I. Introduction
This case study tackles about the disease, diabetes mellitus type II. I have chosen this case since this is one of the most common diseases nowadays and many people from different age groups will be benefited with this case study. Before scanning through other pages, let me first give you a brief overview of what Diabetes Mellitus is. I have specifically focused on Type II Diabetes Mellitus since this is the case of my patient.
Diabetes mellitus is a common disease in which the body cannot use sugar normally. The body of a diabetic person is slow in using glucose (sugar), and so glucose builds up in the blood. The kidneys discharge some of the excess glucose into the urine. In severe cases of diabetes, fats and proteins also cannot be used normally.
Most physicians once believed that all cases of diabetes were caused by a lack of the hormone insulin. Insulin, which is produced by the pancreas, enables the body to use and store glucose quickly. Some diabetics do lack insulin. This form of the disease is called Type I diabetes (also known as insulin-dependent diabetes or juvenile-type diabetes). However, many diabetics--especially those who become diabetic after the age of 40--have normal or even above-normal production of insulin. Their bodies do not respond efficiently to the insulin. Doctors call this form of the disease Type II diabetes (also known as non-insulin-dependent diabetes or adult-type diabetes).
Symptoms of Diabetes include excessive urination, great thirst, hunger, and loss of weight and strength. These symptoms may appear gradually--and even be unnoticed--in Type II diabetes, which is most common in overweight individuals over the age of 40. Many cases of Type II diabetes can be controlled by a diet that is low in calories. Some Type II diabetics whose condition cannot be controlled by diet alone use insulin or take oral drugs that reduce the level of glucose in the blood.
Diabetes can lead to serious complications. For example, it may cause changes in the blood vessels of the retina. This condition is called diabetic retinopathy. In advanced form, it is a major cause of blindness. Diabetes may cause similar changes in the blood vessels of the kidneys. This condition, called diabetic nephropathy, may lead to kidney failure. The nerves may also be affected by diabetes. This complication, known as diabetic neuropathy, can result in loss of feeling or abnormal sensations in different parts of the body. Various treatments can control many cases of diabetic retinopathy, diabetic nephropathy, and diabetic neuropathy. Diabetes can also lead to atherosclerosis, a form of arteriosclerosis (hardening of the arteries) that may cause a stroke, heart failure, or gangrene.
Since you already have an idea of what diabetes mellitus is, I hope you’ll be encouraged to continue reading this case study and be able to implement as well as impart what you have learned in order to lessen or if possible, eradicate the occurrence of disease.
1
II. Objectives
General Objectives
After 2 days of giving holistic nursing care to the patient who have
Diabetes Mellitus type II, the nurse will be able to gain adequate knowledge, attitude and
skills in taking care of a patient who is suffering from this disease condition.
Specific Objectives
After 8 hours of giving holistic nursing care, the student nurse will be able
to:
1. relate the patients history and level of growth and development
2. explain the significance of the diagnostic results
3. review the anatomy and physiology of the pancreas relating it with insulin
4. explain the disease process and organ involved
5. compare the chart in classical and clinical symptoms of the disease
process
6. formulated appropriate nursing care plan based on identified problem of
patient
7. impart health teachings to the patient and significant others on Diabetes
Mellitus
2

After 8 hours of giving holistic nursing care, the patient and significant
others will be able to:
1. gain trust with the nurse
2. verbalize physiologic manifestation as a result of the disease
3. explain the disease process in their own level of understanding
4. relate health history with his present condition.
5. enumerate the different signs and symptoms that needs to be watched for.
6. identify factors that could aggravate his condition.
7. show willingness in the implementation of planned nursing care
8. state some health promotion activities of diabetes mellitus type II.
3
III. Nursing Assessment
1. Personal History
1.1Patient’s Profile
Name: Mrs. Soria, Fe F.
Age: 67 years Old
Sex: Female
Civil Status: Married
Religion: Roman Catholic
Date of Admission: January 23, 2006
Room number: 233
Complaints: Frequent Urination, High Blood Sugar and a Lump on her Right
Breast
Impression/Diagnosis: Type II Diabetes Mellitus
Physician: Dr. Armando Tan
Hospital Number: 187908
1.2 Family and Individual Information, Social and Health History
A case of Mrs. Fe F. Soria, 67 year old, female, Filipino and a Roman
Catholic. She is retired government employee from Bacolod City was admitted at
Chong Hua Hospital for the first time.
Three months prior to admission patient suffered Polyuria and Polydipsia
until it progressed into nausea, feeling nervous or jittery; cold, clammy, wet skin;
excessive sweating not caused by exercise, tachycardia, tingling sensation of the
fingertips lips thus patient was hospitalized. Laboratory works done and was
diagnosed with Type II Diabetes Mellitus.
Also one month prior to admission, patient noted 2 cm firm, movable,
circular non tender mass at left upper outer part of her left breast while taking a
bath. Mammography confirmed the mass and biopsy was done. It revealed
calcification at right breast category IV and MRM was advised. She is scheduled
for MRM.
