Embed Size (px)
Citation preview

B Y
M U H A M M A D Z E E S H A N K H A N
A N D
S A N A J A W E D
ECTOPIC PREGNANCY (EP)
OBJECTIVE OF PRESENTATION
AT THE END OF PRESENTATION YOU SHOULD KNOW:
NORMAL SITE OF IMPLANTATION IN PREGNANCY
DEFINITION OF EP
ABNORMAL SITES OF IMPLANTATION IN EP
INCIDENCE
ETIOLOGY
CLINICAL MANIFESTATION
INVESTIGATION
MANAGEMENT
NORMAL SITES OF IMPLANTATION IN PREGNANCY
Implantation is the very early stage of pregnancy at
which the conceptus adheres to the wall of the uterus. At
this stage of prenatal development, the conceptus is
a blastocyst.
Normal site of implantation is posterior-superior wall of
the Body of uterus in most of the cases.
In addition anterior wall of body of uterus also
constitutes the normal site of implantation.
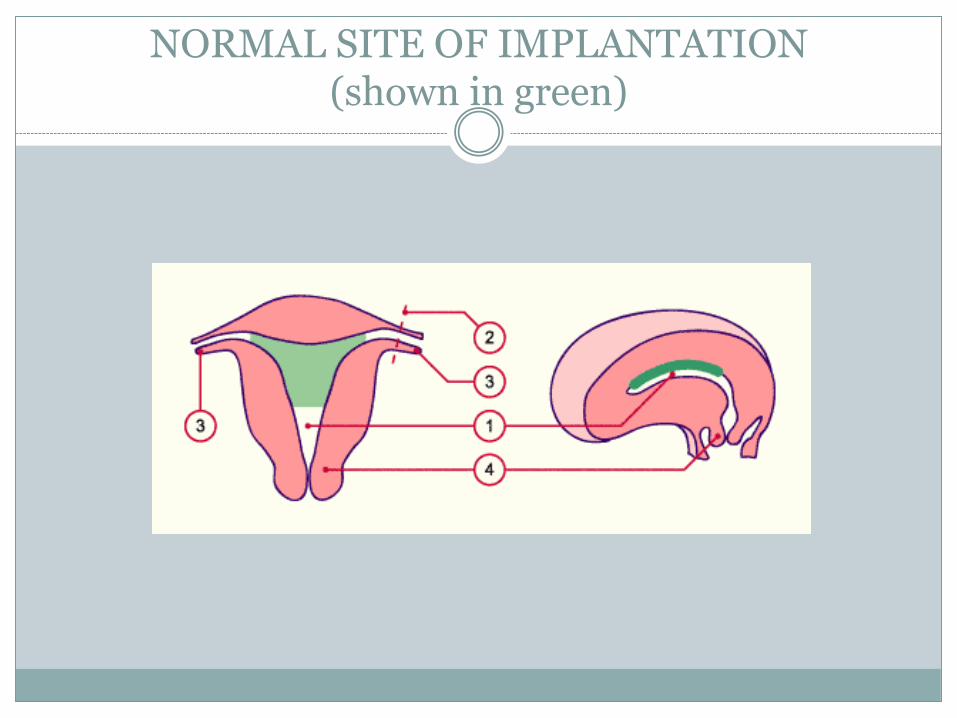
NORMAL SITE OF IMPLANTATION (shown in green)

WHAT IS ECTOPIC PREGNANCY
“IMPLANTATION OF CONCEPTUS OUTSIDE THE
NORMAL UTERINE CAVITY”.
NOTE: 1. ECTOPIC PREGNANCY VIRTUALLY NEVER LEADS TO FETAL
VIABILITY.
2. ALL SITES IN UTERINE CAVITY ARE CONSIDERED NORMAL FOR EP BUT
not IN GENERAL…
SITES OF IMPLANTATION OF ECTOPIC PREGNANCY
COMMON SITES OF IMPLANTATION ARE
1. Fallopian tubes ( 95 % of total cases of ectopic pregnancy )
a. Ampulla (74 % of 95%)
b. Isthmus ( 12 % of 95%)
c. Fimbrial end of the tube ( 12 % of 95%)
d. Interstitium ( 2% of 95%)
2. Ovaries ( 3-4 % of total)
3. Peritoneal cavity ( 1-2 % of total)

