Research ArticleManagement of Penetrating Skull Base Injury A SingleInstitutional Experience and Review of the Literature
Danfeng Zhang Jigang Chen Kaiwei Han Mingkun Yu and Lijun Hou
Department of Neurosurgery Shanghai Institute of Neurosurgery Shanghai Changzheng Hospital415 Fengyang Road Shanghai 200003 China
Correspondence should be addressed to Lijun Hou lijunhoucz126com
Received 7 May 2017 Accepted 18 June 2017 Published 30 July 2017
Academic Editor Hideo Inaba
Copyright copy 2017 Danfeng Zhang et alThis is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Background Penetrating skull base injury (PSBI) is uncommon among head injuries presenting unique diagnostic and therapeuticchallenges Although many cases of PSBIs have been reported comprehensive understanding of its initial diagnosis managementand outcome is still unavailableMaterials andMethodsA retrospective review was performed for patients treated in neurosurgicaldepartment of Changzheng Hospital for PSBIs Presurgical three-dimensional (3D) Slicer-assisted reconstructions were conductedfor each patient Then we reviewed previous literature about all the published cases of PSBIs worldwide and discussed theircommon features Results A total of 5 patients suffering PSBIs were identified Penetrating points as well as the surroundingneurovascular structures were clearly visualized assisting in the presurgical planning of optimal surgical approach and avoidingunexpected vascular injury Four patients underwent craniotomy with foreign bodies removed successfully and 1 patient receivedconservative treatment All of them presented good outcomes after proper management Conclusion Careful physical examinationand radiological evaluation are essential before operation and angiography is recommended for those with suspected vascularinjuries 3D modeling with 3D Slicer is practicable and reliable facilitating the diagnosis and presurgical planning Treatmentdecision should be made upon the comprehensive evaluation of patientrsquos clinicoradiological features and characteristics of foreignbodies
1 Introduction
Penetrating injuries of the skull base caused by foreignbodies are relatively uncommon representing about 04of head injuries [1 2] Various foreign bodies have beenreported in penetrating skull base injuries (PSBIs) includingwood bamboo metallic fragments and toothbrushes PSBIscould present unique diagnostic and therapeutic challengesPatients may be initially asymptomatic but subject to seriousevents for several daysmonths or even years after the injuries[3] It is not difficult to detect most of intracranial foreignbodies by head computed tomography (CT) scan Howeverthe relationships between foreign bodies and its surroundingstructures are hard to decide which is the prerequisite for themanagement of these injuries [4 5]
Treatment for PSBIs includes the surgical retractionof foreign bodies prevention of infection management ofvascular injuries reconstruction of skull base and so forth [35ndash7] Due to the low incidence there is no sufficient literature
about the diagnosis and management of these patients Theaim of our study is to present patients of PSBIs treated in ourdepartment and review related literature in order to highlightthe proper management of PSBIs and improve prognosis inthe long run
2 Materials and Methods
A retrospective review was conducted for patients who weretreated in our hospital between January 2010 and September2016 for PSBIs This study was performed in accordancewith the Declaration of Helsinki (1964) and approved bythe investigational review board of Changzheng HospitalInformed consent was available for each patient Presurgicalhead CT scans were performed for all patients Moreoverdigital subtraction angiography (DSA) was conducted onsuspicion of vascular injuries and magnetic resonance imag-ing (MRI) was performed in case of nonmetallic objectsData concerning patientsrsquo demographics mechanisms of
HindawiBioMed Research InternationalVolume 2017 Article ID 2838167 12 pageshttpsdoiorg10115520172838167
2 BioMed Research International
injury medical managements complications and prognosiswere collected by two authors (D F Zhang and J G Chen)
In order to visualize the location of foreign body and itsrelationship with surrounding structures three-dimensional(3D) Slicer-assisted reconstructions were conducted by aprofessional neuroradiologist (K W Han) according topresurgical imaging data During the reconstruction all theDigital Imaging andCommunications inMedicine (DICOM)images were imported into 3D Slicer (3D Slicer 40sim44Surgical Planning Laboratory Harvard University USA)Segmentation of skull foreign body and cerebral artery wasfirst performed with built-in modules in Slicer Individualmodels of each structure were created which could berotated and viewed from any perspective (Figure 1(g) Figures2(g)ndash2(i) Figure 3(g))
3 Results
A total of 5 patients with PSBIs were identified There were4 males and 1 female aged 29ndash75 years They were all victimsof tumble or work-related accident Four of them underwentsurgical retrieval of foreign bodies and 1 patient receivedconservative treatment Penetrating points as well as thesurrounding neurovascular structures were clearly visualizedin 3Dmodels assisting in the presurgical planning of optimalsurgical approach and avoiding unexpected vascular injuryDetails regarding patientsrsquo demographics locations of foreignbodies and treatment were listed in Table 1
31 Representative Case 1 This 75-year-old female wasadmitted to her local hospital with complaints of headacheand dizziness for 3 days She was conscious and neurologi-cally intact with a slightly elevated body temperature HeadCT scan revealed a low density 4 cm long foreign bodyextending from the left orbit to superior orbital fissure andposteriorly to the left temporal lobe (Figures 1(a)ndash1(c)) Braintissue surrounding the foreign body was swollen and signsof abscess were indicated (Figures 1(d)ndash1(f)) The patientrecalled that while she was walking in a bamboo gardenshe tripped and fell forward striking her left forehead ona bamboo stick She did not feel any discomfort except thepain on her left upper eyelid Symptoms of headache andfever emerged 5 days later and she was taken to the hospitalby her family 8 days after the injury Anti-infective therapieswere given before she was transferred to our hospital Carefulphysical examination revealed a slight skin scar on her leftupper eyelid Head DSA was performed later with no signsof vascular injuries although the bamboo stick was adjacentto the left middle cerebral artery (MCA) in the 3D recon-struction model (Figure 1(g)) Anti-infectious treatment wasadministrated for 12 days to control the brain abscess beforesurgery During operation an orbitozygomatic approach wasadopted and the pterional craniotomy was first performedThen superior orbital fissure was revealed after removing thegreat wing of sphenoid We explored the abscess in the tem-poral lobe After yellowish pus in the abscess was removedthe distal end of the bamboo stick was then visualized Weopened the dura and orbital fascia along the bamboo stickto expose its full length (Figure 1(h)) The stick was removed
completely under direct visualization (Figure 1(i)) and durawas sutured in a water tight fashionThe postoperative coursewas uncomplicated Broad-spectrum antibiotics were givenuntil she was discharged free of symptoms 10 days afteroperation
32 Representative Case 2 This 32-year-old man was hit bythe fragments of a burst grinding wheel on his left cheekduring working hours He was taken to the local hospitalcomplaining of headache and kept neurologically intact onphysical examination Head CT scan suggested a short pieceof metal fragment locating right between the left maxillaryand ramimandibulae and a long piece sticking in the left tem-poral lobe Both pieces presented to be highly dense on theCT scan (Figures 2(a)ndash2(c))The patient was then transferredto our department for further treatment 5 days later DSAsuggested no obvious vascular injury (Figures 2(d) and 2(e))while axial CT scan revealed close relationship between thebone fragment and branch of MCA (Figure 2(f)) The exactlocation of foreign body could be visualized clearly on the3D reconstruction model (Figures 2(g)ndash2(i)) Conservativemanagement was given to control the infection and surgerywas performed 15 days after the injury During operationshort piece of the foreign body was first removed through anintraoral incision Then a temporozygomatic approach wasperformed to remove the long piece which was visualized atthe infratemporal fossa after the zygomatic archwas detachedand retracted downwardly with temporal muscle Severalpieces of bone fragment were found around the foreign bodyAfter the lateral portion of infratemporal fossa was drilledoff the object was removed in a retrograde fashion Duringthis process yellowish pus was drained into infratemporalfossa through the intracranial trajectory of foreign bodyThis trajectory was not explored and defect of dura wassealed with muscle flap (Figures 3(a)ndash3(e)) Postoperativeskull radiography showed complete removal of the foreignbody (Figure 3(f)) A small bone fragment was left in placedue to its close relationship with branch of MCA whichwas found to be stenotic during follow-up (Figure 3(g)) Thepatient was discharged 1 week after operation with sporadicfocal epilepsy which was controlled well with carbamazepineand he recovered well without abscess formation at three-month follow-up (Figures 3(h) and 3(i))
4 Discussion
41 Literature Review Clinicoradiological features of PSBIsin previous literatures were reviewed and summarized inTable 2 [2 3 8ndash24] Most of the subjects were males (662132) with an average age of 24 years old 41 (1332) ofthe patients were children under 10 years of age As for themechanism of injury children injuries were all caused bytumbling or falling while the injury of 4 adults resultedfrom suicidal or homicidal attempt which was absent in ourcase series The most common foreign body was metallic(1232) followed by wooden (932) and plastic (932) Onepatient was injured by a wild deerrsquos antler and another onewas attacked by bear paws both of which had no retainedforeign bodies As a weak area of skull the orbit was the most
BioMed Research International 3
(a)
(a)
(b)
(b)
(c)
(c)
(d)
(d)
(e)
(e)
(f)
(f)
(g)
(g)
f
to
(h)
(h)
(i)
(i)
Figure 1 Head CT scan demonstrated a bamboo stick (hollow arrow) penetrating into the temporal lobe via superior orbital fissure Thebamboo stick presented as high density on the CT scan (a b c) Contrast enhanced MRI revealed an abscess (simple arrowlarr) around thebamboo stick in temporal lobe (d e f) 3D reconstruction of the skull cerebral artery and bamboo stick (hollow arrow ) was performedby 3D Slicer software to visualize the relationship among these structures (g) Intraoperative photography (h) displayed the bamboo stick inoriginal place (o orbital side f frontal side t temporal side) Photography showed the removed bamboo stick (i) 3D three-dimensional CTcomputed tomography MRI magnetic resonance imaging
common penetrating point followed by oral or nasal cavityand maxillofacial region
42 Diagnosis of PSBIs After careful physical examinationproper radiological examination on the basis of patientsrsquocondition is necessary Although the importance of head CTscan in the management of PSBIs has been emphasized in
previous literatures several instructions should be noticedFirstly the density of foreign bodies on CT scan variesaccording to their types For example metal presents as highdensity while wood or plastics are of isodensity or lowdensityand difficult to identify Secondly the density of some foreignbodies would change over time For example bamboo is oflow density on initial CT scan but it would be of high density
4 BioMed Research International
(a)
(a)
(b)
(b)
(c)
(c)
(d)
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 2 Preoperative image of foreign body (burst outer rim of a grinding wheel) in the face andmiddle skull base Anterior-posterior skullradiography (a) and lateral skull radiography (b) demonstrated the short piece (simple arrowlarr) in the face and long piece (hollow arrow) penetrating into the middle skull base Sagittal reconstruction of CT (c) showed the long piece penetrating into the middle cranial fossathrough infratemporal fossa A small piece of bone fragment (hollow arrowhead ) was noticed above the long piece The bone fragmentarose from the hit of the long piece on the middle skull base DSA (d amp e) proved the integrity of MCA Axial CT revealed close relationshipbetween the bone fragment (hollow arrow head ) and branch of MCA (f) 3D reconstruction (g h i) with 3D Slicer software displayedspatial correlation of two pieces of foreign body with the face and skull base 3D three-dimensional CT computed tomography DSA digitalsubtraction angiography MCA middle cerebral artery
