Embed Size (px)
Citation preview

Practical CardiologyValvular DiseasePractical CardiologyValvular Disease
Wendy Blount, DVM
Nacogdoches TX
Wendy Blount, DVM
Nacogdoches TX

DaisyDaisy
Signalment
• 15 year old spayed female mixed terrier
• 11 pounds
Chief Complaint
• Became dyspneic while on vacation, as they drove over a mountain pass
• Come to think of it, she has been breathing hard at night for some time

DaisyDaisy
Exam
• T 100.2, P 185, R – 66, BP – 145, BCS – 3.5
• Increased respiratory effort (heart sounds)
• 3/6 pansystolic murmur loudest at left apex
• Mucous membranes pale pink
• Crackles in the small airways
• Pulses weak, somewhat irregular, no pulse deficits
• CRT 3.5-4 seconds

DaisyDaisy
CBC, mini-panel, electrolytes
• Normal

DaisyDaisy
CBC, mini-panel, electrolytes
• Normal

DaisyDaisy
ECG
DaisyDaisy
Calculating Instantaneous Heart Rate (iHR)• Measure R wave to R wave (9mm)•
• Divide by paper speed (25 mm/sec) for time per beat
9mm x _sec_ = 0.36 sec per heart beat
25mm•
• Calculate beats per minute
_heart beat_ x _60 sec = 166 beats/minute
0.36 sec minute

DaisyDaisy
ECG• Rate – 110 bpm
• Rhythm – sinus arrhythmia with VPCs
• MEA – normal (lead II has tallest R waves)
• P, QRS and T waves – normal– No evidence of enlarged LA and LV on the ECG
• VPC – abnormal QRS– Comes too early (iHR 166 bpm)
– Wide and bizarre shape
– Not preceded by a P wave
– T wave opposite in polarity than normal QRS
– Compensatory pause after the VPC

DaisyDaisy
Initial Therapeutic Plan
• Lasix 25 mg IM, then 12.5 mg PO BID
• Enalapril 2.5 mg PO BID
• Pimobendan 1.25 mg PO BID
• Owner is a med tech, and set up oxygen mask to use PRN at home
DaisyDaisy
When to treat VPCs• VPCs unusual for MR
• Did not treat in this case, because:
– MR dogs not predisposed to sudden death
• PS, SAS and DCM are more associated with sudden death due to arrhythmia
– Ectopic focus not firing at a fast rate (166 bpm)
• <200 bpm iHR is well away from the T wave
– No pulse deficits – did not affect hemodynamics
– Primary treatments for VPC are Sotalol or B blocker
• Negative inotropes not ideal for myocardial failure

DaisyDaisy
Recheck – 4 days
• Daisy’s breathing is much improved (30-40 at rest)
• Lateral chest x-ray
• Electrolytes normal
• BUN 52

DaisyDaisy
Recheck – 4 days
• Daisy’s breathing is much improved (30-40 at rest)
• Lateral chest x-ray
• Electrolytes normal
• BUN 52

DaisyDaisy
Diagnostic Plan - updated• Decrease enalapril to SID
• Recheck BUN 1 week
• Recheck chest rads 1 week
Recheck – 1 week• BUN – 37
• Thoracic rads no change
• Request recheck in 3 months, or sooner if respiratory rate at rest is above 35 per minute

DaisyDaisy
2 months later
• Daisy is breathing hard again at night

DaisyDaisy
2 months later
• Daisy is breathing hard again at night

DaisyDaisy
2 months later
• Daisy is breathing hard again at night
DaisyDaisy
Bloodwork
• CBC, electrolytes normal
• BUN 88
Therapeutic Plan
• Increase furosemide to 18.75 mg PO BID
• Add hydralazine 2.5 mg PO BID
• Recheck chest rads, BUN, electrolytes, blood pressure 1 week

DaisyDaisy
Recheck – 1 week
• Clinically much improved – respiratory rate 30-40 per minute at rest
• electrolytes normal
• BUN 58
• Blood pressure 135

DaisyDaisy
Recheck – 1 week
• Clinically much improved – respiratory rate 30-40 per minute at rest
• electrolytes normal
• BUN 58
• Blood pressure 135

