Achilles Ruptures
Selene G. Parekh, MD, MBAAssociate Professor of Surgery
Partner, North Carolina Orthopaedic Clinic
Department of Orthopaedic Surgery
Adjunct Faculty Fuqua Business School
Duke University
Durham, NC
919.471.9622
http://seleneparekhmd.com
Twitter: @seleneparekhmd
Controversies
• Treatment:
• Operative vs. non-operative
• If surgery:
• Open vs percutaneous
• Augmentation
• Post-op rehab
Who gets them?
• Men (5x) > Women (4-6:1) (80% vs 20%)
• Avg age: 42 yo (increased after age 25)
• About 0.01% of US population
• 11-18/100,000 people
• 68% occur during sports (at least)
Nyyssonen, Scan J Surg, 2008
Who gets them?
• Contributing factors:
• Age: >40yo
• Blood flow decreases
• Stiffness of tendon increases
• Prior rupture: 6-8%
• Steroid injections into tendon
• Medications: fluoroquinolones, statins
Vosseller, FAI, 2013
Kujala, Clin J Sports Med, 2005
Hess, Foot Ankle Spec, 2009
Who gets them?• Elite Athletes
• More likely to get Achilles tendinopathy instead of
a frank rupture
• Older athletes (27 yo vs 25 yo)
• Sprinters more than distance athletes
Gajhede-Knudsen, Br J Sports Med, 2013

Elite Athletes
• Parekh et al, 2009
• NFL players, 1997-2002
• 31 Achilles ruptures (~6/year) in 28 players
• Avg age: 29 years old (avg age of NFL player:
26yo)
• 35% in preseason, 65% in regular seasons
• None occurred in practice
• 36% of athletes never returned to play in NFL
Fluoroquinolone Use
• Exposure increases risk tendon injuries
