Siegburg / Stanford
The Evolution of Drug-Eluting Stents
Biosensors International Cardiology Conference
August 3rd, 2005
Eberhard Grube MDFACC, FSCAI
Heart Center Siegburg, Siegburg, GermanyStanford University, School of Medicine, CA, USA

Siegburg / Stanford
56
7783
87
0
4741
19
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
pe
rce
nt
U.S. Penetration of DES
28% (2003)
75% (2004)
CypherCypher as of 4/03 and as of 4/03 and TaxusTaxus as of 3/04as of 3/04
2003 2004

Market penetration of DES 03/04

==Bare Metal Stents

Drug-Eluting Stents
==

Siegburg / Stanford
Suppression of intimal proliferationBare metal stent versus Drug Eluting Stent
Suppression of intimal proliferationBare metal stent versus Drug Eluting Stent
BMS DES

Siegburg / Stanford
How to Assess Efficacy
Intimal Hyperplasia
Angiographic Surrogate
Late Lumen Loss
Clinical Surrogate
Target Lesion Revascularization

Siegburg / Stanford
Overall 4.1 16.6 0.0001 124
Male 4.4 16.6 0.0001 122
Female 3.4 16.5 0.0007 130
Diabetes 6.9 22.3 0.0006 154
No Diabetes 3.2 14.3 0.0001 111
LAD 5.1 19.8 0.0001 147
Non-LAD 3.4 14.3 0.0001 109
Small Vessel (<2.75) 6.3 18.7 0.0001 125
Large Vessel 1.9 14.8 0.0001 128
Short Lesion 3.2 16.1 0.0001 129
Long Lesion (>13.5) 5.2 17.4 0.0001 122
Overlap 4.5 17.7 0.0003 131
No Overlap 3.9 16.1 0.0001 121
Hazards Ratio 95% CI 1.00.90.80.70.60.50.40.30.20.10 0.70.80.9
# events prevented per1,000 patients
Sirolimus Control P-value
Sirolimus better
SIRIUS ResultsTLR: Subset Summary

Siegburg / Stanford 1.01.0 1.51.5
RRRR TAXUSTAXUS ControlControl PP
All 0.27 3.0 11.3 <0.0001
Non-diabetic 0.24 2.4 9.8 <0.0001
Diabetic, oral meds 0.28 4.8 17.4 0.004
Diabetic, insulin 0.45 5.9 13.0 0.32
LAD 0.25 3.4 13.4 <0.0001
Non-LAD 0.29 2.8 9.7 0.0001
RVD ≤≤≤≤2.5 mm 0.22 3.4 15.4 <0.0001
RVD >2.5-3.0 mm 0.28 3.1 11.2 0.0004
RVD >3.0 mm 0.38 2.5 6.7 0.57
Lsn length <10 mm 0.35 3.3 9.3 0.01
Lsn length 10-20 mm 0.27 2.8 10.5 0.0001
Lsn length >20 mm 0.18 3.3 18.6 0.0009
TAXUS IV ResultsTLR: Subset Summary
00 0.50.5RR [95% CI]

