

• Improve decision making to achieve better outcomes based on the available evidence
• Take into account newer technical and medical advances against the backdrop of rising costs
• Decrease the variability in vascular surgical care within Europe
• Create a current “state-of-the-art” inventory of the knowledge in AAA treatment
• However, there have been new evidences since the publication of these guidelines
Purpose of the guidelines

1a Systematic review of randomised controlled trials (RCT)1b individual RCT2a Systematic review of cohort studies2b individual cohort study3a Systematic review of case-control studies3b individual case-control study4 Case-series and casecontrol studies5 Expert opinion
A Consistent level 1 studiesB Consistent level 2 or 3 studies or extrapolations level 1studiesC Level 4 studies or extrapolations from level 2 or 3 studiesD Level 5 evidence or inconsistent/inconclusive studies any level
Levels of Evidence
Levels of Recommendation

Chapters
1. Epidemiology
2. Screening
3. Decision-making for elective AAA repair
4. Pre- and postoperative imaging
5. Management of non-ruptured AAA
6. Management of ruptured AAA
7. Follow-up after AAA repair
130 recommendations (17 level 1 & 60 level 2)(20 grade A & 59 grade B)

Risk factors
Important risk factors for AAA are advanced age and male gender, a positive family history for AAAs, especially in first-degree relatives. Smoking is a strong risk factor, the associated risk being much higher than for either coronary artery disease or stroke.
EJVES 2011;41:suppl1 – Chapter 1 - Epidemiology
Fleming C - Ann Int Med 2005;142:203Golledge J – Art Thromb Vasc Biol 2006;26:2605 (mod)
Level 2a, Recommendation B
Age
Family history
Smoking
CHD
Hypercholesterol
Hypertension
Female gender
Black race
Diabetes

Population screening of older men for AAA, in regions where the population prevalence is ≥ 4%, reduces aneurysm-related mortality by almost half within 4 years.
Men should be screened with a single scan at 65 years old.
Screening for AAA in men
EJVES 2011;41:suppl1 – Chapter 2 - Screening
Level 1a, Recommendation A
MASS study – Lancet 2002;360:1531 Viborg county – BMJ 2005;330:750

Population screening of older women for AAA does not reduce the incidence of aneurysm rupture.
Opportunistic screening of patients with peripheral arterial disease should be considered.
Screening for AAA in women
EJVES 2011;41:suppl1 – Chapter 2 - Screening
Level 1b, Recommendation B
Level 2a, Recommendation B
Scott RAP – BJS 2002;89:283

Threshold for aneurysm repair
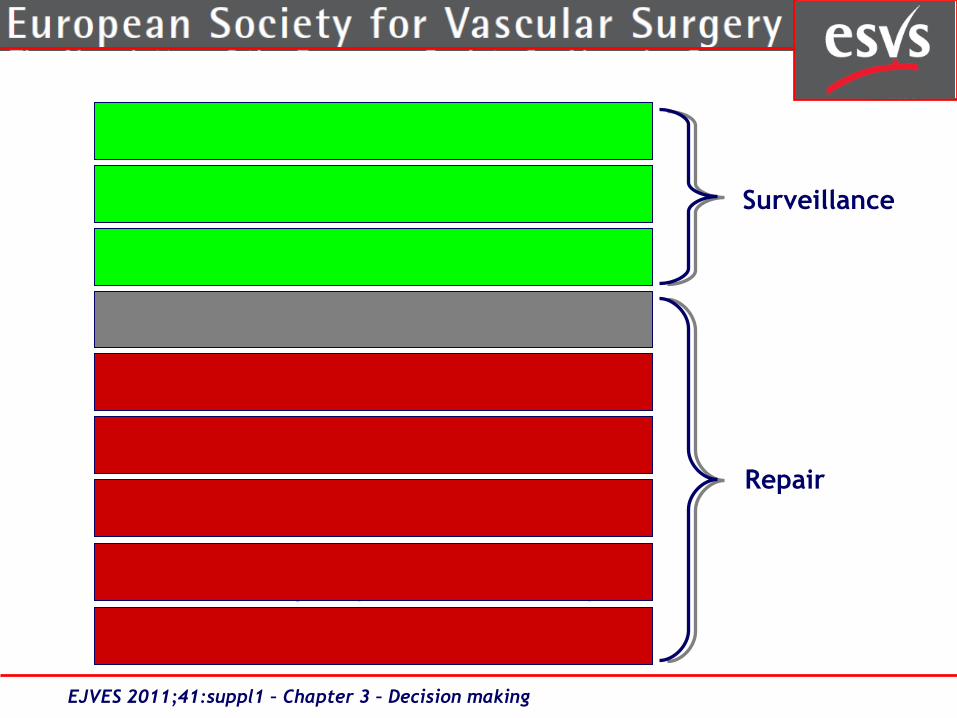
A policy of ultrasonographic surveillance of small aneurysms (4.0-5.5cm) is safe and advised for asymptomatic aneurysms.
UKSAT - BJS 2007;94:702 CAESAR - EJVES 2011;41:13
Level 1a, Recommendation A
EJVES 2011;41:suppl1 – Chapter 3 – Decision making
3 cm
4 cm
5 cm
5.2 cm
5.5 cm
6 cm
7 cm
8 cm
9 cm
Management of co-morbiditiesAAA surveillance programmeManagement of co-morbiditiesAAA surveillance programme
AAA surveillance programmeReferral to surgeon for optimisation
consider repair in FEMALES ONLYReferral to vascular surgeon
assess fitness & morphologyReferral to vascular surgeon
consider urgent open repairif requiring custom made endograft
In-patient managementconsider immediate repair
Surveillance
Repair
EJVES 2011;41:suppl1 – Chapter 3 – Decision making

