Whufrt
Mtndnt
chwenvvrdpstvsmt
FF
moF
v
CASE REPORT
©A
IDENTIFICATION OF ECTOPIC URETER IN INCONTINENTGIRL USING MAGNETIC RESONANCE IMAGING
ANAND KRISHNAN AND LAURENCE S. BASKIN
ABSTRACTe present the case of a 3.5-year-old girl who presented with continuous urinary leakage and a classic
istory suggesting an ectopic ureter, but an inconclusive physical examination and normal imaging byltrasonography. Magnetic resonance imaging was finally able to identify an ectopic ureter draining a poorlyunctioning upper pole of a duplex system as the culprit. We discuss the increasing value of magneticesonance imaging in identifying subtle pediatric genitourinary anomalies, such as in our case, and discusshe management options. UROLOGY 65: 1002.e17–1002.e18, 2005. © 2005 Elsevier Inc.
tfitduc
nsutrpdthdscicagwrftodF
agnetic resonance imaging (MRI) has be-come an increasingly popular modality for
he evaluation and diagnosis of pediatric genitouri-ary tract anomalies. We report a case using MRI toiagnose an ectopic ureter that caused inconti-ence in a girl after a negative workup by tradi-ional imaging modalities.
CASE REPORT
A 3.5-year-old girl presented with a history ofontinuous urinary leakage. A thorough historyad revealed no periods of prolonged dryness andetness within 10 minutes of voiding. Her physical
xamination was unremarkable and showed no ab-ormal perineal openings, and a voiding diary re-ealed continuous incontinence despite frequentoiding. Renal bladder ultrasonography (Fig. 1A)evealed two normal kidneys without evidence ofuplication or ureteral dilation, and a normal-ap-earing bladder. Voiding cystourethrographyhowed no evidence of reflux and a smooth bladderhat voided to completion. She was diagnosed withoiding dysfunction and placed on a timed voidingchedule and bowel regimen. When no improve-ent was noted on follow-up, MRI was performed
hat revealed a complete duplication anomaly of
rom the Department of Urology, University of California, Sanrancisco, School of Medicine, San Francisco, CaliforniaAddress for correspondence: Anand Krishnan, M.D., Depart-
ent of Urology, University of California, San Francisco, Schoolf Medicine, 513 Parnassus Avenue, HSW 1434, Box 0565, Sanrancisco, CA 94122. E-mail: [email protected]: September 20, 2004, accepted (with revisions): No-
tember 22, 2004
2005 ELSEVIER INC.LL RIGHTS RESERVED
he left kidney (Fig. 1B). Open exploration con-rmed the presence of an ectopic ureter draininghe left upper moiety (Fig. 2), and the patient un-erwent distal ureteroureterostomy. At last follow-p, she was voiding at normal intervals and wasontinent.
COMMENT
