7/29/2014
1
Welcome to
FDA Red Flags
Presenter:Chris Gustafson, AAS, ACA, BC‐HIS Evergreen Hearing Center, [email protected]
Fran VincentMarketing & Membership
Manager
Carrie PedersenProject Supervisor
IHS Organizers:
Note:
This presentation highlights recognized principles commonly found
in the legal arena, but in no way connotes nor should be considered as legal advice. It is recommended you consult your legal counsel for specific advice regarding legal matters that may be pertinent to you.
No relationship exists that represents a potential conflict of interest or special business relationship between the International Hearing Society and Chris Gustafson and Evergreen hearing Center or any of
its principals or employees.

7/29/2014
2
Housekeeping
This presentation is being recorded
CE credit is available! Visit ihsinfo.org for details
Note taking handouts are available at ihsinfo.org on the webinar page. Feel free to download now!
Agenda
The importance of the FDA and FTC Red flags
How FDA Red Flags relate to a series of medical conditions
FTC Red Flags and how they relate to marketing and policy
Q&A (enter your questions in the Question Box any time)
7/29/2014
3
THE FDA RED FLAGS
AND WHY ARE THEY SO IMPORTANT
The FDA RED FLAGS
1. Visible congenital or traumatic deformity of the ear
2. Active drainage from the ear in the past 90 days
3. Sudden loss within the past 90 day
4. Reported acute or chronic dizziness
5. Unilateral hearing loss of sudden or recent onset within
90 days
1. Air‐bone gap greater than 15dB at 500, 1 & 2k
2. Reported pain or discomfort
3. Excessive cerumen or foreign body in the ear

7/29/2014
4
#1 Visible congenital or traumatic deformity of the ear
Whenever we see an ear that is deformed, whether it is congenital, (meaning from birth), or acquired, which has occurred since birth or from trauma:
Identify through observation
Question the patient
Refer the patient on to a physician for medical clearance
#1 Visible congenital or traumatic deformity of the ear
Congenital Deformities
The term congenital means conditions that has existed since birth
Developmental
Deprivation
Disease processes
7/29/2014
5
#1 Visible congenital or traumatic deformity of the ear
Congenital Deformities
Microtia – abnormally small ears
Atresia – a congenital absence or complete closure of the ear canal or absence of the external auditory meatus.
This may be accompanied by undeveloped or under‐developed middle ear ossicles.
#1 Visible congenital or traumatic deformity of the ear
Acquired Deformities
Exostosis –
Bony growths arising from the surface of the bone within the bony portion of the ear canal
This results from prolonged exposure to cold water.
This can result in the narrowing or closure of the canal near the tympanic membrane.