Pharmacotherapy for AAA patients
Statins started one month before intervention reduce cardiovascular morbidity; they should be continued in the perioperative period, for an indefinite duration.
Only use beta-blockade in the patients of highest cardiac risk and if beta-blockade can be started one month before intervention.
Patients with vascular disease should be started on low-dose aspirin therapy, unless specific contra-indications exist and this should be continued through the peri-operative period.
Level 1a, Recommendation A
Level 1b, Recommendation A
Level 1a, Recommendation A
EJVES 2011;41:suppl1 – Chapter 3 – Decision making

Pre-operative cardiac evaluation
All patients undergoing AAA repair should have a formal assessment of their cardiac risk.
Patients undergoing EVAR, in the presence of cardiac risk factors, or a positive cardiac history should have a trans-thoracic echocardiogram and consideration of a pharmacological stress test or myocardial perfusion scan prior to AAA repair.
Coronary revascularisation should be considered prior to AAA repair for patients who have ischaemic coronary symptomatic or left main coronary artery disease.
EJVES 2011;41:suppl1 – Chapter 3 – Decision making
Level 1c, Recommendation A
Level 2c, Recommendation B
Level 1b, Recommendation B
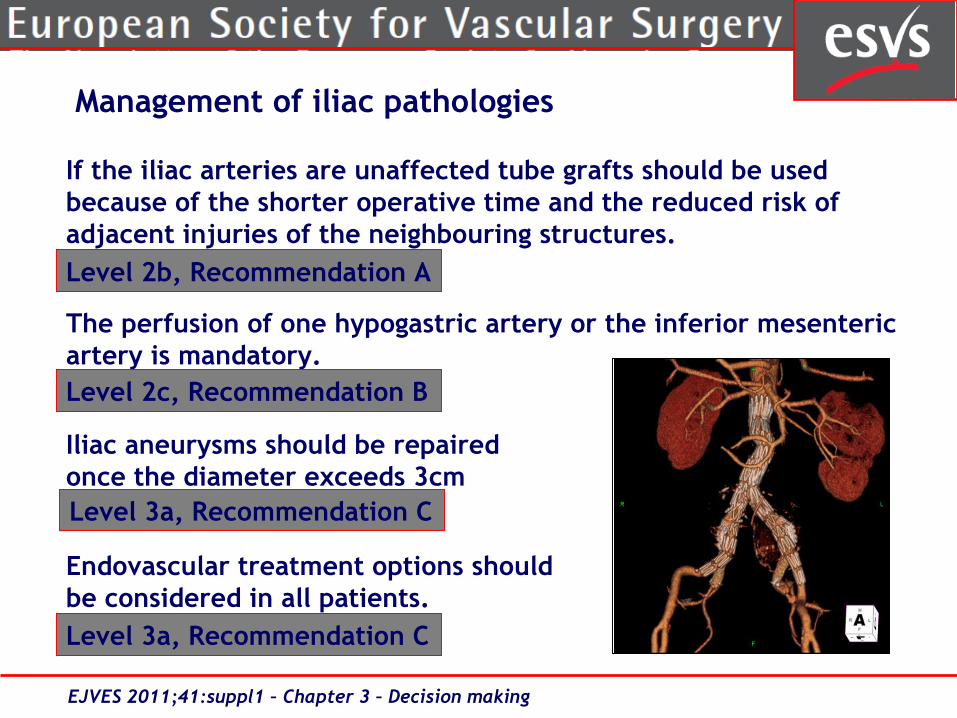
Management of iliac pathologies
If the iliac arteries are unaffected tube grafts should be used because of the shorter operative time and the reduced risk of adjacent injuries of the neighbouring structures.
The perfusion of one hypogastric artery or the inferior mesenteric artery is mandatory.
Iliac aneurysms should be repairedonce the diameter exceeds 3cm
Endovascular treatment options shouldbe considered in all patients.
EJVES 2011;41:suppl1 – Chapter 3 – Decision making
Level 3a, Recommendation C
Level 2b, Recommendation A
Level 2c, Recommendation B
Level 3a, Recommendation C