later which frequently leads to misdiagnosis (Case 1) [25]Therefore MRI is a useful supplement to CT in the detectionof nonmetallic foreign bodies
Angiography such as the CT angiography MR angiogra-phy or DSA is highly recommended for patients in suspicion
of artery injuries or traumatic aneurysms [7 26 27] Asdemonstrated in Case 2 foreign bodies may not causeimmediate vascular injury sometimes but lead to cerebralvasospasm or stenosis in the long run highlighting theimportance of angiography in the setting of PSBIs
BioMed Research International 5
Table1Dem
ograph
icsa
ndclinicald
atafor
patie
ntso
fPSB
I
Case
Age
and
gend
erMechanism
ofinjury
Type
andsiz
eof
foreign
body
Penetrating
pathway
Symptom
sand
concurrent
cond
ition
s
DSA
finding
s
Interval
toop
eration
Operatio
nSurgicalapproach
Resid
ual
fractio
nAntibioticsu
sed
Symptom
sat
discharge
175fe
male
Accident
Bambo
o7c
m
Left
orbit-s
uperior
orbital
fissure-anterior
skullbase-left
tempo
rallob
e
Headache
dizzinessbrain
abscess
Negative
20days
Yes
Orbito
zygomatic
approach
and
pterional
craniotomy
No
Metronidazole
cefta
zidime
vancom
ycin
linezolid
biapenem
Free
ofsymptom
232m
ale
Accident
Grin
ding
wheel
65c
m
Leftmaxilla-
infratem
poral
fossa-middle
cranialfossa
ciste
rnof
lateral
sulcus
Headachebrain
abscess
Negative
19days
Yes
Tempo
rozygomatic
approach
No
Linezolid
Epilepsy
342m
ale
Accident
Electro
drill
22c
m
Lefteyebrow-
anterio
rcranial
base-le
ftfro
ntal
lobe
Headache
cerebral
contusion
Not
cond
ucted
No
operation
No
mdashYes
Linezolid
biapenem
Slight
headache
429m
ale
Accident
Screw
54c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blurredvisio
nanterio
rsku
llbase
fracture
oculom
otor
nerveinjury
Not
cond
ucted
2days
Yes
Fron
totempo
ral
approach
No
Vancom
ycin
linezolid
Improved
visio
noculom
otor
nerve
injury
540
male
Accident
Hot
projectiv
eoil
paint34c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blindn
essrig
hteyep
enetratin
ginjuryfrontal
hematom
a
Not
cond
ucted
4days
Yes
Subfrontal
approach
Yes
Vancom
ycin
ceftriaxone
B lindn
ess
6 BioMed Research International
Table2Clinicoradiologicalfeatureso
fpreviou
slyrepo
rted
caseso
fPSB
I
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Matsumotoet
al1998
3female
Left3c
mPlastic
chop
stick
Falling
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Matsumotoet
al1998
57m
ale
Right2
cmWoo
den
chop
stick
Stickinto
chop
stick
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Hebecker2009
32m
ale
Leftno
foreign
body
Wild
deerrsquos
antler
Accident
Leftorbit
floorla
teral
orbit
Com
aBifro
ntalintradural
neurosurgical
approach
No
Free
ofsymptom
Ishikawae
tal
2000
4male
Left6c
mWoo
den
chop
stick
Falling
Preauricular
area
topo
sterio
rfossa
Feverheadache
Subo
ccipita
lcraniectom
yBrainabscess
Ataxiaand
dysm
etria
Matsuyamae
tal2001
1male
Right2
5cm
Woo
den
chop
sticks
Falling
Superio
rorbita
lfissure
Swolleneye
Transcranial
approach
Meningitis
Free
ofsymptom
Maruyae
tal
2002
56fe
male
Left1cm
Bambo
oTu
mbling
Tempo
ral
(lateralorbit)
Drowsin
ess
Left
frontotem
poral
craniotomyand
orbitozygomatic
osteotom
y
No
Lateralgazein
theleft
eye
Hayashi
etal
2003
71fe
male
Rightn
oforeign
body
Bear
claws
Animal
assault
Fron
talsinus
Laceratedface
CSFfistulas
Fron
tal
craniectom
iesto
repairCS
Ffistulas
No
Free
ofsymptom
Nish
ioetal
2004
6female
Right2
5cm
Woo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Feverheadache
neck
stiffn
ess
Craniotomy
Brainabscess
Fre e
ofsymptom
Kim
etal2005
1male
Right2
cmMetallic
chop
stick
Falling
Fron
tal(orbital
roof)
Crying
Craniotomy
No
Free
ofsymptom
Tsao
etal2006
45m
ale
Left25c
mlowast
25c
mPlastic
chair
glide
Beassaulted
Sino
nasalcavity
anterio
rsku
llbase
Ptosis
impaire
dvisio
n
Transnasal
endo
scop
icexplorationand
removalof
the
foreignbo
dy
No
Ano
smiaand
diplop
ia
DeT
ommasiet
al2006
20m
ale
Right10c
mScrewdriver
Falling
Rightm
axilla
Scotom
ainthe
lefteyeCS
Fleakage
Leftpterional
approach
NK
Resto
redvisio
n
Park200
69female
RightN
KWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
No
Free
ofsymptom
Park200
61m
ale
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gleft
hemiparesis
NK
No
Leftmild
hemiparesis
Park200
65male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
BioMed Research International 7Ta
ble2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Park200
62male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
Nitsch
etal
2007
22m
ale
Right2
cmNail-g
unAc
cident
Rightu
pper
jaw
totempo
rallob
eIntracerebral
haem
atom
a
Simplee
xtraction
ofthen
ailw
ithou
tac
raniotom
yNK
NK
Hira
ishi2007
5female
Left35c
mPlastic
chop
stick
Falling
Fron
tal(orbital
medial)
Feverheadache
neck
stiffn
ess
Craniotomy
Meningitis
brainabscess
Hyposmia
Kawada2009
5female
Left3c
mWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
Brainabscess
Free
ofsymptom
Mitilian
2009
4male
Right11cm
Woo
den
chop
stick
Falling
Superio
rorbita
lfissure
Mild
confusion
vomiting
Craniotomy
Brainabscess
Mild
dysm
etria
ofthea
rm
Wieland
etal
2010
58m
ale
Left-sid
edN
KWoo
denstick
Accident
Maxillofacialto
ethm
oidroof
Feverheadache
nausea
vomiting
mentalstatus
changes
Endo
scop
icrepair
ofthes
kullbase
defect
Intracranial
infection
NK
Hettig
eetal
2010
38fe
male
LeftNK
Plastic
chop
stick
Stum
ble
Poste
riorw
allof
theo
roph
aryn
xto
jugu
lar
foramen
into
the
poste
riorfossa
Nystagm
usleft
9th10thand
12th
cranial
nerves
palsy
qu
adrantanop
ia
Leftoccipital
craniotomy
retro
sigmoid
craniectom
y
No
Left9th10th
and12th
cranial
nerves
palsy
Sweeneyetal
2011
31m
ale
RightN
KKn
ifeSuicidal
attempt
Lower
jawto
anterio
rsku
llbase
Pain
Com
binedrig
htpte rionaland
interhem
ispheric
craniotomies
No
NK
Sweeneyetal
2011
21fe
male
RightN
KKn
ifeHom
icidal
attempt
Leftorbitto
middles
kull
base
Emesis
seizure
Leftcranioor-
bitozygomatic
approach
No
NK
Yonezawa2011
28m
ale
LeftNK
Plastic
chop
stick
Falling
Fron
tal(orbital
medial)
NK
Craniotomy
No
Free
ofsymptom
Arslanetal
2012
13m
ale
Right18c
mIron
bar
Falling
Righto
rbitand
superio
rorbita
lfissure
Com
a(GCS
3)Right
frontop
arietal
craniotomy
No
Died
Shin
etal2012
38m
ale
Left14cm
Plastic
chop
stick
Falling
Superio
rorbita
lfissure
Blindn
ess
swellin
gnu
mbn
ess
arou
ndeye
Removalof
chop
stick
with
out
craniotomy
No
Blindn
ess
Katayamae
tal
2013
18m
ale
Right12c
mMetalrod
Falling
Fron
tal
(sub
zygomatic
bone)
Vomiting
NK
NK
Noneurological
deficit
Wangetal2013
35m
ale
Left18cm
Steel
Falling
Leftmaxillary
sinus
Limited
movem
ento
fneck
Craniotomy
No
Leftfacialpalsy
8 BioMed Research International
Table2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Skochetal2
013
35fe
male
MedialN
KElectric
toothb
rush
Accident
Tempo
ral
(lateralorbit)
Blurredvisio
npain
Mod
ified
frontotem
poral
orbitozygomatic
craniotomy
No
Improved
pain
andvisio
n
Deveere
tal
2013
43m
ale
Right5
6cm
Plastic
pen
Falling
Righto
rbit
No
NK
No
Free
ofsymptom
Yamasakietal
2013
4female
Left65c
mplastic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gNK
Meningitis
enceph
alitis
Free
ofsymptom
Williamse
tal
2014
56m
ale
LeftNK
Speargun
Suicidal
attempt
Subm
andibu
lar
region
oral
cavity
Com
aLargec
raniotom
yCerebritis
Died
ACAA
nteriorC
erebralA
rteryCS
FCerebrospinalFluidGCS
Glasgow
Com
aScaleICA
internalcarotid
arteryN
Kno
tkno
wn
BioMed Research International 9
(a)
(a)
(b)
(b)
(c)
(c)
(d)
lowast
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 3 Photography showed the entry point (black triangle 998787) of foreign body on face and incision for a frontotemporoorbitozygomaticapproach (a) Short piece of foreign body (simple arrow larr) in the face was exposed and removed by a maxillofacial surgeon (b) Theinfratemporal fossa was opened to expose the long piece of foreign body (c) and it (hollow arrow) was removed in a retrograde fashionDuring the removing process yellowish pus (asterisk lowast) was drained into the infratemporal fossa (d) Photography displayed short piece(simple arrowlarr) and long piece (hollow arrow) of the foreign body (e) Postoperative skull radiography suggested complete removal ofthe foreign body (f) The small bone fragment (hollow arrow head) was left in place due to its close relationship with branch of MCA (g)Three-month follow-up MRI revealed no abscess formation (h) The patient recovered uneventfully (i) MCA middle cerebral artery MRImagnetic resonance imaging
3D modeling has been frequently used in the presurgicalplanning of PSBIs in previous studies [8 11 15ndash17 19 2324 28] 3D models can be viewed in 360 degrees rotatedand studied from any perspective [29ndash31] which facilitate thediagnosis and operation to some extent [30 31] 3D Slicer is afree open source software that can be used for segmentation
and 3D modeling with high accuracy and reliability [30 32]It has been used in the management of various diseasesincluding intracranial aneurysms trigeminal neuralgia andintracerebral hematomas [29 30 33] PSBIs in our case serieswere reconstructed using 3D Slicer in which penetratingpoints as well as the surrounding neurovascular structures
10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014

2 BioMed Research International
injury medical managements complications and prognosiswere collected by two authors (D F Zhang and J G Chen)
In order to visualize the location of foreign body and itsrelationship with surrounding structures three-dimensional(3D) Slicer-assisted reconstructions were conducted by aprofessional neuroradiologist (K W Han) according topresurgical imaging data During the reconstruction all theDigital Imaging andCommunications inMedicine (DICOM)images were imported into 3D Slicer (3D Slicer 40sim44Surgical Planning Laboratory Harvard University USA)Segmentation of skull foreign body and cerebral artery wasfirst performed with built-in modules in Slicer Individualmodels of each structure were created which could berotated and viewed from any perspective (Figure 1(g) Figures2(g)ndash2(i) Figure 3(g))
3 Results
A total of 5 patients with PSBIs were identified There were4 males and 1 female aged 29ndash75 years They were all victimsof tumble or work-related accident Four of them underwentsurgical retrieval of foreign bodies and 1 patient receivedconservative treatment Penetrating points as well as thesurrounding neurovascular structures were clearly visualizedin 3Dmodels assisting in the presurgical planning of optimalsurgical approach and avoiding unexpected vascular injuryDetails regarding patientsrsquo demographics locations of foreignbodies and treatment were listed in Table 1
31 Representative Case 1 This 75-year-old female wasadmitted to her local hospital with complaints of headacheand dizziness for 3 days She was conscious and neurologi-cally intact with a slightly elevated body temperature HeadCT scan revealed a low density 4 cm long foreign bodyextending from the left orbit to superior orbital fissure andposteriorly to the left temporal lobe (Figures 1(a)ndash1(c)) Braintissue surrounding the foreign body was swollen and signsof abscess were indicated (Figures 1(d)ndash1(f)) The patientrecalled that while she was walking in a bamboo gardenshe tripped and fell forward striking her left forehead ona bamboo stick She did not feel any discomfort except thepain on her left upper eyelid Symptoms of headache andfever emerged 5 days later and she was taken to the hospitalby her family 8 days after the injury Anti-infective therapieswere given before she was transferred to our hospital Carefulphysical examination revealed a slight skin scar on her leftupper eyelid Head DSA was performed later with no signsof vascular injuries although the bamboo stick was adjacentto the left middle cerebral artery (MCA) in the 3D recon-struction model (Figure 1(g)) Anti-infectious treatment wasadministrated for 12 days to control the brain abscess beforesurgery During operation an orbitozygomatic approach wasadopted and the pterional craniotomy was first performedThen superior orbital fissure was revealed after removing thegreat wing of sphenoid We explored the abscess in the tem-poral lobe After yellowish pus in the abscess was removedthe distal end of the bamboo stick was then visualized Weopened the dura and orbital fascia along the bamboo stickto expose its full length (Figure 1(h)) The stick was removed
completely under direct visualization (Figure 1(i)) and durawas sutured in a water tight fashionThe postoperative coursewas uncomplicated Broad-spectrum antibiotics were givenuntil she was discharged free of symptoms 10 days afteroperation