COMMON SITES OF EP
INCIDENCE
The frequency of ectopic pregnancy was 1 .3%.
Majority of patients with ectopic pregnancy were in 2 1-
30 years age group (74%)
Multiparous women were found to be more prone to have
ectopic pregnancy (6 1%).
The gestational age ranged between 4-11 weeks and the
most frequent gestational age was around 6 weeks.
ETIOLOGY/ RISK FACTORS
AMONG THE KNOWN RISK FACTORS / CAUSES OF ECTOPIC
PREGNANCIES ARE
1. Tubal Disease ; e.g. inflammatory condition due to ascending
infection i.e. PID. accounts for 40 % cases of ectopic pregnancy.
2. Previous EP
3. Previous tubal surgery.
4. Subfertility
5. Use of IUD.
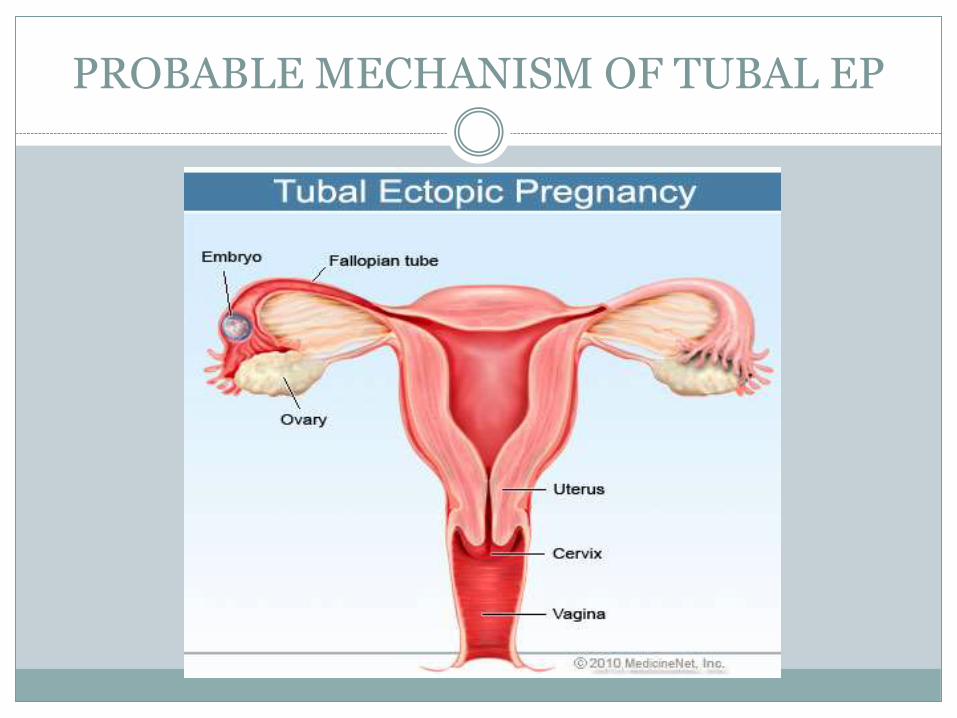
PROBABLE MECHANISM OF TUBAL EP
CLINICAL MANIFESTATION OF EP
SUBACUTE PRESENTATION
1. ABDOMINAL/PELVIC PAIN(79%) , PAIN CAN BE LOCALIZED TO ILIAC FOSSA
2. VAGINAL BLEEDING(53%) , DARK RED INDICATIVE OF OLD BLOOD.
3. PAIN AT SHOULDER TIP RARE PRESENTATION , INDICATIVE OF FREE BLOOD IN ABDOMINAL CAVITY CAUSING DIPHRAGMATIC IRRITAITON.
CONT.

