Embed Size (px)
Citation preview
PENETRATING ABDOMINAL INJURYTIPS & TRICKS
HARYONO YARMAN
ACUTE CARE SURGERY
BANDUNG, FEBRUARY 24, 2018

Topics :1. Prehospital Care : Time, Initial Resuscitation - Avoid over resuscitation, Triad of Death ,
2. Damage Control Resuscitation in Penetrating Trauma: Rules of the Game
3. Determining for Massive Transfusion
4. EAST Recommendations
5. Emergency Laparotomy
6. DCS
Prehospital CareWhen caring for critically ill trauma patients in the prehospital environment :
Time is the single most important factor
Scene time ≥ 20 min was associated with higher odds of mortality than a scene time less than10 min,
The goal is 7 min ALS scene time & 7 min ALS transport time.
“ Treat During Transport.”
The main object of prehospital care is : Get the patient to the highest level trauma center in the shortest possible time
Time to hemorrhage control is a key determinant of outcome for PT patients
Prehospital Care Avoid over-resuscitation ;
A minimal perfusion blood pressure is adequate
Aggressive crystalloid infusion, targeting endpoints : Restoring blood volume
CVP
Worsening the lethal triad of hypothermia, acidosis, coagulopathy.
Triad of Death :Severe hypothermia : a temperature less than 32 °C, correlate with 100 % mortality.
Moderate hypothermia : a temperature between 32 °C and 34 °C, has been associated with a mortality rate of about 14 %.
Mild hypothermia is from 34 °C to 36 °C.
Hypothermia impairs : platelet function
coagulation cascade enzyme activities.
With prolonged extrication times :
heat loss, intoxication, and potentially open body cavities,
trauma patients with hemorrhagic shock have an uncoupling of metabolic pathways resulting in the loss of normal thermoregulatory mechanisms
Tips : All trauma patients should receive :
Warmed fluids,
Passive Adjuncts & Active Adjuncts for warming, to achieve normothermia (36–37 °C, 96.8–98.6 °F)
Triad of Death : Acidosis, generally results from lactic acid production from anaerobic metabolism insufficient oxygen delivery to peripheral tissues.
Oxygen delivery is reduced by : Decreased oxygen-carrying capacity ( Decreased Hb ),
Poor oxygen diffusion,
Decreased cardiac output (pump capacity or intravascular volume).
pH less than 7.2 affects cellular functions such as : ATP generation, fatty acid biosynthesis, & enzymatic reactions
Patients with a pH of less than 7.0 have an ± 70 % mortality rate.

Triad of Death : Hypothermia and Acidosis both contribute to and are exacerbated by the final arm of the triad,
Coagulopathy.
Coagulopathy : Consumption of clotting factors
Dilution of these factors and platelets due to aggressive crystalloid resuscitation.
Trauma-Specific Endogenous Mechanisms of Coagulopathy / Primary Coagulopathy These include activation of the thrombomodulin-protein C system, platelet dysfunction,
endothelial dysfunction, oxidative modification, and hyperfibrinolysis.
Which may be worsened by the rapid administration of crystalloid fluids.
Tips : Crystalloid administration :
Worsening the lethal triad by worsening dilutional coagulopathy.
Do not carry oxygen nor do they clot.
It has become clear that :Significant blood loss must be replaced with blood
The Initial Approach of Resuscitation : Patients who present with class I/II hemorrhage :
Use of small volumes of crystalloid :
Such that the deleterious effects of volume overload are avoided
Maintaining both Macroperfusion and Microperfusion
The Initial Approach of Resuscitation :Large-volume crystalloid resuscitation in the face of exsanguinating hemorrhage :
1. Macroscopically cause :1. Edema of the Gut, Myocardium, and Skeletal Muscles,
2. Compartment Syndrome
3. Acute Respiratory Distress Syndrome
2. Microscopically : 1. Induce Tissue Hypoxia
2. Free-Radical Injury
leading to derangements of cellular, metabolic, and immune functions.
