DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019DERMIRA |
October 17, 2019
Lebrikizumab Program Update
LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019

DERMIRA | LEBRIKIZUMAB PROGRAM OVERVIEW 2
This presentation contains "forward-looking" statements that are based on our management’s beliefs and assumptions and on information currently available to management. Forward-
looking statements include all statements other than statements of historical fact contained in this presentation, including information concerning our vision for lebrikizumab, business
strategy, objectives, opportunities and plans; timing expectations for the Phase 3 lebrikizumab clinical trial; the targeted profile, attributes and performance for lebrikizumab; and
lebrikizumab’s potential to be a best-in-disease therapy for the treatment of atopic dermatitis. Forward-looking statements are subject to known and unknown risks, uncertainties,
assumptions and other factors that may cause our actual results, performance or achievements to differ materially and adversely from those anticipated or implied by our forward-looking
statements, including, but not limited to, those related to our dependence on third-party clinical research organizations, manufacturers, suppliers and distributors; the outcomes of future
meetings with regulatory agencies; our ability to obtain necessary additional capital; market acceptance of our product; the impact of competitive products and therapies; our ability to
attract and retain key employees; the costs of our commercialization plans and development programs; the design, implementation and outcomes of our clinical trials; our ability to
manage the growth and complexity of our organization; our ability to maintain, protect and enhance our intellectual property; and our ability to continue to stay in compliance with our
material contractual obligations, applicable laws and regulations. You should refer to the section entitled “Risk Factors” set forth in our Annual Report on Form 10-K, Quarterly Reports
on Form 10-Q and other filings we make with the Securities and Exchange Commission (SEC) from time to time for a discussion of important factors that may cause our actual results to
differ materially from those expressed or implied by our forward-looking statements. You should not rely upon forward-looking statements as predictions of future events. Neither we nor
any other person assumes responsibility for the accuracy and completeness of the forward-looking statements. We undertake no obligation to update any forward-looking statements
after the date of this presentation except as may be required by law.
This presentation also contains estimates and other statistical data made by independent parties and by us relating to market size and growth and other data about our industry. These
data involve a number of assumptions and limitations, and you are cautioned not to give undue weight to such estimates. Projections, assumptions and estimates of the future
performance of the markets in which we operate are necessarily subject to a high degree of uncertainty and risk. The trademarks included herein are the property of the owners thereof
and are used for reference purposes only.
We use our website (www.dermira.com), LinkedIn page (www.linkedin.com/company/dermira-inc-), Instagram account and corporate Twitter account (@DermiraInc) as channels of
distribution of information about our company, product candidates, planned announcements, attendance at upcoming conferences and other matters. Such information may be deemed
material information and we may use these channels to comply with our disclosure obligations under Regulation FD. Therefore, investors should monitor our website, LinkedIn page,
Twitter account and Instagram page in addition to following our SEC filings, press releases, public conference calls and webcasts.
Forward-looking statements

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Dermira Vision for Lebrikizumab (Lebri)Potential to deliver best-in-disease therapy to atopic dermatitis (AD) patients and those who care for them
3
• Driven by the advent of new, systemic
therapies addressing unmet needs in
moderate-to-severe patients, major-
market sales of branded, systemic
therapies for AD are projected to exceed
$21B by 2027.1
• α-IL-4/13 biologics are establishing the
market and treatment paradigm.
• While other approaches have shown
promise, their full profiles and suitability
for broad adoption remain to be seen.
• Ultimately, the scale of the market and
patient needs will support a range of
products.
• The market is and will remain ripe for
improvements on initial systemics,
including in efficacy, tolerability and
convenience.
• Clinical data suggest lebri may deliver
these improvements together with the
safety of the α-IL-4/13 class.
AD is projected to become the largest
market in dermatology.
Lebri may present an opportunity
to address key market needs.
There will be a large market for safe,
effective and convenient α-IL-4/13
biologics.
1. Decision Resources (2018) Landscape & forecast: Atopic dermatitis/ Eczema.