32 Representative Case 2 This 32-year-old man was hit bythe fragments of a burst grinding wheel on his left cheekduring working hours He was taken to the local hospitalcomplaining of headache and kept neurologically intact onphysical examination Head CT scan suggested a short pieceof metal fragment locating right between the left maxillaryand ramimandibulae and a long piece sticking in the left tem-poral lobe Both pieces presented to be highly dense on theCT scan (Figures 2(a)ndash2(c))The patient was then transferredto our department for further treatment 5 days later DSAsuggested no obvious vascular injury (Figures 2(d) and 2(e))while axial CT scan revealed close relationship between thebone fragment and branch of MCA (Figure 2(f)) The exactlocation of foreign body could be visualized clearly on the3D reconstruction model (Figures 2(g)ndash2(i)) Conservativemanagement was given to control the infection and surgerywas performed 15 days after the injury During operationshort piece of the foreign body was first removed through anintraoral incision Then a temporozygomatic approach wasperformed to remove the long piece which was visualized atthe infratemporal fossa after the zygomatic archwas detachedand retracted downwardly with temporal muscle Severalpieces of bone fragment were found around the foreign bodyAfter the lateral portion of infratemporal fossa was drilledoff the object was removed in a retrograde fashion Duringthis process yellowish pus was drained into infratemporalfossa through the intracranial trajectory of foreign bodyThis trajectory was not explored and defect of dura wassealed with muscle flap (Figures 3(a)ndash3(e)) Postoperativeskull radiography showed complete removal of the foreignbody (Figure 3(f)) A small bone fragment was left in placedue to its close relationship with branch of MCA whichwas found to be stenotic during follow-up (Figure 3(g)) Thepatient was discharged 1 week after operation with sporadicfocal epilepsy which was controlled well with carbamazepineand he recovered well without abscess formation at three-month follow-up (Figures 3(h) and 3(i))
4 Discussion
41 Literature Review Clinicoradiological features of PSBIsin previous literatures were reviewed and summarized inTable 2 [2 3 8ndash24] Most of the subjects were males (662132) with an average age of 24 years old 41 (1332) ofthe patients were children under 10 years of age As for themechanism of injury children injuries were all caused bytumbling or falling while the injury of 4 adults resultedfrom suicidal or homicidal attempt which was absent in ourcase series The most common foreign body was metallic(1232) followed by wooden (932) and plastic (932) Onepatient was injured by a wild deerrsquos antler and another onewas attacked by bear paws both of which had no retainedforeign bodies As a weak area of skull the orbit was the most
BioMed Research International 3
(a)
(a)
(b)
(b)
(c)
(c)
(d)
(d)
(e)
(e)
(f)
(f)
(g)
(g)
f
to
(h)
(h)
(i)
(i)
Figure 1 Head CT scan demonstrated a bamboo stick (hollow arrow) penetrating into the temporal lobe via superior orbital fissure Thebamboo stick presented as high density on the CT scan (a b c) Contrast enhanced MRI revealed an abscess (simple arrowlarr) around thebamboo stick in temporal lobe (d e f) 3D reconstruction of the skull cerebral artery and bamboo stick (hollow arrow ) was performedby 3D Slicer software to visualize the relationship among these structures (g) Intraoperative photography (h) displayed the bamboo stick inoriginal place (o orbital side f frontal side t temporal side) Photography showed the removed bamboo stick (i) 3D three-dimensional CTcomputed tomography MRI magnetic resonance imaging
common penetrating point followed by oral or nasal cavityand maxillofacial region
42 Diagnosis of PSBIs After careful physical examinationproper radiological examination on the basis of patientsrsquocondition is necessary Although the importance of head CTscan in the management of PSBIs has been emphasized in
previous literatures several instructions should be noticedFirstly the density of foreign bodies on CT scan variesaccording to their types For example metal presents as highdensity while wood or plastics are of isodensity or lowdensityand difficult to identify Secondly the density of some foreignbodies would change over time For example bamboo is oflow density on initial CT scan but it would be of high density
4 BioMed Research International
(a)
(a)
(b)
(b)
(c)
(c)
(d)
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 2 Preoperative image of foreign body (burst outer rim of a grinding wheel) in the face andmiddle skull base Anterior-posterior skullradiography (a) and lateral skull radiography (b) demonstrated the short piece (simple arrowlarr) in the face and long piece (hollow arrow) penetrating into the middle skull base Sagittal reconstruction of CT (c) showed the long piece penetrating into the middle cranial fossathrough infratemporal fossa A small piece of bone fragment (hollow arrowhead ) was noticed above the long piece The bone fragmentarose from the hit of the long piece on the middle skull base DSA (d amp e) proved the integrity of MCA Axial CT revealed close relationshipbetween the bone fragment (hollow arrow head ) and branch of MCA (f) 3D reconstruction (g h i) with 3D Slicer software displayedspatial correlation of two pieces of foreign body with the face and skull base 3D three-dimensional CT computed tomography DSA digitalsubtraction angiography MCA middle cerebral artery
later which frequently leads to misdiagnosis (Case 1) [25]Therefore MRI is a useful supplement to CT in the detectionof nonmetallic foreign bodies
Angiography such as the CT angiography MR angiogra-phy or DSA is highly recommended for patients in suspicion
of artery injuries or traumatic aneurysms [7 26 27] Asdemonstrated in Case 2 foreign bodies may not causeimmediate vascular injury sometimes but lead to cerebralvasospasm or stenosis in the long run highlighting theimportance of angiography in the setting of PSBIs
BioMed Research International 5
Table1Dem
ograph
icsa
ndclinicald
atafor
patie
ntso
fPSB
I
Case
Age
and
gend
erMechanism
ofinjury
Type
andsiz
eof
foreign
body
Penetrating
pathway
Symptom
sand
concurrent
cond
ition
s
DSA
finding
s
Interval
toop
eration
Operatio
nSurgicalapproach
Resid
ual
fractio
nAntibioticsu
sed
Symptom
sat
discharge
175fe
male
Accident
Bambo
o7c
m
Left
orbit-s
uperior
orbital
fissure-anterior
skullbase-left
tempo
rallob
e
Headache
dizzinessbrain
abscess
Negative
20days
Yes
Orbito
zygomatic
approach
and
pterional
craniotomy
No
Metronidazole
cefta
zidime
vancom
ycin
linezolid
biapenem
Free
ofsymptom
232m
ale
Accident
Grin
ding
wheel
65c
m
Leftmaxilla-
infratem
poral
fossa-middle
cranialfossa
ciste
rnof
lateral
sulcus
Headachebrain
abscess
Negative
19days
Yes
Tempo
rozygomatic
approach
No
Linezolid
Epilepsy
342m
ale
Accident
Electro
drill
22c
m
Lefteyebrow-
anterio
rcranial
base-le
ftfro
ntal
lobe
Headache
cerebral
contusion
Not
cond
ucted
No
operation
No
mdashYes
Linezolid
biapenem
Slight
headache
429m
ale
Accident
Screw
54c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blurredvisio
nanterio
rsku
llbase
fracture
oculom
otor
nerveinjury
Not
cond
ucted
2days
Yes
Fron
totempo
ral
approach
No
Vancom
ycin
linezolid
Improved
visio
noculom
otor
nerve
injury
540
male
Accident
Hot
projectiv
eoil
paint34c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blindn
essrig
hteyep
enetratin
ginjuryfrontal
hematom
a
Not
cond
ucted
4days
Yes
Subfrontal
approach
Yes
Vancom
ycin
ceftriaxone
B lindn
ess
6 BioMed Research International
Table2Clinicoradiologicalfeatureso
fpreviou
slyrepo
rted
caseso
fPSB
I
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Matsumotoet
al1998
3female
Left3c
mPlastic
chop
stick
Falling
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Matsumotoet
al1998
57m
ale
Right2
cmWoo
den
chop
stick
Stickinto
chop
stick
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Hebecker2009
32m
ale
Leftno
foreign
body
Wild
deerrsquos
antler
Accident
Leftorbit
floorla
teral
orbit
Com
aBifro
ntalintradural
neurosurgical
approach
No
Free
ofsymptom
Ishikawae
tal
2000
4male
Left6c
mWoo
den
chop
stick
Falling
Preauricular
area
topo
sterio
rfossa
Feverheadache
Subo
ccipita
lcraniectom
yBrainabscess
Ataxiaand
dysm
etria
Matsuyamae
tal2001
1male
Right2
5cm
Woo
den
chop
sticks
Falling
Superio
rorbita
lfissure
Swolleneye
Transcranial
approach
Meningitis
Free
ofsymptom
Maruyae
tal
2002
56fe
male
Left1cm
Bambo
oTu
mbling
Tempo
ral
(lateralorbit)
Drowsin
ess
Left
frontotem
poral
craniotomyand
orbitozygomatic
osteotom
y
No
Lateralgazein
theleft
eye
Hayashi
etal
2003
71fe
male
Rightn
oforeign
body
Bear
claws
Animal
assault
Fron
talsinus
Laceratedface
CSFfistulas
Fron
tal
craniectom
iesto
repairCS
Ffistulas
No
Free
ofsymptom
Nish
ioetal
2004
6female
Right2
5cm
Woo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Feverheadache
neck
stiffn
ess
Craniotomy
Brainabscess
Fre e
ofsymptom
Kim
etal2005
1male
Right2
cmMetallic
chop
stick
Falling
Fron
tal(orbital
roof)
Crying
Craniotomy
No
Free
ofsymptom
Tsao
etal2006
45m
ale
Left25c
mlowast
25c
mPlastic
chair
glide
Beassaulted
Sino
nasalcavity
anterio
rsku
llbase
Ptosis
impaire
dvisio
n
Transnasal
endo
scop
icexplorationand
removalof
the
foreignbo
dy
No
Ano
smiaand
diplop
ia
DeT
ommasiet
al2006
20m
ale
Right10c
mScrewdriver
Falling
Rightm
axilla
Scotom
ainthe
lefteyeCS
Fleakage
Leftpterional
approach
NK
Resto
redvisio
n
Park200
69female
RightN
KWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
No
Free
ofsymptom
Park200
61m
ale
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gleft
hemiparesis
NK
No
Leftmild
hemiparesis
Park200
65male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
BioMed Research International 7Ta
ble2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Park200
62male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
Nitsch
etal
2007
22m
ale
Right2
cmNail-g
unAc
cident
Rightu
pper
jaw
totempo
rallob
eIntracerebral
haem
atom
a
Simplee
xtraction
ofthen
ailw
ithou
tac
raniotom
yNK
NK
Hira
ishi2007
5female
Left35c
mPlastic
chop
stick
Falling
Fron
tal(orbital
medial)
Feverheadache
neck
stiffn
ess
Craniotomy
Meningitis
brainabscess
Hyposmia
Kawada2009
5female
Left3c
mWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
Brainabscess
Free
ofsymptom
Mitilian
2009
4male
Right11cm
Woo
den
chop
stick
Falling
Superio
rorbita
lfissure
Mild
confusion
vomiting
Craniotomy
Brainabscess
Mild
dysm
etria
ofthea
rm
Wieland
etal
2010
58m
ale
Left-sid
edN
KWoo
denstick
Accident
Maxillofacialto
ethm
oidroof
Feverheadache
nausea
vomiting
mentalstatus
changes
Endo
scop
icrepair
ofthes
kullbase
defect
Intracranial
infection
NK
Hettig
eetal
2010
38fe
male
LeftNK
Plastic
chop
stick
Stum
ble
Poste
riorw
allof
theo
roph
aryn
xto
jugu
lar
foramen
into
the
poste
riorfossa
Nystagm
usleft
9th10thand
12th
cranial
nerves
palsy
qu
adrantanop
ia
Leftoccipital
craniotomy
retro
sigmoid
craniectom
y
No
Left9th10th
and12th
cranial
nerves
palsy
Sweeneyetal
2011
31m
ale
RightN
KKn
ifeSuicidal
attempt
Lower
jawto
anterio
rsku
llbase
Pain
Com
binedrig
htpte rionaland
interhem
ispheric
craniotomies
No
NK
Sweeneyetal
2011
21fe
male
RightN
KKn
ifeHom
icidal
attempt
Leftorbitto
middles
kull
base
Emesis
seizure
Leftcranioor-
bitozygomatic
approach
No
NK
Yonezawa2011
28m
ale
LeftNK
Plastic
chop
stick
Falling
Fron
tal(orbital
medial)
NK
Craniotomy
No
Free
ofsymptom
Arslanetal
2012
13m
ale
Right18c
mIron
bar
Falling
Righto
rbitand
superio
rorbita
lfissure
Com
a(GCS
3)Right
frontop
arietal
craniotomy
No
Died
Shin
etal2012
38m
ale
Left14cm
Plastic
chop
stick
Falling
Superio
rorbita
lfissure
Blindn
ess
swellin
gnu
mbn
ess
arou
ndeye
Removalof
chop
stick
with
out
craniotomy
No
Blindn
ess
Katayamae
tal
2013
18m
ale
Right12c
mMetalrod
Falling
Fron
tal
(sub
zygomatic
bone)
Vomiting
NK
NK
Noneurological
deficit
Wangetal2013
35m
ale
Left18cm
Steel
Falling
Leftmaxillary
sinus
Limited
movem
ento
fneck
Craniotomy
No
Leftfacialpalsy
8 BioMed Research International
Table2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Skochetal2
013
35fe
male
MedialN
KElectric
toothb
rush
Accident
Tempo
ral
(lateralorbit)
Blurredvisio
npain
Mod
ified
frontotem
poral
orbitozygomatic
craniotomy
No
Improved
pain
andvisio
n
Deveere
tal
2013
43m
ale
Right5
6cm
Plastic
pen
Falling
Righto
rbit
No
NK
No
Free
ofsymptom
Yamasakietal
2013
4female
Left65c
mplastic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gNK
Meningitis
enceph
alitis
Free
ofsymptom
Williamse
tal
2014
56m
ale
LeftNK
Speargun
Suicidal
attempt
Subm
andibu
lar
region
oral
cavity
Com
aLargec
raniotom
yCerebritis
Died
ACAA
nteriorC
erebralA
rteryCS
FCerebrospinalFluidGCS
Glasgow
Com
aScaleICA
internalcarotid
arteryN
Kno
tkno
wn
BioMed Research International 9
(a)
(a)
(b)
(b)
(c)
(c)
(d)
lowast
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 3 Photography showed the entry point (black triangle 998787) of foreign body on face and incision for a frontotemporoorbitozygomaticapproach (a) Short piece of foreign body (simple arrow larr) in the face was exposed and removed by a maxillofacial surgeon (b) Theinfratemporal fossa was opened to expose the long piece of foreign body (c) and it (hollow arrow) was removed in a retrograde fashionDuring the removing process yellowish pus (asterisk lowast) was drained into the infratemporal fossa (d) Photography displayed short piece(simple arrowlarr) and long piece (hollow arrow) of the foreign body (e) Postoperative skull radiography suggested complete removal ofthe foreign body (f) The small bone fragment (hollow arrow head) was left in place due to its close relationship with branch of MCA (g)Three-month follow-up MRI revealed no abscess formation (h) The patient recovered uneventfully (i) MCA middle cerebral artery MRImagnetic resonance imaging