CLINICAL MANIFESTATION OF EP
ACUTE PRESENTATION
It occurs in cases of ruptured ectopic pregnancy and
patient presents with the symptoms of massive
intraperitoneal bleeding.
1. Hypovolemic Shock
2. Acute abdomen
INVESTIGATIONS OF EP
Useful investigations for the diagnosis of ectopic pregnancy.
OBSERVATIONS- VITALS
βHCG
TVS
LAPROSCOPY
Rarely used
Progesterone levels
βHCG
This hormone is a glycoprotein produced by placenta
Half life is 24 hours
Peaks at around 10weeks
Levels double every 48 hours in a normally developing pregnancy
Beta HCG less than 5mIU/ml is considered negative for pregnancy
Anything more than 25mIU/ml is considered positive for
pregnancy
In ectopic pregnancy:
Empty uterus on abdominal U/S with BHCG >6000mIU/ml
Empty uterus on vaginal U/S with BHCG >200mIU/ml
TRANSVAGINAL U/S SCAN(TVS)
An intrauterine GS should be visualized at 4.5weeks and corresponding
BHCG is 1500mIU/ml.
At 5th week GS with fetal heartbeat is detected with BHCG level around
3000mIU/ml
High BHCG level and no IU pregnancy seen on TVS is suggestive of
ectopic pregnancy
Presence of free fluid during TVS is suggestive of ruptured ectopic
pregnancy
FALSE NEGATIVE occurs in case of heterotopic pregnancy. i.e.
simultaneous pregnancy within and outside the uterus.

DIAGRAM SHOWING TVS
LAPROSCOPY
This is the gold standard test
Endoscope is inserted into the abdomen to allow a
surgeon to see fallopian tubes and other organs and
do surgery at the same time

DIAGRAM SHOWING LAPROSCOPY
PROGESTERONE LEVELS
Progesterone is a hormone formed by corpus luteum
>25ng/ml is related with normal intrauterine
pregnancy
<5ng/ml is related with ectopic or non viable
pregnancy
MANAGEMENT OF EP
Depending on clinical presentation and patients
choice:
EXPECTANT (Do nothing)
MEDICAL (Do something)
SURGICAL (Do everything)
EXPECTANT
Based on assumption that all tubal pregnancies
will resolve through regression or miscarriage
without any treatment.
Suitable for patients who are hemodynamically
stable and asymptomatic
Requires serial βHCG measurements and
ultrasonography
MEDICAL MANAGEMENT BY METHOTREXATE
METHOTREXATE
Folic acid antagonist that inhibits DNA synthesis in the
trophoblastic cells
Standard dose is 50mg/m2
Can be administered as a single I/M injection or multiple
fixed dose regimen.
INDICAITONS
Cornual pregnancy
Persistent trophoblastic disease
Patient with one fallopian tube and fertility desired
Patient who refuses surgery
Ectopic pregnancy where trophoblast is adherent to
bowel or blood vessel
GS is <4cm
CONTRAINDICATIONS
Chronic liver, renal or hematological disorder
Active infection
Immunodeficiency
Breastfeeding
SIDE EFFECTS
Nausea, vomiting
Stomatitis, conjunctivitis
GI upset
Photosensitive skin reactions
Non specific abdominal pain
SPECIAL ADVICE PRIOR TO USE
Avoid sexual intercourse during treatment
Take contraception for 3months after treatment
Avoid alcohol and sunlight exposure during
treatment
SURGICAL MANAGEMENT
INDICATIONS FOR SURGEICAL MANAGEMENT
Patient is not suitable for medical therapy
Medical therapy has failed
Patient has heterotropic pregnancy with viable
uterine pregnancy
Heamodynamically unstable and needs immediate
treatment
GS is >4cm
METHODS OF SURGERY
1. LAPROSCOPY- surgery through small incision,
having many advantages, like. less blood loss, shorter
hospital stay, less analgesia requirement, shorter
convalescence than laprotomy.
2. LAPROTOMY- surgery through large incision
especially reserved for severely compromised patient or
due lack of endoscopic facilities.
PROCEDURE OF SURGERY
1. SALPINGECTOMY
During surgery the fallopian tubes are removed
Done in patients:
• Who have tubal rupture
• Who no longer desire fertility
• Who have history of ectopic pregnancy in the same tube before
• Who have severely damaged tubes

PROCEDURE OF SURGERY
2. SALPINGOTOMY
During surgery, a small opening can be made at the site of ectopic
pregnancy and the trophoblastic tissue is extracted out via that
opening
Done when the tube has not ruptured or patient desires to
conserve her fertility
Monitoring needed for BHCG levels to identify persistent
trophoblast
High risk of subsequent ectopic pregnancy
PROGNOSIS AFTER MANAGEMENT
Rate of IU pregnancy may be higher following
treatment with methoteraxate as compared to
surgery
Rate of fertility may be better following
salpingotomy as compared to salpingectomy