Siegburg / Stanford
PaclitaxelSirolimusRavelSirius
The Winners
1. FIM (45)2. Sirolimus PK (19)
3. SECURE (252)
4. RAVEL (238)
5. SIRIUS (1058)
6. China (41)7. Taiwan (50)
8. Argentina (20)
9. BIF (86)
10. E-SIRIUS (353)
11. C-SIRIUS (100)12. ISR-Feas (41)
13. US ISR-Feas (8)
14. TROPICAL (160)
15. SISR (400)16. ISR-Barragan (23)
17. ARTS II (600)
18. FREEDOM (2600)
19. 2.25 mm (100)
20. 4.00 mm (100)21. ATLAS (100)
1. FIM (45)2. Sirolimus PK (19)
3. SECURE (252)
4. RAVEL (238)
5. SIRIUS (1058)
6. China (41)7. Taiwan (50)
8. Argentina (20)
9. BIF (86)
10. E-SIRIUS (353)
11. C-SIRIUS (100)12. ISR-Feas (41)
13. US ISR-Feas (8)
14. TROPICAL (160)
15. SISR (400)16. ISR-Barragan (23)
17. ARTS II (600)
18. FREEDOM (2600)
19. 2.25 mm (100)
20. 4.00 mm (100)21. ATLAS (100)
22. SICTO (25)23. SVG-Feas (150)
24. DIRECT (220)
25. DECODE US (100)
26. DECODE (100)
27. BRIDGE (1000)28. PORTO I & II (300)
29. SCORPIUS (190)
30. Cypher-SMART (256)
31. EVASTENT (2000)
32. TYPHOON (700)33. DESSERT (250)
34. SVELTE (101)
35. REDOX (60)
36. 3D (44)
37. SC US (tbd)38. SC EU (tbd)
39. SVS-Feas (45)
40. SIROCCO I (36)
41. SIROCCO II (57)42. GREAT (101)
22. SICTO (25)23. SVG-Feas (150)
24. DIRECT (220)
25. DECODE US (100)
26. DECODE (100)
27. BRIDGE (1000)28. PORTO I & II (300)
29. SCORPIUS (190)
30. Cypher-SMART (256)
31. EVASTENT (2000)
32. TYPHOON (700)33. DESSERT (250)
34. SVELTE (101)
35. REDOX (60)
36. 3D (44)
37. SC US (tbd)38. SC EU (tbd)
39. SVS-Feas (45)
40. SIROCCO I (36)
41. SIROCCO II (57)42. GREAT (101)
TAXUS

Siegburg / Stanford
5,7%3,5%
17,1%19,2%
TLR TVR
%
Sirolimus (n=1204) Control (n=870)
CYPHER Trials - Clinical Events
All Events (to 9 months)
P<0.0001P<0.0001
80% 70%

Siegburg / Stanford
TAXUS II + IV + VI Meta-analysis (n=2,289)
12 Month TLR and TVR
17.5%15.6%
7.6%4.9%
12
Mo
nth
Ev
en
ts (
%)
12
Mo
nth
Ev
en
ts (
%)
ControlControl TAXUSTAXUS
TVRTVRTLRTLR
RR=0.31 [0.24,0.42], P<0.0001 RR=0.44 [0.34,0.55], P<0.0001
N=1,148 N=1,141 N=1,148 N=1,141

Siegburg / Stanford
Control TAXUST
LR
(%
)
Insulin reqDiabeticsall patients
14.8
5.8
18.6
7.3
16.9
5.8
P<0.0001 P<0.0001 P<0.0001
TAXUS metaanalysis
TAXUS in diabetic patients

Siegburg / Stanford
II IIaIIa IIbIIb IIIIII
Recommendation DES
CypherCypher™™
RAVELRAVEL
SIRIUSSIRIUS
EE--SIRIUSSIRIUS
CC--SIRIUSSIRIUS
TAXUSTAXUS™™
TAXUSTAXUS--II
TAXUSTAXUS--IIII
TAXUSTAXUS--IVIV
TAXUSTAXUS--VIVI
De-Novo Läsionen
RVD 2.5 – 3.75 mm, ≤≤≤≤30 mm in length

DES - 2005Need for more Evidence ?
�� Long Long LesionsLesions
�� Small Small vesselsvessels
�� ISR ISR lesionslesions (esp. (esp. ultraultra--diffusediffuse andand s/p VBT)s/p VBT)
�� Bifurcations (esp. Bifurcations (esp. ostialostial sidebranchsidebranch))
�� LM LM diseasedisease (esp. distal bifurcation)(esp. distal bifurcation)
�� SVGsSVGs
�� CTOsCTOs
�� AMIAMI
�� MultivesselMultivessel DiseaseDisease
�� ……

Siegburg / Stanford
P<0.0001 P<0.0001
Binary restenosis in-stent
(%)
Control TAXUS MR
40.4
7.3
23/57 4/55
7.0
50.0
17/34 3/43
40.5
8.1
17/42 3/37
P<0.0001
Small vessels<2.5mm
Long lesions≥26mm
Diabetics
82 % 86 % 80 %
Overlappingstents
25/55 3/62
45.5
4.8
89 %
P=0.0015
TAXUS VIRestenosis benefit independent of classic risk factors