The Initial Approach of Resuscitation : Damage Control Resuscitation :
is an Early Coordinated Effort to improve outcomes in injured patients
Two major concepts have become standard practice :
1. Hypotensive resuscitation
2. Haemostatic resuscitation
Large-Volume Crystalloid infusion has largely been replaced by Blood Product Transfusion
Ratios of Red Blood Cells : Plasma : Platelets approaching 1:1:1 or 1:1:2
Even when ratios are maintained, increasing volume of crystalloid is a predictor of mortality
The Initial Approach of Resuscitation :• Patients in hemorrhagic shock :
• who do not respond to an Initial Small Volume Bolus of NaCl 0,9% or RL solution :• Blood products in a 1:1:1 or 1:2:1 ratio,
• With Little to No crystalloid solution,
• Along with efforts to Control Source of Hemorrhage :
• Either temporarily, or definitively
• if able to be achieved outside of the operating room
Adjuncts to Massive Transfusion : Tranexamate acid should be considered
Determining Need for Massive Transfusion •The need for ≥10 unit PRBCs in the first 24 h
•The Trauma-Associated Severe Hemorrhage (TASH) Score
• Cohort of blunt trauma patients
•Relatively complicated calculation of 7 variables : 1. Systolic Blood Pressure,
2. Sex,
3. Hemoglobin,
4. FAST,
5. Heart Rate,
6. Base Excess (BE),
7. Extremity or Pelvic Fractures
•The possible range of scores is between 0 and 28,• each point corresponds to increased risk,
• 100 % of ptnts with a score ≥27 require Massive Transfusion.
•The Assessment of Blood Consumption (ABC) Score
•Simpler to derive.
•Consist of : 1. Mechanism of Injury (Penetrating vs. Blunt)
2. Systolic Blood Pressure ≤ 90 mmHg on ER arrival,
3. Heart Rate ≥120 /m on ER arrival,
4. Positive FAST,
•where each parameter equals 1 point
•85 % of patients with a score of ≥2 will require massive transfusion
TIPS :
•all hospitals should establish Massive Transfusion Protocols (MTPs) :
• Based on local resources
• Designed to bring appropriate balanced ratio of blood products to the patient < 10 minutes.
Hypotensive , Controlled & Delayed Resuscitation Hypotensive Resuscitation, infusion rates are adjusted to maintain a goal blood pressure
(typically MAP of 40–50 mmHg or SBP of 80–90 mmHg).
Controlled Resuscitation, useful in prehospital or austere environments where sphygmomanometry may not be available,
rate of fluid infusion is maintained at a predetermined rate (60–80 mL/ kg/h) ,there is little chance of achieving normotension.
Delayed Resuscitation, fluids are withheld until definitive hemorrhage control,
useful in areas with short transport times.
Hypotensive , Controlled & Delayed Resuscitation
