Embed Size (px)
Citation preview

Poster Print Size: This poster template is 44” high by 44” wide. It can be used to print any poster with a 1:1 aspect ratio.
Placeholders: The various elements included in this poster are ones we often see in medical, research, and scientific posters. Feel free to edit, move, add, and delete items, or change the layout to suit your needs. Always check with your conference organizer for specific requirements.
Image Quality: You can place digital photos or logo art in your poster file by selecting the Insert, Picture command, or by using standard copy & paste. For best results, all graphic elements should be at least 150-200 pixels per inch in their final printed size. For instance, a 1600 x 1200 pixel photo will usually look fine up to 8“-10” wide on your printed poster.
To preview the print quality of images, select a magnification of 100% when previewing your poster. This will give you a good idea of what it will look like in print. If you are laying out a large poster and using half-scale dimensions, be sure to preview your graphics at 200% to see them at their final printed size.
Please note that graphics from websites (such as the logo on your hospital's or university's home page) will only be 72dpi and not suitable for printing.
[This sidebar area does not print.]
Change Color Theme: This template is designed to use the built-in color themes in the newer versions of PowerPoint.
To change the color theme, select the Design tab, then select the Colors drop-down list.
The default color theme for this template is “Office”, so you can always return to that after trying some of the alternatives.
Printing Your Poster: Once your poster file is ready, visit www.genigraphics.com to order a high-quality, affordable poster print. Every order receives a free design review and we can deliver as fast as next business day within the US and Canada.
Genigraphics® has been producing output from PowerPoint® longer than anyone in the industry; dating back to when we helped Microsoft® design the PowerPoint® software.
US and Canada: 1-800-790-4001
Email: [email protected]
[This sidebar area does not print.]
Using Transtympanic Gadolinium and MRI in distinguishing between Meniere’s and Migraine
Warren C. Swegal, MD and Syed F. Ahsan, MD
Dept. of Otolaryngology, Henry Ford Health System, Detroit, MI
Dr. Warren C. Swegal Dept. of Otolaryngology Henry Ford Health System Email: [email protected] Phone: 313-916-7086 Fax: 313-916-7263
Contact 1. Boismier TE, Disher MJ. Spontaneous vertigo and headache: endolymphatic hydrops or migraine? Ear Nose Throat J. 2001;80(12):881 2. Lee HJ, Jeon JH, Park S, Kim BG, Lee WS, Kim SH. Prevalence and clinical significance of spontaneous low-frequency air-bone gaps in Ménière's disease. Otol Neurotol. 2014 Mar;35(3):489-94. 3. Hong HR, Shim DB, Kim TS, Shim BS, Ahn JH, Chung JW, Yoon TH, Park HJ. Results of caloric and sensory organization testing of dynamic posturography in migrainous vertigo: comparison with Meniere's
disease and vestibular neuritis. Acta Otolaryngol. 2013 Dec;133(12):1236-41 4. Rauch SD, Zhou G, Kujawa SG, Guinan JJ, Herrmann BS. Vestibular evoked myogenic potentials show altered tuning in patients with Ménière's disease. Otol Neurotol. 2004;25(3):333. 5. Orchik DJ, Shea JJ Jr, Ge X. Transtympanic electrocochleography in Menière's disease using clicks and tone-bursts. Am J Otol. 1993 May;14(3):290-4. Review. 6. Shi H, Li Y, Yin S, Zou J. The predominant vestibular uptake of gadolinium through the oval window pathway is compromised by endolymphatic hydrops in Ménière's disease. Otol Neurotol. 2014
Feb;35(2):315-22. 7. Claes G, Van den Hauwe L, Wuyts F, Van de Heyning P. Does intratympanic gadolinium injection predict efficacy of gentamicin partial chemolabyrinthectomy in Menière's disease patients? Eur Arch
Otorhinolaryngol. 2012 Feb;269(2):413-8. 8. Hornibrook J, Coates M, Goh A, Gourley J, Bird P. Magnetic resonance imaging for Ménière's disease: correlation with tone burst electrocochleography. J Laryngol Otol. 2012 Feb;126(2):136-41. 9. Fukuoka H, Takumi Y, Tsukada K, Miyagawa M, Oguchi T, Ueda H, Kadoya M, Usami S. Comparison of the diagnostic value of 3 T MRI after intratympanic injection of GBCA, electrocochleography, and the
glycerol test in patients with Meniere's disease. Acta Otolaryngol. 2012 Feb;132(2):141-5.
References
Objective: To describe the use of MRI imaging using Transtympanic Gadolinium (TT Gad) in distinguishing between Vertiginous Migraine and Meniere's Disease (MD) in a patient with vertigo. Study Design: Case Report Methods: Patient’s chart was reviewed for reports of vertigo, vestibular function tests and Imaging. The patient underwent TT Gad injection followed by MRI to assess for endolymphatic hydrops (EH). Audiogram before and after was assessed. Results: A 43 yo man presented with recurrent vertigo attacks lasting more than one hour with right side aural fullness, tinnitus, sensitivity to sound and temperature as well as left side headaches. Vestibular testing demonstrated reduced vestibular response on the left, possible EH on the right, and cervical Vestibular Evoked Myogenic Potential suggesting possible right side superior semicircular canal dehiscence. Patient was counseled about performing an MRI after TT Gad injection to rule in Meniere’s disease. MRI 3D FLAIR sequence ruled out EH and he was started on a Migraine diet. He was treated for migraines and his vertigo and headaches improved by over 90%. Discussion: This is an interesting report because using TT Gad and MRI was able to distinguish between MD and Migraine in a patient who presented with symptoms suggestive of both and when conventional vestibular testing gave inconclusive and a complex picture. This has the potential to save the patient from unnecessary treatment for MD and side effects as well as reduced the time to a diagnosis.