Siegburg / Stanford Neumann et al., PCR 2004
SES vs. Historical Gamma VBT
n= 162 SES262 VBT
TROPICALTROPICAL
Clinical Outcome at 180 DaysClinical Outcome at 180 Days
Non- Hierarchical Event Rate (%)TROPICAL
GAMMA I/II
0
5
10
15
20
Death MI Clinicallydriven TLR
Stent thrombosis
MACE
P=0.490
P=0.004
P<0.001
P=0.080
P<0.001
3.7
0.6 1.82.5
0.6
18.8
2.0
25
9.4
14
3.9
30

Siegburg / Stanford
CYPHER in CYPHER in CTOCTO’’ss
RESEARCH RegistryRESEARCH Registry

Siegburg / Stanford
ISAR – DESIRECYPHER vs. TAXUS

Siegburg / Stanford
ISAR – DESIRECYPHER vs. TAXUS

Siegburg / Stanford
-- 3400 randomized patients undergoing primary PCI 3400 randomized patients undergoing primary PCI --
Hypothesis: Hypothesis: Use of the TAXUS Use of the TAXUS PTxPTx--
eluting eluting stentstent will safely reduce the 1will safely reduce the 1--year year
rate of ischemiarate of ischemia--driven TVRdriven TVR
Hypothesis: Use of bivalirudin + bailHypothesis: Use of bivalirudin + bail--out out
IIb/IIIa will rIIb/IIIa will reduce the composite rate of educe the composite rate of
death, death, reinfarctionreinfarction, TVR, disabling stroke , TVR, disabling stroke
and major bleeding at 30and major bleeding at 30--daysdays
HORIZONS AMI Study
Target vessel Target vessel stentingstenting
Bare metalBare metal
ExpressExpress™™ stentstentTAXUSTAXUS
stentstent
Randomize 1:3Randomize 1:3
AntiAnti--thromboticthrombotictherapytherapy
UFH + UFH +
IIb/IIIaIIb/IIIa
inhibitorinhibitor
BivalirudinBivalirudin++
bailbail--outout
IIb/IIIa IIb/IIIa
Randomize 1:1Randomize 1:1
PI: Gregg W. StonePI: Gregg W. Stone

MV-sirolimus stentingWith abciximab
Multivessel Sirolimus Stenting vs. CABG in Diabetics
Eligibility: DM patients with MV-CAD eligible for stent or surgeryExclude: Patients with acute MI and/or cardiogenic shock
CABGWith or without CPB
All concomitant Meds shown to be beneficial are encouraged, including: Plavix, ACE inhibitors, b-blockers, statins, etc.
1o Endpoint: 5-year mortality 5-year MACE2o Endpoint : MACE/stroke at 12 months
2300 pts Randomized 1:1
FREEDOM Trial

Siegburg / Stanford
SYNTAX StudieTAXUS vs. CABG
Left main disease 3-vessel disease
Primary endpoint – MACCE•All cause death •MI
•Cerebrovascular events•Repeat revascularization
TAXUS PCI CABG
OR
R
De novo disease acceptable for revascularization
N=4500

Need for Improvements?
Of course....

Siegburg / Stanford
Safety
Efficacy
Cost

Drug Eluting Stents

Siegburg / Stanford
Safety
Efficacy
Cost

DES - Animal StudiesWhat do the “bad things” look like…
• Excessive thrombus• Incomplete endothelialization
• Severe inflammatory response
• Persistent fibrin + inflammation
• Medial necrosis• Malapposition

Siegburg / Stanford
0.6
1.6
0.4
1.8
0.0
0.5
1.0
1.5
2.0
2.5
Intention-to-Treat Actually-Treated*
CYPHER® TAXUS™
0.6
1.6
0.4
1.8
0.0
0.5
1.0
1.5
2.0
2.5
Intention-to-Treat Actually-Treated*
CYPHER® TAXUS™
PP=0.0723=0.0723 PP=0.0196=0.0196
111144 121233
% of % of PatientsPatients
Stent Thrombosis (Acute + Subacute)
Per protocol analysis: CYPHERPer protocol analysis: CYPHER®® 0.4, TAXUS0.4, TAXUS™™ 1.7: 1.7: PP=0.033=0.033* 1 patient randomized to CYPHER* 1 patient randomized to CYPHER®® actually treated with a TAXUSactually treated with a TAXUS™™ stentstent
REALITY