Hypoperfusion of this magnitude may be tolerated for 60 minutes, beyond that physiological reserve will be exhausted,
MOD is the rule, and mortality is extremely high.
Resuscitation is not a substitute for early hemorrhage control !!
Recommendations : EAST J Trauma 2010 Mar; 68(3) : 721-33
1. Hemodynamically Unstable or have Diffuse Abdominal Tenderness Laparotomy
2. Routine laparotomy is not indicated in hemodynamically stable ptnts w SW without signs of Peritonitis
3. Routine laparotomy is not indicated in hemodynamically stable ptnts w GSW if the wounds are tangential & no peritoneal signs
4. Serial physical examination is reliable in detecting significant injuries after PAI
5. In ptnts selected for initial NOM, abdominopelvic CT should be strongly considered to facilitate initial management decisions
6. The vast majority NOM ptnts may be discharged after 24 hours of observation in the presence of a reliable abdominal examination & minimal to no abdominal tenderness

Recommendations : EASTJ Trauma 2010 Mar; 68(3) : 721-33
Non tangensial GSW with no generalized abdominal tenderness & is hemodynamically stable :
no consensus :
Some operate
Some other : try NOM
depend on :Degree of expertise , Structure of the trauma center , Imaging , Diagnostic Laparoscopy
Laparoscopy in PAIThe goal of diagnostic laparoscopy :
Prevent unnecessary laparotomies
Laparoscopy reduce the rate of negative laparotomies
Laparotomy must be performed in patients where any doubt of injury remains
If hemodynamically unstable or multiple injuries are suspected, do not attempt laparoscopy
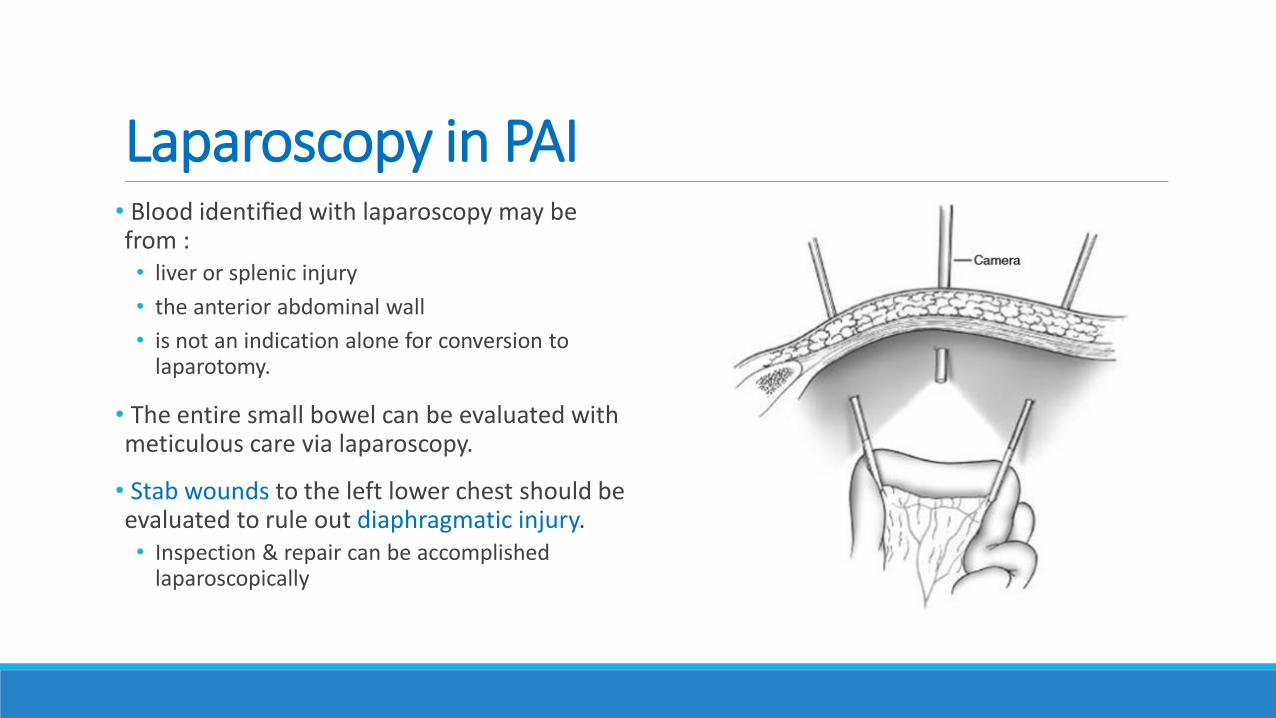
Laparoscopy in PAI• Blood identified with laparoscopy may be from :• liver or splenic injury
• the anterior abdominal wall
• is not an indication alone for conversion to laparotomy.
• The entire small bowel can be evaluated with meticulous care via laparoscopy.
• Stab wounds to the left lower chest should be evaluated to rule out diaphragmatic injury. • Inspection & repair can be accomplished
laparoscopically

Surgical Strategies in Penetrating Trauma to the Abdomen and Pelvis
Emergency Laparotomy George C. Velmahos
1. Position and Preparation : Supine / Preparation Neck – Mid Thigh
2. Incision : Long Mid Line
3. Bleeding and Contamination Control
4. Systematic Exploration
5. Closure
Bleeding & Contamination Control Blind packing is ineffective and unnecessary.
Suction the blood that is in the abdomen and localize its source.
Pack this area meaningfully to achieve temporary control.
Make sure there is no other bleeding site. Often, there is more than one.
Focus now on control of contamination
Have a quick look for perforations
If there is any, control it by placing a Babcock clamp or a quick occluding suture.