4

1.3 Level of Growth and Development
1.3.1 Normal Development of an Older Adult (65 and above)
Physical
Integumentary System
The skin losses resilience and moisture. The epithelial layer thins, and
elastic collagen fibers shrink and become rigid. Wrinkles of the face and neck
reflect lifelong patterns of muscle activity and facial expressions, the pull of
gravity on tissue and diminished elasticity. Skin has spotty pigmentation in
areas exposed to the sun. It is also dry and scaly. There is also decreased fat
distribution on extremities and increase amount on abdomen. There is also
thinning and graying on scalp; often, decreased amount of axillary and pubic
hair and hair in extremities; decreased facial hair in men; possible chin and
upper lip hair in women
Head and Neck
Head is sharp and angular nasal and facial bones; loss of eyebrow hair in
women. Eyes are having decreased visual acuity; decreased accommodation;
reduced adaptation to darkness; and sensitivity to glare. Ears are having
decreased pitch discrimination; diminished light reflex; decreased sense of
smell; mouth and pharynx may use dentures; decreased sense of taste; atrophy
of papillae of lateral edges of tongue. Neck may have nodular thyroid gland;
slight tracheal deviation resulting from muscle atrophy.
5
Thorax and Lungs
There is significant increase in systolic pressure with slight increase in
diastolic pressure; usually insignificant changes in heart rate at rest; common
diastolic murmurs; easily palpated peripheral pulses; weakened pedal pulses
and colder lower extremities, especially at night.
Breast
Decreased muscle mass, tone, and elasticity result in smaller breast in
older women. In addition, the breast sag. Atrophy of the glandular tissue,
coupled with more fat deposits, results in a slightly smaller, less dense, and
less nodular breast. Gynecomastia, enlarged breast in men, may be due to
medication side effects, hormonal changes, or obesity. Both men and women
are at risk of breast cancer development.
Gastrointestinal System
Decreased salivary secretions, which may make swallowing more
difficult; decreased peristalsis; decreased production of digestive enzymes,
including hydrochloric acid, pepsin, and pancreatic enzymes; constipation;
reduced motility.
Reproductive System
Changes in the structure and function of the reproductive system occur as
the result of hormonal alterations. Female menopause is related to a reduced
responsiveness of the ovaries to pituitary hormones and a resultant decrease in
estrogen and progesterone levels. In men, there is no definite cessation of
fertility associated with aging. Spermatogenesis begins to decline during the
fourth decade but continues into the ninth. The change in reproductive
6
structure and function, however do not affect libido. Less frequent sexual
activity can result from illness, death of a sexual partner, decreased
socialization, or loss of sexual interest.
Urinary System
Decreased renal filtration and renal efficiency; subsequent loss of protein
from kidney; nocturia; decreased bladder capacity; increased incontinence.
Female
Urgency and stress incontinence resulting from decrease in perineal
muscle tone.
Male
Urinary frequency and retention resulting from prostatic enlargement.
Musculoskeletal System
Decreased muscle mass and strength; bone demineralization; shortening of
trunk as result of intervetebral space narrowing; decreased joint mobility;
decreased range of joint motion; enhanced bony prominences.
Neurological System
Decreased rate of voluntary or automatic reflexes, decreased ability to
respond to multiple stimuli; insomnia; shorter sleeping periods.
7
Psychosocial Development
According to Erik Erikson, the developmental task at this time is Ego
Integrity vs. Despair. People who attain ego integrity view in life with a
sense of wholeness and derive satisfaction from past accomplishments.
They view death as an acceptable completion of life. According to
Erikson, people who develop integrity accept “one’s one and only life
cycle.” By contrast, people who despair often believe they have made
poor choices during life and wish they could live life over.
Cognitive Development
Piaget’s phases of cognitive development end with Formal Operations
Phase. Changes in cognitive structures occur as a person ages. It is
believed that there is progressive loss of neurons. In addition, blood flow
to the brain decrease, the meninges appear to thicken, and brain
metabolism slows. Older people need additional time for learning,
largely because of the problem of retrieving information.
Moral Development
According to Kohlberg, moral development is completed in the early
adult years. Most old people stay at Kohlberg’s conventional level of
moral development and some are at the preconventional level. An
elderly at the preconvetional level obeys rules to avoid pain and the
displeasure of others. Elderly people at the conventional level follow
society’s rules of conduct in response to the expectation of others.
8
Spiritual Development
According to Fowler and Keen, some people enter the sixth stage of
spiritual development, Universalizing. People whose spiritual
development reaches their level thinking and act in a way that
exemplifies love and justice.
Sexual Development
Sex drives persist into 70’s, 80’s, and 90’s, provided that health is good
and an interested partner is available. Interest in sexual activity in old
age depends, in large measure, on interest earlier in life. However,
sexual activity does become less frequent. Many factors may play a role
in the ability of an elderly person to engage in sexual activity.
9
1.3.2 The Ill Person at a Particular Stage of Patient
The three most common causes of death in older adults are heart
disease, cancer and stroke. Other frequently reported causes of death are
lung disease, accidents/falls, diabetes, kidney disease, and liver disease.
Heart disease is the leading cause of death in older adults. Common
cardiovascular disorders are hypertension and coronary artery disease.
Cancer or malignant neoplasm’s are the second most common cause of
death among older adults. Cerebrovascular accidents, the third leading
cause of death, occurring as brain ischemia or brain hemorrhage.
Cigarette smoking has been recognized as a risk factor in the four most
common cause of death for older adults: heart disease, cancer, stroke and
lung disease. Dental carries, gingivitis, broken or missing teeth and ill-
fitting or missing dentures may affect nutritional adequacy, cause pain,
and lead to infection.
Older adults should be encouraged to maintain physical exercise
and activity. The primary benefits of exercise include maintaining the
strengthening functional ability and promoting a sense of enhanced well-
being. Arthritis is also a common condition in older adults, especially in
women. The degree to which the mobility of older adults is impaired
depends on the extent of the disease and joint affected. Falls are a safety
concern of many older adults, falls my lead to fear of additional falls,
withdrawal from usual activities and loss of independence.