3D modeling has been frequently used in the presurgicalplanning of PSBIs in previous studies [8 11 15ndash17 19 2324 28] 3D models can be viewed in 360 degrees rotatedand studied from any perspective [29ndash31] which facilitate thediagnosis and operation to some extent [30 31] 3D Slicer is afree open source software that can be used for segmentation
and 3D modeling with high accuracy and reliability [30 32]It has been used in the management of various diseasesincluding intracranial aneurysms trigeminal neuralgia andintracerebral hematomas [29 30 33] PSBIs in our case serieswere reconstructed using 3D Slicer in which penetratingpoints as well as the surrounding neurovascular structures
10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014

BioMed Research International 3
(a)
(a)
(b)
(b)
(c)
(c)
(d)
(d)
(e)
(e)
(f)
(f)
(g)
(g)
f
to
(h)
(h)
(i)
(i)
Figure 1 Head CT scan demonstrated a bamboo stick (hollow arrow) penetrating into the temporal lobe via superior orbital fissure Thebamboo stick presented as high density on the CT scan (a b c) Contrast enhanced MRI revealed an abscess (simple arrowlarr) around thebamboo stick in temporal lobe (d e f) 3D reconstruction of the skull cerebral artery and bamboo stick (hollow arrow ) was performedby 3D Slicer software to visualize the relationship among these structures (g) Intraoperative photography (h) displayed the bamboo stick inoriginal place (o orbital side f frontal side t temporal side) Photography showed the removed bamboo stick (i) 3D three-dimensional CTcomputed tomography MRI magnetic resonance imaging
common penetrating point followed by oral or nasal cavityand maxillofacial region
42 Diagnosis of PSBIs After careful physical examinationproper radiological examination on the basis of patientsrsquocondition is necessary Although the importance of head CTscan in the management of PSBIs has been emphasized in
previous literatures several instructions should be noticedFirstly the density of foreign bodies on CT scan variesaccording to their types For example metal presents as highdensity while wood or plastics are of isodensity or lowdensityand difficult to identify Secondly the density of some foreignbodies would change over time For example bamboo is oflow density on initial CT scan but it would be of high density
4 BioMed Research International
(a)
(a)
(b)
(b)
(c)
(c)
(d)
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 2 Preoperative image of foreign body (burst outer rim of a grinding wheel) in the face andmiddle skull base Anterior-posterior skullradiography (a) and lateral skull radiography (b) demonstrated the short piece (simple arrowlarr) in the face and long piece (hollow arrow) penetrating into the middle skull base Sagittal reconstruction of CT (c) showed the long piece penetrating into the middle cranial fossathrough infratemporal fossa A small piece of bone fragment (hollow arrowhead ) was noticed above the long piece The bone fragmentarose from the hit of the long piece on the middle skull base DSA (d amp e) proved the integrity of MCA Axial CT revealed close relationshipbetween the bone fragment (hollow arrow head ) and branch of MCA (f) 3D reconstruction (g h i) with 3D Slicer software displayedspatial correlation of two pieces of foreign body with the face and skull base 3D three-dimensional CT computed tomography DSA digitalsubtraction angiography MCA middle cerebral artery
later which frequently leads to misdiagnosis (Case 1) [25]Therefore MRI is a useful supplement to CT in the detectionof nonmetallic foreign bodies
Angiography such as the CT angiography MR angiogra-phy or DSA is highly recommended for patients in suspicion
of artery injuries or traumatic aneurysms [7 26 27] Asdemonstrated in Case 2 foreign bodies may not causeimmediate vascular injury sometimes but lead to cerebralvasospasm or stenosis in the long run highlighting theimportance of angiography in the setting of PSBIs
BioMed Research International 5
Table1Dem
ograph
icsa
ndclinicald
atafor
patie
ntso
fPSB
I
Case
Age
and
gend
erMechanism
ofinjury
Type
andsiz
eof
foreign
body
Penetrating
pathway
Symptom
sand
concurrent
cond
ition
s
DSA
finding
s
Interval
toop
eration
Operatio
nSurgicalapproach
Resid
ual
fractio
nAntibioticsu
sed
Symptom
sat
discharge
175fe
male
Accident
Bambo
o7c
m
Left
orbit-s
uperior
orbital
fissure-anterior
skullbase-left
tempo
rallob
e
Headache
dizzinessbrain
abscess
Negative
20days
Yes
Orbito
zygomatic
approach
and
pterional
craniotomy
No
Metronidazole
cefta
zidime
vancom
ycin
linezolid
biapenem
Free
ofsymptom
232m
ale
Accident
Grin
ding
wheel
65c
m
Leftmaxilla-
infratem
poral
fossa-middle
cranialfossa
ciste
rnof
lateral
sulcus
Headachebrain
abscess
Negative
19days
Yes
Tempo
rozygomatic
approach
No
Linezolid
Epilepsy
342m
ale
Accident
Electro
drill
22c
m
Lefteyebrow-
anterio
rcranial
base-le
ftfro
ntal
lobe
Headache
cerebral
contusion
Not
cond
ucted
No
operation
No
mdashYes
Linezolid
biapenem
Slight
headache
429m
ale
Accident
Screw
54c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blurredvisio
nanterio
rsku
llbase
fracture
oculom
otor
nerveinjury
Not
cond
ucted
2days
Yes
Fron
totempo
ral
approach
No
Vancom
ycin
linezolid
Improved
visio
noculom
otor
nerve
injury
540
male
Accident
Hot
projectiv
eoil
paint34c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blindn
essrig
hteyep
enetratin
ginjuryfrontal
hematom
a
Not
cond
ucted
4days
Yes
Subfrontal
approach
Yes
Vancom
ycin
ceftriaxone
B lindn
ess
6 BioMed Research International
Table2Clinicoradiologicalfeatureso
fpreviou
slyrepo
rted
caseso
fPSB
I
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Matsumotoet
al1998
3female
Left3c
mPlastic
chop
stick
Falling
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Matsumotoet
al1998
57m
ale
Right2
cmWoo
den
chop
stick
Stickinto
chop
stick
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Hebecker2009
32m
ale
Leftno
foreign
body
Wild
deerrsquos
antler
Accident
Leftorbit
floorla
teral
orbit
Com
aBifro
ntalintradural
neurosurgical
approach
No
Free
ofsymptom
Ishikawae
tal
2000
4male
Left6c
mWoo
den
chop
stick
Falling
Preauricular
area
topo
sterio
rfossa
Feverheadache
Subo
ccipita
lcraniectom
yBrainabscess
Ataxiaand
dysm
etria
Matsuyamae
tal2001
1male
Right2
5cm
Woo
den
chop
sticks
Falling
Superio
rorbita
lfissure
Swolleneye
Transcranial
approach
Meningitis
Free
ofsymptom
Maruyae
tal
2002
56fe
male
Left1cm
Bambo
oTu
mbling
Tempo
ral
(lateralorbit)
Drowsin
ess
Left
frontotem
poral
craniotomyand
orbitozygomatic
osteotom
y
No
Lateralgazein
theleft
eye
Hayashi
etal
2003
71fe
male
Rightn
oforeign
body
Bear
claws
Animal
assault
Fron
talsinus
Laceratedface
CSFfistulas
Fron
tal
craniectom
iesto
repairCS
Ffistulas
No
Free
ofsymptom
Nish
ioetal
2004
6female
Right2
5cm
Woo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Feverheadache
neck
stiffn
ess
Craniotomy
Brainabscess
Fre e
ofsymptom
Kim
etal2005
1male
Right2
cmMetallic
chop
stick
Falling
Fron
tal(orbital
roof)
Crying
Craniotomy
No
Free
ofsymptom
Tsao
etal2006
45m
ale
Left25c
mlowast
25c
mPlastic
chair
glide
Beassaulted
Sino
nasalcavity
anterio
rsku
llbase
Ptosis
impaire
dvisio
n
Transnasal
endo
scop
icexplorationand
removalof
the
foreignbo
dy
No
Ano
smiaand
diplop
ia
DeT
ommasiet
al2006
20m
ale
Right10c
mScrewdriver
Falling
Rightm
axilla
Scotom
ainthe
lefteyeCS
Fleakage
Leftpterional
approach
NK
Resto
redvisio
n
Park200
69female
RightN
KWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
No
Free
ofsymptom
Park200
61m
ale
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gleft
hemiparesis
NK
No
Leftmild
hemiparesis
Park200
65male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
BioMed Research International 7Ta
ble2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Park200
62male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
Nitsch
etal
2007
22m
ale
Right2
cmNail-g
unAc
cident
Rightu
pper
jaw
totempo
rallob
eIntracerebral
haem
atom
a
Simplee
xtraction
ofthen
ailw
ithou
tac
raniotom
yNK
NK
Hira
ishi2007
5female
Left35c
mPlastic
chop
stick
Falling
Fron
tal(orbital
medial)
Feverheadache
neck
stiffn
ess
Craniotomy
Meningitis
brainabscess
Hyposmia
Kawada2009
5female
Left3c
mWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
Brainabscess
Free
ofsymptom
Mitilian
2009
4male
Right11cm
Woo
den
chop
stick
Falling
Superio
rorbita
lfissure
Mild
confusion
vomiting
Craniotomy
Brainabscess
Mild
dysm
etria
ofthea
rm
Wieland
etal
2010
58m
ale
Left-sid
edN
KWoo
denstick
Accident
Maxillofacialto
ethm
oidroof
Feverheadache
nausea
vomiting
mentalstatus
changes
Endo
scop
icrepair
ofthes
kullbase
defect
Intracranial
infection
NK
Hettig
eetal
2010
38fe
male
LeftNK
Plastic
chop
stick
Stum
ble
Poste
riorw
allof
theo
roph
aryn
xto
jugu
lar
foramen
into
the
poste
riorfossa
Nystagm
usleft
9th10thand
12th
cranial
nerves
palsy
qu
adrantanop
ia
Leftoccipital
craniotomy
retro
sigmoid
craniectom
y
No
Left9th10th
and12th
cranial
nerves
palsy
Sweeneyetal
2011
31m
ale
RightN
KKn
ifeSuicidal
attempt
Lower
jawto
anterio
rsku
llbase
Pain
Com
binedrig
htpte rionaland
interhem
ispheric
craniotomies
No
NK
Sweeneyetal
2011
21fe
male
RightN
KKn
ifeHom
icidal
attempt
Leftorbitto
middles
kull
base
Emesis
seizure
Leftcranioor-
bitozygomatic
approach
No
NK
Yonezawa2011
28m
ale
LeftNK
Plastic
chop
stick
Falling
Fron
tal(orbital
medial)
NK
Craniotomy
No
Free
ofsymptom
Arslanetal
2012
13m
ale
Right18c
mIron
bar
Falling
Righto
rbitand
superio
rorbita
lfissure
Com
a(GCS
3)Right
frontop
arietal
craniotomy
No
Died
Shin
etal2012
38m
ale
Left14cm
Plastic
chop
stick
Falling
Superio
rorbita
lfissure
Blindn
ess
swellin
gnu
mbn
ess
arou
ndeye
Removalof
chop
stick
with
out
craniotomy
No
Blindn
ess
Katayamae
tal
2013
18m
ale
Right12c
mMetalrod
Falling
Fron
tal
(sub
zygomatic
bone)
Vomiting
NK
NK
Noneurological
deficit
Wangetal2013
35m
ale
Left18cm
Steel
Falling
Leftmaxillary
sinus
Limited
movem
ento
fneck
Craniotomy
No
Leftfacialpalsy
8 BioMed Research International
Table2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Skochetal2
013
35fe
male
MedialN
KElectric
toothb
rush
Accident
Tempo
ral
(lateralorbit)
Blurredvisio
npain
Mod
ified
frontotem
poral
orbitozygomatic
craniotomy
No
Improved
pain
andvisio
n
Deveere
tal
2013
43m
ale
Right5
6cm
Plastic
pen
Falling
Righto
rbit
No
NK
No
Free
ofsymptom
Yamasakietal
2013
4female
Left65c
mplastic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gNK
Meningitis
enceph
alitis
Free
ofsymptom
Williamse
tal
2014
56m
ale
LeftNK
Speargun
Suicidal
attempt
Subm
andibu
lar
region
oral
cavity
Com
aLargec
raniotom
yCerebritis
Died
ACAA
nteriorC
erebralA
rteryCS
FCerebrospinalFluidGCS
Glasgow
Com
aScaleICA
internalcarotid
arteryN
Kno
tkno
wn
BioMed Research International 9
(a)
(a)
(b)
(b)
(c)
(c)
(d)
lowast
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 3 Photography showed the entry point (black triangle 998787) of foreign body on face and incision for a frontotemporoorbitozygomaticapproach (a) Short piece of foreign body (simple arrow larr) in the face was exposed and removed by a maxillofacial surgeon (b) Theinfratemporal fossa was opened to expose the long piece of foreign body (c) and it (hollow arrow) was removed in a retrograde fashionDuring the removing process yellowish pus (asterisk lowast) was drained into the infratemporal fossa (d) Photography displayed short piece(simple arrowlarr) and long piece (hollow arrow) of the foreign body (e) Postoperative skull radiography suggested complete removal ofthe foreign body (f) The small bone fragment (hollow arrow head) was left in place due to its close relationship with branch of MCA (g)Three-month follow-up MRI revealed no abscess formation (h) The patient recovered uneventfully (i) MCA middle cerebral artery MRImagnetic resonance imaging
3D modeling has been frequently used in the presurgicalplanning of PSBIs in previous studies [8 11 15ndash17 19 2324 28] 3D models can be viewed in 360 degrees rotatedand studied from any perspective [29ndash31] which facilitate thediagnosis and operation to some extent [30 31] 3D Slicer is afree open source software that can be used for segmentation
and 3D modeling with high accuracy and reliability [30 32]It has been used in the management of various diseasesincluding intracranial aneurysms trigeminal neuralgia andintracerebral hematomas [29 30 33] PSBIs in our case serieswere reconstructed using 3D Slicer in which penetratingpoints as well as the surrounding neurovascular structures
10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