Abstract
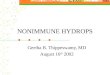
Thus, it was recommended that the patient undergo an MRI using TT Gad to assess for EH. The injection was performed as an outpatient. - Magnevist gadolinium 1/8th dilution in sterile water - 0.6mL injected through the posterior anterior quadrant - Patient was observed for 30 min, patient tolerated it well - The following day the patient underwent an MRI Results: - Limited visualization of lateral semicircular canals bilaterally on
T2-eighted images, likely a susceptibility artifact (Figure 2) - Homogenous distribution of injected gadolinium on perilymphatic
inversion recovery on right ear - Membranous labyrinth in continuity on Endolymphatic sequence No evidence of endolymphatic hydrops
Case Details
The patient’s initial audiogram (Figure 1) demonstrated a right sided conductive hearing loss. At this point multiple etiologies were discussed with the patient. However it was felt that the 2 most likely etiologies included Meniere’s Disease vs. Vertiginous Migraines with semicircular canal dehiscence also a possibility. The patient was referred for further testing including videonystagmography (VNG), electrocochleography (ECOG), cervical vestibular-evoked myogenic potential (cVEMP) testing, and rotational chair testing to better delineate the cause of vertigo. (Table 1) However, when taken together, balance function testing was inconclusive although Rotary Chair test demonstrated vestibular compensation.
Clinical Course
Vertigo can be a challenging patient complaint. However there are multiple modalities to help delineate the route cause of this symptom. Our patient’s clinical picture did not lead to a definitive diagnosis. Prior research would suggest that treating the patient for MD and switching to treat migraines is reasonable.1 However, this approach may cause a delay in diagnosis and could potential lead to future non-compliance. Thus further testing was pursued. The audiogram, with the low frequency hearing loss may be suggestive of meniere’s.2 The VNG was showed vestibular weakness on the left and cVEMP demonstrated hypersensitivity on the right, opposite of what would be expected in either MD or migraines.3,4 However, ECOG demonstrated EH, suggestive of MD.5 Recently, MRI with TT Gad has been shown to be safe and effective at assessing for EH.6,7 Furthermore, there is limited evidence to suggest it may be more effective than ECOG at identifying EH.8,9 In this case, MRI with TT Gad did not demonstrate EH when ECOG did. The MRI findings allowed the patient to be diagnosed correctly and treated appropriate. The success of the migraine treatment further confirms that this patient suffered from Vertiginous Migraines and not MD.
Discussion
In a patient who’s clinical picture lead to several different diagnoses, and who’s test results did not support a single diagnosis, MRI with TT Gad was able to rule out Meniere’s disease as the cause of his symptoms. This prevented unnecessary trial and error medical treatment and a delay in diagnosis. Furthermore, this case demonstrated the relative feasibility of the MRI with TT Gad, potentially paving the way for it to be used in other disease models.
Conclusions
Test Details Right Ear Left Ear
VNG Warm Caloric 53 degree/sec 6 Degree/sec
Cold Caloric 9 Degree/sec 3 Degree/sec
Summary 75% Weakness on Left
cVEMP Tone Burst Threshold
60dBnHl 90dBnHL
Summary Hypersensitivity on Right (Normal 75-100nHL)
ECOG SP/AP Ratio 0.77 0.38
Summary Consistent with EH on right (Normal <0.5)
HPI: The patient is a 43 yo male who presented with episodic vertigo for 3-4 years with sound hypersensitivity. - Attacks were preceded by Right side aural fullness, pressure
sensation, tinnitus, and occasionally headaches - Episodes lasted over 1 hour but less than 4 hours - He denied hearing loss or autophony - Increased frequency of attacks with higher salt intake PMHx: Sinusitis, GERD, Anxiety, Migraines Physical Exam: - Otoscopic exam benign, TMs mobile - Cranial Nerves Grossly intact - Hennebert’s and Tullio’s negative - Negative Head thrust, Dix Hallpike and Fukuda tests - Non-specific imbalance during Romberg
MRI with TT Gad
Figure 1. Initial Audiogram
Table 1. Selected results from balance function testing.
- 1 week after the MRI, the patient denied any major effects from the TT-Gad. He denied otalgia, otorrhea, tinnitus or vertigo.
- 2 months after MRI, patient had seen a neurologist and was being treat for with valproate for the migraines, no vertigo
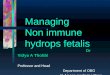
- 5 months after MRI, headaches 90% improved, no vertigo - 8 months after MRI, no vertigo, Audiogram normal (Figure 3)
Post Scan Follow up
Figure 2. MRI with TT Gad
Figure 3. Audiogram 8 Months post injection