• Achilles tendon more than others
• Increased risk:
• First month of use (even first 7 days)
• Combined with oral corticosteroids
• >60 yo
• Renal disease
• Type of fluoroquinolone
• Black Box warningStephenson, Drug Saf. 2013
Parmar, FAI, 2007
Corticosteroid Use
• No clear etiological role
• Injections:
• Animal studies:
• Necrosis at site of injection
• Delay in healing response
• Clinical studies: case reports
• 5 athletes after injection: residual corticosteroid steroid found at the site of injection
• Oral:
• Case reports suggest increased risk of rupture
Balasubramaniam, JBJS-Br, 1972
Unverferth, JBJS, 1973
Mechanism
• 53% at push off (eccentric contraction)
• Occurs during running or jumping
• Tears 2-6cm from insertion (80%)
Hess, Foot Ankle Spec, 2010
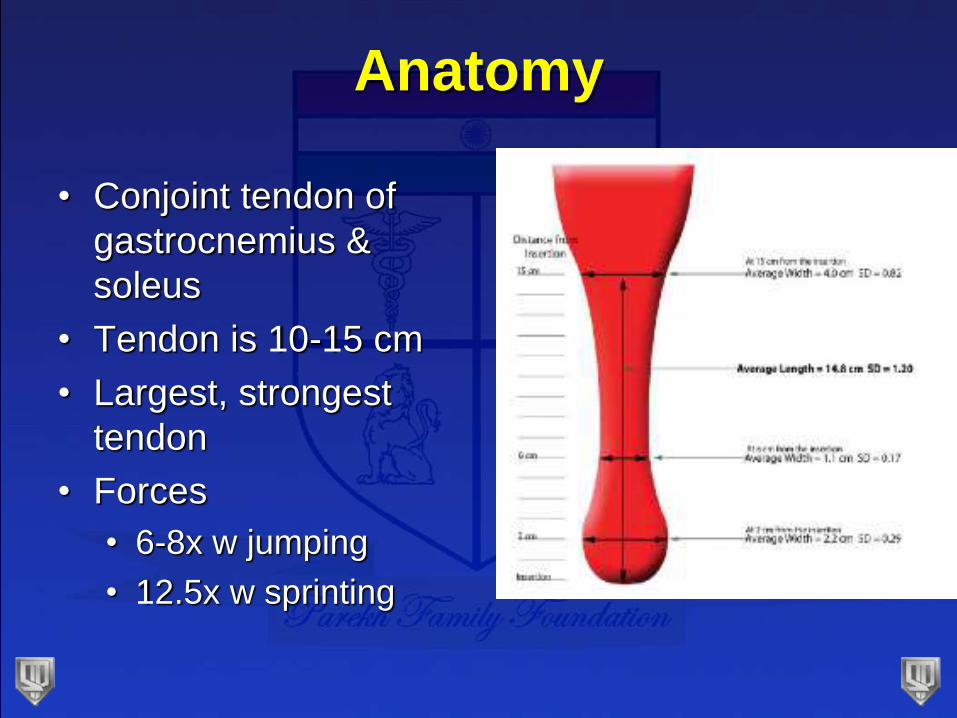
Anatomy
• Conjoint tendon of
gastrocnemius &
soleus
• Tendon is 10-15 cm
• Largest, strongest
tendon
• Forces
• 6-8x w jumping
• 12.5x w sprinting

Anatomy
• Contribution variable
• More from gastroc
• Fibers rotate 90o
• Gastroc contribution is lateral
• Maximum rotation of fibers is at 2-5cm proximal
to insertion
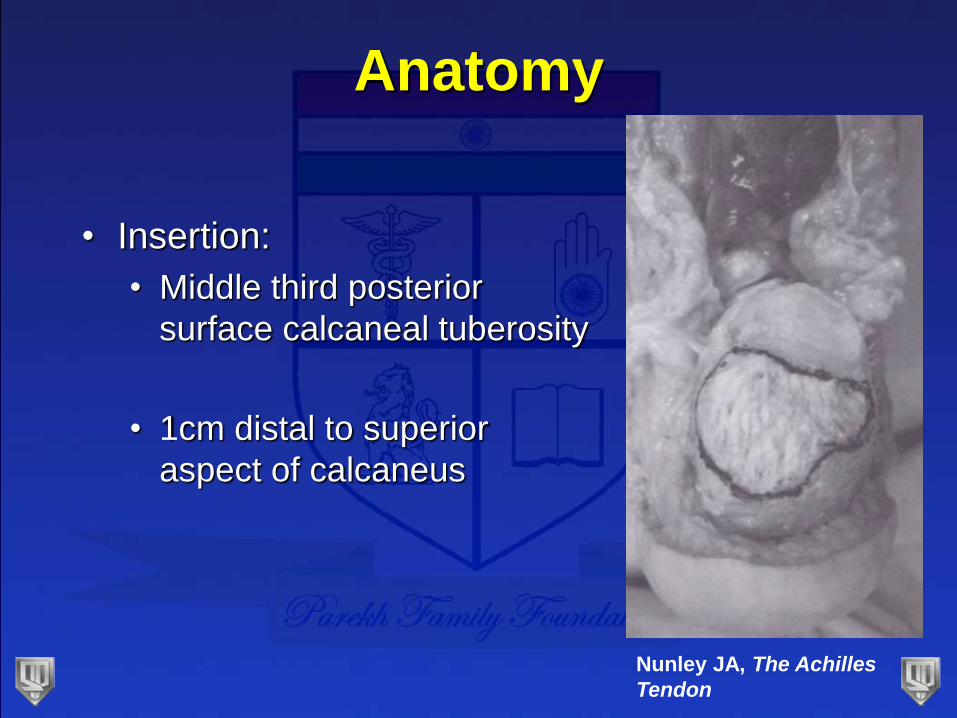
Anatomy
• Insertion:
• Middle third posterior
surface calcaneal tuberosity
• 1cm distal to superior
aspect of calcaneus
Nunley JA, The Achilles
Tendon
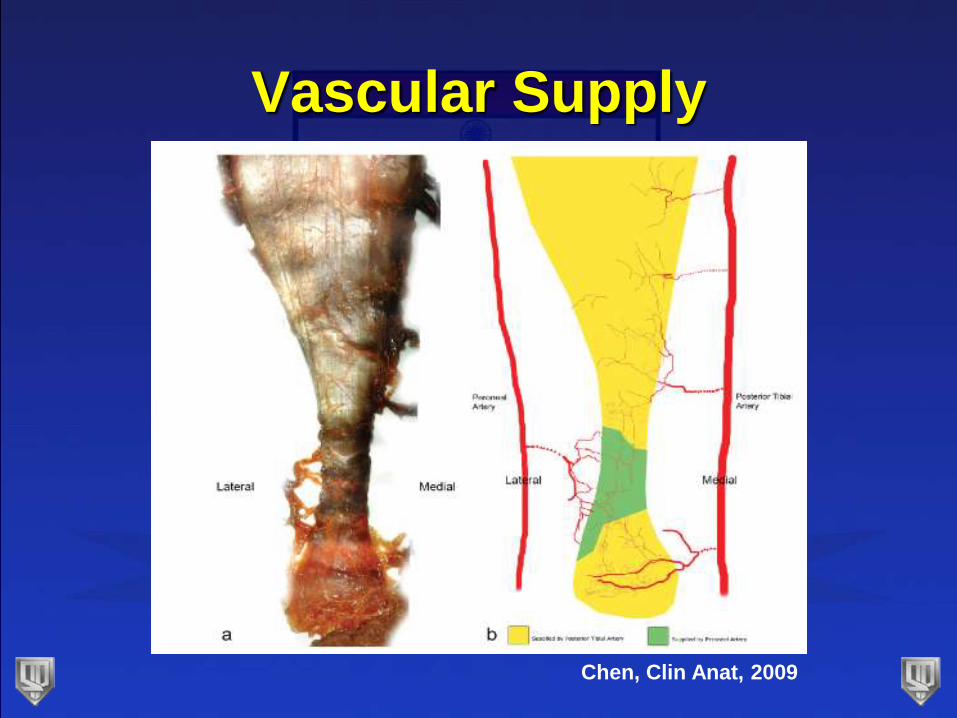
Vascular Supply
Chen, Clin Anat, 2009
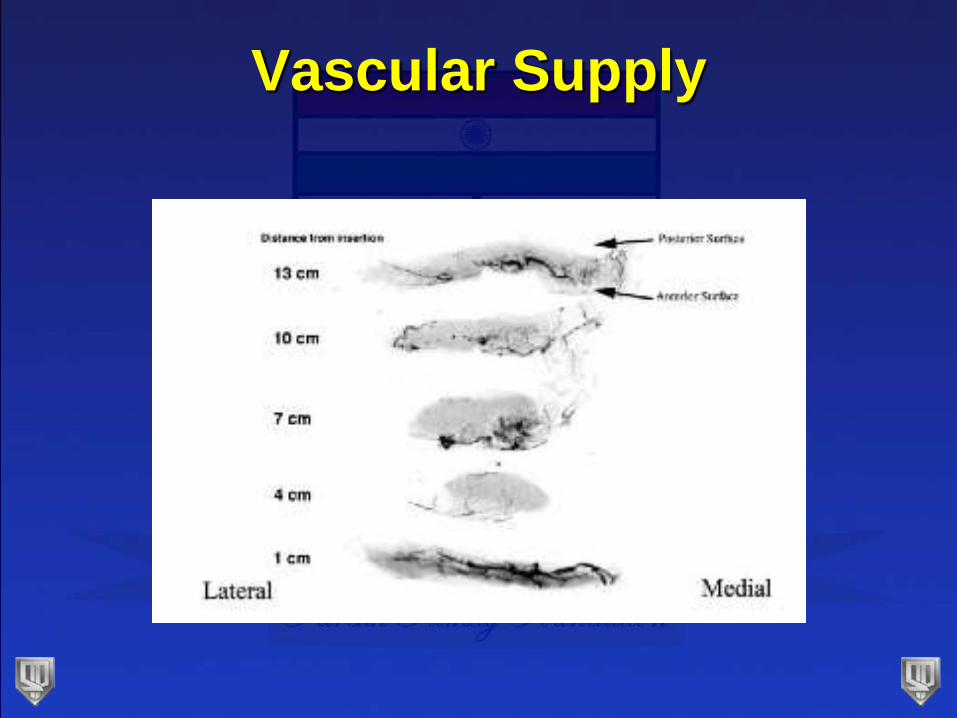
Vascular Supply
Vascular Supply