Patient‘s preference
The patient’s preference for type of aneurysm repair should be considered.
Where morphologically suitable, patients should be offered EVAR, which has a lower operative Mortality for symptomatic casesthan open repair.
EJVES 2011;41:suppl1 – Chapter 3 – Decision making
Level 2a, Recommendation B
Level 2c, Recommendation B
Technical considerations
Fast track surgery can positively influence perioperative outcome after abdominal aortic aneurysm repair. If patients and nursing staff are willing to follow the suggested requirements, it should be implemented in daily routine.
In the absence of convincing evidence favouring any one type of incision, the incision for open repair should be tailored to the patient needs and local expertise.
Level 2b, Recommendation B
Level 2b, Recommendation C
EJVES 2011;41:suppl1 – Chapter 5 – Non-ruptured AAA
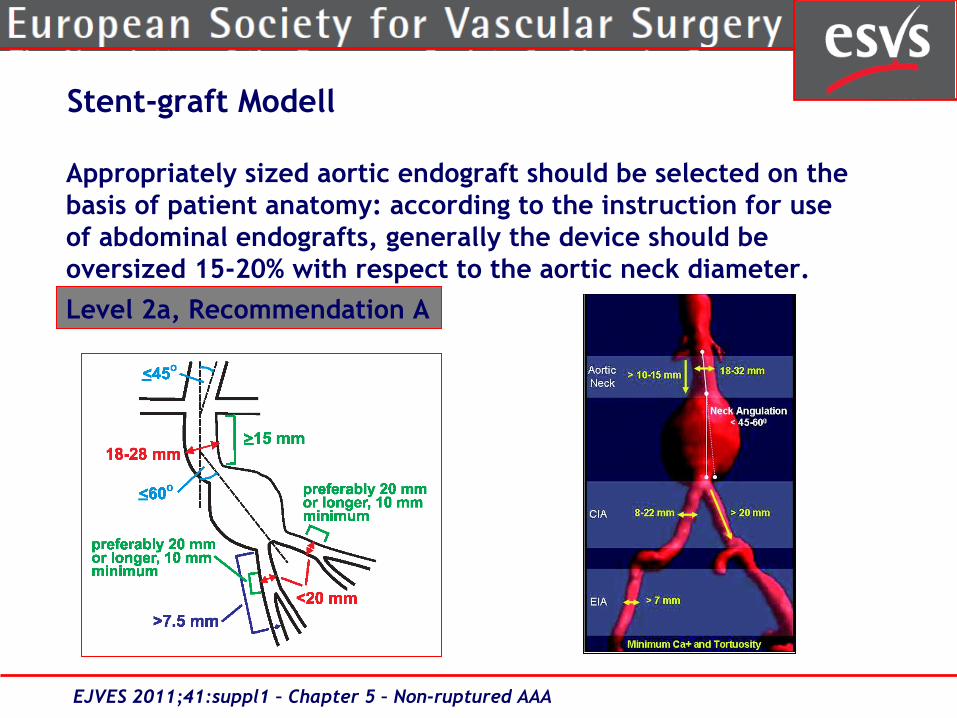
Stent-graft Modell
Appropriately sized aortic endograft should be selected on the basis of patient anatomy: according to the instruction for use of abdominal endografts, generally the device should be oversized 15-20% with respect to the aortic neck diameter.
Level 2a, Recommendation A
EJVES 2011;41:suppl1 – Chapter 5 – Non-ruptured AAA