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
AD Insights Following EADV 2019
4
What We Heard
• Excitement from the dermatology community about the focus on innovation being made in AD, given the high unmet need
• Continued enthusiasm for the IL-4/13 class as a new standard of care with broad efficacy and favorable safety
• Focus on opportunities for improvements in key areas including:
• Efficacy, particularly in itch, given the significant burden of this symptom on patients
• Tolerability, particularly in view of high rates of conjunctivitis observed with dupilumab
• Convenience, particularly less frequent dosing
What We Saw
• Consistent with what we expected based on previously reported data
• Most relevant new disclosures were for JAK inhibitors
• Despite efficacy, comparable to lebri, at high doses in certain cases, safety risks and tolerability challenges remain
• While JAK inhibitors may play a role in a market as large and diverse as AD is expected to become, utilization may be limited,
relative to that of IL-4/13 biologics

Phase 2b Study ResultsApril W. Armstrong, MD, MPHProfessor of Dermatology and Associate Dean of Clinical Research, University of Southern California Keck School of Medicine
Lebrikizumab Study Investigator

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019DERMIRA |
E. Guttman-Yassky,1 A. Blauvelt,2 L. Eichenfield,3 A. Paller,4 A. Armstrong,5 J. Drew,6 R. Gopalan,6 E. Simpson7
Lebrikizumab, a High Affinity IL-13 Inhibitor, Improves Clinical Manifestations in Moderate-to-
Severe Atopic Dermatitis: Primary Results From a Randomized, Double‐Blinded, Placebo-Controlled,
Dose-Ranging, Phase 2b Study
1Icahn School of Medicine at Mount Sinai, New York, NY, USA; 2Oregon Medical Research Center, Portland, OR, USA; 3Department of Dermatology and Pediatrics, University of California, San Diego, CA, USA, and Rady Children's Hospital, San Diego, CA, USA; 4Department of Dermatology, Northwestern University Feinberg School of Medicine, Chicago, IL,
USA; 5Department of Dermatology, Keck School of Medicine at University of Southern California, Los Angeles, CA, USA; 6Dermira, Inc., Menlo Park, CA, USA; 7Department of Dermatology, Oregon Health and Science University, Portland, OR, USA
LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
IL-13 is a Central Pathogenic Mediator in AD
7
1Brunner PM et al. J Allergy Clin Immunol. 2017;139:S65-76; 2Buzney CD et al. J Drugs Dermatol. 2016;15:165-71; 3Brandt EB et al. J Clin Cell Immunol. 2011;10:doi:10.4172/2155-9899.1000110; 4May RD et al. Cytokine. 2015;75:89-116; 5Purwar R et al. J Invest Dermatol. 2006;126:1043-
51; 6Sebire G et al. Cytokine. 1996;8:636–41; 7Oetjen LK et al. Cell. 2017;171:http://dx.doi.org/10.1016/j.cell.2017.08.006
AD, atopic dermatitis; IL, interleukin

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Lebrikizumab Mechanism of Action
8
Lebrikizumab is a novel, high-affinity monoclonal antibody targeting IL-13 that selectively prevents
formation of the IL-13Rα1/IL-4Rα heterodimer receptor signaling complex while leaving endogenous
regulation of IL-13 intact
P
“Decoy”
IL-4RαIL-13Rα1
TYK2
IL-13
IL-13Rα2
STAT 6
JAK1
Lebrikizumab

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Study Design
9
Screening (≤30 days)
LEB 125 mg Q4W, n=73
LEB 250 mg Q4W, n=80
LEB 250 mg Q2W, n=75500 mg LD
Wk 0 & 2
Placebo Q2W, n=52
Week 0 Week 16
Randomized, Double-Blind Treatmenta
500 mg
LD Wk 0
250 mg LD
Wk 0
Safety follow-
up to Week 32
Week 4 Week 8 Week 32Week 12
3:3:3:2
Randomization
N=280
Key inclusion criteria
• Adults with moderate-to-severe AD inadequately
controlled with topicals or for whom topical treatment is
medically inadvisable
− Chronic ADb for ≥ 1 y
− EASI ≥16
− IGA score ≥3 (5-point scale [0-4])
− ≥10% BSA involvement
Key endpoints
• Primary: % change in EASI from Baseline at Wk 16
• Secondary:
− Skin lesions: IGA 0/1, EASI50/75/90
− Pruritus: Pruritus NRS change ≥4 points and
% change from Baseline
Concomitant therapies
• TCS, TCI and prescription
moisturizers washed out ≥1 wk prior
to Baseline
• OTC emollient used bid for ≥1 wk
prior to Baseline and duration of study
• Medications known to affect AD only
used as rescue therapies
aPatients were seen every two weeks and received all study drug injections in the clinic; bAs defined by Hanifin and Rajka
AD, atopic dermatitis; bid, twice daily; BSA, body surface area; EASI, Eczema Area and Severity Index; EASI50/75/90, ≥50%/75%/90% improvement from Baseline in EASI; IGA, Investigator’s Global Assessment; IGA 0/1, score of 0 ‘clear’ or 1 ‘almost clear’ IGA from Baseline;
LEB, lebrikizumab; LD, loading dose; NRS, numeric rating scale; OTC, over-the-counter; Q2W, every 2 weeks; Q4W, every 4 weeks; TCI, topical calcineurin inhibitors; TCS, topical corticosteroids; Wk, week