7/29/2014
6
#1 Visible congenital or traumatic deformity of the ear
Acquired Deformities
Osteoma –
This is a single benign tumor resembling cortical bone occurring at the tympanomastoid structure line that tends to have a narrow base.
Again, this can result in the narrowing or closure of the canal near the tympanic membrane.
#1 Visible congenital or traumatic deformity of the ear
Acquired Deformities
Traumatic Deformity –
We are apt to see more of this as the veterans come into our offices as they have been exposed to violent explosions, extreme noise or embedment of a foreign object. Other trauma‐induced conditions may result from a blow to the head or result in cauliflower ear.
7/29/2014
7
#1 Visible congenital or traumatic deformity of the ear
Acquired Deformities
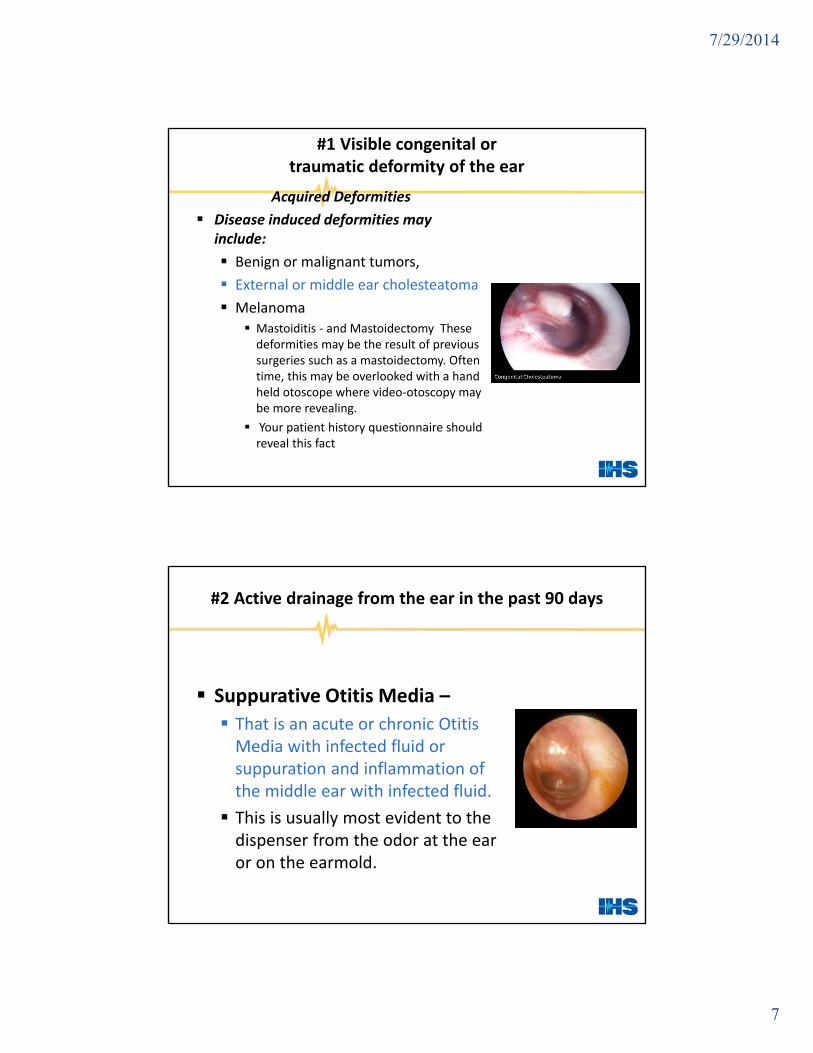
Disease induced deformities may include:
Benign or malignant tumors,
External or middle ear cholesteatoma
Melanoma Mastoiditis ‐ and Mastoidectomy These deformities may be the result of previous surgeries such as a mastoidectomy. Often time, this may be overlooked with a hand held otoscope where video‐otoscopy may be more revealing.
Your patient history questionnaire should reveal this fact
#2 Active drainage from the ear in the past 90 days
Suppurative Otitis Media –
That is an acute or chronic Otitis Media with infected fluid or suppuration and inflammation of the middle ear with infected fluid.
This is usually most evident to the dispenser from the odor at the ear or on the earmold.

7/29/2014
8
#2 Active drainage from the ear in the past 90 days
Staphylococcus – These bacteria is one of the most common forms of acute or chronic external otitis.
With extreme cases of Staphylococcus;
the external meatus may close entirely.
There may be edema (swelling due to abnormal accumulation of fluid), exudates (an infected fluid substance discharged from the cells or blood vessels ‐ pus).
#2 Active drainage from the ear in the past 90 days
Staphylococcus – The patient will report having pain at or near the ear. Staphylococcus usually responds well to antibiotics.
This may be more prevalent with swimmers.
It is more common in hot and humid climates.
7/29/2014
9
#2 Active drainage from the ear in the past 90 days
Staphylococcus – These bacteria is one of the most common forms of acute or chronic external otitis.
With extreme cases of Staphylococcus;
the external meatus may close entirely.
There may be edema (swelling due to abnormal accumulation of fluid), exudates (an infected fluid substance discharged from the cells or blood vessels ‐ pus).
#2 Active drainage from the ear in the past 90 days
Otomycosis – This is an infection due to a fungus in the external auditory canal. The most common complaint is itching.
Cerumen has a pH of 4 to 5 and so suppresses both bacterial and fungal growth. Aquatic sports, including swimming and surfing, are particularly associated because repeated exposure to water results in removal of cerumen and drying of the external auditory canal.
7/29/2014
10
#3 Sudden loss within the past 90 days
Any reported sudden or rapidly progressive hearing loss should set that little red flag waving in the back of our minds.
#3 Sudden loss within the past 90 days
The causes of a sudden loss may be from trauma, infection, disease, cochlear stroke, acoustic neuroma, ototoxicity or allergies.
In some cases with prompt medical attention, the loss may be reversed. So refer the patient immediately.