Consideration for repair
Assessment of fitness Assessment of morphology
Fit for repair
optimisation Standard
AAA repair OPEN or EVAR
Transabdominal
Unfit for repair
optimisation
FitUnfit for
OPEN or EVAR
Manage conservatively
Suitable for EVAR
Not suitable for EVAR
Custom Open Laparoscopic
Retroperitoneal
Patient preference
Center preference
> 8cm
urgent
EJVES 2011;41:suppl1 – Chapter 5 – Non-ruptured AAA
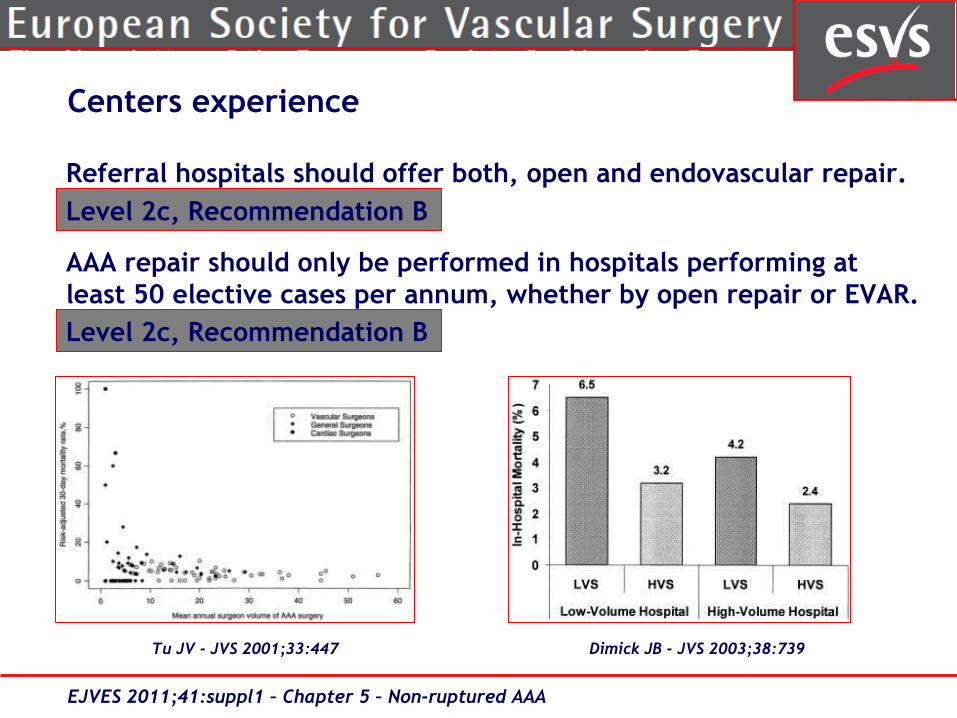
Referral hospitals should offer both, open and endovascular repair.
AAA repair should only be performed in hospitals performing at least 50 elective cases per annum, whether by open repair or EVAR.
Centers experience
Level 2c, Recommendation B
Level 2c, Recommendation B
EJVES 2011;41:suppl1 – Chapter 5 – Non-ruptured AAA
Tu JV - JVS 2001;33:447 Dimick JB - JVS 2003;38:739
Management of ruptured AAA
Immediate repair is recommended in patients with documented aneurysm rupture.
In symptomatic but unruptured AAA an optimization of the patient and delayed repair within 24 hours might be discussed.
EVAR should be considered as a treatment option for ruptured AAA, provided that anatomy of the aneurysm is suitable, and the centre is equipped and experienced in endovascular aneurysm procedures.
EJVES 2011;41:suppl1 – Chapter 6 – Ruptured AAA
Level 1a, Recommendation A
Level 3b, Recommendation C
Level 2b, Recommendation B