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Patient Demographics and Baseline Disease Characteristics
10
Placebo Q2W
n=52
LEB 125 mg Q4W
n=73
LEB 250 mg Q4W
n=80
LEB 250 mg Q2W
n=75
Age, mean (SD), years 42.2 (18.2) 36.7 (16.5) 40.2 (17.9) 38.9 (17.4)
Male, no. (%) 28 (53.8) 27 (37.0) 33 (41.3) 26 (34.7)
Race, no. (%)
White 26 (50.0) 37 (50.7) 42 (52.5) 40 (53.3)
Black or African American 16 (30.8) 26 (35.6) 28 (35.0) 23 (30.7)
American Indian or Alaska Native 0 1 (1.4) 1 (1.3) 1 (1.3)
Asian 6 (11.5) 8 (11.0) 7 (8.8) 6 (8.0)
Multiple/Other 4 (7.7) 1 (1.4) 2 (2.5) 5 (6.7)
BMI, mean (SD), kg/m2 29.7 (8.0) 30.1 (7.7) 29.2 (6.9) 28.1 (6.4)
Disease duration, mean (SD), years 24.4 (17.4) 22.8 (15.4) 23.3 (16.7)b 22.1 (17.2)
EASI, mean (SD) 28.9 (11.8) 29.9 (13.5) 26.2 (10.1) 25.5 (11.2)
IGA, no. (%)
3, moderate 32 (61.5) 43 (58.9) 54 (67.5) 53 (70.7)
4, severe 20 (38.5) 30 (41.1) 26 (32.5) 22 (29.3 )
BSA involvement, mean (SD), percent 46.5 (22.7) 45.5 (24.5) 41.1 (20.9) 39.4 (21.5)
Pruritus NRS score,a mean (SD) 7.4 (2.4) 7.6 (2.0) 7.1 (2.4) 7.6 (1.9)
aPlacebo Q2W, n=49; LEB 125 mg Q4W, n=68; LEB 250 mg Q4W, n=77; LEB 250 mg Q2W, n=69; bn=79
Percentages are based on the number of patients in the modified intent-to-treat (mITT) population with a non-missing response
BMI, body mass index; BSA, body surface area; EASI, Eczema Area and Severity Index; IGA, Investigator’s Global Assessment (5-point scale); LEB, lebrikizumab; NRS, numeric rating scale; Q2W, every 2 weeks; Q4W, every 4 weeks; SD, standard deviation

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Patient Disposition
11
Placebo Q2W
n=52
n=23 (44.2%)
Screened
N=424
Randomized
n=280
LEB 125 mg Q4W
n=73
LEB 250 mg Q4W
n=80
LEB 250 mg Q2W
n=75
Discontinued
Adverse event
Lost to follow-up
Pregnancy
Protocol deviation
Withdrawal by patient
Physician decision
Other
n=58 (79.5%)
n=62 (77.5%)
n=58 (77.3%)
Completed
Week 16
Discontinued
Adverse event
Lost to follow-up
Pregnancy
Protocol deviation
Withdrawal by patient
Physician decision
Other
15
2
6
0
0
6
0
1
Discontinued
Adverse event
Lost to follow-up
Pregnancy
Protocol deviation
Withdrawal by patient
Physician decision
Other
18
3
5
0
0
7
2
1
Discontinued
Adverse event
Lost to follow-up
Pregnancy
Protocol deviation
Withdrawal by patient
Physician decision
Other
17
3
6
0
0
8
0
0
29
1
4
1
2
20
1
0
Reasons for discontinuation shown here are through Week 16 only, not end of study; percentages are based on the number of randomized subjects; one patient who was randomized in error was not included in the figure
LEB, lebrikizumab; Q2W, every 2 weeks; Q4W, every 4 weeks