Bleeding & Contamination temporarily controlled
Return to the bleeding site : Unpack carefully & Check the extent of the injury
If there is something that can easily be repaired or ligated, then do so.
Otherwise, repack, as your next step is to explore the entire abdomen
Systematic Exploration The exploration of the abdominal cavity should be performed systematically,
I always start from the left upper quadrant and visualize : Stomach, Spleen, Left diaphragm, and Left Lobe of the Liver.
Then move to the right upper quadrant :
Retracting the Liver & visualizing its superior and inferior surfaces,
The Right Diaphragm, the Duodenum, and the Hepatic hilum.
The assistant holds up the transverse mesocolon and the surgeon pulls all the small boweltoward the right side This exposes the ligament of Treitz,
The exploration of the small bowel begins by “running” it segment by segment
Inspect the anterior and posterior surfaces of it up to the ileocolic area
The colon is inspected in detail all the way to the rectum and the peritoneal reflection.
The pelvis is checked for retroperitoneal hematomas
Damage Control Surgery Standard of care for the severely injured patient
Minimising the physiological insult : by performing only essential surgery :
Control of Haemorrhage and Contamination
Avoidance of prolonged reconstructive surgery.

Damage Control Surgery Stages of Damage Control
is regarded as having 5 Stages :
1. Stage 1: Patient selection
2. Stage 2: Operative control of haemorrhage and contamination
3. Stage 3: Resuscitation in the intensive care unit (ICU)
4. Stage 4: Definitive surgery
5. Stage 5: Closure of the abdomen
Riaan Pretorius , Frank Plani , Kenneth D. Boffard
Stage 1 : Indications for Damage Control( Patients Selection )
PHYSIOLOGICAL PARAMETERS :
1. Nonresponder to resuscitation with SBP <70 mmHg
2. Temp <34 °C
3. pH <7.2
4. Lactate > 5 mmol/L
5. Worsening of intraoperative acidosis, hypothermia and coagulopathy
6. Increased inotropic requirements during surgery
ANATOMICAL PARAMETERS :
1. Injury Severity Score (ISS) > 25
2. Multiple cavity / Multiple injuries that will need prolonged surgery to correct
3. Massive transfusion or fluid resuscitation with risk of ACS
4. Packing to control haemorrhage
5. Severe contamination
Stage 2: Operative Control of Haemorrhage & Contamination
GENERAL PRINCIPLES :
1. Needs a team effort.
2. The Anaesthetic Team should adopt the Haemorrhagic Resuscitation Principles, • cutting down on their clear fluids,
3. The Nursing Staff should have a trauma cupboard ready with all possible equipment available for DCS
4. The patient should be cleaned from the chin to the knees,
5. Temperature in the OR should be as high as possible (36 °C),
6. Warm fluids should be used all to combat hypothermia
7. Continuous communication between all the parties involved :◦ The surgeon should inform all about the injuries sustained and ongoing blood loss and planned surgery
◦ The Anaesthetist should keep the Surgeon & ICU informed about :◦ The physiological status, inotropic , units of blood transfused & the duration of the surgery.
Stage 2: Operative Control of Haemorrhage & Contamination
Solid Organs :
Haemorrhage is the most pressing problem in the abdomen and is usually dealt with by a combination of suturing, packing or removal of the organ
Spleen
Splenectomy is the treatment of choice for the unstable patient
Sometimes packs need to be left in the splenic bed to control oozing (especially in thecoagulopathic patient) post-splenectomy.