10
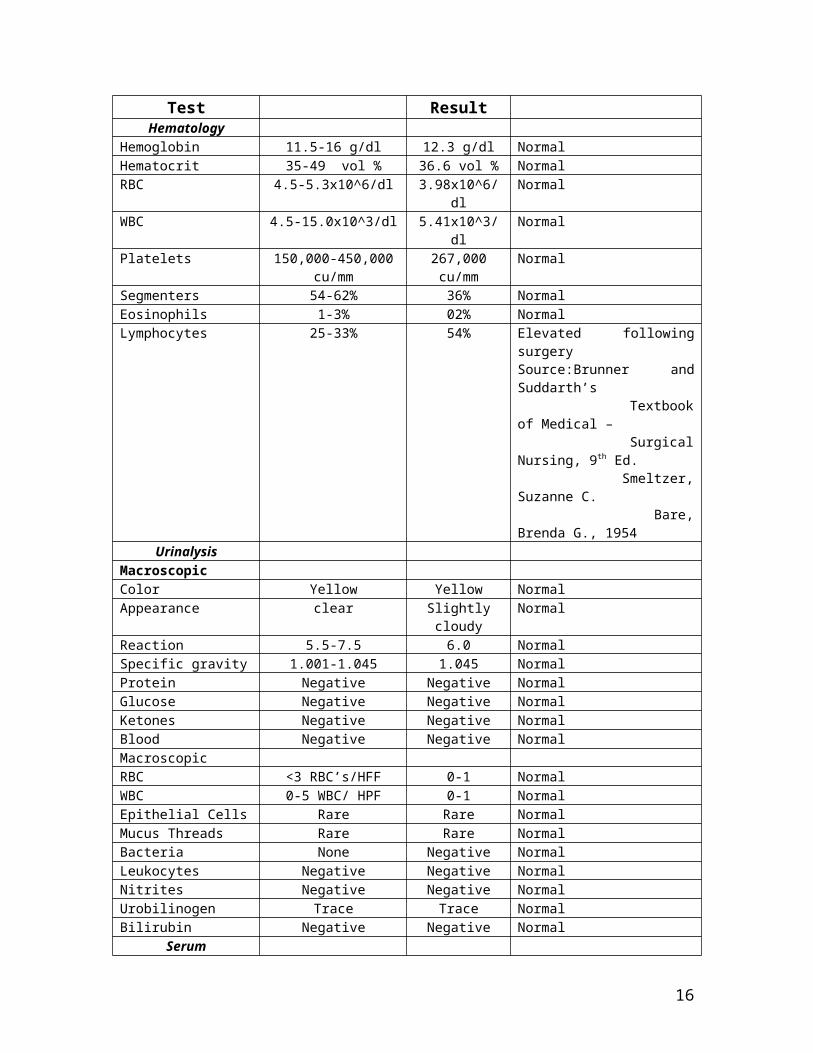
2. Diagnostic Results
Diagnostic Test Normal Values Patient’s Result
Significance
HematologyHemoglobin 11.5-16 g/dl 12.3 g/dl NormalHematocrit 35-49 vol % 36.6 vol % NormalRBC 4.5-5.3x10^6/dl 3.98x10^6/dl NormalWBC 4.5-15.0x10^3/dl 5.41x10^3/dl Normal
Platelets 150,000-450,000 cu/mm 267,000 cu/mm NormalSegmenters 54-62% 36% NormalEosinophils 1-3% 02% NormalLymphocytes 25-33% 54% Elevated following surgery
Source:Brunner and Suddarth’s Textbook of Medical – Surgical Nursing, 9th Ed. Smeltzer, Suzanne C. Bare, Brenda G., 1954
UrinalysisMacroscopicColor Yellow Yellow NormalAppearance clear Slightly cloudy NormalReaction 5.5-7.5 6.0 NormalSpecific gravity 1.001-1.045 1.045 Normal Protein Negative Negative NormalGlucose Negative Negative NormalKetones Negative Negative NormalBlood Negative Negative NormalMacroscopicRBC <3 RBC’s/HFF 0-1 NormalWBC 0-5 WBC/ HPF 0-1 NormalEpithelial Cells Rare Rare NormalMucus Threads Rare Rare NormalBacteria None Negative NormalLeukocytes Negative Negative NormalNitrites Negative Negative NormalUrobilinogen Trace Trace NormalBilirubin Negative Negative Normal
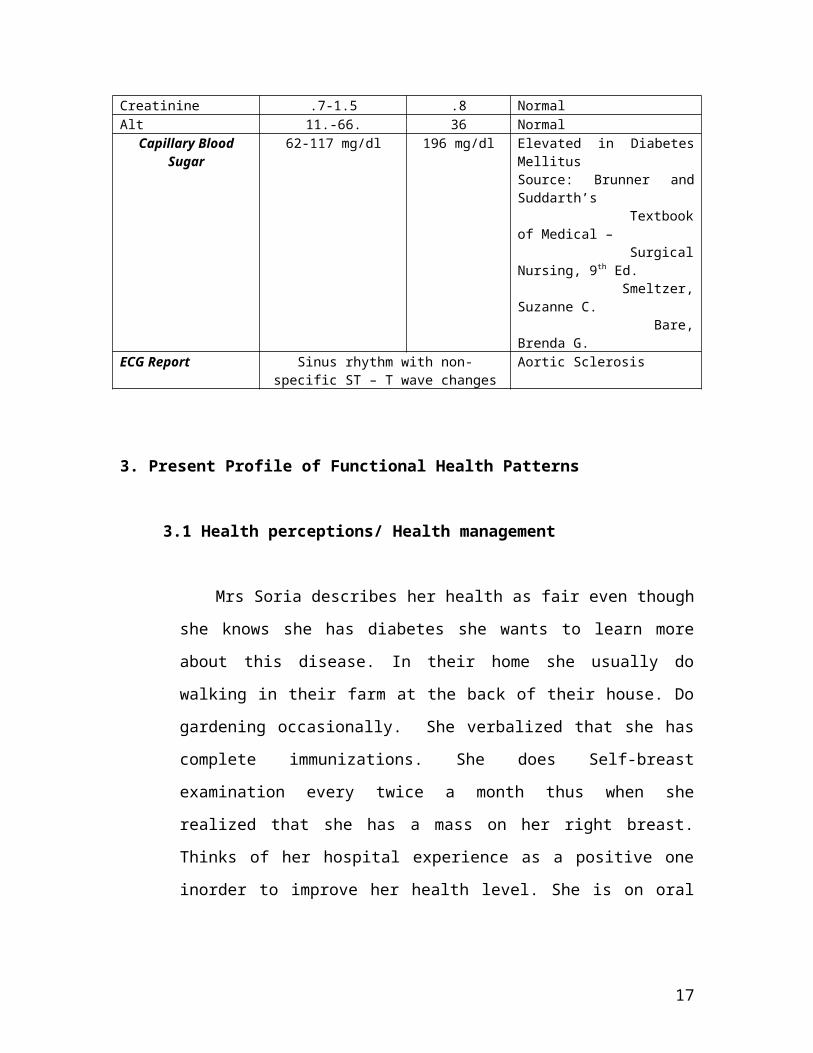
SerumCreatinine .7-1.5 .8 NormalAlt 11.-66. 36 NormalCapillary Blood Sugar 62-117 mg/dl 196 mg/dl Elevated in Diabetes Mellitus
Source: Brunner and Suddarth’s Textbook of Medical – Surgical Nursing, 9th Ed. Smeltzer, Suzanne C. Bare, Brenda G.
ECG Report Sinus rhythm with non-specific ST – T wave changes
Aortic Sclerosis
11
3. Present Profile of Functional Health Patterns
3.1 Health perceptions/ Health management
Mrs Soria describes her health as fair even though she knows she has
diabetes she wants to learn more about this disease. In their home she usually do
walking in their farm at the back of their house. Do gardening occasionally.
She verbalized that she has complete immunizations. She does Self-breast
examination every twice a month thus when she realized that she has a mass on
her right breast. Thinks of her hospital experience as a positive one inorder to
improve her health level. She is on oral hypoglycemic and on a diabetic diet but
she is usually tempted with sweets.
3.2 Nutritional/Metabolic pattern
Prior to admission, patient usually eats 3 meals a day with occasional
snacks in between meals. She has no allergies to foods. She eats almost
anything, but usually her diet is composed of fish and meat. She drinks more
than 8 glasses of water a day. She is taking glucophage as maintenance
medication. Currently, she is on a diabetic diet carefully balanced by the dietary