7/29/2014
11
#3 Sudden loss within the past 90 days
Trauma –
Head injuries resulting in
temporal bone fracture
concussion
direct injuries to middle or inner ear
barotrauma (drastic air pressure changes)
These are common with water skiing and scuba diving accidents
#3 Sudden loss within the past 90 days
influenza
scarlet fever
whooping cough
meningoencephalitis
viral cochleitis
mumps
measles
chicken pox
diphtheria
herpes zoster otitis
Viral Disease

7/29/2014
12
#3 Sudden loss within the past 90 days
Bacterial Disease
Meningitis
Bacterial labyrinthitis
#3 Sudden loss within the past 90 days
Case in Point The patient claimed her hearing aid died.
But . . .

7/29/2014
13
#3 Sudden loss within the past 90 days
Aminoglycosides
Aminoglycosides are a class of antibiotics used in treating infections caused by gram negative aerobic bacteria. All of these are ototoxic, and to some degree these are most vestiblotoxic.
#3 Sudden loss within the past 90 days
Aminoglycosides
• amikacin
• gentamycin
• kanamycin
• livodomycin
• neomycin
• netilmycin
• sisomycin
• streptomycin
• tobramycin
• So, basically –
• Any of the mycin family drugs.

7/29/2014
14
#3 Sudden loss within the past 90 days
Other Ototoxic Drugs
salicylates (aspirin)
iodine
sulfa drugs
quinine
#3 Sudden loss within the past 90 days
Tumors of the Middle and Inner Ear
glomus tumor
osteoma
middle ear carcinoma
cholesteatoma
acoustic neuroma
7/29/2014
15
#4 Reported acute or chronic dizziness
First, we must understand the difference between dizziness and vertigo. In either case, these patients should be referred to a physician for immediate investigation.
#4 Reported acute or chronic dizziness
Dizziness is a general term referring to an inability to maintain normal balance may be described as with nausea, hyperventilation, asphyxia or faintness, or light‐headedness due to circulatory problems or the sensation of spinning.

7/29/2014
16
#4 Reported acute or chronic dizziness
Vertigo is a vestibular symptom affecting spatial nystagmus, which the patient reports to having a spinning sensation or senses the environment spinning around.
#4 Reported acute or chronic dizziness
The causes might be the result of
Medication
Serious oto‐pathological illness vestibular dysfunction
acoustic neuroma
viral cochleitis
cochlear stroke
or Meniere's Disease

7/29/2014
17
#4 Reported acute or chronic dizziness
Meniere's Disease or endolymphatic hydrops
This is pathology affecting the inner ear and results in a sensorineural hearing loss, tinnitus and vertigo and a sensation of ear fullness.
These symptoms may appear separately or simultaneously.
The hearing loss can fluctuate usually affecting the lower frequencies at first and spreading to all frequencies as time elapses.
#5 Unilateral hearing loss of sudden or recent onset within 90 days
Trauma and disease are generally unilateral in nature and should be referred to a physician prior to proceeding with auditory rehabilitation.