DaisyDaisy
Recheck – 6 months
• Daisy dyspneic again
Exam
• Similar to last crisis – BP 90

DaisyDaisy
Bloodwork
• CBC, electrolytes normal
• BUN 105, creat 2.1

DaisyDaisy
Bloodwork
• CBC, electrolytes normal
• BUN 105, creat 2.1
Chest x-rays

DaisyDaisy
Bloodwork
• CBC, electrolytes normal
• BUN 105, creat 2.1
Chest x-rays
• Similar to last crisis
ECG
• Sinus tachycardia, wide P wave

Daisy - EchoDaisy - Echo
Short Axis – LV apex (video)• LV looks big
Short Axis – LV papillary muscles• IVSTD – 6.0 mm – low normal
• LVIDD – 35 mm (n 20.2-25)
• LVPWD – 4.3 mm – low normal
• IVSTS – 9.4 mm – normal
• LVIDS – 25 mm (n 11.1-14.6)
• LVPWS – 8.4 mm - normal

Daisy - EchoDaisy - Echo
Short Axis – LV papillary muscles• IVSTD – 6.0 mm – low normal
• LVIDD – 35 mm (n 20.2-25)
• LVPWD – 4.3 mm – low normal
• IVSTS – 9.4 mm – normal
• LVIDS – 25 mm (n 11.1-14.6)
• LVPWS – 8.4 mm – normal
• FS – (35-25)/35 = 29% (normal 30-46%)

Daisy - EchoDaisy - Echo
Short Axis - MV
• MV leaflets hyperechoic and thickened
• EPSS – 8 mm (n 0-6)
Short Axis – Aortic Valve/RVOT
• LA appears 2-3x normal size
• AoS – 13.0 – normal
• LAD – 33 mm (n 12.8-15.6)
• LA/Ao = 2.5 (n 0.8-1.3)
Daisy - EchoDaisy - Echo
Long View – 4 Chamber
• LV and LA both appear large
• MV is very thick and knobby, with some prolapse into the LA

Daisy - EchoDaisy - Echo
Long View – 4 Chamber
• LV and LA both appear large
• MV is very thick and knobby, with some prolapse into the LA

Daisy - EchoDaisy - Echo
Long View – 4 Chamber
• LV and LA both appear large
• MV is very thick and knobby, with some prolapse into the LA
• Pulmonary vein markedly enlarged
Long View – LVOT
• Large LA, Large LV

DaisyDaisy
Therapeutic Plan
• Increase hydralazine to 5 mg PO BID
• Add spironolactone 12.5 mg PO BID
• Increase furosemide to 18.75 mg PO TID x 2 days, then decrease to BID if respiratory rate decreases to less than 40 per minute at rest.
• Recheck 1 week – BUN, creat, phos, electrolytes, chest rads, BP

DaisyDaisy
Recheck – 1 week
• Clinically improved again
• BP - 125
• BUN 132, creat 2.6, phos 6.6
• Electrolytes normal
• chest rads improved pulmonary edema
Therapeutic Plan – Update
• Add aluminum hydroxide gel 2 cc PO BID

DaisyDaisy
5 Months later
• Coughing getting worse
• Chest rad show no pulmonary edema
• LA getting larger
Therapeutic Plan – Update
• Add torbutrol 2.5 mg PO PRN to control cough

DaisyDaisy
18 Months after initial presentation
• Owner discontinue pimobendan due to GI upset
28 months after initial presentation
• Daisy finally took her final breath
• BUN >100 for 22 months

Chronic MV DiseaseChronic MV Disease
• May be accompanied by similar TV disease (80%)
• TV disease without MV disease possible but rare
• LHF and/or RHF can result
• Right heart enlargement can develop due to pulmonary hypertension, in turn due to LHF
Chronic MV DiseaseChronic MV Disease
Thoracic radiograph abnormalities:• LV enlargement
– Elevated trachea
– increased VHS
• LA enlargement – often largest chamber– Compressed left bronchus
• + left heart failure– Pulmonary edema
– Lobar veins larger than arteries
Chronic MV DiseaseChronic MV Disease
Echo abnormalities: (doppler echo)• LA and/or RA dilation, LV and/or RV dilation
• Exaggerated IVS motion (toward RV in diastole)
• Increased FS first, then later decreased FS
• Thickened valve leaflets (video) (video 2)
• If TV only affected, left heart can appear compressed, small and perhaps artifactually thick
• Ruptured CT –– MV flips around in diastole
– MV flies up into LA during systole – “MV flail” (video)
– May see trailing CT, or CT floating in the LV