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Topical Rescue Medication Use Was Low in Lebri-Treated Patients
12
• These findings suggest that TCS use would not have confounded study results
Placebo Q2W
n=52
LEB 125 mg
Q4W
n=73
LEB 250 mg
Q4W
n=80
LEB 250 mg
Q2W
n=75
Use of rescue meds, n (%) 18 (34.6) 9 (12.3) 10 (12.5) 10 (13.3)
Topical only 15 (28.8) 9 (12.3) 3 (3.8) 6 (8.0)
Systemic only 3 (5.8) 0 6 (7.5) 4 (5.3)
Topical and Systemic 0 0 1 (1.3) 0
Rescue medication duration (days), mean (SD)
Topical rescue 8.0 (12.6) 4.9 (5.2) 1.0 (0.0a) 2.5 (3.2)
aAll LEB 250 mg Q4W-treated patients who received topical rescue only required medication for 1 day; for this reason, the SD is zero
Modified intent-to-treat (mITT) population
LEB, lebrikizumab; Q2W, every 2 weeks; Q4W, every 4 weeks; SD, standard deviation; TCS, topical corticosteroids

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
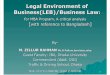
Early and Sustained Improvements in EASI Were Seen Through Week 16
13
At Week 16(Primary Endpoint)
To Week 16
-41.1
-62.3* -69.2
**-72.1***
-100
-80
-60
-40
-20
0
PlaceboQ2W (n=52)
LEB 125 mgQ4W (n=73)
LEB 250 mgQ4W (n=80)
LEB 250 mgQ2W (n=75)
LS
Me
an
Ch
an
ge
fro
m B
ase
line
(%
)
-25.4-31.3
-34.0
-40.6-42.4
-53.9
-62.5 -61.5*
-46.5
-61.2
-64.7-69.7**
-50.4
-64.1
-73.5 -72.8***
-100
-80
-60
-40
-20
0
0 4 8 12 16
Me
an
Ch
an
ge
fro
m B
ase
line
(%
)
Placebo Q2W (n=52)LEB 125 mg Q4W (n=73)LEB 250 mg Q4W (n=80)LEB 250 mg Q2W (n=75)
Week
*P<0.05, **P<0.01, and ***P<0.001 versus placebo from LS mean values and an analysis of covariance with a factor of treatment group and corresponding Baseline EASI score as a covariate
Missing values up through the Week 16 visit imputed using MCMC multiple imputation; post-Baseline up through Week 16 visit summary statistics represent average values, obtained by averaging the summary statistics generated from each imputed dataset
Modified intent-to-treat (mITT) population
EASI, Eczema Area and Severity Index; LEB, lebrikizumab; LS, least squares; MCMC, Markov chain Monte Carlo; Q2W, every 2 weeks; Q4W, every 4 weeks

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Dose-Dependent Improvements in Skin Manifestations Seen Across Secondary Endpoints
14
2.716.7 16.6
24.316.7
30.8
43.8 43.3
23.4
38.5
48.356.1
30.4
45.5
66.960.6
0
20
40
60
80
100
0 4 8 12 16
0.54.0 5.2
11.4
3.7 17.320.5
26.17.626.0
28.4
36.1
14.2
29.8
36.444.0
0
20
40
60
80
100
0 4 8 12 16
0.1
4.8 3.4 15.3
3.1
14.7
22.126.610.0
24.029.9
33.7
13.9
31.3
42.2 44.6
0
20
40
60
80
100
0 4 8 12 16
Placebo Q2W (n=52) LEB 125 mg Q4W (n=73) LEB 250 mg Q4W (n=80) LEB 250 mg Q2W (n=75)
EASI75
Week
EASI90
Week
IGA 0/1
Week
Pa
tie
nts
(%
)
Pa
tie
nts
(%
)
Pa
tie
nts
(%
)***
*****
**
**
*
*P<0.05, **P<0.01, and ***P<0.001 versus placebo from pairwise Cochran-Mantel-Haenszel tests
Missing values up through the Week 16 visit imputed using MCMC multiple imputation; post-Baseline up through Week 16 visit summary statistics represent average values, obtained by averaging the summary statistics generated from each imputed dataset
Modified intent-to-treat (mITT) population
EASI75/90, 75%/90% improvement from Baseline in Eczema Area and Severity Index; IGA 0/1, score of 0 ‘clear’ or 1 ‘almost clear’ in Investigator’s Global Assessment from Baseline; LEB, lebrikizumab; MCMC, Markov chain Monte Carlo; Q2W, every 2 weeks; Q4W, every 4 weeks