7/29/2014
18
#5 Unilateral hearing loss of sudden or recent onset within 90 days
Some of the causes can include:
Meniere's disease
Acoustic neuroma
Perilymphatic Fistula
Trauma
Autoimmune Disease
Perforation of the Tympanic Membrane
Cholesteatoma
Otitis media
#6 Air‐bone gap greater than 15dB at 500, 1 & 2k Hz
When air‐bone gap of 15dB or greater occurs at 500Hz, 1,000Hz and 2,000Hz, it indicates that there is a potentially significant medically treatable condition.
7/29/2014
19
#6 Air‐bone gap greater than 15dB at 500, 1 & 2k Hz
Some causes of an air‐bone gap are:
In the outer ear and canal –
• Closure of the tragus
• Collapsed canal
• Atresia of the external ear
• Obstructions in the external auditory canal
• Accumulated cerumen or other debris
• Foreign object
• External otitis
• Fungus
• Pre‐and cancerous growths
#6 Air‐bone gap greater than 15dB at 500, 1 & 2k Hz
At the tympanic membrane:
Perforation
Post‐infection or surgical scar tissue
Thickening of the TM from tympanosclerosis
Extreme flaccidness
Fluid
Cholesteatoma
Glomus tumor

7/29/2014
20
#6 Air‐bone gap greater than 15dB at 500, 1 & 2k Hz
Within the middle ear:
Otosclerosis
Disarticulation
Otitis media
Mastoiditis
Cholesteatoma
Glomus tumor
#7 Reported pain or discomfort
The patient may report to having pain in and around the ear which may indeed be related to the ear or it may be as a result of mandibular joint (TMJ) or orthodontic abnormalities such as dental oversensitivity or sinus problems.
These should be reported unless they are under the current care of a physician or dentist.

7/29/2014
21
#7 Reported pain or discomfort
With visual assessment we should be able to determine the presence of swelling, the absence of the cone of light on the TM, redness or drainage in the ear canal.
Serious ear disease, trauma, or acquired abnormalities may also be the cause.
All, of which, should raise that red flag and be referred for immediate medical treatment.
#8 Excessive cerumen or foreign body in the ear
Impacted cerumen may result in:
Conductive hearing loss
Increased incidence of Tinnitus
Chronic cough
Tearing eyes
Interaural attenuation
Complaints of occlusion

7/29/2014
22
#8 Excessive cerumen or foreign body in the ear
Impacted cerumen may result in:
Depending on the sensorineural hearing loss, the audiometric pattern may be worse in the low frequencies with normal SN hearing to a flat loss configuration with a high frequency hearing loss.
#8 Excessive cerumen or foreign body in the ear
Impacted cerumen may result in:
Obstructed otoscopy of the canal and tympanic membrane.
Inability to perform impedance audiometry and acoustic reflexes
Inaccurate Audiometric test results
Inability to perform probe mic measurements
An accurate ear impression cannot be taken
The use of a hearing aid may cause excessive feedback or reduced gain

7/29/2014
23
#8 Excessive cerumen or foreign body in the ear
"Significant," but not impacted, cerumen accumulation may result in:
Loss of natural ear canal resonance
Inaccurate Tympanometry results
Inaccurate probe mic measurements
Obstructed view of the canal and TM landmarks
Cerumen adhering to the tympanic membrane may cause Interaural attenuation and elevated hearing thresholds
Taking an ear impression may cause increased cerumen impaction
FTC RED FLAGSAND WHAT IT MEANS TO THE DISPENSER

7/29/2014
24
FTC RED FLAGS
According to the Federal Trade Commission
“Our mission”: To prevent business practices that are anticompetitive, deceptive, or unfair to consumers
The Federal Trade Commission works for consumers to prevent fraudulent, deceptive, and unfair business practices and to provide information to help spot, stop, and avoid them.
FTC RED FLAGS
Expert Endorsements
If an ad claims the endorser is an expert, the endorser must be qualified as an expert
Endorsements must be supported by actual exercise of expertise in evaluating the product
Comparison claims must be based on the expert’s evaluation

7/29/2014
25
FTC RED FLAGS
Endorsements
Focus is on the consumer’s perception of whether the message is an “endorsement” Fundamental question is whether the relationship between the advertiser and the speaker is objectively such that the speaker’s statement can be considered “sponsored by the advertiser”
If it is, then an endorsement
FTC RED FLAGS
Examples – Expert Endorsements
Hearing aid ad where endorser is referred to as a “doctor” implies she is a medical doctor; ad must make clear the nature and limits of endorser’s expertise.