Stage 2: Operative Control of Haemorrhage & Contamination
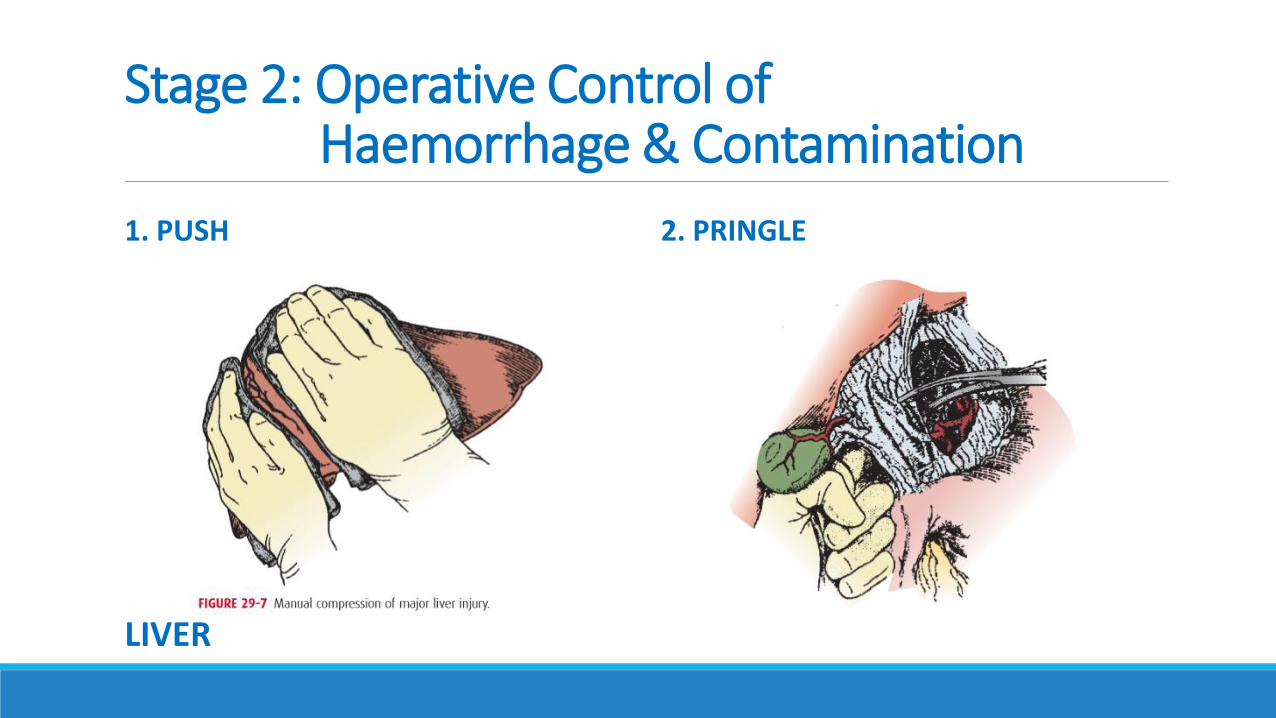
1. PUSH 2. PRINGLE
LIVER
Stage 2: Operative Control of Haemorrhage & Contamination
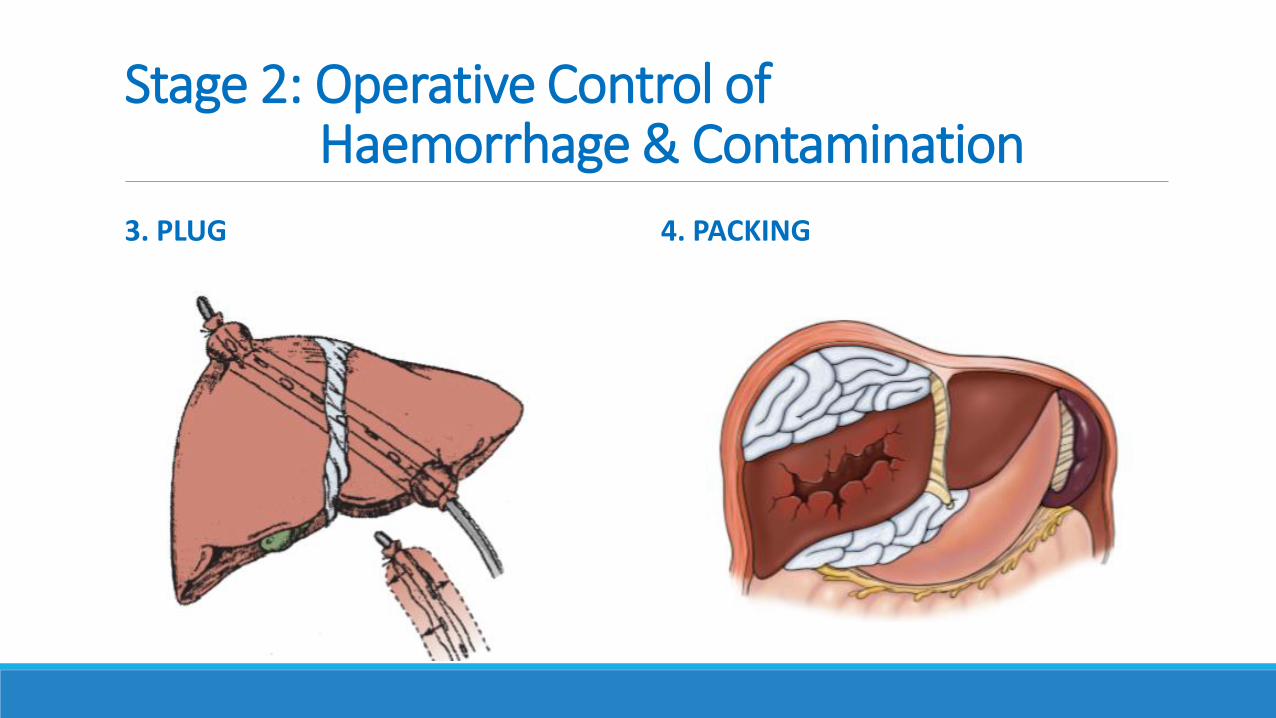
3. PLUG 4. PACKING
Stage 2: Operative Control of Haemorrhage & Contamination
Hollow Viscus Injuries :
Control of contamination and can be done by :
Primarily repair, stapling, ligation or diversion, shunt or drainage.
TACD
Trick : To prevent adhesions , insert TACD between viscera & abdominal wall
RESUSCITATION AFTER BLEEDING CONTROL
After the bleeding vessel is controlled , by clamp or suture :
Resuscitation should be aimed at :Preventing damage to the cardiorespiratory system leading to hypoperfusion & tissue hypoxia.
This is accomplished by :Low volume boluses of Crystalloid or Blood Products 250–500 mL is given to maintain MAP 65 mmHg.
Blood products should be used preferentially for ongoing bleeding and coagulopathies.
Stage 3: Resuscitation in ICU
Correction of Hypothermia
Correction of Acidosis
Correction of Coagulopathy
Resuscitation EndpointsClassic Markers :
Blood pressure >100 mmHg,
Heart rate <90 beats per minute,
Pulse oximetry >92 %,
Urine output >0.5 ml/kg/h,
Hemoglobin >7 gm/dL,
Normothermia.
Normal Coagulation Profile,
Normal Cardiac Output,
pH,
Lactate,
Base deficit,
Mixed venous saturation.
Stage 4 : Definitive Surgery Ideally the patient should be taken back to theatre :
