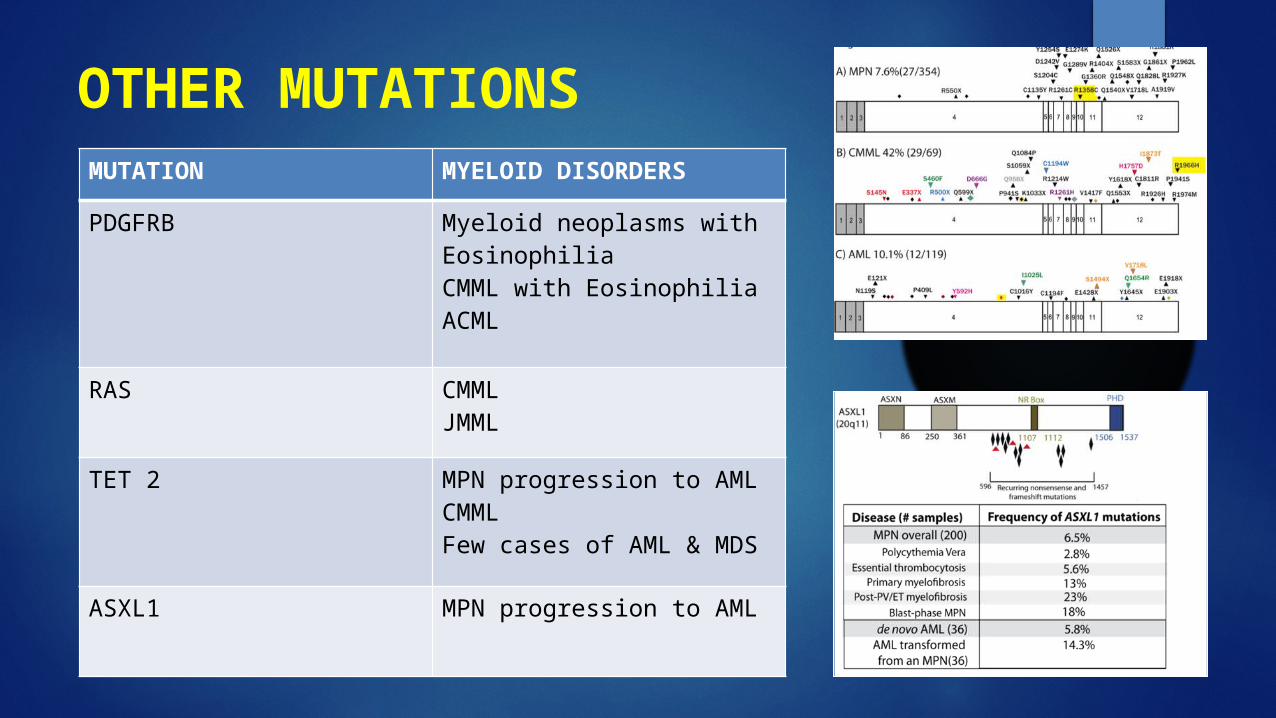
OTHER MUTATIONSMUTATION MYELOID DISORDERS
PDGFRB Myeloid neoplasms with EosinophiliaCMML with EosinophiliaACML
RAS CMMLJMML
TET 2 MPN progression to AMLCMMLFew cases of AML & MDS
ASXL1 MPN progression to AML

http://ghr.nlm.nih.gov/
THANK YOU….
Recommended