department to fit her daily caloric needs. Her diet now composed of 60%
carbohydrate, 30% protein, and 10% fat with less than 300 mg cholesterol a
day, no simple sugar and high fiber diet
3.3 Elimination Patterns
Mrs. Soria can void and defecate independently but she complains of this
occasional frequent urination and it makes her uncomfortable. She defecates
about once a day with formed stools without and mucus or blood but sometimes
defecates with slightly loose stools.
12
3.4 Activity/ Exercise Pattern
The patient verbalized that after her retirement her daily activities are
gardening and early in the morning walking around at the farm at the back of
her house. She can independently ambulate with perfect balance, bathe, dress,
groom, and perform general hygiene by herself. But she complains of easily
getting tired, sometimes she loses drive in performing activities, getting
disinterested and sometimes becomes irritable.
3.5 Cognitive/Perceptual Pattern
She uses reading glasses as her vision is not to good because of advancing
age. She doesn’t have any complaints regarding occurrence or vertigo and
insensitivity to cold/ heat/pain. As she is a college level graduate, she can
perfectly read and legibly write.
3.6 Rest/ Sleep Pattern
She usually sleeps at around 10 pm and wakes up at around 6 am. She
sleeps for about 8 hours. She doesn’t use any medication to induce sleep but she
sometimes take snacks before sleeping. She verbalized that she usually takes a
bath before sleeping. She does not have problems sleeping.
3.7 Self- Perception Pattern
She is concern about her diagnosis on whether it could have a huge impact
on her life. Her present health goal is to keep on visiting her doctor for her
disease condition. She describes herself doing fine. Having this disease make
her a stronger person as verbalized and will seek treatments in order to manage
her condition.
13
3.8 Roles- Relationship Pattern
Mrs. Soria speaks fluent English and Bisaya. Her speech is very coherent
and clear. She usually expresses herself by speaking and sometimes making
gestures, forming faces to express her emotions.
She lives with her husband in their farm, who she been married for quite
sometime now, and she verbalized than when theirs a need for help she turn to
her husband or call her daughter who is working abroad.
3.10 Coping- Stress Management Pattern
She makes decisions together with her husband. When in stress she
usually gets some sleep and rest and hope that waking up will calm things
down.