Siegburg / Stanford
2229 patients after successful DES implantation 2229 patients after successful DES implantation
PESPES
1167 pts1167 pts
2223 stents 2223 stents
SATSAT
4 (0.4%)4 (0.4%)SATSAT
10 (0.9%)10 (0.9%)
LSTLST
5 (0.5%)5 (0.5%)
LSTLST
10 (0.9%)10 (0.9%)
Total SESTotal SES
9 (0.9%) 9 (0.9%) Total PESTotal PES
20 (1.7%)20 (1.7%)
9.3 9.3 ±±±±±±±± 5.6 months 5.6 months
Total DES 29/2229 Total DES 29/2229 (1.3%)(1.3%)
P=0.5P=0.5
P=0.3P=0.3
P=0.09P=0.09
10.2 10.2 ±±±±±±±± 4.44.4 mm 7.9 7.9 ±±±±±±±± 3.63.6 mm
Stent Thrombosis after DES
SESSES
1062 pts 1062 pts
2272 stents 2272 stents

Siegburg / Stanford
Acute stent thrombosis: Up to 30 days
Range in each program
4.0 0 4.02.0 2.0
Observed
Range
Observed
Range
Stent Thrombosis (%)
SIRIUSMILESTONE
II
Limus Paclitaxel
TAXUS IV
SIRTAX
ENDEAVOR
IITAXUS V
REALITY REALITY
ARRIVEE-SIRIUS
C-SIRIUS
SIRTAX
RESEARCH
/TSEARCH
WISDOM
MILAN DES
TAXUS II SR
TAXUS VI
2.0 0.2 0.2 1.6

Siegburg / Stanford
Single TLR in TAXUS-SR at Day 522
•• Mid RCAMid RCA
•• RVD:4 mmRVD:4 mm
•• LL: 4 mmLL: 4 mm
•• % DS: 75%% DS: 75%
Baseline61 y.o. male with prior MI and hypercholesterolemia61 y.o. male with prior MI and hypercholesterolemia
•• PrePre--dilationdilation
•• 1 SS: 3.5 x 15mm1 SS: 3.5 x 15mm
•• No complicationsNo complications
•• 6mo FU 6mo FU
•• AsymptomaticAsymptomatic
•• No restenosisNo restenosis
Post
•• Non QNon Q--wave MIwave MI
•• Thrombectomy, PTCAThrombectomy, PTCA
•• On ASA, off On ASA, off
clopidogrelclopidogrel
Stent Thrombosis
Day 522
2 year
•• AsymptomaticAsymptomatic
Day 738

Siegburg / Stanford
Stent thrombosis

Siegburg / Stanford
0,3 0,3
0,3
0,2
0,3 0,5
0 0,5 1 1,5
Control
(n=613)
TAXUS
(n=625)
Stent thrombosis, %
In-hospital Discharge - 30 days
31 days - 1 year* 1-2 years
P=0.77
1.1%(n=7)
0.8%(n=5)
* All within 1-6 months
TAXUS IV TAXUS IV
Stent ThrombosisStent Thrombosis

Siegburg / Stanford
Safety
Efficacy
Cost

Siegburg / Stanford
Restenosis of ABT-578-eluting stent (OCT)
ENDEAVOR-II 8 mths follow-up
Stent overlap area
4.8 mm2
2.1 mm2
1.0 mm21.4 mm2
3.5 mm2
6.1 mm2 5.5 mm2
6.5 mm2
53.8%
25.5%16.4%
43.8%
LA / SA
Lumen A
Stent A

Siegburg / Stanford
TAXUS V9-Month Angiography2.25 mm Stent Subgroup (n=203)
44,749,4
24,731,2
InIn--stentstent InIn--SegmentSegmentInIn--stentstent InIn--SegmentSegment
Late LossLate Loss Binary RestenosisBinary Restenosis
Control (n=85)Control (n=85) TAXUS (n=93)TAXUS (n=93)
0.900.90±±±±±±±±0.630.63
0.490.49±±±±±±±±0.610.61
0.610.61±±±±±±±±0.590.59
0.360.36±±±±±±±±0.530.53
p<0.0001 p=0.01p=0.004 p=0.007
8585 9393 8585 9393 38/8538/85 23/9323/93 42/8542/85 29/9329/93