Chronic MV DiseaseChronic MV Disease
Right Heart Failure
• Medications similar to LHF
• Medications not as effective at eliminating fluid
congestion
– More effective at preventing fluid accumulation, once controlled
• Periodic abdominocentesis and/or pleurocentesis
required
• Prognosis for RHF and LHF is extremely variable
Chronic MV DiseaseChronic MV Disease
Classification of Chronic AV Valve Disease
• Class I - small, discrete nodules along the edge of the
valve leaflets
• Class II - free edges are thickened and the edges of
the leaflets become irregular. Some CT are thickened.
• Class III - valve edges grossly thickened and nodular,
extending to the base of the valve leaflets. There is
redundant tissue, resulting in prolapse into the LA. CT
are thickened and may rupture, resulting in mitral valve
flail. CT to the septal leaflet can also elongate.

Chronic MV DiseaseChronic MV Disease
LA Jet Lesions
• fibrous plaques in the endocardium in a region
subjected to the impact of the high velocity MR jet.
• Endomyocardial splits or tears may also be identified.
• On occasion, a full thickness left atrial tear occurs
resulting in hemopericardium, pericardial tamponade,
and usually death.
• Rarely, a full thickness endomyocardial tear will involve
the interatrial septum, causing an acquired atrial septal
defect.
(MR Client Handout) (ACVIM MVD Guidelines)

MVD in CavaliersMVD in Cavaliers
• Leading cause of death in Cavaliers
• CHF can develop as young as 1-3 years old
• First sign of disease is mitral murmur
– Careful annual auscultation
• Radiographs should be done as soon as murmur is
detected
– q6months when progressing
– annually for stable disease
– Sooner when respiratory rate exceeds 35-40 per minute
• Doppler Echo when abnormalities are present on rads

MVD in CavaliersMVD in Cavaliers
• The median survival period from grade III CHF due to
MVD is approximately seven months, with 75% of the
dogs dead by one year
• Current recommendation is that no Cavalier be bred
until after 5 years of age, with no murmur
• At this time, a majority of Cavaliers are affected
(Client Handout)