3.11 Values- Belief System
She finds her source of strength to God and her Family who is always with
her. She is a devout Roman Catholic and a very active church goer. She
verbalized that religion is very important to her for spiritual growth
14

4. Pathophysiology and Rationale
4.1 Normal Anatomy and Physiology of Organ System Affected
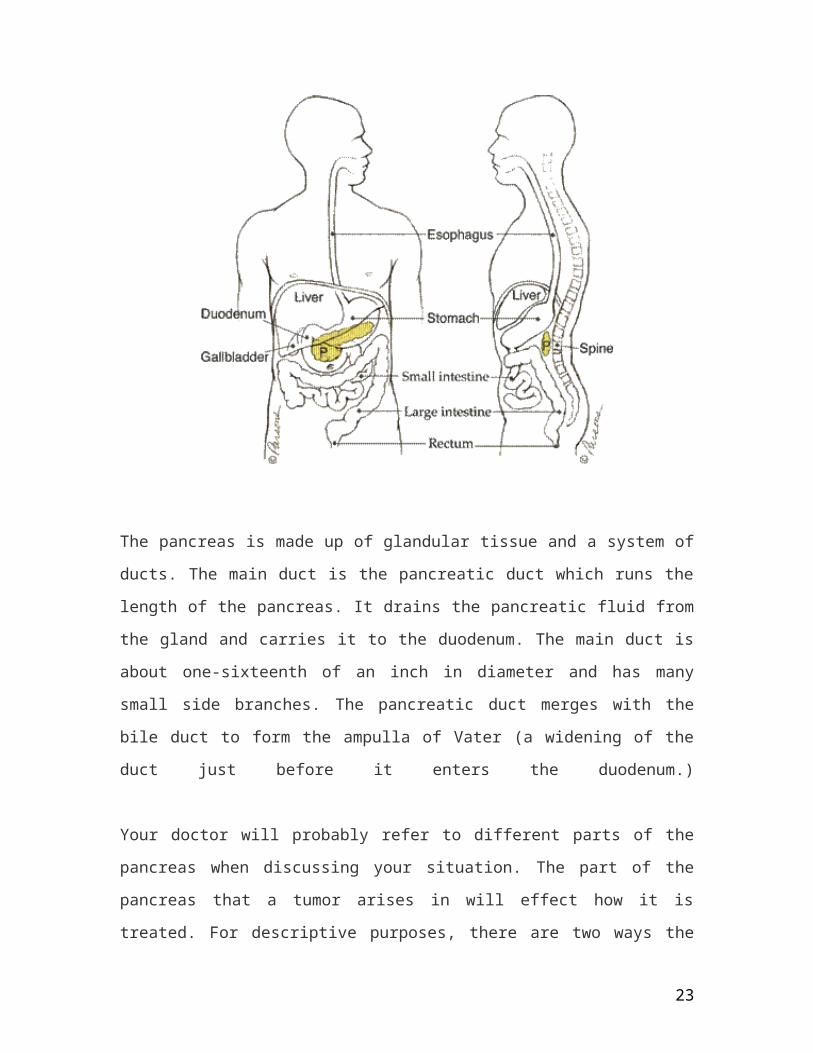
The pancreas is located deep in the abdomen, sandwiched between the stomach and the
spine. It lies partially behind the stomach. The other part is nestled in the curve of the
duodenum (small intestine). To visualize the position of the pancreas, try this: Touch the
thumb and "pinkie" finger of your right hand together, keeping the other three fingers
together and straight. Then, place your hand in the center of your belly just below your
lower ribs with your fingers pointing to the left. Your hand will be at the approximate
level of your pancreas.
Because of the pancreas' deep location, tumors are rarely palpable (able to be felt by
pressing on the abdomen.) It also explains why many symptoms of pancreatic cancer
often do not appear until the tumor grows large enough to interfere with the function of
nearby structures such as the stomach, duodenum, liver, or gallbladder.
15
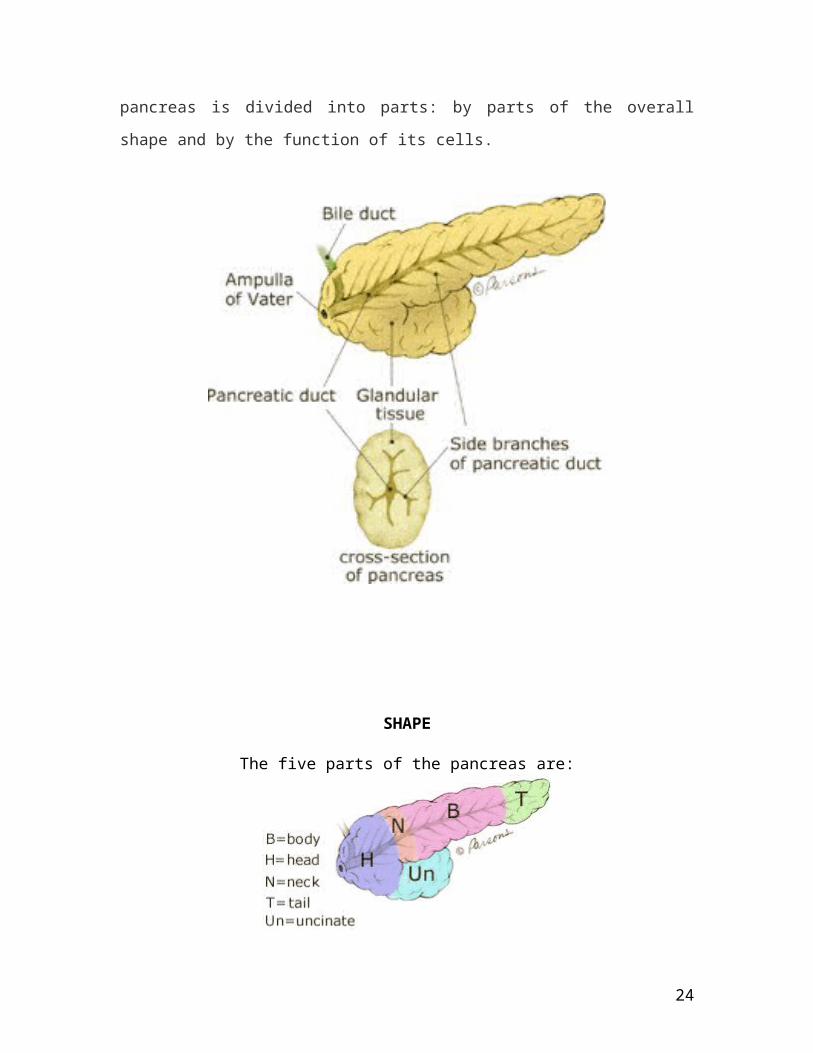
The pancreas is made up of glandular tissue and a system of ducts. The main duct is the
pancreatic duct which runs the length of the pancreas. It drains the pancreatic fluid from
the gland and carries it to the duodenum. The main duct is about one-sixteenth of an inch
in diameter and has many small side branches. The pancreatic duct merges with the bile
duct to form the ampulla of Vater (a widening of the duct just before it enters the
duodenum.)