• Posterior longitudinal midline incision
• Least disruptive
• Close the paratenon and deep fascia
• Thought to help healing
• Skin perfusion
• Maximized at 20o plantar flexion
Poynton, FAI 2001
Presentation
• Sudden pain
• “kicked in the back of my calf”
• Audible snap
• Weakness in ankle
• Initial diagnosis missed as often as 25%
• Commonly diagnosed as ankle sprain
Kvist, Sports Med. 1994
Diagnosis
• “Should not pose a diagnostic problem”
• At least 2 positive physical exam tests
• Palpation: least sensitive
• Calf squeeze: most sensitive
• Maltes: knee flexion test (88% sensitive)
• Copeland: blood pressure cuff test
• O’Brien: needle test
Maffulli, Am J Sports Med. 1998
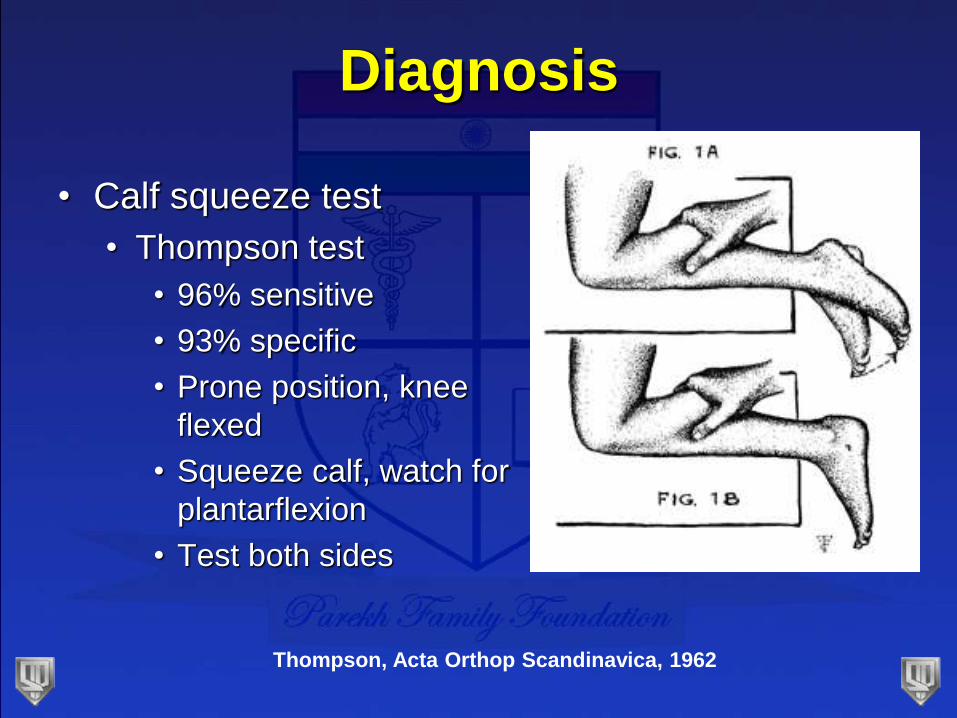
Diagnosis
• Calf squeeze test
• Thompson test
• 96% sensitive
• 93% specific
• Prone position, knee
flexed
• Squeeze calf, watch for
plantarflexion
• Test both sides
Thompson, Acta Orthop Scandinavica, 1962
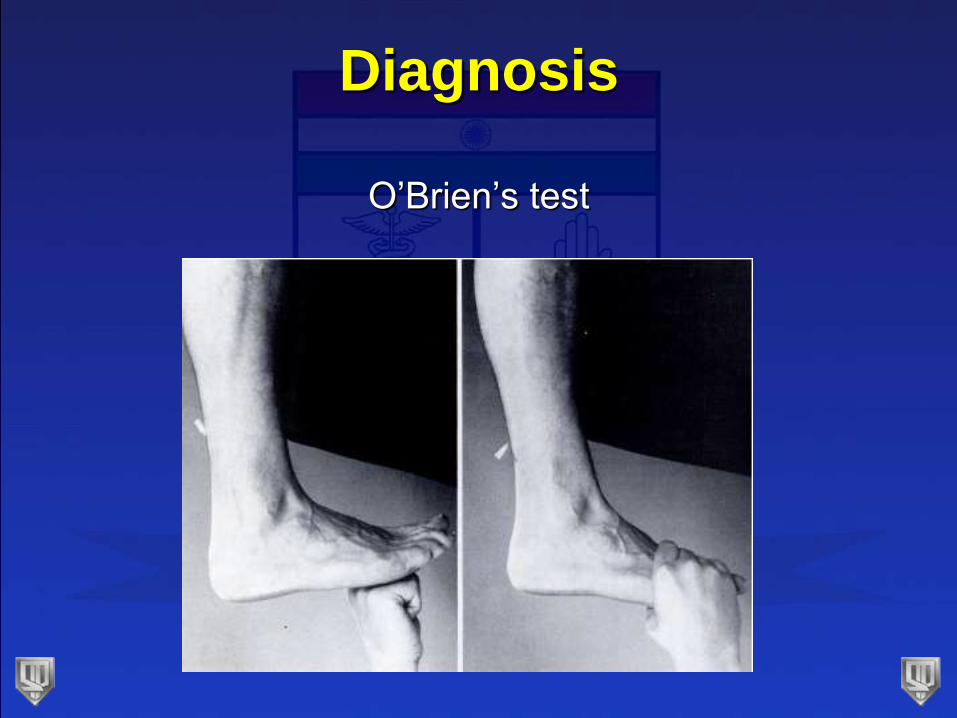
Diagnosis
O’Brien’s test
Imaging
• Should not rely on imaging
• Radiographs:
• Useful for distal avulsions
• Particularly with chronic insertional disease
• Loss of configuration of Kager’s triangle
• Toygar’s sign
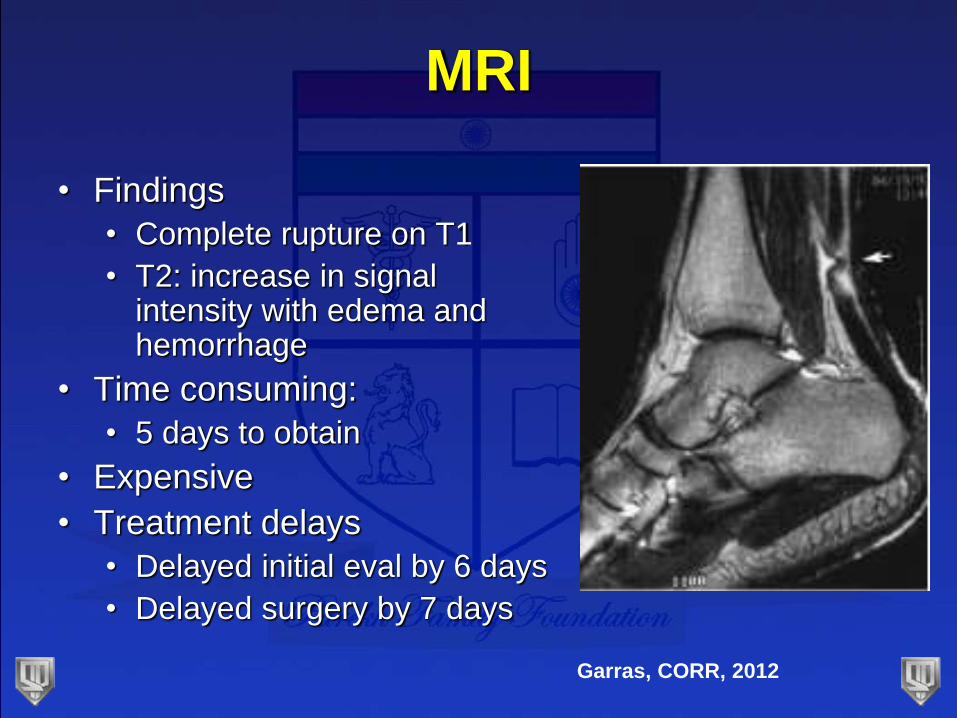
MRI
• Findings
• Complete rupture on T1
• T2: increase in signal intensity with edema and hemorrhage
• Time consuming:
• 5 days to obtain
• Expensive
• Treatment delays
• Delayed initial eval by 6 days
• Delayed surgery by 7 days
Garras, CORR, 2012

Ultrasound