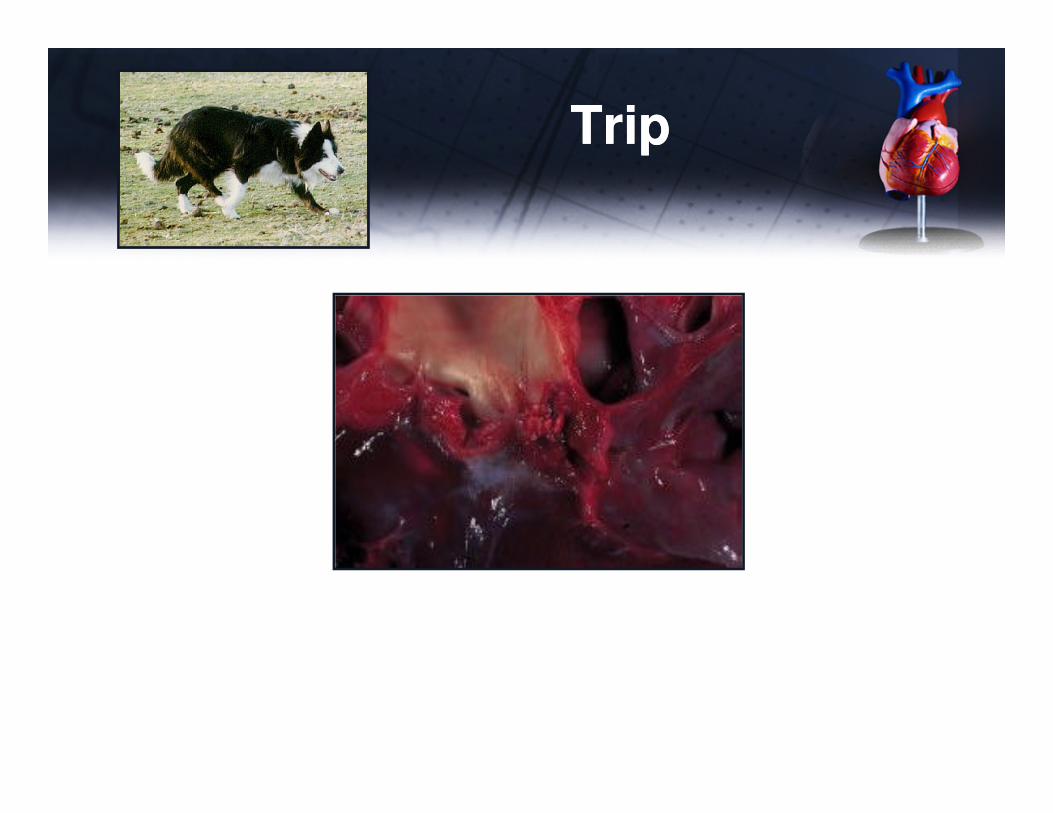
TripTrip
Signalment
• 2 year old castrated male border collie
Chief Complaint/History
• Productive Cough, weight loss for 2 months
• Breathing hard for a 2 days
• Energy good; did well in agility 4 days ago
• Owner thinks has had lifelong PU-PD
• Has wanted to be in AC this summer – unlike last summer when he enjoyed being outside
TripTrip
Exam
• T 102.2, P 168, R 42, CRT 3 sec
• BCS 2.5
• BP 100
• Bounding pulses, notable in dorsal pedal artery
• Precordial – exaggerated left apical heave
• Lung sounds clear

TripTrip
Exam
• 3 murmurs:
1. PMI left base (audio)
– To-and-fro murmur 3/6
– aortic stenosis in systole, regurg in diastole
2. PMI left apex, but heard all over chest (link)
– Holosystolic murmur 3/6
– Mitral regurgitation due to LHF
3. PMI Carotid artery (audio)
– 2/6 ejection murmur
– aortic stenosis

TripTrip
Differential Diagnoses
• Aortic endocarditis
• SAS with aortic regurgitation
• Mitral regurgitation (endocarditis?)
Diagnostic Plan
• Thoracic radiographs
• EKG
• Echocardiography