Your doctor will probably refer to different parts of the pancreas when discussing your
situation. The part of the pancreas that a tumor arises in will effect how it is treated. For
descriptive purposes, there are two ways the pancreas is divided into parts: by parts of the
overall shape and by the function of its cells.
16
SHAPE
The five parts of the pancreas are:
uncinate process
The part of the gland that bends backwards and underneath the body of the
pancreas. Two very important blood vessels, the superior mesenteric artery and vein
cross in front of the uncinate process.
head
The widest part of the gland. It is found in the right part of abdomen, nestled in
the curve of the duodenum which forms an impression in the side of the gland.
neck
The thin section between the head and the body of the gland
body
The middle part of gland between the neck and the tail. The superior mesenteric
blood vessels run behind this part of the gland.
tail
The thin tip of gland in the left part of abdomen in close proximity with the spleen
FUNCTION
The pancreas can also be thought of as having different functional components, the
endocrine and exocrine parts. Tumors can arise in either part. However, the vast majority
arise in the exocrine (also called non-endocrine) part. Since the parts have different
normal functions, when tumors interfere with these functions, different kinds of
symptoms will occur.
17
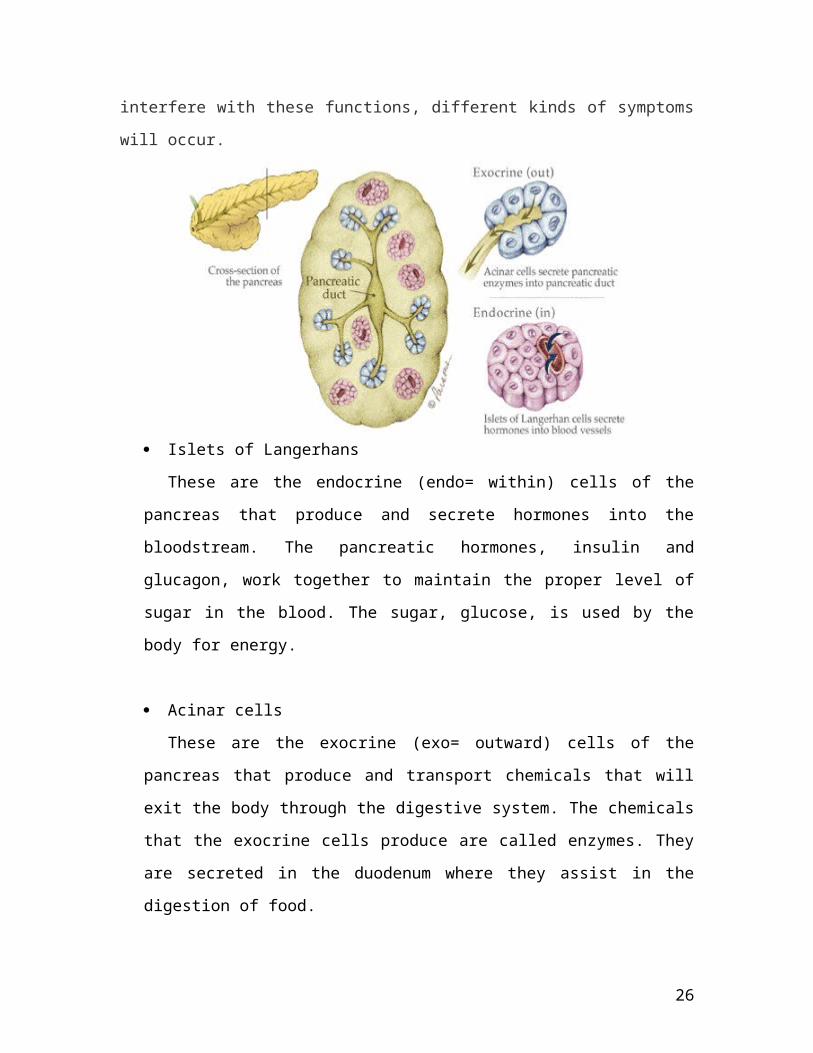
Islets of Langerhans
These are the endocrine (endo= within) cells of the pancreas that produce and
secrete hormones into the bloodstream. The pancreatic hormones, insulin and
glucagon, work together to maintain the proper level of sugar in the blood. The sugar,
glucose, is used by the body for energy.