• Performed in office
• Faster
• Cheaper
• Can examine healing or repair
• Best method to follow treatment
• Still not necessary
Maffulli, Internat J Sports Med, 1990
Treatment
• AAOS guidelines, published in 2009:
• Conflicting Evidence
• No definitive answer on operative vs
nonoperative treatment
• 16 recommendations:
• None graded as strong
• 2 consensus statements
• 2 moderate strength recommendations
AAOS Clinical Practice
Guidelines• Consensus:
• Detailed history & physical exam (2 physical exam
tests)
• Surgery is option
• Approach cautiously in pts >65, systemic issues,
obesity, or tobacco
• Moderate:
• Early protected weight bearing after surgical repair
• Protective device for mobilization b/t 2-4wk post-op

Operative vs Non-operative
Non-Operative Treatment
• Traditionally treated w immobilization
• 6-8wks cast
• High re-rupture rates
• Lee and smith, 1972: 13%
• Person and Wedmark, 1976: 32%
• Inglis, 1976: 39%
Non-Operative Treatment
• Functional rehab instead of cast immobilization
• Post-op: mobile cast is better than immobilization
Cetti, CORR 1994
• Meta-analysis of operative vs non-operative
• 12 trials w over 800 patients
• Less re-ruptures w surgery
• Higher complications with surgery (wound)
• Post-op:
• Functional brace with lower complication rate
than castingKhan, JBJS 2005
• Largest series of pts with non-op, functional rehab
• 2.8% re-rupture rate overall
• 2.7% re-rupture rate w delayed presentation (>2
wks)