7/29/2014
26
FTC RED FLAGS
Examples – General Considerations
• False and misleading – Doctor claims product is “clinically proven to work” even though she knows the clinical study has serious flaws
• False and misleading – Company pays a blogger to try new product and write a review; company is liable for any claims blogger makes about product and blogger is liable for misleading or unsubstantiated claims and is liable if she fails to disclose clearly and conspicuously that she is being paid
FTC RED FLAGS
ADVERTISING
If you take a manufacturer’s ad and change it, you need to send it back to the manufacturer for approval before you print and publish the ad.
You, may be liable as well as the manufacturer, if the ad is not accurate!

7/29/2014
27
FTC RED FLAGS
Example of Unsubstantiated and False Claims
Dahlberg, Inc. (1995) Hearing aid manufacturer claimed product would enable persons to distinguish and understand speech sounds in group or noisy situations, would restore natural hearing, and could reverse, halt or delay hearing loss progression
FTC concluded claims were unsubstantiated and false Failure to disclose material fact that person may not receive any significant benefit from any hearing aid Violation of a 1976 FTC order Settlement of $2.75 million
FTC RED FLAGS
Example of Unsubstantiated and False Claims
Media Maverick, Inc. (2004)
Marketer of metal bracelet that was allegedly “electro‐polarized” claimed product relieved pain; product was promoted on 30‐minute informercials and on the internet
FTC concluded claims were unsubstantiated and false Clinical testing showed product was no better than placebo
Settlement of $400,000

7/29/2014
28
FTC RED FLAGS
Providers who allow deferred payments must comply with the FTC Rulings by August 1, 2012
Interim Final Rule Narrows the Circumstances Under Which Creditors Are Covered
For Release
November 30, 2012
FTC RED FLAGS
Under the Rule, Red Flag Programs must have four parts. First, the Program must include reasonable policies and procedures to identify signs – or “red flags” – of identity theft in the day‐to‐day operations of the business.

7/29/2014
29
FTC RED FLAGS
Second, the Program must be designed to detect the red flags of identity theft identified by the business.
FTC RED FLAGS
Third, the Program must set out the actions the business will take upon detecting red flags.

7/29/2014
30
FTC RED FLAGS
Finally, because identity theft is an ever‐changing threat, a business must re‐evaluate its program periodically to reflect new risks from this crime.
FTC RED FLAGS
Case in Point
John Doe comes in to buy
Educate your staff and keep your programs current

7/29/2014
31
References
FDA
Singular’s Illustrated Dictionary of Audiology
Patient.co.uk
WebMD Health Search
The FDA Red Flags Video Otoscopy Observation and Referral
By Max Stanley Chartrand, PhD, BC‐HIS
www.fda.gov/medicaldevices/deviceregulationandguidance
Meg Gustafson. MS, FAAA
References
FTC ‐
www.ftc.gov/opa/2013/06/redflags.shtm
Google search FTC Red Flags
HIA Annual Meeting
Jeffrey N. GibbsHyman, Phelps & McNamara, P.C.
Washington, DC

7/29/2014
32
Questions
Enter your question in the Question Box on your webinar dashboard
THANK YOU FOR ATTENDING!
Contact Chris Gustafson:
For more info on obtaining a CE credit for this webinar, visit www.ihsinfo.org
Recommended




![The Assessment of Endolymphatic Hydrops with High-resolution … · 2020. 6. 27. · canal [17, 18], our assessment was limited to the cochlea and the vestibule. A significantly higher](https://img.pdfslide.us/doc/110x75/6140ce9583382e045471af25/the-assessment-of-endolymphatic-hydrops-with-high-resolution-2020-6-27-canal.jpg)