Siegburg / Stanford
Various Approaches to Improve Drug Eluting Stents
Better Better Stent designStent design
Better Better
Pharmacologic Pharmacologic
agentagent
Better Better Drug carrier Drug carrier
vehiclevehicle
Drug-
Eluting
Stent
DrugDrug--
Eluting Eluting
StentStent

Siegburg / Stanford
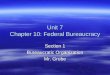
BioMatrix™ Stent Components(Biosensors International Group)
S-Stent™ (stainless steel)• Quadrature-link design; increased flexibility
• Excellent scaffolding
• Reduced turbulence and wall injury
PLA Polymer• Uniform thickness; bioresorbable
• Simultaneously releases drug and polymer
• Controlled biodegradability
• High drug-carrying capacity
• Minimizes polymer weight to minimize
inflammation; polymer absorbed into tissue
Stent
Biolimus A9™ (rapamycin derivative)• Powerful immunosuppressant, anti-inflammatory
• Prevents smooth muscle cell proliferation
• More lipophilic; faster cellular absorption

Siegburg / Stanford
STEALTH I: Clinical Follow-up
6-Month Follow-up:
95% (n=114)
12-Month Follow-up:
99.2% (n=119)
120 Patients
Control BMS S-Stentn = 40
BioMatrixn = 80

Siegburg / Stanford
STEALTH I: Hierarchical MACE at 6 and12 Months
Cumulative
1.3%0.0%0.0%0.0%TLR-CABG
1.3%0.0%1.3%0.0%TLR-PTCA
12 Months*6 Months
RESULTS
2.5%
0.0%
2.5%
5.0%
S-Stent
1.3%1.3%2.5%Non-Q Wave MI
6.3%3.8%2.5%MACE
1.3%0.0%0.0%Death**
1.3%1.3%0.0%Q Wave MI
BioMatrixBioMatrixS-Stent
*Not adjudicated
**Death events were noncardiac: 1 traffic accident (S-Stent); 1 acute leukemia (BioMatrix)

Siegburg / Stanford
Biolimus-eluting stent
STEALTH-1 12 mths follow-up

Siegburg / Stanford
STEALTH I: Late Loss—Edge Results
In-segment
0.140,00
0,20
0,40
0,60
0,80
Late Loss
Proximal In-Stent Distal In-
Segment
Control BMSBiolimus A9
P=0.004P=0.73P=0.23 P<0.001
50%
65%20%
69%
0.170.10
0.08
0.74
0.26 0.10
0.400.14

Siegburg / Stanford
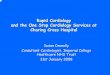
Comparison of Neointimal Volume
32,0
16,712,8 12,2
7,9 7,23,1 2,9 2,6 1,5 1,1 1,00,0
5,010,015,020,025,030,035,0
%
BMS
ASPE
CT L
owAS
PECT
Hig
hTA
XUS
IVTA
XUS
IITA
XUS
ISI
RIUS
FUTU
RE 1
STEA
LTH
ISV
ELTE
FUTU
RE II
RAVE
L
Taxol family Limus family
No PolymerNo Polymer
PolymerPolymer
PolymerPolymer
Courtesy Shimada, Honda, Hassan, Fitzgerald

Siegburg / Stanford
DES are highly efficient in prevention of restenosis; this DES are highly efficient in prevention of restenosis; this
has been demonstrated by the largest body of has been demonstrated by the largest body of
evidence ever collected in the history of device evidence ever collected in the history of device
evaluation evaluation
More data are coming up soon, which will expand the More data are coming up soon, which will expand the
official recommendations for DES use; however there official recommendations for DES use; however there
is still need for further investigations in specific is still need for further investigations in specific
subgroups (SVG, etc)subgroups (SVG, etc)
DES are safe, but continuing surveillance is recommended to monitor the unknown long-term effects of this young technology
New DES will improve both safety and efficacy of this revolutionary treatment concept
Conclusions

Siegburg / Stanford

Siegburg / Stanford
Thank youThank you

Siegburg / Stanford
Stent thrombosis in BMS

Siegburg / Stanford
Stent thrombosis in BMS
Recommended