Acinar cells
These are the exocrine (exo= outward) cells of the pancreas that produce and
transport chemicals that will exit the body through the digestive system. The
chemicals that the exocrine cells produce are called enzymes. They are secreted in the
duodenum where they assist in the digestion of food.
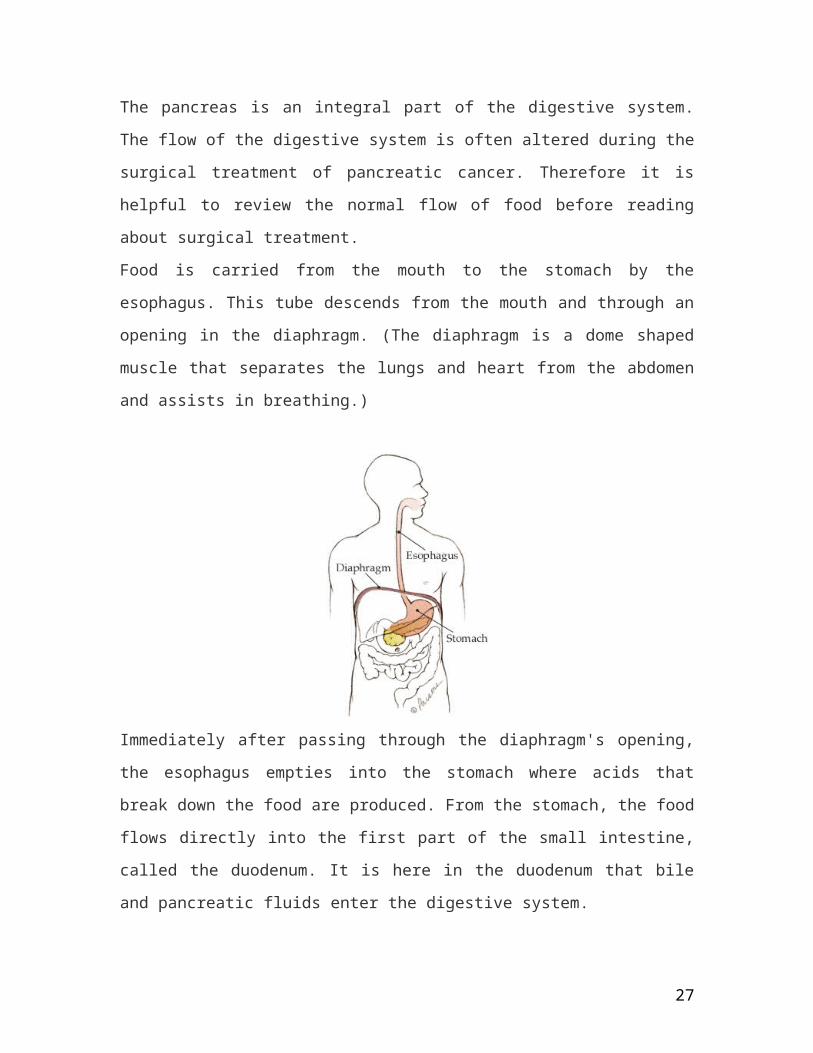
The pancreas is an integral part of the digestive system. The flow of the digestive system
is often altered during the surgical treatment of pancreatic cancer. Therefore it is helpful
to review the normal flow of food before reading about surgical treatment.
Food is carried from the mouth to the stomach by the esophagus. This tube descends from
the mouth and through an opening in the diaphragm. (The diaphragm is a dome shaped
muscle that separates the lungs and heart from the abdomen and assists in breathing.)
18
Immediately after passing through the diaphragm's opening, the esophagus empties into
the stomach where acids that break down the food are produced. From the stomach, the
food flows directly into the first part of the small intestine, called the duodenum. It is here
in the duodenum that bile and pancreatic fluids enter the digestive system.