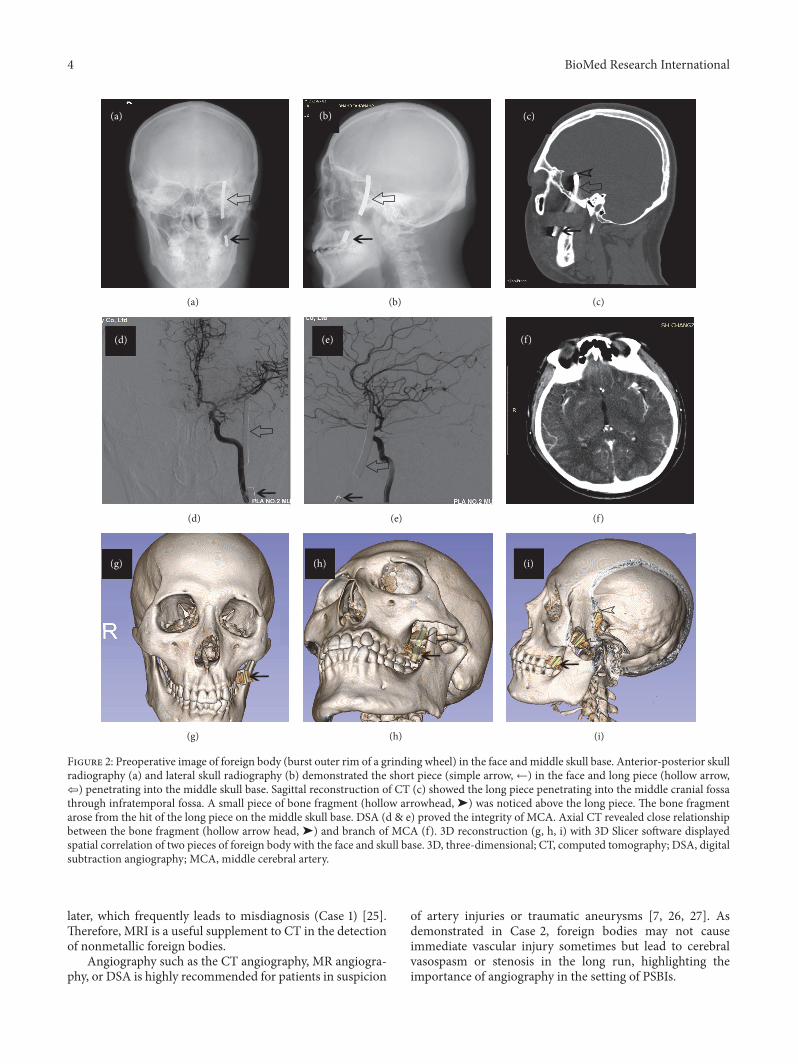
4 BioMed Research International
(a)
(a)
(b)
(b)
(c)
(c)
(d)
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 2 Preoperative image of foreign body (burst outer rim of a grinding wheel) in the face andmiddle skull base Anterior-posterior skullradiography (a) and lateral skull radiography (b) demonstrated the short piece (simple arrowlarr) in the face and long piece (hollow arrow) penetrating into the middle skull base Sagittal reconstruction of CT (c) showed the long piece penetrating into the middle cranial fossathrough infratemporal fossa A small piece of bone fragment (hollow arrowhead ) was noticed above the long piece The bone fragmentarose from the hit of the long piece on the middle skull base DSA (d amp e) proved the integrity of MCA Axial CT revealed close relationshipbetween the bone fragment (hollow arrow head ) and branch of MCA (f) 3D reconstruction (g h i) with 3D Slicer software displayedspatial correlation of two pieces of foreign body with the face and skull base 3D three-dimensional CT computed tomography DSA digitalsubtraction angiography MCA middle cerebral artery
later which frequently leads to misdiagnosis (Case 1) [25]Therefore MRI is a useful supplement to CT in the detectionof nonmetallic foreign bodies
Angiography such as the CT angiography MR angiogra-phy or DSA is highly recommended for patients in suspicion
of artery injuries or traumatic aneurysms [7 26 27] Asdemonstrated in Case 2 foreign bodies may not causeimmediate vascular injury sometimes but lead to cerebralvasospasm or stenosis in the long run highlighting theimportance of angiography in the setting of PSBIs
BioMed Research International 5
Table1Dem
ograph
icsa
ndclinicald
atafor
patie
ntso
fPSB
I
Case
Age
and
gend
erMechanism
ofinjury
Type
andsiz
eof
foreign
body
Penetrating
pathway
Symptom
sand
concurrent
cond
ition
s
DSA
finding
s
Interval
toop
eration
Operatio
nSurgicalapproach
Resid
ual
fractio
nAntibioticsu
sed
Symptom
sat
discharge
175fe
male
Accident
Bambo
o7c
m
Left
orbit-s
uperior
orbital
fissure-anterior
skullbase-left
tempo
rallob
e
Headache
dizzinessbrain
abscess
Negative
20days
Yes
Orbito
zygomatic
approach
and
pterional
craniotomy
No
Metronidazole
cefta
zidime
vancom
ycin
linezolid
biapenem
Free
ofsymptom
232m
ale
Accident
Grin
ding
wheel
65c
m
Leftmaxilla-
infratem
poral
fossa-middle
cranialfossa
ciste
rnof
lateral
sulcus
Headachebrain
abscess
Negative
19days
Yes
Tempo
rozygomatic
approach
No
Linezolid
Epilepsy
342m
ale
Accident
Electro
drill
22c
m
Lefteyebrow-
anterio
rcranial
base-le
ftfro
ntal
lobe
Headache
cerebral
contusion
Not
cond
ucted
No
operation
No
mdashYes
Linezolid
biapenem
Slight
headache
429m
ale
Accident
Screw
54c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blurredvisio
nanterio
rsku
llbase
fracture
oculom
otor
nerveinjury
Not
cond
ucted
2days
Yes
Fron
totempo
ral
approach
No
Vancom
ycin
linezolid
Improved
visio
noculom
otor
nerve
injury
540
male
Accident
Hot
projectiv
eoil
paint34c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blindn
essrig
hteyep
enetratin
ginjuryfrontal
hematom
a
Not
cond
ucted
4days
Yes
Subfrontal
approach
Yes
Vancom
ycin
ceftriaxone
B lindn
ess
6 BioMed Research International
Table2Clinicoradiologicalfeatureso
fpreviou
slyrepo
rted
caseso
fPSB
I
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Matsumotoet
al1998
3female
Left3c
mPlastic
chop
stick
Falling
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Matsumotoet
al1998
57m
ale
Right2
cmWoo
den
chop
stick
Stickinto
chop
stick
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Hebecker2009
32m
ale
Leftno
foreign
body
Wild
deerrsquos
antler
Accident
Leftorbit
floorla
teral
orbit
Com
aBifro
ntalintradural
neurosurgical
approach
No
Free
ofsymptom
Ishikawae
tal
2000
4male
Left6c
mWoo
den
chop
stick
Falling
Preauricular
area
topo
sterio
rfossa
Feverheadache
Subo
ccipita
lcraniectom
yBrainabscess
Ataxiaand
dysm
etria
Matsuyamae
tal2001
1male
Right2
5cm
Woo
den
chop
sticks
Falling
Superio
rorbita
lfissure
Swolleneye
Transcranial
approach
Meningitis
Free
ofsymptom
Maruyae
tal
2002
56fe
male
Left1cm
Bambo
oTu
mbling
Tempo
ral
(lateralorbit)
Drowsin
ess
Left
frontotem
poral
craniotomyand
orbitozygomatic
osteotom
y
No
Lateralgazein
theleft
eye
Hayashi
etal
2003
71fe
male
Rightn
oforeign
body
Bear
claws
Animal
assault
Fron
talsinus
Laceratedface
CSFfistulas
Fron
tal
craniectom
iesto
repairCS
Ffistulas
No
Free
ofsymptom
Nish
ioetal
2004
6female
Right2
5cm
Woo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Feverheadache
neck
stiffn
ess
Craniotomy
Brainabscess
Fre e
ofsymptom
Kim
etal2005
1male
Right2
cmMetallic
chop
stick
Falling
Fron
tal(orbital
roof)
Crying
Craniotomy
No
Free
ofsymptom
Tsao
etal2006
45m
ale
Left25c
mlowast
25c
mPlastic
chair
glide
Beassaulted
Sino
nasalcavity
anterio
rsku
llbase
Ptosis
impaire
dvisio
n
Transnasal
endo
scop
icexplorationand
removalof
the
foreignbo
dy
No
Ano
smiaand
diplop
ia
DeT
ommasiet
al2006
20m
ale
Right10c
mScrewdriver
Falling
Rightm
axilla
Scotom
ainthe
lefteyeCS
Fleakage
Leftpterional
approach
NK
Resto
redvisio
n
Park200
69female
RightN
KWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
No
Free
ofsymptom
Park200
61m
ale
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gleft
hemiparesis
NK
No
Leftmild
hemiparesis
Park200
65male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
BioMed Research International 7Ta
ble2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Park200
62male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
Nitsch
etal
2007
22m
ale
Right2
cmNail-g
unAc
cident
Rightu
pper
jaw
totempo
rallob
eIntracerebral
haem
atom
a
Simplee
xtraction
ofthen
ailw
ithou
tac
raniotom
yNK
NK
Hira
ishi2007
5female
Left35c
mPlastic
chop
stick
Falling
Fron
tal(orbital
medial)
Feverheadache
neck
stiffn
ess
Craniotomy
Meningitis
brainabscess
Hyposmia
Kawada2009
5female
Left3c
mWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
Brainabscess
Free
ofsymptom
Mitilian
2009
4male
Right11cm
Woo
den
chop
stick
Falling
Superio
rorbita
lfissure
Mild
confusion
vomiting
Craniotomy
Brainabscess
Mild
dysm
etria
ofthea
rm
Wieland
etal
2010
58m
ale
Left-sid
edN
KWoo
denstick
Accident
Maxillofacialto
ethm
oidroof
Feverheadache
nausea
vomiting
mentalstatus
changes
Endo
scop
icrepair
ofthes
kullbase
defect
Intracranial
infection
NK
Hettig
eetal
2010
38fe
male
LeftNK
Plastic
chop
stick
Stum
ble
Poste
riorw
allof
theo
roph
aryn
xto
jugu
lar
foramen
into
the
poste
riorfossa
Nystagm
usleft
9th10thand
12th
cranial
nerves
palsy
qu
adrantanop
ia
Leftoccipital
craniotomy
retro
sigmoid
craniectom
y
No
Left9th10th
and12th
cranial
nerves
palsy
Sweeneyetal
2011
31m
ale
RightN
KKn
ifeSuicidal
attempt
Lower
jawto
anterio
rsku
llbase
Pain
Com
binedrig
htpte rionaland
interhem
ispheric
craniotomies
No
NK
Sweeneyetal
2011
21fe
male
RightN
KKn
ifeHom
icidal
attempt
Leftorbitto
middles
kull
base
Emesis
seizure
Leftcranioor-
bitozygomatic
approach
No
NK
Yonezawa2011
28m
ale
LeftNK
Plastic
chop
stick
Falling
Fron
tal(orbital
medial)
NK
Craniotomy
No
Free
ofsymptom
Arslanetal
2012
13m
ale
Right18c
mIron
bar
Falling
Righto
rbitand
superio
rorbita
lfissure
Com
a(GCS
3)Right
frontop
arietal
craniotomy
No
Died
Shin
etal2012
38m
ale
Left14cm
Plastic
chop
stick
Falling
Superio
rorbita
lfissure
Blindn
ess
swellin
gnu
mbn
ess
arou
ndeye
Removalof
chop
stick
with
out
craniotomy
No
Blindn
ess
Katayamae
tal
2013
18m
ale
Right12c
mMetalrod
Falling
Fron
tal
(sub
zygomatic
bone)
Vomiting
NK
NK
Noneurological
deficit
Wangetal2013
35m
ale
Left18cm
Steel
Falling
Leftmaxillary
sinus
Limited
movem
ento
fneck
Craniotomy
No
Leftfacialpalsy
8 BioMed Research International
Table2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Skochetal2
013
35fe
male
MedialN
KElectric
toothb
rush
Accident
Tempo
ral
(lateralorbit)
Blurredvisio
npain
Mod
ified
frontotem
poral
orbitozygomatic
craniotomy
No
Improved
pain
andvisio
n
Deveere
tal
2013
43m
ale
Right5
6cm
Plastic
pen
Falling
Righto
rbit
No
NK
No
Free
ofsymptom
Yamasakietal
2013
4female
Left65c
mplastic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gNK
Meningitis
enceph
alitis
Free
ofsymptom
Williamse
tal
2014
56m
ale
LeftNK
Speargun
Suicidal
attempt
Subm
andibu
lar
region
oral
cavity
Com
aLargec
raniotom
yCerebritis
Died
ACAA
nteriorC
erebralA
rteryCS
FCerebrospinalFluidGCS
Glasgow
Com
aScaleICA
internalcarotid
arteryN
Kno
tkno
wn
BioMed Research International 9
(a)
(a)
(b)
(b)
(c)
(c)
(d)
lowast
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 3 Photography showed the entry point (black triangle 998787) of foreign body on face and incision for a frontotemporoorbitozygomaticapproach (a) Short piece of foreign body (simple arrow larr) in the face was exposed and removed by a maxillofacial surgeon (b) Theinfratemporal fossa was opened to expose the long piece of foreign body (c) and it (hollow arrow) was removed in a retrograde fashionDuring the removing process yellowish pus (asterisk lowast) was drained into the infratemporal fossa (d) Photography displayed short piece(simple arrowlarr) and long piece (hollow arrow) of the foreign body (e) Postoperative skull radiography suggested complete removal ofthe foreign body (f) The small bone fragment (hollow arrow head) was left in place due to its close relationship with branch of MCA (g)Three-month follow-up MRI revealed no abscess formation (h) The patient recovered uneventfully (i) MCA middle cerebral artery MRImagnetic resonance imaging
3D modeling has been frequently used in the presurgicalplanning of PSBIs in previous studies [8 11 15ndash17 19 2324 28] 3D models can be viewed in 360 degrees rotatedand studied from any perspective [29ndash31] which facilitate thediagnosis and operation to some extent [30 31] 3D Slicer is afree open source software that can be used for segmentation
and 3D modeling with high accuracy and reliability [30 32]It has been used in the management of various diseasesincluding intracranial aneurysms trigeminal neuralgia andintracerebral hematomas [29 30 33] PSBIs in our case serieswere reconstructed using 3D Slicer in which penetratingpoints as well as the surrounding neurovascular structures
10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
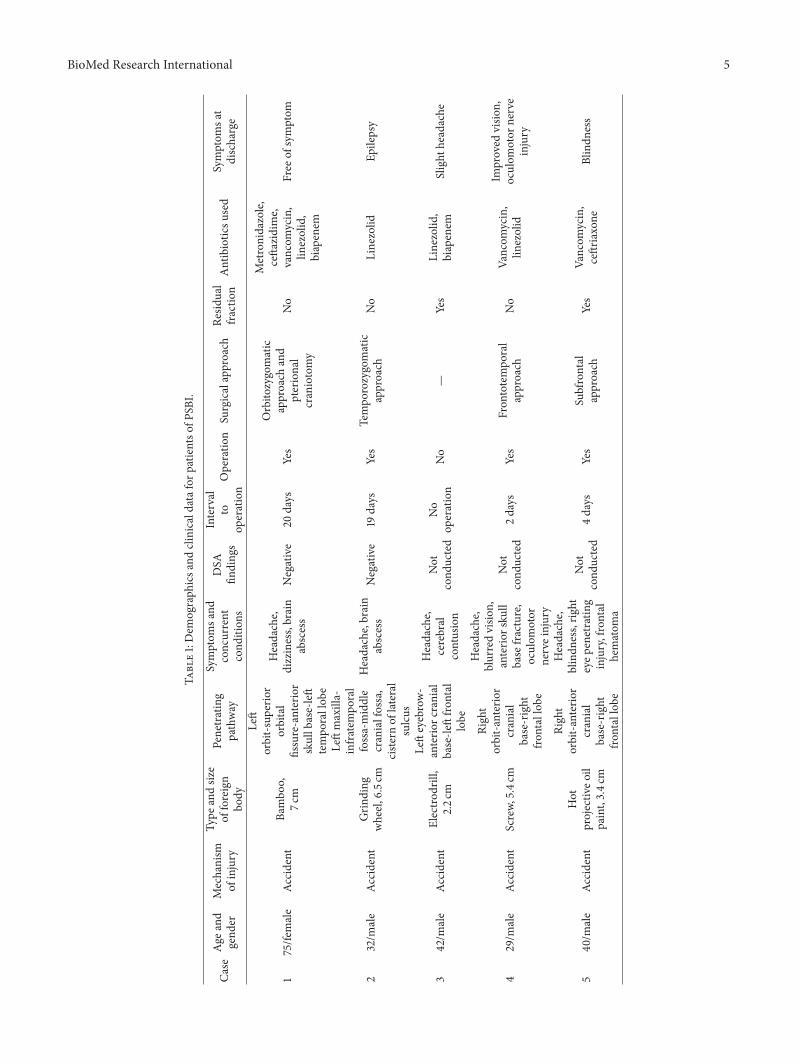
BioMed Research International 5
Table1Dem
ograph
icsa
ndclinicald
atafor
patie
ntso
fPSB
I
Case
Age
and
gend
erMechanism
ofinjury
Type
andsiz
eof
foreign
body
Penetrating
pathway
Symptom
sand
concurrent
cond
ition
s
DSA
finding
s
Interval
toop
eration
Operatio
nSurgicalapproach
Resid
ual
fractio
nAntibioticsu
sed
Symptom
sat
discharge
175fe
male
Accident
Bambo
o7c
m
Left
orbit-s
uperior
orbital
fissure-anterior
skullbase-left
tempo
rallob
e
Headache
dizzinessbrain
abscess
Negative
20days
Yes
Orbito
zygomatic
approach
and
pterional
craniotomy
No
Metronidazole
cefta
zidime
vancom
ycin
linezolid
biapenem
Free
ofsymptom
232m
ale
Accident
Grin
ding
wheel
65c
m
Leftmaxilla-
infratem
poral
fossa-middle
cranialfossa
ciste
rnof
lateral
sulcus
Headachebrain
abscess
Negative
19days
Yes
Tempo
rozygomatic
approach
No
Linezolid
Epilepsy
342m
ale
Accident
Electro
drill
22c
m
Lefteyebrow-
anterio
rcranial
base-le
ftfro
ntal
lobe
Headache
cerebral
contusion
Not
cond
ucted
No
operation
No
mdashYes
Linezolid
biapenem
Slight
headache
429m
ale
Accident
Screw
54c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blurredvisio
nanterio
rsku
llbase
fracture
oculom
otor
nerveinjury
Not
cond
ucted
2days
Yes
Fron
totempo
ral
approach
No
Vancom
ycin
linezolid
Improved
visio
noculom
otor
nerve
injury
540
male
Accident
Hot
projectiv
eoil
paint34c
m
Right
orbit-a
nterior
cranial
base-right
frontallobe
Headache
blindn
essrig
hteyep
enetratin
ginjuryfrontal
hematom
a
Not
cond
ucted
4days
Yes
Subfrontal
approach
Yes
Vancom
ycin
ceftriaxone
B lindn
ess
6 BioMed Research International
Table2Clinicoradiologicalfeatureso
fpreviou
slyrepo
rted
caseso
fPSB
I
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Matsumotoet
al1998
3female
Left3c
mPlastic
chop
stick
Falling
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Matsumotoet
al1998
57m
ale
Right2
cmWoo
den
chop
stick
Stickinto
chop
stick
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Hebecker2009
32m
ale
Leftno
foreign
body
Wild
deerrsquos
antler
Accident
Leftorbit
floorla
teral
orbit
Com
aBifro
ntalintradural
neurosurgical
approach
No
Free
ofsymptom
Ishikawae
tal
2000
4male
Left6c
mWoo
den
chop
stick
Falling
Preauricular
area
topo
sterio
rfossa
Feverheadache
Subo
ccipita
lcraniectom
yBrainabscess
Ataxiaand
dysm
etria
Matsuyamae
tal2001
1male
Right2
5cm
Woo
den
chop
sticks
Falling
Superio
rorbita
lfissure
Swolleneye
Transcranial
approach
Meningitis
Free
ofsymptom
Maruyae
tal
2002
56fe
male
Left1cm
Bambo
oTu
mbling
Tempo
ral
(lateralorbit)
Drowsin
ess
Left
frontotem
poral
craniotomyand
orbitozygomatic
osteotom
y
No
Lateralgazein
theleft
eye
Hayashi
etal
2003
71fe
male
Rightn
oforeign
body
Bear
claws
Animal
assault
Fron
talsinus
Laceratedface