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Robust Improvement in Pruritus Scores at Week 16
15
NRS Change ≥4 Points Percent Change from Baseline
27.3
41.847.4
***70.0
39.343.5
46.2
**67.2
0
20
40
60
80
100
PlaceboQ2W
LEB 125 mgQ4W
LEB 250 mgQ4W
LEB 250 mgQ2W
Pa
tie
nts
(%
)
4.3
-35.9**
-49.6*** -60.6
***
-4.6
-36.5** -46.4
***-58.5***
-100
-80
-60
-40
-20
0
20
PlaceboQ2W
LEB 125 mgQ4W
LEB 250 mgQ4W
LEB 250 mgQ2W
LS
Me
an
Ch
an
ge
fro
m B
ase
line
(%
)
No imputation (observed cases)
MCMC imputation
n: 22 52 55 73 57 80 50 75
n: 22 52 55 73 56 80 50 75
No imputation (observed cases)
MCMC imputation
**P<0.01 and ***P<0.001 versus placebo; panel A: from pairwise Cochran-Mantel-Haenszel tests; panel B: from an analysis of covariance with a factor of treatment group and corresponding Baseline pruritus NRS as the covariate
Modified intent-to-treat (mITT) population
LEB, lebrikizumab; LS, least squares; MCMC, Markov chain Monte Carlo; NRS, numeric rating scale; Q2W, every 2 weeks; Q4W, every 4 weeks

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Rapid Improvements in Pruritus Scores
16
NRS Change ≥4 Points Percent Change from Baseline
Week
Week
13.2
27.5
37.1
39.3
28.6
16.7 19.0
27.321.1
32.7
34.0
42.3
51.0
44.7 46.741.8
19.7
30.9
46.6
50.9
50.057.1
56.8
47.4
31.7
51.9 51.958.5 61.8
63.368.2 70.0
0
20
40
60
80
100
0 2 4 6 8 10 12 14 16
Pa
tie
nts
(%
)
Placebo Q2WLEB 125 mg Q4WLEB 250 mg Q4WLEB 250 mg Q2W
-4.7
-25.4 -27.7-21.7 -22.4
-13.3
-15.8
6.8
-29.6-31.3
-32.0-39.6
-31.3-41.2 -41.9
-36.9
-21.9
-34.4
-45.0
-48.6
-44.5-50.9 -52.3
-48.6
-25.2
-38.8-53.0 -45.7
-57.1 -60.1-63.7 -61.8
-100
-80
-60
-40
-20
0
20
0 2 4 6 8 10 12 14 16
Me
an
Ch
an
ge
fro
m B
ase
line
(%
)
Placebo Q2WLEB 125 mg Q4WLEB 250 mg Q4WLEB 250 mg Q2W
***
**
***
***
● Differences in the proportions of patients achieving pruritus NRS change ≥4 points were seen by Day 2: 6.3%, 5.6%, 15.3% of LEB 125 mg Q4W, 250 mg Q4W, 250 mg Q2W versus 4.5% of placebo-treated patients, respectively
**P<0.01 and ***P<0.001 versus placebo; panel A: from pairwise Cochran-Mantel-Haenszel tests; panel B: from LS mean and an analysis of covariance with a factor of treatment group and corresponding Baseline pruritus NRS as the covariate
Modified intent-to-treat (mITT) population
Patient numbers fluctuate at each week as these are observed data
LEB, lebrikizumab; LS, least squares; NRS, numeric rating scale; Q2W, every 2 weeks; Q4W, every 4 weeks