Non-Operative Treatment
• Willits et al. JBJS 2010
• Prospective, randomized, multicenter trial
• 144 pts (72 operative, 72 non-op)
• All patients with accelerated rehab
• No difference in:
• Re-ruptures (2 in operative, 3 in nonoperative)
• Strength
• ROM
• Functional score (leppilahti score)
• Calf circumference
• Complications:
• 13 in operative group
• 6 in non-operative group

• No difference in:
• Re-rupture rate
• Strength and calf size
• Lower complications in non-operative group
• Faster return to work
• Concluded: consider non-op treatment if center
has functional rehab protocol
Comparison Study
• Gwynne-Jones, FAI, 2011
• Functional rehab in both operative and non-
operative
• Pts <40 yo with improved outcomes with surgery
• Lower re-rupture
• Low complications (1.4% wound complications)
• Non-operative is better in pts >40
• <40 yo: 13.1%
• >40 yo: 4.1%
• Recommend surgery for younger pts and athletes
Non-operative treatment
• Strong evidence for both non-operative and
operative treatment
• Must be functional rehab (if not, operate)
• Patients should be informed, ultimately their
decision
• Athletes may favor operative treatment
• Faster return to work and sport
• Questionable improved outcomes
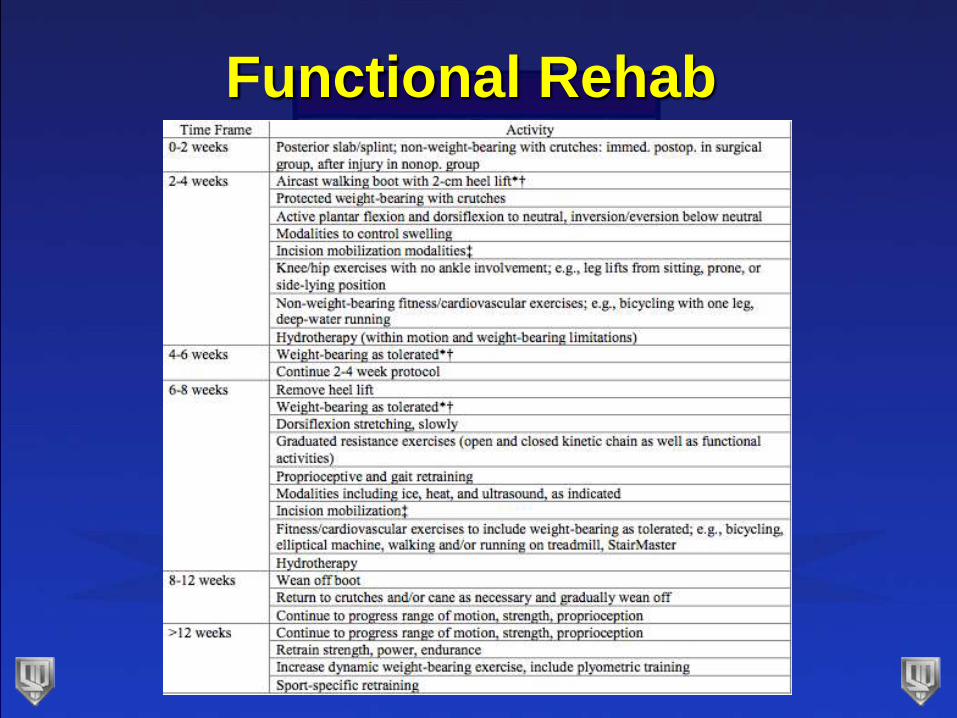
Functional Rehab
Who should have surgery
• Elite athletes
• Delayed presentation
• Inability for functional rehab
If surgery…
• More controversy
• How to repair
• Open vs percutaneous
• Post-op rehab
• Augment repair?