Preoperative fluid administration should be restricted to a minimum to maintain hypotensive hemostasis.
Measurement of the intraabdominal pressureis recommended in these patients. If theabdominal pressure is>20mmHg in combinationwith organ dysfunction, decompressive surgeryshould immediately be performed with theuse of temporary abdominal closure systems.
EJVES 2011;41:suppl1 – Chapter 6 – Ruptured AAA
Management of ruptured AAA
Level 2b, Recommendation A
Level 2c, Recommendation A
Follow-up
All patients treated for an AAA should receive the best medical treatment including aspirin, statins, and beta-blockers, with annual cardiac evaluation.
Follow-up of patients after AAA repair should include, in addition to clinical examination, a color duplex ultrasound with ABI on a regular basis.
Any gastrointestinal bleeding in a patient having an aortic graft should prompt the evaluation of a prosthetic-enteric fistula.
Level 2a, Recommendation B
Level 2a, Recommendation B
Level 1c, Recommendation B
EJVES 2011;41:suppl1 – Chapter 7 – Follow-up
EVAR - Follow-up
All patients should have a CTA and plain radiographs with anteroposterior and lateral projections at 30 days.
If there is any endoleak or less than one stent component, CTA at 6 mo. and 12 mo. with plain radiographs should be done.
At 12 months, if there is no endoleak and a stable or shrinking AAA, a yearly DU is recommended with plain radiographs.
Level 2c, Recommendation A
Level 2b, Recommendation B
Level 2b, Recommendation B
EJVES 2011;41:suppl1 – Chapter 7 – Follow-up

Endoleak after EVAR
All Type I endoleaks should be treated.
Treatment is recommended for Type III endoleaks.
Treatment is not recommended forType IV endoleaks.
An enlarging abdominal aortic aneurysmafter EVAR without evidence of anendoleak (≥10 mm) should be repaired.
Level 1b, Recommendation B
Level 1b, Recommendation B
Level 2b, Recommendation B
Level 2b, Recommendation B
EJVES 2011;41:suppl1 – Chapter 7 – Follow-up

Endoleak after EVAR
Type II endoleaks without increased sac diameter can be observed, computed tomographic scans with delayed arterial phase are the best detection method.
Endovascular or laparoscopic treatment is recommended for type II endoleaks with increased sac diameter ≥ 10 mm/year, with conversion to open surgery in case of failure.
Any increasing aneurysm diameter or new endoleak, after prior imaging studies have shown complete aneurysm sac exclusion, should prompt complete imaging with CTA and plain radiographs.
Level 2b, Recommendation B
Level 2b, Recommendation B
Level 2b, Recommendation B
EJVES 2011;41:suppl1 – Chapter 7 – Follow-up

Critical issues
• There is a need to develop postoperative surveillance protocols, including optimal use of DU, contrast enhanced DU, and CT imaging at various time periods after EVAR.
• New techniques concerning visualization of endoleak, including magnetic resonance imaging with a blood pool contrast agent, should be developed.
EJVES 2011;41:suppl1 – Chapter 7 – Follow-up
Chaer RA – JVS 2009;49:845Van der Laan – EJVES 2006;32:361

ESVS Clinical Practice Guidelines
Invasive treatment for carotid stenosis 2009
Management of abdominal aortic aneurysms 2010
Critical leg ischemia 2011
Management of descending thoracic aortic diseases 2012
Venous diseases 2013
Access surgery 2013
An annual (electronic) update of the earlier guidelines is planned
Recommended











![arranged by tom wallace percussion by tony mccutchen 11 a a 10 aaa > e] aa aaa 6 aaa aaa aaa aaa aaa aaa 13 > 19 — 18 15 a a aa 16 a a 12 20 23 a > 24 aaa > 25 a > 26 aaa > 27 gÆ4k](https://img.pdfslide.us/doc/110x75/5e6c4dfc8bd84b079d5a5076/arranged-by-tom-wallace-percussion-by-tony-mccutchen-11-a-a-10-aaa-e-aa-aaa.jpg)