TripTrip
EKG
• Normal sinus rhythm for 10 minutes
TripTrip
EKG
• Normal sinus rhythm for 10 minutes
TripTrip
EKG
• Normal sinus rhythm for 10 minutes
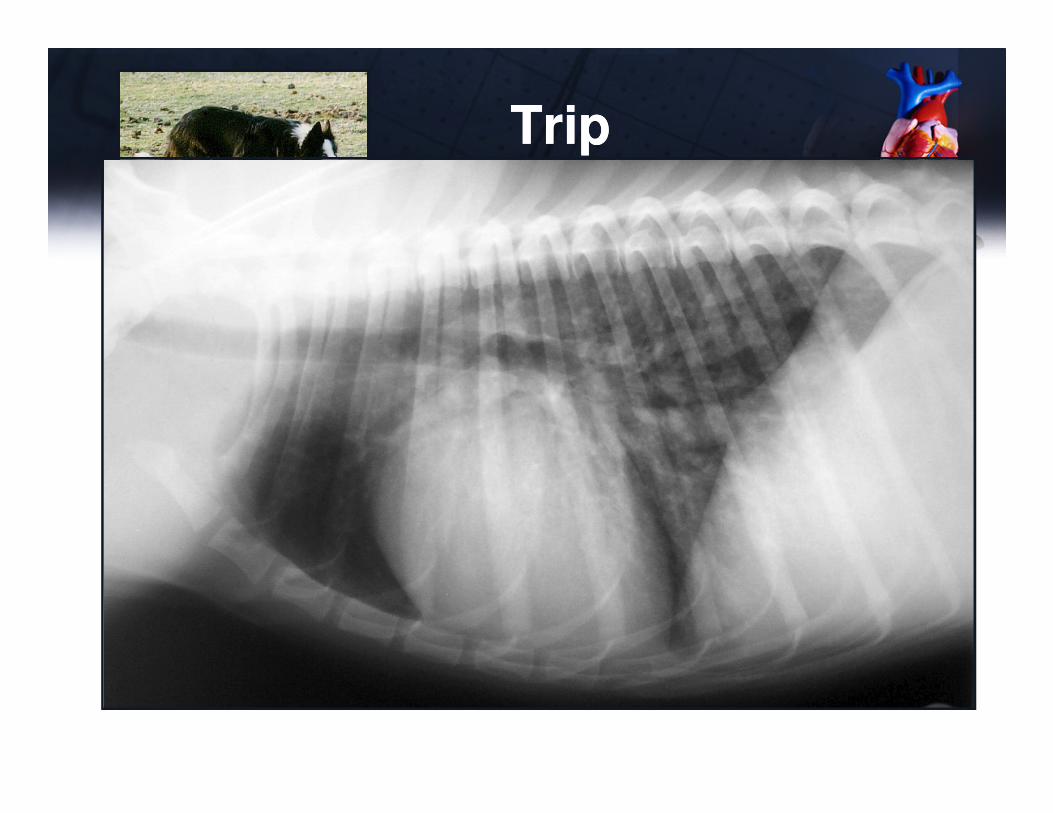
Thoracic Radiographs
• Interstitial pattern caudal lung fields
• Vertebral heart score 10.5
• Enlarged cranial pulmonary lobar vein
• Mildly enlarged left atrium
• Early left congestive heart failure

Trip - EchoTrip - Echo
Short Axis – LV Apex
• No abnormalities noted
Short Axis – LV PM

Trip - EchoTrip - Echo
Short Axis – LV Apex
• No abnormalities noted
Short Axis – LV PM

Trip - EchoTrip - Echo
Short Axis – LV Apex
• No abnormalities noted
Short Axis – LV PM
• LVIDD – 57.3 (n 31.3-34)
• IVSTS – 15.5 mm (n 12.6-13.7)
• LVIDS – 41.1 mm (18.8-20.7)
• FS = (57.3-41.1)/57.3 = 28% (n 30-46%)
• EF = 54% (n >70%)