How to repair
• Watson, FAI, 1995
• Single Kessler
• Single Bunnel
• Double Krackow
• Double Krackow had double the strength
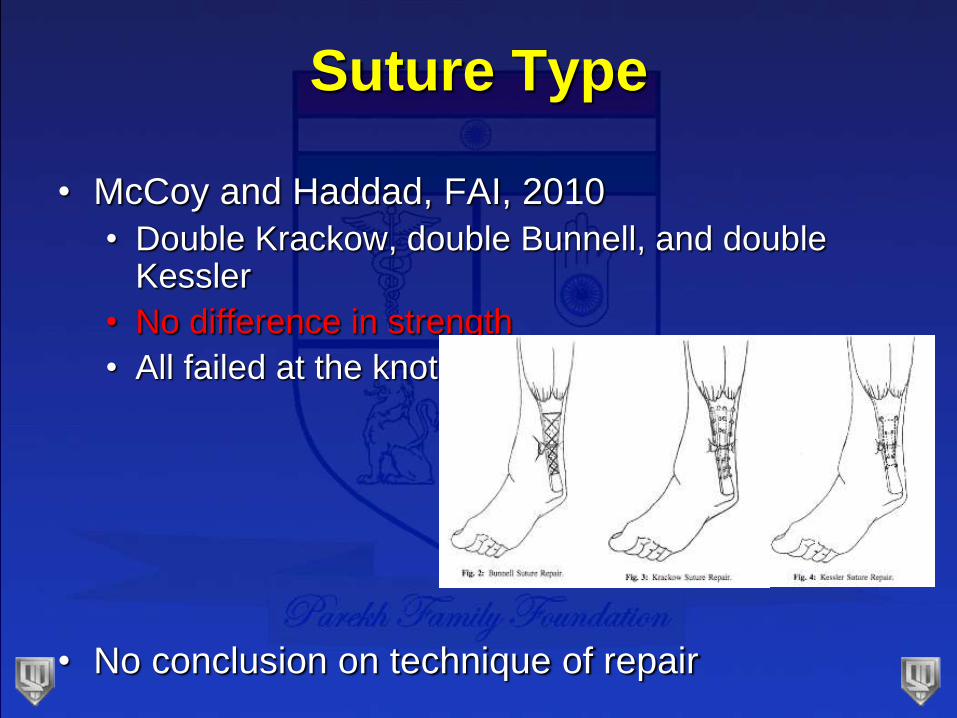
Suture Type
• McCoy and Haddad, FAI, 2010
• Double Krackow, double Bunnell, and double Kessler
• No difference in strength
• All failed at the knot
• No conclusion on technique of repair
Percutaneous Repair
• Minimizes trauma to tenuous skin
• Reduces surface area for adhesion formation
• Decreases possibility of contamination
• Minimal complications (11%)
• Skin dimple at operative site
• Tender nodule at operative site
Does Incision Size Matter?