CSFfistulas
Fron
tal
craniectom
iesto
repairCS
Ffistulas
No
Free
ofsymptom
Nish
ioetal
2004
6female
Right2
5cm
Woo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Feverheadache
neck
stiffn
ess
Craniotomy
Brainabscess
Fre e
ofsymptom
Kim
etal2005
1male
Right2
cmMetallic
chop
stick
Falling
Fron
tal(orbital
roof)
Crying
Craniotomy
No
Free
ofsymptom
Tsao
etal2006
45m
ale
Left25c
mlowast
25c
mPlastic
chair
glide
Beassaulted
Sino
nasalcavity
anterio
rsku
llbase
Ptosis
impaire
dvisio
n
Transnasal
endo
scop
icexplorationand
removalof
the
foreignbo
dy
No
Ano
smiaand
diplop
ia
DeT
ommasiet
al2006
20m
ale
Right10c
mScrewdriver
Falling
Rightm
axilla
Scotom
ainthe
lefteyeCS
Fleakage
Leftpterional
approach
NK
Resto
redvisio
n
Park200
69female
RightN
KWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
No
Free
ofsymptom
Park200
61m
ale
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gleft
hemiparesis
NK
No
Leftmild
hemiparesis
Park200
65male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
BioMed Research International 7Ta
ble2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Park200
62male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
Nitsch
etal
2007
22m
ale
Right2
cmNail-g
unAc
cident
Rightu
pper
jaw
totempo
rallob
eIntracerebral
haem
atom
a
Simplee
xtraction
ofthen
ailw
ithou
tac
raniotom
yNK
NK
Hira
ishi2007
5female
Left35c
mPlastic
chop
stick
Falling
Fron
tal(orbital
medial)
Feverheadache
neck
stiffn
ess
Craniotomy
Meningitis
brainabscess
Hyposmia
Kawada2009
5female
Left3c
mWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
Brainabscess
Free
ofsymptom
Mitilian
2009
4male
Right11cm
Woo
den
chop
stick
Falling
Superio
rorbita
lfissure
Mild
confusion
vomiting
Craniotomy
Brainabscess
Mild
dysm
etria
ofthea
rm
Wieland
etal
2010
58m
ale
Left-sid
edN
KWoo
denstick
Accident
Maxillofacialto
ethm
oidroof
Feverheadache
nausea
vomiting
mentalstatus
changes
Endo
scop
icrepair
ofthes
kullbase
defect
Intracranial
infection
NK
Hettig
eetal
2010
38fe
male
LeftNK
Plastic
chop
stick
Stum
ble
Poste
riorw
allof
theo
roph
aryn
xto
jugu
lar
foramen
into
the
poste
riorfossa
Nystagm
usleft
9th10thand
12th
cranial
nerves
palsy
qu
adrantanop
ia
Leftoccipital
craniotomy
retro
sigmoid
craniectom
y
No
Left9th10th
and12th
cranial
nerves
palsy
Sweeneyetal
2011
31m
ale
RightN
KKn
ifeSuicidal
attempt
Lower
jawto
anterio
rsku
llbase
Pain
Com
binedrig
htpte rionaland
interhem
ispheric
craniotomies
No
NK
Sweeneyetal
2011
21fe
male
RightN
KKn
ifeHom
icidal
attempt
Leftorbitto
middles
kull
base
Emesis
seizure
Leftcranioor-
bitozygomatic
approach
No
NK
Yonezawa2011
28m
ale
LeftNK
Plastic
chop
stick
Falling
Fron
tal(orbital
medial)
NK
Craniotomy
No
Free
ofsymptom
Arslanetal
2012
13m
ale
Right18c
mIron
bar
Falling
Righto
rbitand
superio
rorbita
lfissure
Com
a(GCS
3)Right
frontop
arietal
craniotomy
No
Died
Shin
etal2012
38m
ale
Left14cm
Plastic
chop
stick
Falling
Superio
rorbita
lfissure
Blindn
ess
swellin
gnu
mbn
ess
arou
ndeye
Removalof
chop
stick
with
out
craniotomy
No
Blindn
ess
Katayamae
tal
2013
18m
ale
Right12c
mMetalrod
Falling
Fron
tal
(sub
zygomatic
bone)
Vomiting
NK
NK
Noneurological
deficit
Wangetal2013
35m
ale
Left18cm
Steel
Falling
Leftmaxillary
sinus
Limited
movem
ento
fneck
Craniotomy
No
Leftfacialpalsy
8 BioMed Research International
Table2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Skochetal2
013
35fe
male
MedialN
KElectric
toothb
rush
Accident
Tempo
ral
(lateralorbit)
Blurredvisio
npain
Mod
ified
frontotem
poral
orbitozygomatic
craniotomy
No
Improved
pain
andvisio
n
Deveere
tal
2013
43m
ale
Right5
6cm
Plastic
pen
Falling
Righto
rbit
No
NK
No
Free
ofsymptom
Yamasakietal
2013
4female
Left65c
mplastic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gNK
Meningitis
enceph
alitis
Free
ofsymptom
Williamse
tal
2014
56m
ale
LeftNK
Speargun
Suicidal
attempt
Subm
andibu
lar
region
oral
cavity
Com
aLargec
raniotom
yCerebritis
Died
ACAA
nteriorC
erebralA
rteryCS
FCerebrospinalFluidGCS
Glasgow
Com
aScaleICA
internalcarotid
arteryN
Kno
tkno
wn
BioMed Research International 9
(a)
(a)
(b)
(b)
(c)
(c)
(d)
lowast
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 3 Photography showed the entry point (black triangle 998787) of foreign body on face and incision for a frontotemporoorbitozygomaticapproach (a) Short piece of foreign body (simple arrow larr) in the face was exposed and removed by a maxillofacial surgeon (b) Theinfratemporal fossa was opened to expose the long piece of foreign body (c) and it (hollow arrow) was removed in a retrograde fashionDuring the removing process yellowish pus (asterisk lowast) was drained into the infratemporal fossa (d) Photography displayed short piece(simple arrowlarr) and long piece (hollow arrow) of the foreign body (e) Postoperative skull radiography suggested complete removal ofthe foreign body (f) The small bone fragment (hollow arrow head) was left in place due to its close relationship with branch of MCA (g)Three-month follow-up MRI revealed no abscess formation (h) The patient recovered uneventfully (i) MCA middle cerebral artery MRImagnetic resonance imaging
3D modeling has been frequently used in the presurgicalplanning of PSBIs in previous studies [8 11 15ndash17 19 2324 28] 3D models can be viewed in 360 degrees rotatedand studied from any perspective [29ndash31] which facilitate thediagnosis and operation to some extent [30 31] 3D Slicer is afree open source software that can be used for segmentation
and 3D modeling with high accuracy and reliability [30 32]It has been used in the management of various diseasesincluding intracranial aneurysms trigeminal neuralgia andintracerebral hematomas [29 30 33] PSBIs in our case serieswere reconstructed using 3D Slicer in which penetratingpoints as well as the surrounding neurovascular structures
10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
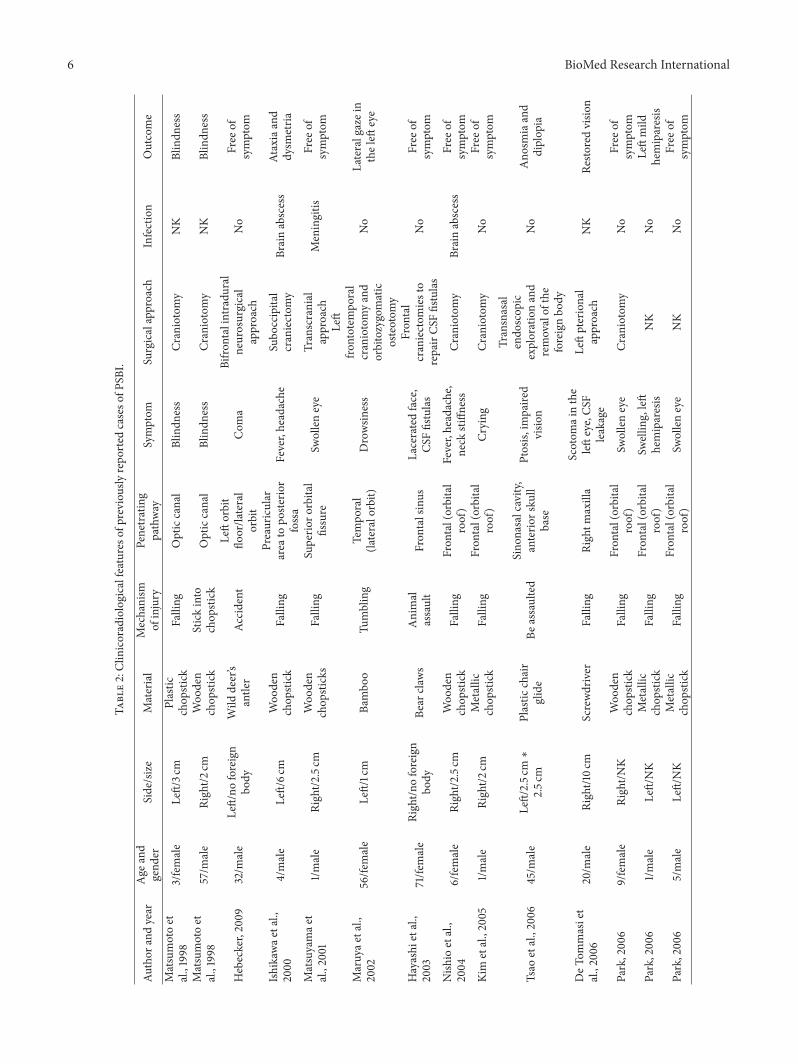
6 BioMed Research International
Table2Clinicoradiologicalfeatureso
fpreviou
slyrepo
rted
caseso
fPSB
I
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Matsumotoet
al1998
3female
Left3c
mPlastic
chop
stick
Falling
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Matsumotoet
al1998
57m
ale
Right2
cmWoo
den
chop
stick
Stickinto
chop
stick
Opticcanal
Blindn
ess
Craniotomy
NK
Blindn
ess
Hebecker2009
32m
ale
Leftno
foreign
body
Wild
deerrsquos
antler
Accident
Leftorbit
floorla
teral
orbit
Com
aBifro
ntalintradural
neurosurgical
approach
No
Free
ofsymptom
Ishikawae
tal
2000
4male
Left6c
mWoo
den
chop
stick
Falling
Preauricular
area
topo
sterio
rfossa
Feverheadache
Subo
ccipita
lcraniectom
yBrainabscess
Ataxiaand
dysm
etria
Matsuyamae
tal2001
1male
Right2
5cm
Woo
den
chop
sticks
Falling
Superio
rorbita
lfissure
Swolleneye
Transcranial
approach
Meningitis
Free
ofsymptom
Maruyae
tal
2002
56fe
male
Left1cm
Bambo
oTu
mbling
Tempo
ral
(lateralorbit)
Drowsin
ess
Left
frontotem
poral
craniotomyand
orbitozygomatic
osteotom
y
No
Lateralgazein
theleft
eye
Hayashi
etal
2003
71fe
male
Rightn
oforeign
body
Bear
claws
Animal
assault
Fron
talsinus
Laceratedface
CSFfistulas
Fron
tal
craniectom
iesto
repairCS
Ffistulas
No
Free
ofsymptom
Nish
ioetal
2004
6female
Right2
5cm
Woo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Feverheadache
neck
stiffn
ess
Craniotomy
Brainabscess
Fre e
ofsymptom
Kim
etal2005
1male
Right2
cmMetallic
chop
stick
Falling
Fron
tal(orbital
roof)
Crying
Craniotomy
No
Free
ofsymptom
Tsao
etal2006
45m
ale
Left25c
mlowast
25c
mPlastic
chair
glide
Beassaulted
Sino
nasalcavity
anterio
rsku
llbase
Ptosis
impaire
dvisio
n
Transnasal
endo
scop
icexplorationand
removalof
the
foreignbo
dy
No
Ano
smiaand
diplop
ia
DeT
ommasiet
al2006
20m
ale
Right10c
mScrewdriver
Falling
Rightm
axilla
Scotom
ainthe
lefteyeCS
Fleakage
Leftpterional
approach
NK
Resto
redvisio
n
Park200
69female
RightN
KWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
No
Free
ofsymptom
Park200
61m
ale
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gleft
hemiparesis
NK
No
Leftmild
hemiparesis
Park200
65male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
BioMed Research International 7Ta
ble2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Park200
62male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
Nitsch
etal
2007
22m
ale
Right2
cmNail-g
unAc
cident
Rightu
pper
jaw
totempo
rallob
eIntracerebral
haem
atom
a
Simplee
xtraction
ofthen
ailw
ithou
tac
raniotom
yNK
NK
Hira
ishi2007
5female
Left35c
mPlastic
chop
stick
Falling
Fron
tal(orbital
medial)
Feverheadache
neck
stiffn
ess
Craniotomy
Meningitis
brainabscess
Hyposmia
Kawada2009
5female
Left3c
mWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
Brainabscess
Free
ofsymptom
Mitilian
2009
4male
Right11cm
Woo
den
chop
stick
Falling
Superio
rorbita
lfissure
Mild
confusion
vomiting
Craniotomy
Brainabscess
Mild
dysm
etria
ofthea
rm
Wieland
etal
2010
58m
ale
Left-sid
edN
KWoo
denstick
Accident
Maxillofacialto
ethm
oidroof
Feverheadache
nausea
vomiting
mentalstatus
changes
Endo
scop
icrepair
ofthes
kullbase
defect
Intracranial
infection
NK
Hettig
eetal
2010
38fe
male
LeftNK
Plastic
chop
stick
Stum
ble
Poste
riorw
allof
theo
roph
aryn
xto
jugu
lar
foramen
into
the
poste
riorfossa
Nystagm
usleft
9th10thand
12th
cranial
nerves
palsy
qu
adrantanop
ia
Leftoccipital
craniotomy
retro
sigmoid
craniectom
y
No
Left9th10th
and12th
cranial
nerves
palsy
Sweeneyetal
2011
31m
ale
RightN
KKn
ifeSuicidal
attempt
Lower
jawto
anterio
rsku
llbase
Pain
Com
binedrig
htpte rionaland
interhem
ispheric
craniotomies
No
NK
Sweeneyetal
2011
21fe
male
RightN
KKn
ifeHom
icidal
attempt
Leftorbitto
middles
kull
base
Emesis
seizure
Leftcranioor-
bitozygomatic
approach
No
NK
Yonezawa2011
28m
ale
LeftNK
Plastic
chop
stick
Falling
Fron
tal(orbital
medial)
NK
Craniotomy
No
Free
ofsymptom
Arslanetal
2012
13m
ale
Right18c
mIron
bar
Falling
Righto
rbitand
superio
rorbita
lfissure
Com
a(GCS
3)Right
frontop
arietal
craniotomy
No
Died
Shin
etal2012
38m
ale
Left14cm
Plastic
chop
stick
Falling
Superio
rorbita
lfissure
Blindn
ess
swellin
gnu
mbn
ess
arou
ndeye
Removalof
chop
stick
with
out
craniotomy
No
Blindn
ess
Katayamae
tal
2013
18m
ale
Right12c
mMetalrod
Falling
Fron
tal
(sub
zygomatic
bone)
Vomiting
NK
NK
Noneurological
deficit
Wangetal2013
35m
ale
Left18cm
Steel
Falling
Leftmaxillary
sinus
Limited
movem
ento
fneck
Craniotomy
No
Leftfacialpalsy
8 BioMed Research International
Table2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Skochetal2
013
35fe
male
MedialN
KElectric
toothb
rush
Accident
Tempo
ral
(lateralorbit)
Blurredvisio
npain
Mod
ified
frontotem
poral
orbitozygomatic
craniotomy
No
Improved
pain
andvisio
n
Deveere
tal
2013
43m
ale
Right5
6cm
Plastic
pen
Falling
Righto
rbit
No
NK
No
Free
ofsymptom
Yamasakietal
2013
4female
Left65c
mplastic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gNK
Meningitis
enceph
alitis
Free
ofsymptom
Williamse
tal
2014
56m
ale
LeftNK
Speargun
Suicidal
attempt
Subm
andibu
lar
region
oral
cavity
Com
aLargec
raniotom
yCerebritis
Died
ACAA
nteriorC
erebralA
rteryCS
FCerebrospinalFluidGCS
Glasgow
Com
aScaleICA
internalcarotid
arteryN
Kno
tkno
wn
BioMed Research International 9
(a)
(a)
(b)
(b)
(c)
(c)
(d)
lowast
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 3 Photography showed the entry point (black triangle 998787) of foreign body on face and incision for a frontotemporoorbitozygomaticapproach (a) Short piece of foreign body (simple arrow larr) in the face was exposed and removed by a maxillofacial surgeon (b) Theinfratemporal fossa was opened to expose the long piece of foreign body (c) and it (hollow arrow) was removed in a retrograde fashionDuring the removing process yellowish pus (asterisk lowast) was drained into the infratemporal fossa (d) Photography displayed short piece(simple arrowlarr) and long piece (hollow arrow) of the foreign body (e) Postoperative skull radiography suggested complete removal ofthe foreign body (f) The small bone fragment (hollow arrow head) was left in place due to its close relationship with branch of MCA (g)Three-month follow-up MRI revealed no abscess formation (h) The patient recovered uneventfully (i) MCA middle cerebral artery MRImagnetic resonance imaging
3D modeling has been frequently used in the presurgicalplanning of PSBIs in previous studies [8 11 15ndash17 19 2324 28] 3D models can be viewed in 360 degrees rotatedand studied from any perspective [29ndash31] which facilitate thediagnosis and operation to some extent [30 31] 3D Slicer is afree open source software that can be used for segmentation
and 3D modeling with high accuracy and reliability [30 32]It has been used in the management of various diseasesincluding intracranial aneurysms trigeminal neuralgia andintracerebral hematomas [29 30 33] PSBIs in our case serieswere reconstructed using 3D Slicer in which penetratingpoints as well as the surrounding neurovascular structures
10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
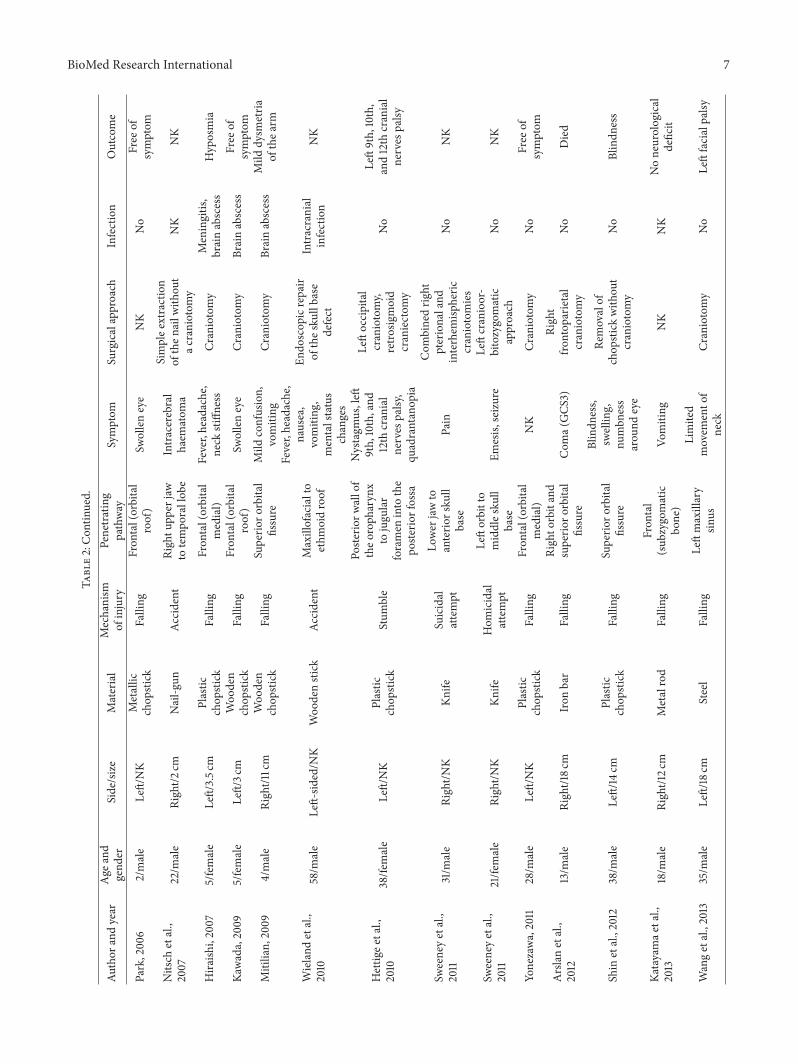
BioMed Research International 7Ta