Trip - EchoTrip - Echo
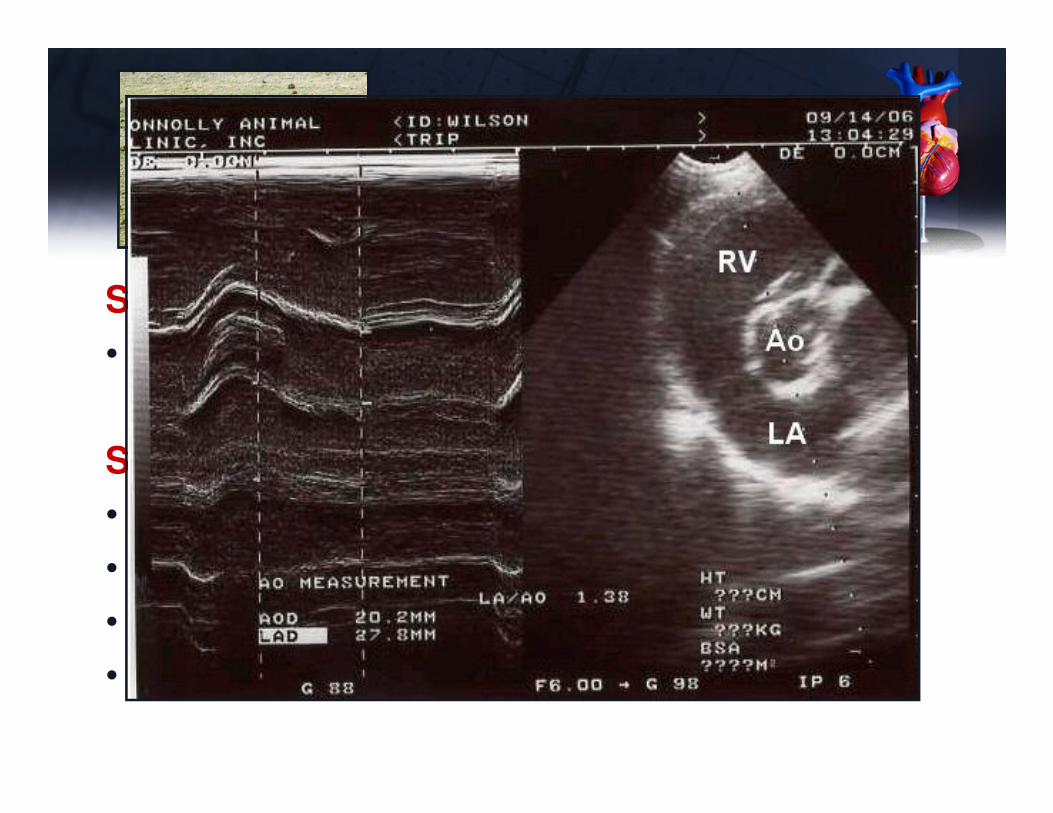
Short Axis – MV
• EPSS – 8 mm (n 0-6)
Short Axis – Ao/RVOT
• AoS – 20.2 (normal)
• LAD – 27.8 (n 19.0-20.5)
• LA/Ao – 27.8/20.2 = 1.38 (n 0.8-1.3)
• Aortic valve leaflets are hyperechoic
Trip - EchoTrip - Echo
Short Axis – MV
• EPSS – 8 mm (n 0-6)
Short Axis – Ao/RVOT
• AoS – 20.2 (normal)
• LAD – 27.8 (n 19.0-20.5)
• LA/Ao – 27.8/20.2 = 1.38 (n 0.8-1.3)
• Aortic valve leaflets are hyperechoic

Trip - EchoTrip - Echo
Short Axis – MV
• EPSS – 8 mm (n 0-6)
Short Axis – Ao/RVOT
• AoS – 20.2 (normal)
• LAD – 27.8 (n 19.0-20.5)
• LA/Ao – 27.8/20.2 = 1.38 (n 0.8-1.3)
• Aortic valve leaflets are hyperechoic

Trip - EchoTrip - Echo
Short Axis – PA
• No abnormalities noted
Long Axis – 4 Chamber

Trip - EchoTrip - Echo
Short Axis – PA
• No abnormalities noted
Long Axis – 4 Chamber

Trip - EchoTrip - Echo
Short Axis – PA
• No abnormalities noted
Long Axis – 4 Chamber
• LA appeared mildly enlarged
• IVS bowed anteriorly toward RV
• No evidence of mitral encodarditis or
endocardiosis
• Vegetation on aortic valve

Trip - EchoTrip - Echo

Trip - EchoTrip - Echo
Long Axis – LVOT (video)
• Hyperechoic thickened aortic valve leaflets
Diagnosis
• Aortic endocarditis
Therapeutic Plan
• Elected euthanasia due to poor prognosis
TripTrip

Valvular EndocarditisValvular Endocarditis
Clinical Features
• Present for FUO, weight loss or heart failure
• Aortic much more common than mitral
• Dogs much more common than cats
• Many bacteria including Bartonella
• Breed predisposition
– Rottweiler, Boxer, Golden retriever
– Newfoundland, German shepard

Valvular EndocarditisValvular Endocarditis
Clinical Features
• Abnormal valve + bacteremia = endocarditis
• Bacteremia caused routinely by:
– Dental cleaning
– Brushing your teeth (chewing)
– Constipation, any GI illness
– defecation
– Urinary catheterization
– infection

Valvular EndocarditisValvular Endocarditis
ECG abnormalities
• Tall, wide P wave (LA enlargement)
• Tall R wave (LV enlargement)
• Ventricular arrhythmias common– Treat if multiform of >30 per minute
– Class I or III antiarrhythmic
– Sotalol 2-3 mg/kg PO BID
Thoracic radiographs
• Left heart failure