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Safety and Tolerability
17
Placebo Q2W
n=52
LEB 125 mg Q4W
n=73
LEB 250 mg Q4W
n=80
LEB 250 mg Q2W
n=75
Patients reporting ≥1 TEAE, n (%) 24 (46.2) 42 (57.5) 39 (48.8) 46 (61.3)
Patients reporting ≥1 serious TEAE , n (%) 2 (3.8) 2 (2.7) 0 2 (2.7)
Number of serious TEAEs, no. 3 2 0 2
Deaths, n (%) 0 0 0 0
Patients who discontinued study due to TEAE,a n (%) 1 (1.9) 2 (2.7) 4 (5.0) 3 (4.0)
Common TEAEs reported in ≥5% in any LEB treatment group,b n (%)
Upper respiratory tract infection 3 (5.8) 6 (8.2) 9 (11.3) 2 (2.7)
Nasopharyngitis 2 (3.8) 4 (5.5) 2 (2.5) 9 (12.0)
Headache 3 (5.8) 3 (4.1) 1 (1.3) 4 (5.3)
Injection site pain 1 (1.9) 0 3 (3.8) 4 (5.3)
Fatigue 0 0 4 (5.0) 0
TEAEs of clinical interest, n (%)
Injection site reactionsc 1 (1.9) 2 (2.7) 4 (5.0) 7 (9.3)
Herpes viral infectionsd 2 (3.8) 2 (2.7) 4 (5.0) 2 (2.7)
Conjunctivitise 0 1 (1.4) 3 (3.8) 2 (2.7)
● Most TEAEs were mild or moderate in severity and did not lead to discontinuation
● Across all LEB AD studies,1 conjunctivitis has been reported at low rates similar to placeboaincludes 1 patient (in 250 mg Q4W) who discontinued after Week 16; bMedDRA Version 20.1 preferred terms; cIncludes MedDRA preferred terms injection site pain, erythema, pruritus, edema, swelling, rash, dermatitis, infection, and reaction; dIncludes MedDRA preferred terms oral
herpes, herpes zoster, genital herpes, herpes simplex, and eczema herpeticum; eIncludes MedDRA preferred terms conjunctivitis, conjunctivitis bacterial, and conjunctivitis allergic1Simpson EL, Flohr C, Eichenfield LF, et al. J Am Acad Dermatol. 2018;78(5):863-71.
LEB, lebrikizumab; Q2W, every 2 weeks; Q4W, every 4 weeks; TEAE, treatment-emergent adverse event

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Conclusions
18
▪ Lebri demonstrated a dose-dependent response across all endpoints measured, with marked improvement at both 250mg Q2W and Q4W doses
▪ For skin symptoms, an effect was seen at Week 4
▪ Effects on itch were observed as early as Day 2 in patients who received a 500 mg loading dose at Day 0
▪ Lebri was well tolerated, and consistent with previous studies, TEAE rates were low; across all lebri AD studies,1 conjunctivitis has been reported at low rates similar to those in patients receiving placebo
▪ These data highlight that selective blockade of IL-13 with lebri leads to improvements in key AD clinical severity scores and pruritus while maintaining a favorable safety profile
▪ In this Phase 2b, placebo-controlled study, all lebri groups showed dose-dependent and statistically significant improvement in the primary endpoint (percent change in EASI from Baseline at Week 16)
1Simpson EL, Flohr C, Eichenfield LF, et al. J Am Acad Dermatol. 2018;78(5):863-71.
AD, atopic dermatitis; IL, interleukin; LEB, lebrikizumab; Q2W, every 2 weeks; Q4W, every 4 weeks

Phase 3 Program OverviewLuis Peña, Chief Development Officer

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Phase 2b Data Support Opportunity for Best-in-Disease ProfileTarget product profile
20
Excellent
safety and
ease of use
• Safety profile consistent with that observed with dupilumab and other IL-13 inhibitors, with no
expectation of requirement for lab monitoring
Improved
tolerability
• Generally well tolerated, with a very low rate of conjunctivitis (similar to that reported in placebo patients)
Improved
efficacy
• Robust efficacy profile spanning skin lesions and pruritus, including strong performance across key
measures of most importance to patients and prescribers (e.g., EASI90, IGA0/1, pruritus NRS)
Improved
convenience• Opportunity for Q4W maintenance dosing