• Cochrane review in 2010 (Khan et al)
• Percutaneous surgery vs open:
• Lower risk of infection
• Interpret with caution
• JBJS meta-anaylsis (Khan, 2005)
• Percutaneous with lower complication rate
Open vs Percutaneous
• Meta-analysis of randomized controlled trials
• No difference between groups:
• Re-rupture
• Sural nerve injury
• Deep infection
• Minimally invasive:
• Less superficial wound infection
• 3 times greater patient satisfaction
Foot Ankle Surg, 2011
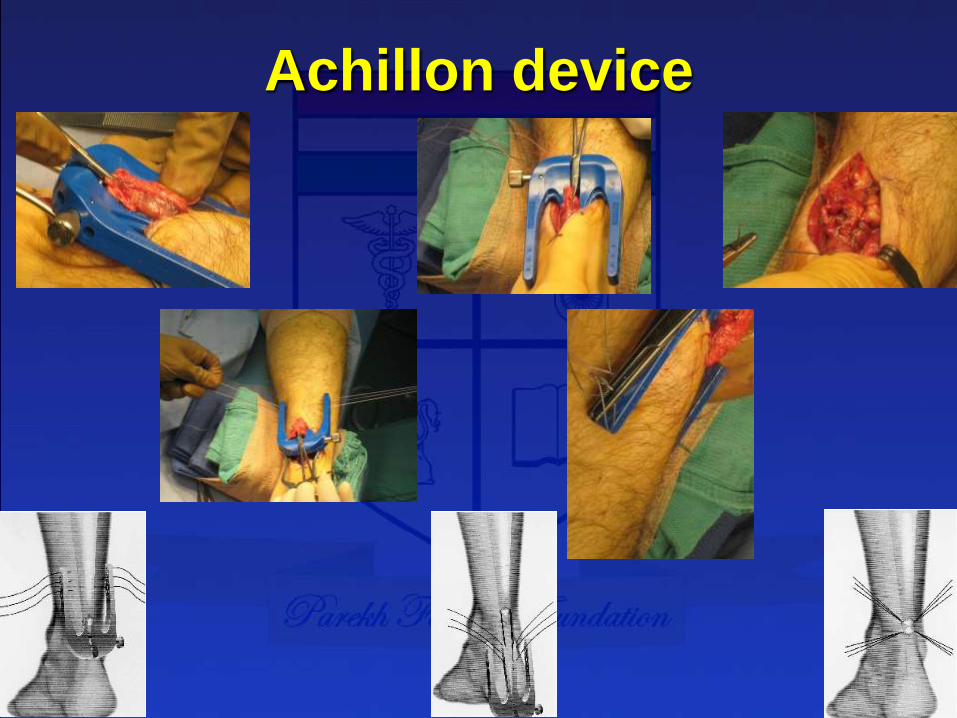
Achillon device
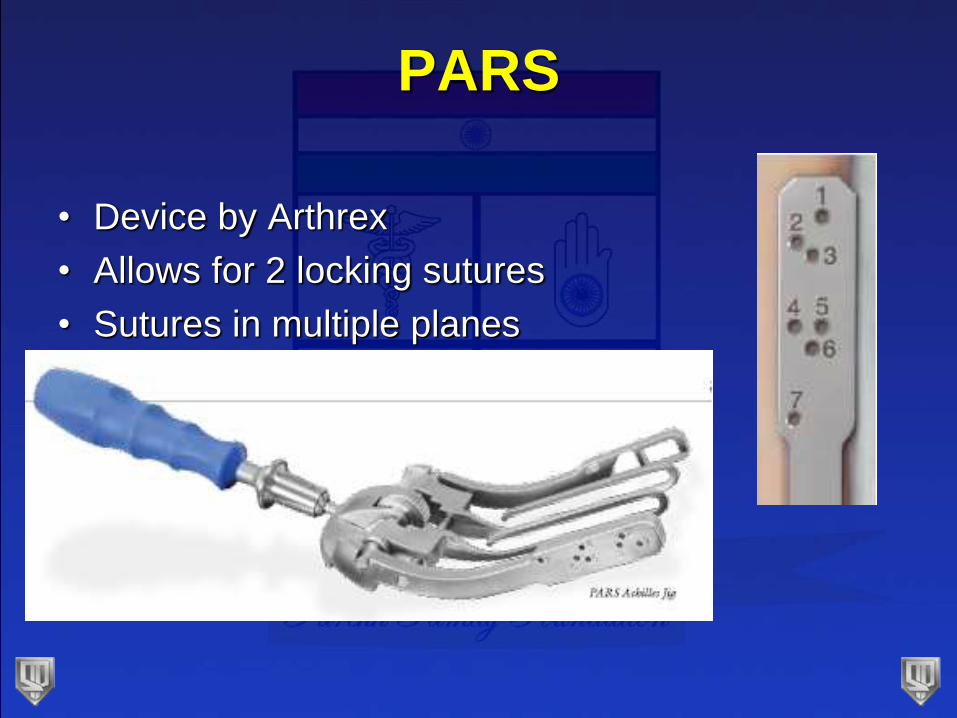
PARS
• Device by Arthrex
• Allows for 2 locking sutures
• Sutures in multiple planes
PARS
• Charlotte experience
• AOFAS 2012
• 46 pts
• AOFAS: 97
• 45/46 satisfied at 6 months
• No re-ruptures
• No sural nerve complications
• No wound healing issues
• Paid consultants
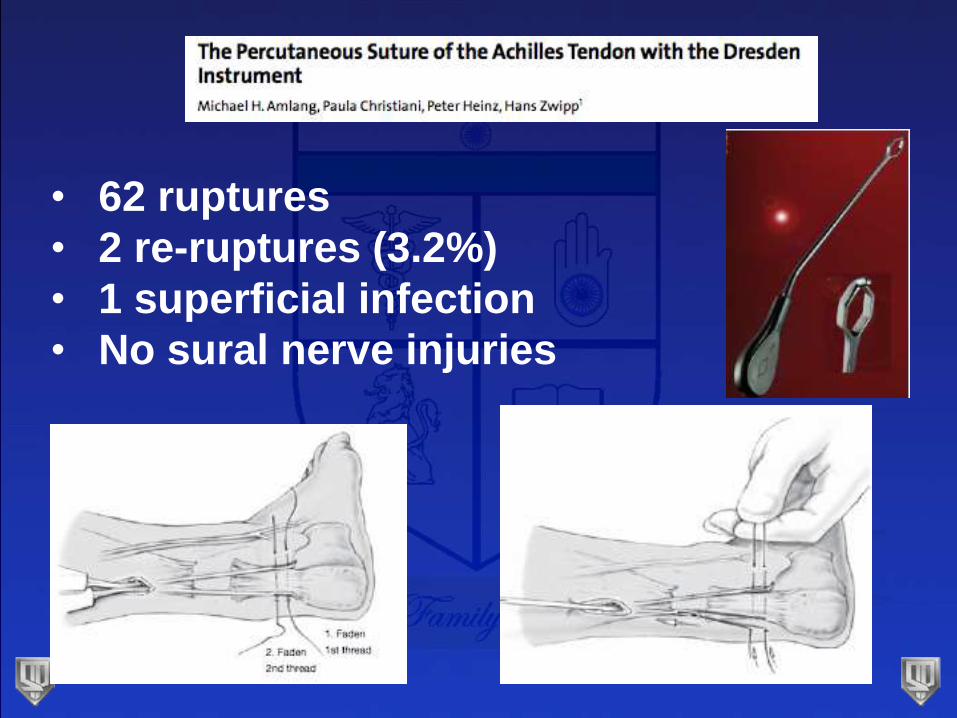
• 62 ruptures
• 2 re-ruptures (3.2%)
• 1 superficial infection
• No sural nerve injuries
Problems with Percutaneous
Repair?