Valvular EndocarditisValvular Endocarditis
ECG abnormalities
• Tall, wide P wave (LA enlargement)
• Tall R wave (LV enlargement)
• Ventricular arrhythmias common– Treat if multiform of >30 per minute
– Class I or III antiarrhythmic
– Sotalol 2-3 mg/kg PO BID
Thoracic radiographs
• Left heart failure

Valvular EndocarditisValvular Endocarditis
Echocardiographic abnormalities
• Thickened, hyperechoic valves
• Vegetation may flop around – MV in diastole, AV in systole
• Variable LV dilation (more with time)
• FS normal to low normal until myocardial failure
• MV endocarditis can be difficult to distinguish from MV endocardiosis – Endocarditis dogs are systemically ill

Valvular EndocarditisValvular Endocarditis
Treatment
• Based on urine and blood culture and sensitivity, Bartonella PCR
• Antibiotics– IV 3-5 days – broad spectrum until culture results
– SC/IM 3-5 days
– Then PO long term – often for life
• Treat Heart failure (severe)
• Treat ventricular arrhythmia if present
• Watch for and treat bacterial embolization of abdominal organs, skin, IVDiscs, CNS, joints, etc.
• Watch for and treat immune complex disease

Valvular EndocarditisValvular Endocarditis
Prognosis
• <20% survival
• Antibiotic therapy often required for life
• Median survival is 6 days from diagnosis for aortic
endocarditis
• Survival is longer for mitral endocarditis
– LHF due to MR not as severe as AoR
(Client Handout)

MaximusMaximus
18 month old male Boxer
Chief Complaint
• Drastic and rapid weight loss
• Not eating well
• Coughing up blood tinged fluid since yesterday
Exam, Chest rads, ECG
• Similar to Trip, except temp 103.8
• And BCS 2

MaximusMaximus
Diagnostics
• Blood culture
– negative (2 samples 2 hours apart)
• Urine culture– Enterobacter susceptible to all
• CBC
– neutrophilia 23,100/ul
– Mild anemia – PCV 35.5%

MaximusMaximus
Diagnostics
• General Health Profile, electrolytes
– BUN – 55 (n 10-29)
– ALT – 225 (n 10-120)
– Albumin – 2.2 (n 2.3-3.7)
• Urinalysis
– USG – 1.045
– WBC 7-10/hpf, rare bacteria seen

MaximusMaximus
Treatment (58 lbs, BCS 2, RR 66)
• Antibiotics
– IV - ampicillin 750 mg TID, Baytril 150 mg BID x 3 days
– IM – ampicillin 750 mg BID, Baytril 150 mg x 3 days
– PO – ampicillin 750 mg BID, Baytril 136 mg PO for life
• Furosemide
– 100 mg IV TID the first day - RR down to 28
– Then 75 mg PO BID
• Enalapril – 15 mg PO BID
• Pimobendan – 5 mg PO BID
MaximusMaximus
Treatment – Day 3 – RR 30, eating well
• Chest x-rays
– Pulmonary edema much improved, but mild amount
still present
• Continue Furosemide, Enalapril,
Pimobandan
• Added Spironolactone – 25 mg PO BID

MaximusMaximus
Diagnostics – Day 5 – RR 36, BP 150
• Chest x-rays - No change
• BUN – 43
• Electrolytes - normal
Treatment – Day 5
• Continue Furosemide, Enalapril, Pimobendan
• Spironolactone – increased to 50 mg PO BID
• Added Hydralazine – 12.5 mg PO BID

MaximusMaximus
Diagnostics – Day 10
RR 30, BP 135, Wt 61.8, Temp 103
• Chest x-rays – perihilar edema resolved
• BUN – 11, albumin 2.3
• Electrolytes – normal
• CBC – neutrophilia 23,000/ul
Continued this treatment for the rest of Max’s life – 3 months

SummarySummary
• PowerPoint – Cases – Valvular Disease
• .pdf of PowerPoint – Valvular Disease
• All Audio and Video Files
• ACVIM Position Statement on CHF
• Client Handouts– Endocarditis
– Valvular Dysplasia
– Congestive Heart Failure
– MVD in Cavaliers