ble2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Park200
62male
LeftNK
Metallic
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
NK
No
Free
ofsymptom
Nitsch
etal
2007
22m
ale
Right2
cmNail-g
unAc
cident
Rightu
pper
jaw
totempo
rallob
eIntracerebral
haem
atom
a
Simplee
xtraction
ofthen
ailw
ithou
tac
raniotom
yNK
NK
Hira
ishi2007
5female
Left35c
mPlastic
chop
stick
Falling
Fron
tal(orbital
medial)
Feverheadache
neck
stiffn
ess
Craniotomy
Meningitis
brainabscess
Hyposmia
Kawada2009
5female
Left3c
mWoo
den
chop
stick
Falling
Fron
tal(orbital
roof)
Swolleneye
Craniotomy
Brainabscess
Free
ofsymptom
Mitilian
2009
4male
Right11cm
Woo
den
chop
stick
Falling
Superio
rorbita
lfissure
Mild
confusion
vomiting
Craniotomy
Brainabscess
Mild
dysm
etria
ofthea
rm
Wieland
etal
2010
58m
ale
Left-sid
edN
KWoo
denstick
Accident
Maxillofacialto
ethm
oidroof
Feverheadache
nausea
vomiting
mentalstatus
changes
Endo
scop
icrepair
ofthes
kullbase
defect
Intracranial
infection
NK
Hettig
eetal
2010
38fe
male
LeftNK
Plastic
chop
stick
Stum
ble
Poste
riorw
allof
theo
roph
aryn
xto
jugu
lar
foramen
into
the
poste
riorfossa
Nystagm
usleft
9th10thand
12th
cranial
nerves
palsy
qu
adrantanop
ia
Leftoccipital
craniotomy
retro
sigmoid
craniectom
y
No
Left9th10th
and12th
cranial
nerves
palsy
Sweeneyetal
2011
31m
ale
RightN
KKn
ifeSuicidal
attempt
Lower
jawto
anterio
rsku
llbase
Pain
Com
binedrig
htpte rionaland
interhem
ispheric
craniotomies
No
NK
Sweeneyetal
2011
21fe
male
RightN
KKn
ifeHom
icidal
attempt
Leftorbitto
middles
kull
base
Emesis
seizure
Leftcranioor-
bitozygomatic
approach
No
NK
Yonezawa2011
28m
ale
LeftNK
Plastic
chop
stick
Falling
Fron
tal(orbital
medial)
NK
Craniotomy
No
Free
ofsymptom
Arslanetal
2012
13m
ale
Right18c
mIron
bar
Falling
Righto
rbitand
superio
rorbita
lfissure
Com
a(GCS
3)Right
frontop
arietal
craniotomy
No
Died
Shin
etal2012
38m
ale
Left14cm
Plastic
chop
stick
Falling
Superio
rorbita
lfissure
Blindn
ess
swellin
gnu
mbn
ess
arou
ndeye
Removalof
chop
stick
with
out
craniotomy
No
Blindn
ess
Katayamae
tal
2013
18m
ale
Right12c
mMetalrod
Falling
Fron
tal
(sub
zygomatic
bone)
Vomiting
NK
NK
Noneurological
deficit
Wangetal2013
35m
ale
Left18cm
Steel
Falling
Leftmaxillary
sinus
Limited
movem
ento
fneck
Craniotomy
No
Leftfacialpalsy
8 BioMed Research International
Table2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Skochetal2
013
35fe
male
MedialN
KElectric
toothb
rush
Accident
Tempo
ral
(lateralorbit)
Blurredvisio
npain
Mod
ified
frontotem
poral
orbitozygomatic
craniotomy
No
Improved
pain
andvisio
n
Deveere
tal
2013
43m
ale
Right5
6cm
Plastic
pen
Falling
Righto
rbit
No
NK
No
Free
ofsymptom
Yamasakietal
2013
4female
Left65c
mplastic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gNK
Meningitis
enceph
alitis
Free
ofsymptom
Williamse
tal
2014
56m
ale
LeftNK
Speargun
Suicidal
attempt
Subm
andibu
lar
region
oral
cavity
Com
aLargec
raniotom
yCerebritis
Died
ACAA
nteriorC
erebralA
rteryCS
FCerebrospinalFluidGCS
Glasgow
Com
aScaleICA
internalcarotid
arteryN
Kno
tkno
wn
BioMed Research International 9
(a)
(a)
(b)
(b)
(c)
(c)
(d)
lowast
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 3 Photography showed the entry point (black triangle 998787) of foreign body on face and incision for a frontotemporoorbitozygomaticapproach (a) Short piece of foreign body (simple arrow larr) in the face was exposed and removed by a maxillofacial surgeon (b) Theinfratemporal fossa was opened to expose the long piece of foreign body (c) and it (hollow arrow) was removed in a retrograde fashionDuring the removing process yellowish pus (asterisk lowast) was drained into the infratemporal fossa (d) Photography displayed short piece(simple arrowlarr) and long piece (hollow arrow) of the foreign body (e) Postoperative skull radiography suggested complete removal ofthe foreign body (f) The small bone fragment (hollow arrow head) was left in place due to its close relationship with branch of MCA (g)Three-month follow-up MRI revealed no abscess formation (h) The patient recovered uneventfully (i) MCA middle cerebral artery MRImagnetic resonance imaging
3D modeling has been frequently used in the presurgicalplanning of PSBIs in previous studies [8 11 15ndash17 19 2324 28] 3D models can be viewed in 360 degrees rotatedand studied from any perspective [29ndash31] which facilitate thediagnosis and operation to some extent [30 31] 3D Slicer is afree open source software that can be used for segmentation
and 3D modeling with high accuracy and reliability [30 32]It has been used in the management of various diseasesincluding intracranial aneurysms trigeminal neuralgia andintracerebral hematomas [29 30 33] PSBIs in our case serieswere reconstructed using 3D Slicer in which penetratingpoints as well as the surrounding neurovascular structures
10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
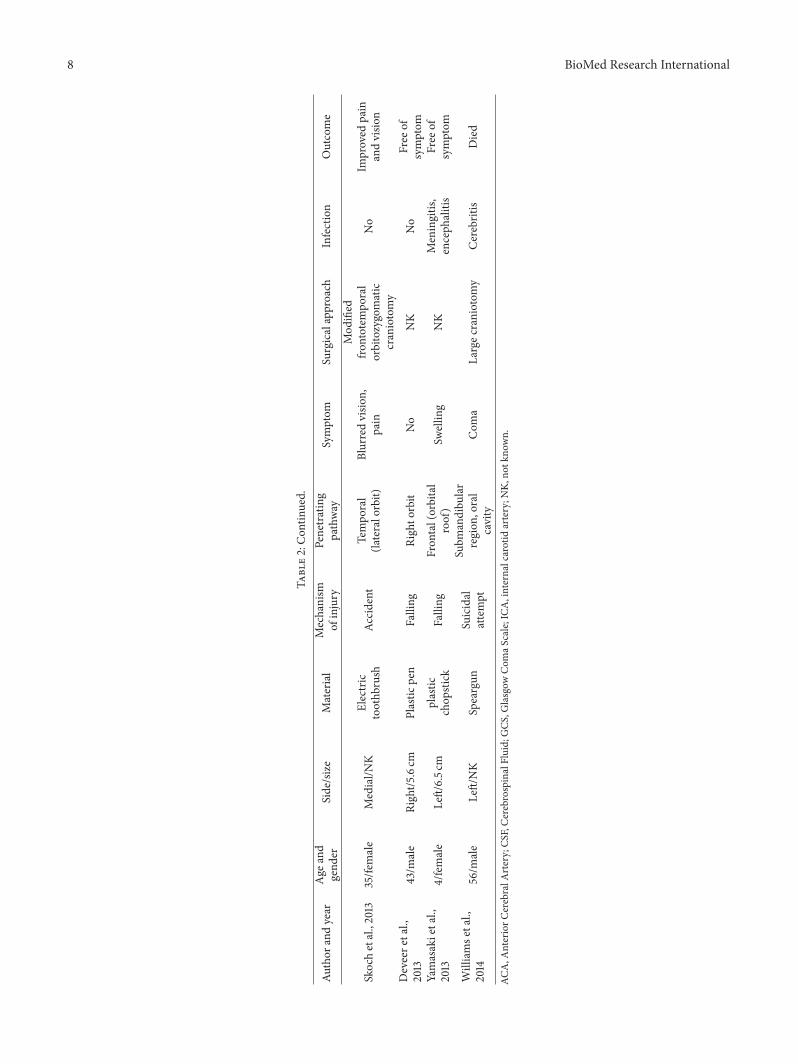
8 BioMed Research International
Table2Con
tinued
Author
andyear
Age
and
gend
erSidesize
Material
Mechanism
ofinjury
Penetrating
pathway
Symptom
Surgicalapproach
Infection
Outcome
Skochetal2
013
35fe
male
MedialN
KElectric
toothb
rush
Accident
Tempo
ral
(lateralorbit)
Blurredvisio
npain
Mod
ified
frontotem
poral
orbitozygomatic
craniotomy
No
Improved
pain
andvisio
n
Deveere
tal
2013
43m
ale
Right5
6cm
Plastic
pen
Falling
Righto
rbit
No
NK
No
Free
ofsymptom
Yamasakietal
2013
4female
Left65c
mplastic
chop
stick
Falling
Fron
tal(orbital
roof)
Swellin
gNK
Meningitis
enceph
alitis
Free
ofsymptom
Williamse
tal
2014
56m
ale
LeftNK
Speargun
Suicidal
attempt
Subm
andibu
lar
region
oral
cavity
Com
aLargec
raniotom
yCerebritis
Died
ACAA
nteriorC
erebralA
rteryCS
FCerebrospinalFluidGCS
Glasgow
Com
aScaleICA
internalcarotid
arteryN
Kno
tkno
wn
BioMed Research International 9
(a)
(a)
(b)
(b)
(c)
(c)
(d)
lowast
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 3 Photography showed the entry point (black triangle 998787) of foreign body on face and incision for a frontotemporoorbitozygomaticapproach (a) Short piece of foreign body (simple arrow larr) in the face was exposed and removed by a maxillofacial surgeon (b) Theinfratemporal fossa was opened to expose the long piece of foreign body (c) and it (hollow arrow) was removed in a retrograde fashionDuring the removing process yellowish pus (asterisk lowast) was drained into the infratemporal fossa (d) Photography displayed short piece(simple arrowlarr) and long piece (hollow arrow) of the foreign body (e) Postoperative skull radiography suggested complete removal ofthe foreign body (f) The small bone fragment (hollow arrow head) was left in place due to its close relationship with branch of MCA (g)Three-month follow-up MRI revealed no abscess formation (h) The patient recovered uneventfully (i) MCA middle cerebral artery MRImagnetic resonance imaging
3D modeling has been frequently used in the presurgicalplanning of PSBIs in previous studies [8 11 15ndash17 19 2324 28] 3D models can be viewed in 360 degrees rotatedand studied from any perspective [29ndash31] which facilitate thediagnosis and operation to some extent [30 31] 3D Slicer is afree open source software that can be used for segmentation
and 3D modeling with high accuracy and reliability [30 32]It has been used in the management of various diseasesincluding intracranial aneurysms trigeminal neuralgia andintracerebral hematomas [29 30 33] PSBIs in our case serieswere reconstructed using 3D Slicer in which penetratingpoints as well as the surrounding neurovascular structures
10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
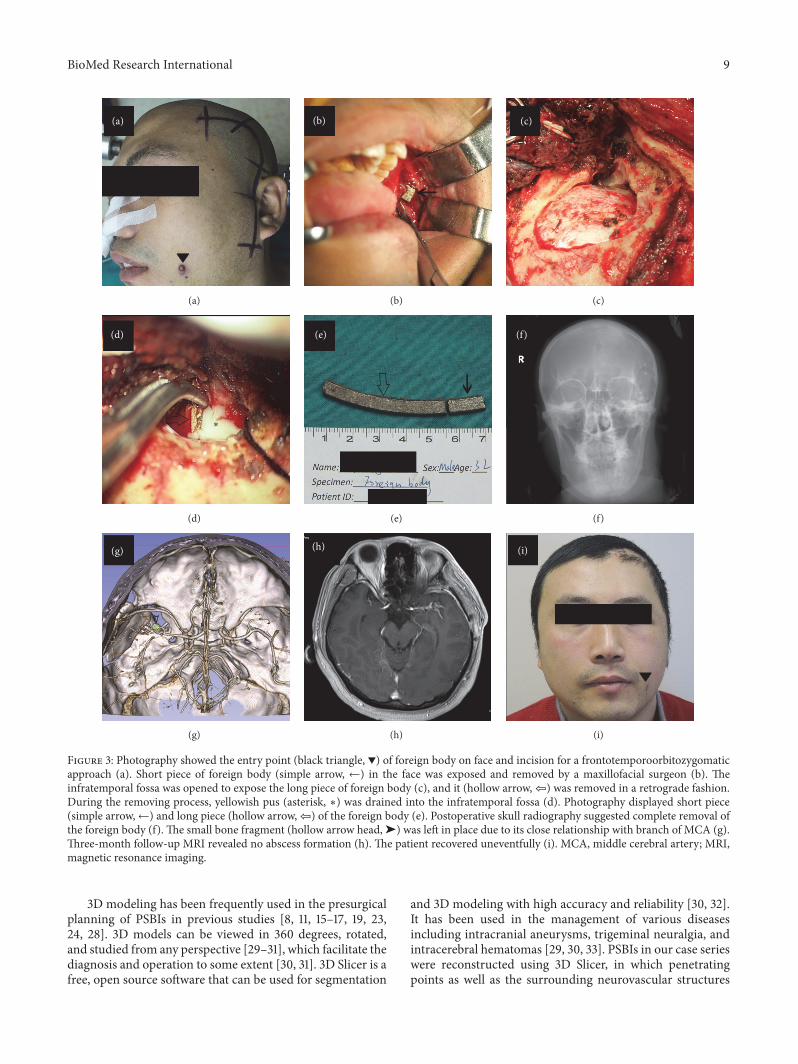
BioMed Research International 9
(a)
(a)
(b)
(b)
(c)
(c)
(d)
lowast
(d)
(e)
(e)
(f)
(f)
(g)
(g)
(h)
(h)
(i)
(i)
Figure 3 Photography showed the entry point (black triangle 998787) of foreign body on face and incision for a frontotemporoorbitozygomaticapproach (a) Short piece of foreign body (simple arrow larr) in the face was exposed and removed by a maxillofacial surgeon (b) Theinfratemporal fossa was opened to expose the long piece of foreign body (c) and it (hollow arrow) was removed in a retrograde fashionDuring the removing process yellowish pus (asterisk lowast) was drained into the infratemporal fossa (d) Photography displayed short piece(simple arrowlarr) and long piece (hollow arrow) of the foreign body (e) Postoperative skull radiography suggested complete removal ofthe foreign body (f) The small bone fragment (hollow arrow head) was left in place due to its close relationship with branch of MCA (g)Three-month follow-up MRI revealed no abscess formation (h) The patient recovered uneventfully (i) MCA middle cerebral artery MRImagnetic resonance imaging
3D modeling has been frequently used in the presurgicalplanning of PSBIs in previous studies [8 11 15ndash17 19 2324 28] 3D models can be viewed in 360 degrees rotatedand studied from any perspective [29ndash31] which facilitate thediagnosis and operation to some extent [30 31] 3D Slicer is afree open source software that can be used for segmentation
and 3D modeling with high accuracy and reliability [30 32]It has been used in the management of various diseasesincluding intracranial aneurysms trigeminal neuralgia andintracerebral hematomas [29 30 33] PSBIs in our case serieswere reconstructed using 3D Slicer in which penetratingpoints as well as the surrounding neurovascular structures
10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014

10 BioMed Research International
were clearly visualized It contributed to the presurgical plan-ning of optimal surgical approach and avoiding unexpectedvascular injury Our findings confirmed the feasibility andreliability of 3D Slicer in the modeling of foreign objects andadjacent neurovascular structures Moreover the segmenta-tion and modeling procedure using 3D Slicer allowed higherquality of visualization better view of objects and richerinformation than workstation reconstruction (Figures 1(g)2(g)ndash2(i) and 3(g)) [30] To our knowledge this is the firststudy to visualize PSBIs with 3D Slicer granting preoperativesurgical plan for proper approaches
43 Treatment of PSBIs Owing to the low incidence ofPSBIs prospective or controlled study is difficult to conducton the limited cases Temporary management of PBSIsconstantly depends on the experience of different institutions[7 15] Despite the availability of some complicated guidelinesfor penetrating brain injury they were mostly based onthe data of scattered cases without systematic summaryfor PSBIs [3 8ndash10] Thus we discussed the treatment ofPSBIs based on related cases we treated and previouslyreported
Operation is themajor strategy for the treatment of PSBIsIndications for surgery are retained objects CSF leakagefracture displacement intracranial hemorrhage and vascularinjury [34ndash38] The purpose of surgery is to remove foreignobjects decompress brain tissue and reconstruct skull baseGenerally operation is suggested in 12 hours after PSBIs [3940] However delayed operation is not recommended untilfull physical and radiological examination are performedsince premature surgery might lead to fatal results Arteryinjury is one of the common concurrent conditions thatshould be identified before surgery the presence of whichwillbe a disaster for emergent operation [16]
In PSBIs with vascular injuries protection of injuredarteries through preoperative endovascular occlusion orintraoperative artery control would be helpful in theremoval of foreign bodies [41] In contrast in PSBIs with-out vascular injuries foreign bodies could be removeddirectly [7] For some typical cases the metal foreign bod-ies or bone fragments are adjacent to important struc-tures and difficult to extract but cause no obvious symp-toms These foreign bodies could be retained in the brain(Case 2)
Surgical approach for skull base injury should be indi-vidualized according to the penetrating trajectory location offoreign body and accompanying vascular and brain injuriesIn current study different modifications of frontotemporoor-bitozygomatic approach were adopted tomanage the anteriorand middle skull base injuries By removing the superiorand lateral bony orbit we could deal with most of foreignbodies penetrating from the orbit into frontal lobe Theremoval of zygomatic arch enables inferior displacement oftemporalis muscle allowing exploration of undersurface oftemporal lobe Generally principles for skull base surgery canalso be applied to PSBIs Proximal vascular control shouldbe first guaranteed to prevent intraoperative hemorrhageAnd direct visualization of foreign object should be achievedbefore its removal Usually it is necessary to drill away the
bone of skull base to expose the foreign bodies Thoroughdebridement along the exposed trajectory as well as carefulreconstruction of the skull base is of great significance toprevent postoperative infection and CSF leakage Howeveraggressive debridement for deep seated debris should beavoided which may be associated with increased disabilityand mortality [20]