As soon as the Endpoints of Resuscitation are achieved : Reverse of acidosis, coagulopathy and hypothermia
Mixed venous saturation >70 %
On optimal dose of inotropes that would allow safe bowel anastomosis
Within the first 24–48 h
Stage 4 : Definitive Surgery Removal of all packs
If there is still bleeding after removal of packs, repacking might be indicated
Exclusion of possible missed injuries
Restoration of anatomy : Includes bowel anastomosis, stomas construction depending on physiology and the nature of the injury
Stage 5: Definitive Closure of the Abdomen The decision to close the abdomen will depend on:
Timing since initial surgery :
The longer the delay since the initial surgery, the more the anterior abdominal wall retracts , at a stage the abdomen can’t be closed due to tension on the sheath.
Ideally, the abdominal wall should be closed within 5 days
Closure of the abdomen could be managed as :
1. Initial primary closure
2. Closure with possibility ventral hernia will developed that would be closed at a later stage. Intra-abdominal oedema
Intra-abdominal contamination

PAI SummaryTIPS
1. Get the unstable ptnt as soon as possible to highest rank hospital
2. Limited fluid resuscitation / Hypotensive resuscitation
3. Early blood components
4. Build Massive Transfusion Protocol in our hospital
5. Stop the bleeding quickly : DCS
TRICKS
1. TACD bags beetwen viscera & abdominal wall