Management of COPD VISN 4 Primary Care Webinar
Charles W. Atwood, Jr., MD, FCCP
Pulmonary Physician – VA Pittsburgh Healthcare System
Assoc. Professor, University of Pittsburgh

Disclosures
Research grants: Vapotherm, Forest Research Institute, Medimmune
Consultant: Vapotherm

Objectives
1. Understand basic pathophysiologic concepts about COPD
2. Understand how COPD is diagnosed
3. Understand the role of commonly used medications for COPD
4. Be aware of new therapies which may affect how we manage COPD in the future

COPD - Definitions
• Chronic Bronchitis
– Chronic cough x 3mos
– Productive of sputum
– 2 successive years
• Blue bloaters
• Emphysema
– Presence of enlargement of and loss of integrity of the walls of lung alveoli
• Pink puffers

COPD
• Less than fully reversible airflow obstruction
• Related to cigarette smoking almost always
• Biomass burning
• Rarely, industrial chemical exposure
• ~ 15 million patients in US

COPD and other related conditions
• Asthma - classic asthma
• Asthma – non-classic asthma, adult onset
• Asthmatic bronchitis
• Bronchiectasis
• Constrictive bronchiolitis
• Asymptomatic airflow obstruction and emphysema

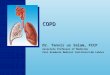
Asthma, Chronic Bronchitis and Emphysema

Pathophysiology of COPD

COPD Pathophysiology

Diagnosis of COPD
• Clinical symptoms
– Shortness of breath
• Quantify dyspnea
– Cough
• Productive vs. non-productive
– Risk factor assessment
• Smoking exposure
• 10 Pk yr is minimal amount consistent with COPD
• Other exposures

Diagnosis of COPD
• Other factors to consider
– Childhood lung disease, esp asthma
– Family history
– Prior exacerbations if COPD is previously diagnosed
– Comorbid conditions
• CAD and CHF
• Depression / Anxiety
• OSA

Diagnosis of COPD
• Physical exam
– SPO2
– Chest exam
• Barrel chest; pursed lip breathing; cyanosis
• Cyanosis
• Plethoric face
– Chest auscultation
• Hyper – resonance
• Decreased airflow with forced exhalation

Diagnosis of COPD
• Physical exam
– Cardiac exam
• Split 2nd heart sound cor pulmonale
– Extremity exam
• Lower ext edema; venous stasis;

Pulmonary Function Testing

Pulmonary Function Testing
• Spirometry
• Reversibility testing
– Focus on FEV1 and FVC
– Minimum of 200ml increase absolute value
– AND minimum of 12% increase
– FEV1/FVC < 0.70 indicates airflow obstruction
• Optional testing – Diffusing Capacity, lung volumes

Time Course of COPD

Severity of COPD
American Thoracic Society Criteria
• Based on % reduction of FEV1
– Mild >70%
– Moderate 60-69%
– Mod Severe 50-59%
– Severe 35-49%
– Very Severe <35%

GOLD Criteria for COPD

Changing Prevalence of COPD

Dyspnea Assessment Modified Medical Research Council Scale

Treatment of COPD
Goals 1. Prevent further damage to lungs
2. Decrease symptoms, esp. dyspnea
3. Maintain or even improve daily functioning
4. Prevent worsening as much as possible

Therapy Topics
• Smoking cessation
• Influenza vaccine
• Beta agonists
• LABAs
• Inhaled Steroids
• Anticholinergics
• Treatment of exacerbations

Smoking Cessation
• 5 A’s
• Ask – ask about smoking every visit
• Advise – advise quitting every visit
• Assess – assess willingness to quit every visit
• Assist – give practical help; medications, etc
• Arrange – smoking cessation classes; office follow-up

Smoking Cessation
• 5 Rs
• Relevance – why is quitting necessary
• Risks – help identify with pt neg consequences
• Rewards – identify benefits of quitting
• Roadblocks- identify barriers
• Repetition – repeat the process as needed

Vaccinate
• Annual vaccination for influenza –
– good evidence that it lowers morbidity and mortality in high risk patients
• Pneumococcal vaccine –
– Follow the CDC guidelines
– Vaccinate at age 65 only once
– If vaccinated before 65, repeat once after 5 years

Step-up Care for COPD Therapy

Step-Care Pharmacotherapy in COPD


Case Examples

Mr. Jones
• 64 yo male
• 40 pack year smoking
• Farmer
• Has dyspnea with exertion, cough in morning with sputum production
• Exam: normal lung and heart exam
• What should be done for this evaluation?

Mr. Jones, Continued
MANDATORY
1. Smoking cessation
2. PFT’s – determine physiology and effect of the smoking exposure
3. Determine vaccine status
CONSIDER
1. Xray of Chest
2. Start bronchodilator
3. Referral to a pulmonologist

Mr. Smith
• 74 yo
• Heavy smoker: 70 PY
• Dyspnea on exertion with mild exertion
• Cough and sputum in the mornings
• 2 admissions for COPD exacerbations in past 18 months
• PFT’s - - > show severe obstruction
• What would you do next?

Mr. Smith
• O2 evaluation
• Medication review
– SABA
– ICS + LABA + LAAC – worse case scenario
• Vaccination review
• Consider pulmonary rehabilitation

Conclusions
• COPD is very common
• It is treatable
• Goals should be to – prevent more lung damage by eliminating tobacco
use,
– trying to prevent exacerbations,
– appropriate vaccines
• Consult pulmonary when you need to
• E-consults work well in these cases
Recommended