• Aracil, FAI, 1992
• Sural nerve injury
• Taken back to OR for suture to be cut
• Re-rupture
• 33% re-rupture rate
• Didn’t limit dorsiflexion
• Hockenbury, Foot Ankle, 1990
• 60% sural nerve injury
• All within 2.5 cm from rupture site
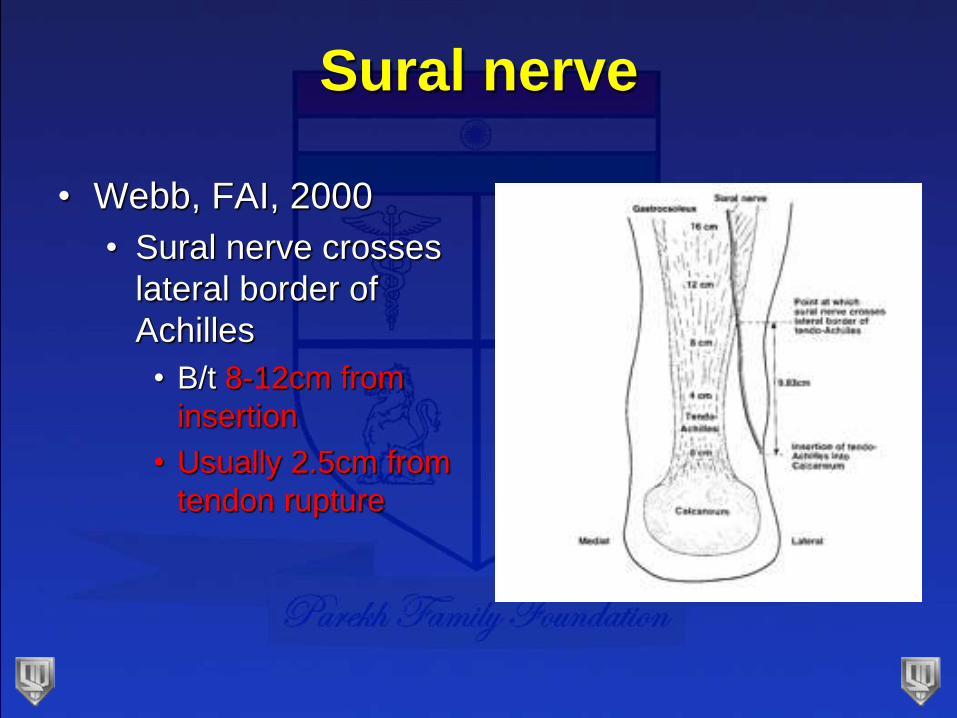
Sural nerve
• Webb, FAI, 2000
• Sural nerve crosses
lateral border of
Achilles
• B/t 8-12cm from
insertion
• Usually 2.5cm from
tendon rupture
Avoid Sural Nerve
• Don’t place percutaneous sutures in lateral half
of proximal tendon
• Make small proximal incision to find the nerve
(Webb, JBJS-Br, 1999, Klein, 1991)
• Place suture in medial half of proximal tendon
Post-op Rehab
• Maffulli, AJSM, 2003
• Prospective randomized study
• Early weight-bearing and ROM after open repair
• Fewer outpatient visits
• Discarded crutches early
• Higher satisfaction
• No difference in:
• Ultrasound appearance of tendon
• Isometric strength
Conclusions
• Increasing evidence for non-operative treatment
• Must be functional rehab
• Elite athletes still favor operative repair
• Safe, low re-rupture
• Best functional outcome (fastest)
• Pressure (athlete, coach, media)
• Maffulli, FAI, 2011
• Mini-open is a good option
• Risk of sural nerve injury
• Do what works in your hands
RE
ECTthe ankle
the foot
Recommended