Continuous day and nighttime urinary inconti-ence in a young girl should always raise a red flaguggesting ureteral duplication with an ectopicreter as the culprit. In the modern era of imaging,his finding can usually be detected by ultrasonog-aphy, which will show a duplicated system andossibly hydroureteronephrosis, depending on theegree of residual function and drainage of the ec-opic system. Sometimes, despite a classic clinicalistory, a thorough physical examination and tra-itional radiographic imaging may fail to reveal theuspected anomaly. This should not, however, dis-ourage the urologist from pursuing this diagnosisf a strong clinical suspicion remains. MRI is be-oming an increasingly popular modality for bothnatomic and functional imaging of the pediatricenitourinary tract. It has shown equal efficacyith traditional functional imaging studies, supe-
ior morphologic imaging of the urinary tract be-ore surgical intervention,1 and avoids the poten-ially deleterious effects of ionizing radiation. Inur case, MRI was invaluable in making the correctiagnosis despite negative ultrasound findings.ew such reports have been published.2The treatment options for the ectopic ureter in
he incontinent girl include partial nephrectomy if
0090-4295/05/$30.00doi:10.1016/j.urology.2004.11.040 1002.e17
tcmf
niaws
itrost
sai1
dn
co
Fg ure
Fpeo
1
he moiety has minimal function and ureteroneo-ystostomy or ureteroureterostomy if an attempt isade at renal salvage. Ureteroureterostomy allows
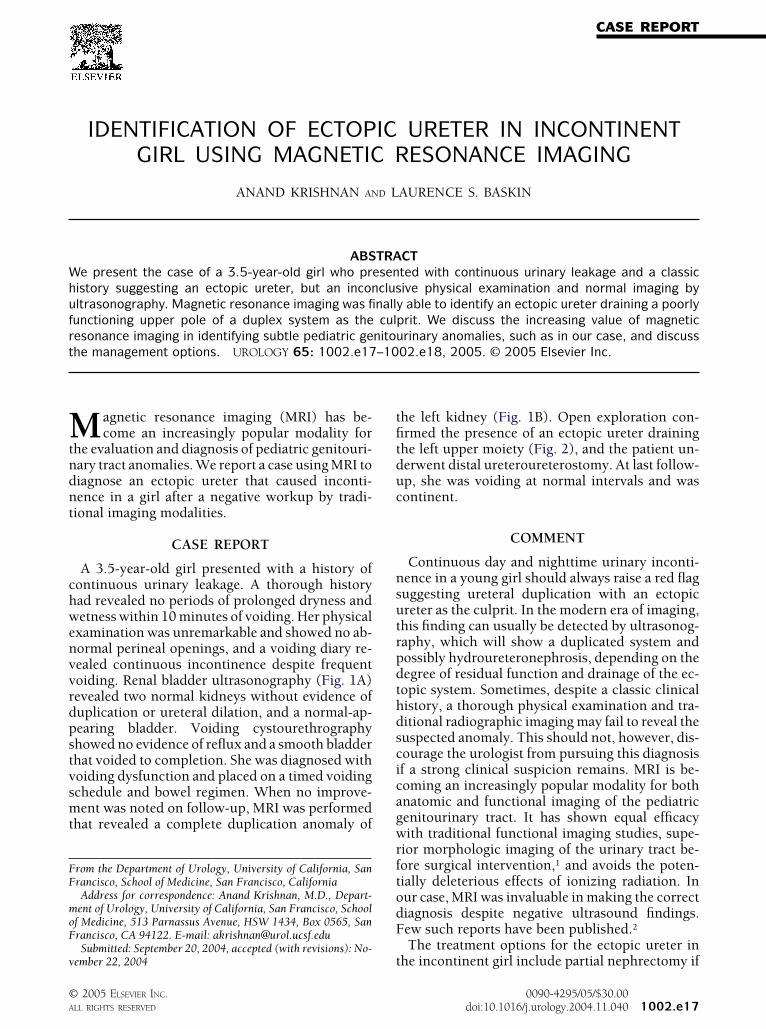
IGURE 1. (A) Ultrasound scan demonstrating normaladolinium (7-minute image). Arrow identifies separate
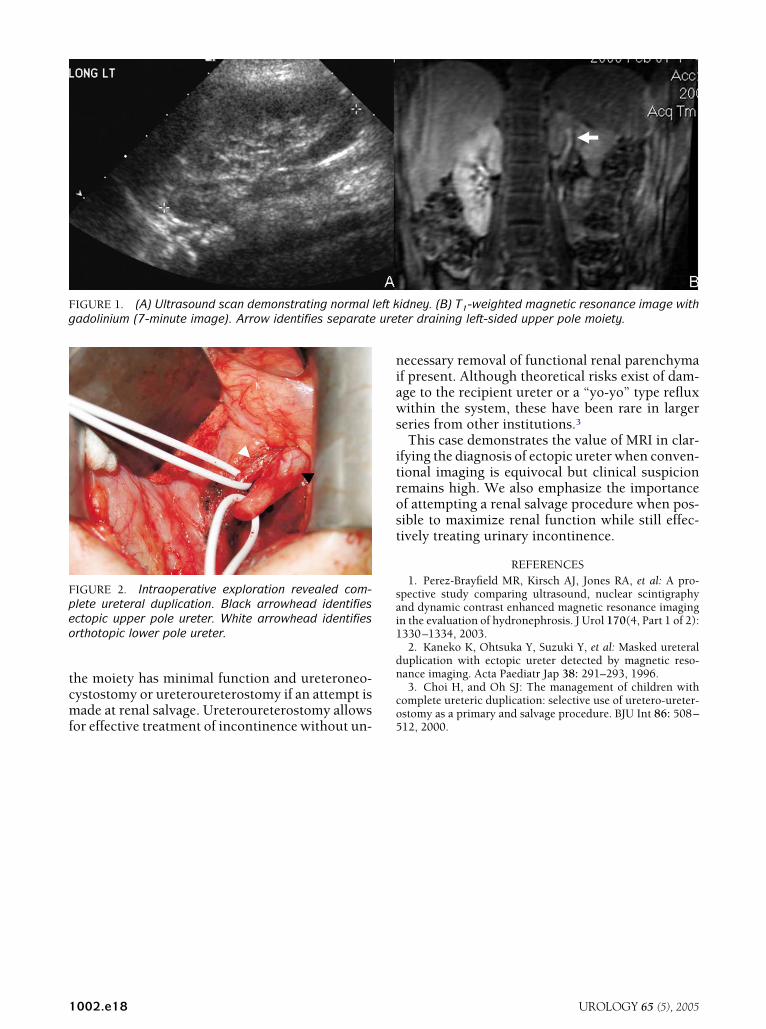
IGURE 2. Intraoperative exploration revealed com-lete ureteral duplication. Black arrowhead identifiesctopic upper pole ureter. White arrowhead identifiesrthotopic lower pole ureter.
or effective treatment of incontinence without un- 5
002.e18
ecessary removal of functional renal parenchymaf present. Although theoretical risks exist of dam-ge to the recipient ureter or a “yo-yo” type refluxithin the system, these have been rare in larger
eries from other institutions.3This case demonstrates the value of MRI in clar-
fying the diagnosis of ectopic ureter when conven-ional imaging is equivocal but clinical suspicionemains high. We also emphasize the importancef attempting a renal salvage procedure when pos-ible to maximize renal function while still effec-ively treating urinary incontinence.
REFERENCES1. Perez-Brayfield MR, Kirsch AJ, Jones RA, et al: A pro-
pective study comparing ultrasound, nuclear scintigraphynd dynamic contrast enhanced magnetic resonance imagingn the evaluation of hydronephrosis. J Urol 170(4, Part 1 of 2):330–1334, 2003.2. Kaneko K, Ohtsuka Y, Suzuki Y, et al: Masked ureteral
uplication with ectopic ureter detected by magnetic reso-ance imaging. Acta Paediatr Jap 38: 291–293, 1996.3. Choi H, and Oh SJ: The management of children with
omplete ureteric duplication: selective use of uretero-ureter-stomy as a primary and salvage procedure. BJU Int 86: 508–
idney. (B) T1-weighted magnetic resonance image withter draining left-sided upper pole moiety.
left k
12, 2000.
UROLOGY 65 (5), 2005
Recommended