Infection is the main complication of PSBIs with areported overall rate of 64ndash70 and mortality rate of 14ndash57[42ndash44] Organic foreign body like wood or bamboo is notonly the carrier but also the best medium for infection suchas brain abscess meningitis and cerebritis [36 45] In thisway organic foreign bodies should be totally retrieved whilesome other deep seated foreign bodies such as small metalor bone fragments could be retained since total extractionwould cause more damage In the absence of sufficient dataand definitive guidelines the type timing and durationof antibiotic use remains uncertain especially when theresult of CSF culture is negative In recent publicationsprophylactic use of broad-spectrum antibiotic was suggestedwithin 7ndash14 days after the injury [16 39] while othersindicated that antibiotic therapy should be administratedaccording to the findings of CSF culture [46] We recom-mended prophylactic use of antibiotics and proper adjust-ment according to CSF culture results especially for woodenobjects
5 Conclusions
PSBI is a rare disease with various injury mechanismsand complicated traumatic conditions Lots of difficultiesregarding the diagnosis and management of PSBIs remain tobe solved Based on our experience and review of previousstudies we suggest full physical examination and radio-logical evaluation before surgery Preoperative 3D model-ing with 3D Slicer could help visualize penetrating path-way and surrounding neurovascular structures in detailgranting free view from any angle and selection of opti-mal approach However caution is needed in interpretingour findings because of the limited cases Further largescale prospective studies are required to identify the effectof preoperative 3D reconstruction on the prognosis ofPSBIs as well as the guideline for the management ofPSBIs
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article
Authorsrsquo Contributions
Danfeng Zhang performed data collection data analysis andwriting of the article Jigang Chen collaborated in literaturesearch and study design Kaiwei Han collaborated in figuregeneration and study design Mingkun Yu collaborated instudy design data analysis and editing of the article LijunHou collaborated in literature research figure generation andediting of the article
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International 11
References
[1] T A Gennarelli H R Champion W J Sacco W S Copesand W M Alves ldquoMortality of patients with head injuryand extracranial injury treated in trauma centersrdquo Journal ofTrauma vol 29 no 9 pp 1193ndash1201 1989
[2] Y Hayashi H Fujisawa Y Tohma J Yamashita and H InabaldquoPenetrating head injury caused by bear claws case reportrdquoJournal of Trauma - Injury Infection and Critical Care vol 55no 6 pp 1178ndash1180 2003
[3] J Maruya et al ldquoBrain abscess following transorbital penetrat-ing injury due to bamboo fragmentsmdashcase reportrdquo Neurol MedChir (Tokyo) vol 42 no 3 pp 143ndash146 2002
[4] M S Walid J C Yelverton and J S Robinson Jr ldquoPenetratingorbital trauma with internal carotid injuryrdquo Southern MedicalJournal vol 102 no 1 pp 116-117 2009
[5] A Agrawal A Pratap C S Agrawal A Kumar and SRupakheti ldquoTransorbital orbitocranial penetrating injury dueto bicycle brake handle in a childrdquo Pediatric Neurosurgery vol43 no 6 pp 498ndash500 2007
[6] F H Chowdhury M R Haque Z Hossain N K ChowdhurySMAlam andMH Sarker ldquoNonmissile Penetrating Injury tothe Head Experience with 17 Casesrdquo World Neurosurgery vol94 pp 529ndash543 2016
[7] M Schreckinger DOrringer B GThompson F LaMarca andO Sagher ldquoTransorbital penetrating injury Case series reviewof the literature and proposed management algorithm Reportof 4 casesrdquo Journal ofNeurosurgery vol 114 no 1 pp 53ndash61 2011
[8] M Deveer F Imamoglu C Imamoglu and S Okten ldquoAnincidental case of asymptomatic intracranial foreign body onCTrdquo BMJ case reports vol 2013 2013
[9] S Hettige K Kok P Epaliyanage and N W M ThomasldquoChopstick injury penetrating the skull base A case reportrdquoSkull Base vol 20 no 3 pp 219ndash222 2010
[10] A De Tommasi P Cascardi C De Tommasi S Luzzi and PCiappetta ldquoEmergency surgery in a severe penetrating skullbase injury by a screwdriver Case report and literature reviewrdquoWorld Journal of Emergency Surgery vol 1 no 1 article 36 2006
[11] J Skoch T L Ansay and G M Lemole ldquoInjury to the temporallobe via medial transorbital entry of a toothbrushrdquo Journal ofNeurological Surgery Reports vol 74 no 1 pp 23ndash28 2013
[12] E Ishikawa K Meguro K Yanaka et al ldquoIntracerebellar pene-trating injury and abscess due to a wooden foreign bodymdashcasereportrdquo Neurologia Medico-Chirurgica vol 40 no 9 pp 458ndash462 2000
[13] S Matsumoto K Hasuo A Mizushima et al ldquoIntracranialpenetrating injuries via the optic canalrdquo AJNR AmericanJournal of Neuroradiology vol 19 no 6 pp 1163ndash1165 1998
[14] A MWielandW T Curry M L Durand and E H HolbrookldquoManagement of a long-standing organic intracranial foreignbodyrdquo Skull Base vol 20 no 6 pp 487ndash490 2010
[15] J M Sweeney J J Lebovitz J L Eller J R Coppens RD Bucholz and S I Abdulrauf ldquoManagement of nonmissilepenetrating brain injuries a description of three cases andreview of the literaturerdquo Skull Base vol 1 no 1 pp 39ndash46 2011
[16] J R Williams D M Aghion C E Doberstein R G CosgroveandW F Asaad ldquoPenetrating brain injury after suicide attemptwith speargun case study and review of literaturerdquo Frontiers inNeurology vol 5 article 113 2014
[17] A Nitsch R Verheggen and H-A Merten ldquoPenetratingpneumatic nail-gun injury to skull baserdquo British Journal of Oraland Maxillofacial Surgery vol 45 no 8 p 692 2007
[18] Y Wang L Pan and H Xu ldquoThe surgical treatment of rein-forced steel bar injury penetrating the skull base and maxilla-mandibular areardquo Journal of Craniofacial Surgery vol 25 no 6pp e521ndashe523 2014
[19] K Katayama N Shimamura Y Ogasawara M Naraoka andH Ohkuma ldquoTranslucent three-dimensional CT is useful inconsidering the treatment strategy for the penetrating skullbase injury with a metal rod Case reportrdquo Neurologia Medico-Chirurgica vol 53 no 9 pp 613ndash615 2013
[20] M Arslan M Eseoglu B O Gudu and I Demir ldquoTransorbitalorbitocranial penetrating injury caused by a metal barrdquo Journalof Neurosciences in Rural Practice vol 3 no 2 pp 178ndash181 2012
[21] T Matsuyama et al ldquoTransorbital penetrating injury by achopstickmdashcase reportrdquo Neurol Med Chir (Tokyo) vol 41 no7 pp 345ndash348 2001
[22] Y-H Tsao C-H Kao H-W Wang S-C Chin and K SMoe ldquoTransorbital penetrating injury of paranasal sinusesand anterior skull base by a plastic chair glide Managementoptions of a foreign body in multiple anatomic compartmentsrdquoOtolaryngology - Head and Neck Surgery vol 134 no 1 pp 177ndash179 2006
[23] F Yamasaki H Ohge R Tsumura et al ldquoTransorbital penetrat-ing intracranial injury by a chopstick a case report and reviewof the literaturerdquo No Shinkei Geka vol 41 no 11 pp 1001ndash10092013
[24] S Kim J Y Lee J S Song and J Oh ldquoTransorbital-intracranialinjury by a chopstick Three-dimensional computed tomogra-phyrdquoActaOphthalmologica Scandinavica vol 83 no 5 pp 609-610 2005
[25] H Imokawa T Tazawa N Sugiura D Oyake and K YosinoldquoPenetrating neck injuries involvingwooden foreign bodies therole of MRI and the misinterpretation of CT imagesrdquo AurisNasus Larynx vol 30 pp S145ndashS147 2003
[26] A Carothers ldquoOrbitofacial Wounds and Cerebral ArteryInjuries Caused by Umbrella Tipsrdquo JAMA The Journal of theAmerican Medical Association vol 239 no 12 pp 1151-11521978
[27] R Eidsness D J Coupal M E B Kelly and S HattinghldquoTraumatic orbital injuryrdquo Journal of TraumamdashInjury Infectionand Critical Care vol 62 no 5 pp 1286-1287 2007
[28] T-H Shin J-H Kim K-WKwak and S-H Kim ldquoTransorbitalpenetrating intracranial injury by a chopstickrdquo Journal ofKorean Neurosurgical Society vol 52 no 4 pp 414ndash416 2012
[29] X Xu X Chen J Zhang et al ldquoComparison of the tada formulawith software slicer Precise and low-cost method for volumeassessment of intracerebral hematomardquo Stroke vol 45 no 11pp 3433ndash3435 2014
[30] K-W Han D-F Zhang J-G Chen and L-J Hou ldquoPresurgicalvisualization of the neurovascular relationship in trigeminalneuralgia with 3D modeling using free Slicer softwarerdquo ActaNeurochirurgica vol 158 no 11 pp 2195ndash2201 2016
[31] B You Y Cheng J Zhang et al ldquoApplication of contrast-enhanced T1-weighted MRI-based 3D reconstruction of thedural tail sign in meningioma resectionrdquo Journal of Neuro-surgery vol 125 no 1 pp 46ndash52 2016
[32] A Fedorov R Beichel J Kalpathy-Cramer et al ldquo3D sliceras an image computing platform for the quantitative imagingnetworkrdquoMagnetic Resonance Imaging vol 30 no 9 pp 1323ndash1341 2012
[33] A Can A Mouminah A L Ho and R Du ldquoEffect of vascularanatomy on the formation of basilar tip aneurysmsrdquo Neuro-surgery vol 76 no 1 pp 62ndash66 2015
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
12 BioMed Research International
[34] J Fezza and R Wesley ldquoThe Importance of CT Scans inPlanning the Removal of Orbital-Frontal Lobe Foreign BodiesrdquoOphthalmic Plastic amp Reconstructive Surgery vol 15 no 5 pp366ndash368 1999
[35] K A Greene C A Dickman K A Smith E J Kinder and JMZabramski ldquoSelf-inflicted orbital and intracranial injury witha retained foreign body associated with psychotic depressionCase report and reviewrdquo Surgical Neurology vol 40 no 6 pp499ndash503 1993
[36] S A Sadiq and G Thurairajan ldquoA case of transorbital intracra-nial damage underlying a seemingly innocuous injuryrdquo Injuryvol 26 no 4 pp 279-280 1995
[37] K A Szabo S H Cheshier M Y S Kalani J W Kim andR Guzman ldquoSupraorbital approach for repair of open anteriorskull base fracture case reportrdquo Journal of Neurosurgery Pedi-atrics vol 2 no 6 pp 420ndash423 2008
[38] T Yamashita T Mikami T Baba et al ldquoTransorbital intracra-nial penetrating injury from impaling on an earpickrdquo Journal ofNeuro-Ophthalmology vol 27 no 1 pp 48-49 2007
[39] S F Kazim M S Shamim M Z Tahir S A Enam and SWaheed ldquoManagement of penetrating brain injuryrdquo Journal ofEmergencies Trauma and Shock vol 4 no 3 pp 395ndash402 2011
[40] T S Helling W Kendall McNabney C Keith Whittaker CC Schultz and M Watkins ldquoThe role of early surgical inter-vention in civilian gunshot wounds to the headrdquo Journal ofTraumamdashInjury Infection and Critical Care vol 32 no 3 pp398ndash400 1992
[41] E J Cunningham B Albani T J Masaryk et al ldquoTemporaryballoon occlusion of the cavernous carotid artery for removal ofan orbital and intracranial foreign body technical case reportrdquoNeurosurgery vol 55 no 5 p 1225 2004
[42] Y Nishio N Hayashi H Hamada Y Hirashima and S EndoldquoA case of delayed brain abscess due to a retained intracranialwooden foreign body a case report and review of the last 20yearsrdquoActa Neurochir (Wien) vol 146 no 8 pp 847ndash850 2004
[43] C F Miller J S Brodkey and B J Colombi ldquoThe danger ofintracranial woodrdquo Surg Neurol vol 7 no 2 pp 95ndash103 1977
[44] Q Chunhua andW Qun ldquoA late-onset seizure due to a retainedintracranial foreign body-pencil lead a case report and reviewrdquoJournal of Craniofacial Surgery vol 25 no 2 pp e109ndashe1102014
[45] I F Dunn D H Kim P A Rubin R Blinder J Gates and A JGolby ldquoOrbitocranial wooden foreign body a pre- intra- andpostoperative chronicle case reportrdquo Neurosurgery vol 65 no2 pp E383ndashE384 2009
[46] R Gutierrez-Gonzalez G R Boto M Rivero-Garvıa A Perez-Zamarron andGGomez ldquoPenetrating brain injury by drill bitrdquoClinical Neurology andNeurosurgery vol 110 no 2 pp 207ndash2102008
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Submit your manuscripts athttpswwwhindawicom
Neurology Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Alzheimerrsquos DiseaseHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
International Journal of
ScientificaHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentSchizophrenia
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neural Plasticity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAutism
Sleep DisordersHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neuroscience Journal
Epilepsy Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Psychiatry Journal
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
Depression Research and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Brain ScienceInternational Journal of
StrokeResearch and TreatmentHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Neurodegenerative Diseases
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
Cardiovascular Psychiatry and NeurologyHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Recommended
