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Phase 3 Program OverviewDesigned to leverage Phase 2b results and health authority input to deliver best-in-disease profile
21
• Phase 3 program is designed to demonstrate a best-in-disease profile in AD, in accordance with the following key objectives:
• Maximize efficacy via use of 250 mg Q2W regimen as induction therapy (through Week 16 primary endpoint)
• Offer enhanced convenience via Q4W administration during maintenance therapy (after Week 16)
• Confirm attractive safety and tolerability profile
• Support simultaneous launch in adults and adolescents, to be followed quickly by launch in younger age groups
• Leveraging Phase 2b results and health authority input, the clinical program is designed as follows:
• Two pivotal, 52-week monotherapy studies in adults and adolescents
• ~800 patients (in aggregate) at ~200 sites in U.S., Europe and Asia
• Study in combination with TCS in adults and adolescents
• Additional studies to support registrational packages
1. Estimate provided as of October 17, 2019.

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Phase 3 Pivotal Monotherapy Study DesignTwo replicate studies designed to demonstrate best-in-disease profile in moderate-to-severe AD
22
Week 32 Week 40
Week 16
Objectives
• Replicate safety and
efficacy
• Establish long-term safety
and maintenance therapy
regimen
• Deliver best-in-disease
profile
Key inclusion criteria
• Adolescents (≥ 12 yo and ≥ 40 kg) and adults with
moderate-to-severe AD inadequately controlled with
topicals or for whom topical treatment is medically
inadvisable
− Chronic AD for ≥ 1 y
− EASI ≥ 16
− IGA ≥ 3 (on 0-4 scale)
− BSA ≥ 10%
Key endpoints
• Primary1: IGA0/1
• Secondary1:
− Skin lesions: EASI75/ 90, ∆EASI, BSA
− Pruritus: Pruritus NRS, sleep loss score
• Other:
− QOL: POEM, (C)DLQI, EQ5D, PROMIS
Anxiety and Depression, ACQ5
− Disease severity: SCORAD
Concomitant therapies
• TCS, TCI and prescription
moisturizers washed out ≥ 1 w prior
to baseline
• OTC emollient used bid for ≥ 1 w
prior to baseline and duration of
study
• Topical and systemic rescue therapy
only per protocol
Maintenance
Non-responders
(neither IGA0/1
nor EASI75)
Induction
Baseline
Op
en
-la
be
l e
xte
nsio
n
D/c
Week 24 Week 48 Week 52
Re
-ra
nd
om
ize
resp
on
de
rs:
(IG
A0
/1 a
nd
/or
EA
SI7
5, 2
:2:1
)
Lebri (n=267)
Loading dose + 250 mg Q2W
Placebo (n=133)
Lebri
250 mg Q2W
Scre
en
Ra
nd
om
ize
(n=
40
0, 2
:1)
Lebri
250 mg Q4W
Placebo
Escape: Lebri 250 mg Q2W
Non-responders (EASI50)
Non-responders (EASI50)
1. All primary and secondary endpoints will be assessed at week 16; in addition, certain secondary endpoints will be measured at earlier time points; EASI75 and IGA0/1 will be co-primary endpoints for European approval.

DERMIRA | LEBRIKIZUMAB PROGRAM UPDATE – OCTOBER 2019
Lebri is Positioned to Meaningfully Advance the Standard of Care for Patients with Moderate-to-Severe Atopic Dermatitis
23
AD is projected to become the largest market in dermatology.
Market for branded, systemic products is predicted to exceed $21B by 2027 driven by the introduction of new, differentiated
t therapies.
Lebri offers a differentiated mechanism of action that has the potential to be a best-in-disease therapy for AD.
IL-4/13 class is a validated, targeted approach that is becoming the standard-of-care for moderate-to-severe AD.
Phase 2b data suggest lebri may deliver the safety of the IL-4/13 class in addition to improvements in efficacy,
tolerability and convenience.
A profile well-suited for first-line use.
Based on the Phase 2b results, a Phase 3 program was initiated in early October 2019.
Topline results from the 16-week induction period of the two monotherapy studies expected in 1H 2021.
Recommended