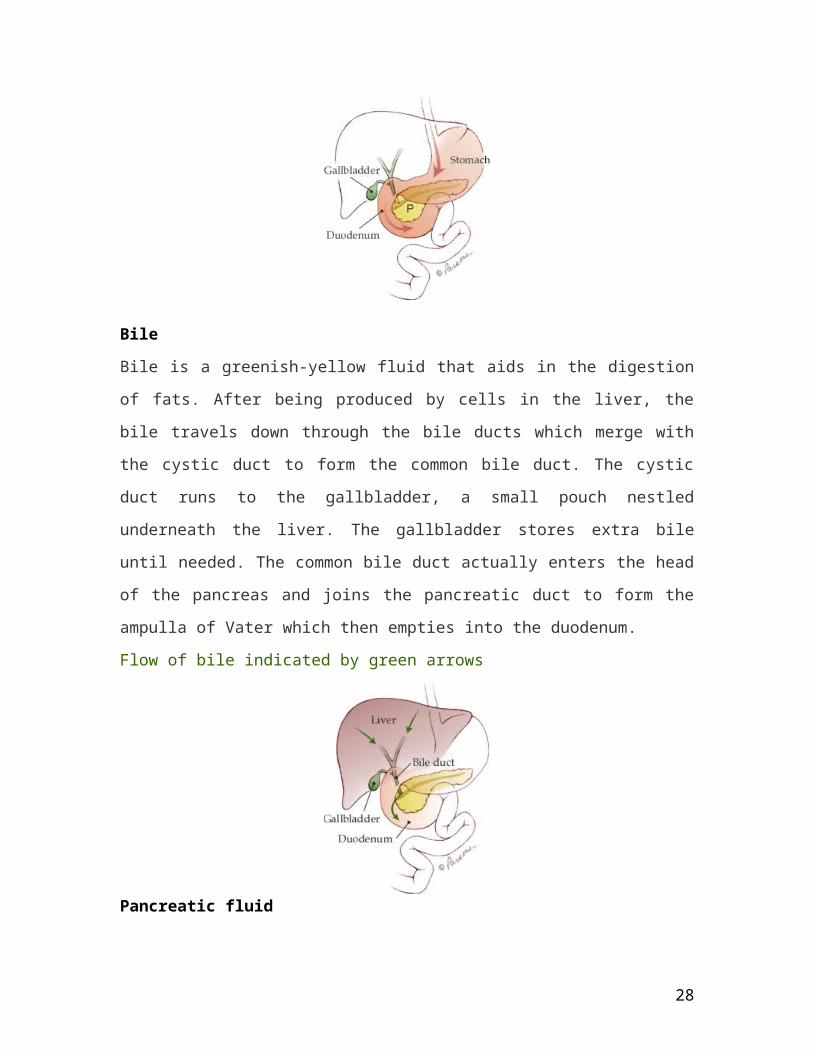
Bile
Bile is a greenish-yellow fluid that aids in the digestion of fats. After being produced by
cells in the liver, the bile travels down through the bile ducts which merge with the cystic
duct to form the common bile duct. The cystic duct runs to the gallbladder, a small pouch
nestled underneath the liver. The gallbladder stores extra bile until needed. The common
bile duct actually enters the head of the pancreas and joins the pancreatic duct to form the
ampulla of Vater which then empties into the duodenum.
Flow of bile indicated by green arrows
19
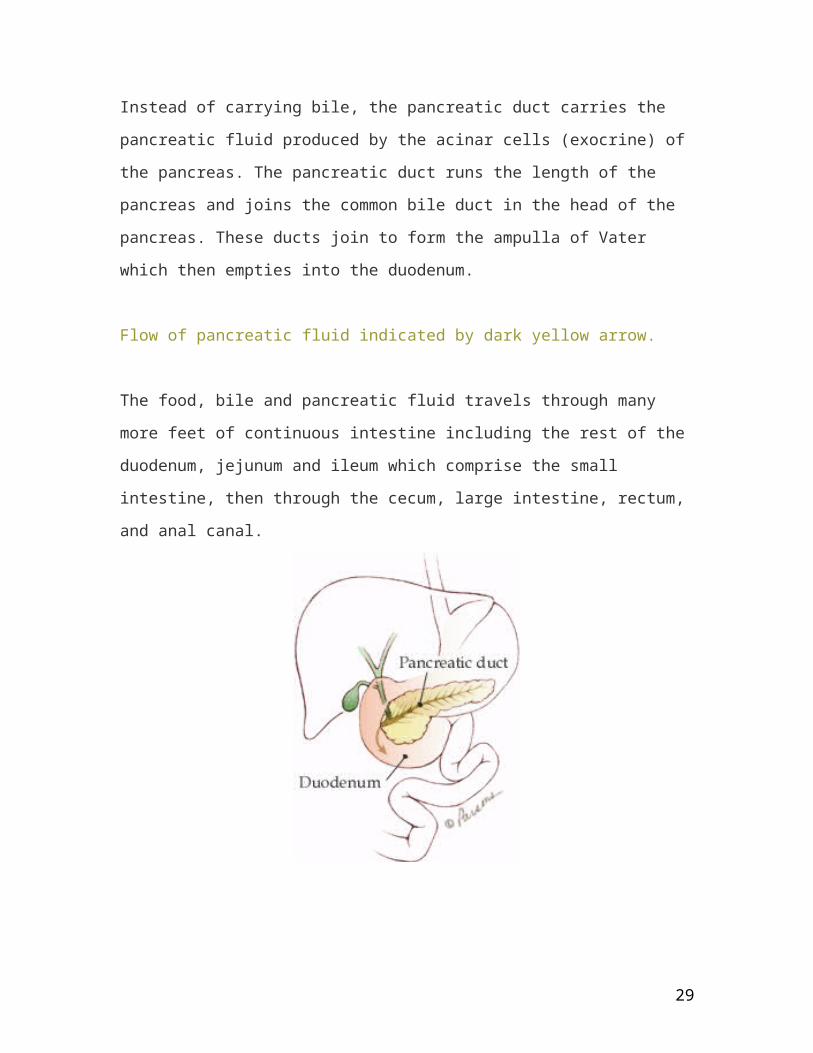
Pancreatic fluid
Instead of carrying bile, the pancreatic duct carries the pancreatic fluid produced by the
acinar cells (exocrine) of the pancreas. The pancreatic duct runs the length of the
pancreas and joins the common bile duct in the head of the pancreas. These ducts join to
form the ampulla of Vater which then empties into the duodenum.
Flow of pancreatic fluid indicated by dark yellow arrow.
The food, bile and pancreatic fluid travels through many more feet of continuous intestine
including the rest of the duodenum, jejunum and ileum which comprise the small
intestine, then through the cecum, large intestine, rectum, and anal canal.
20
21
4.3 Disease process and Effects on Different Organ System
Genetic factors, usually polygenic, form disease background in a prevailing number of patients. Environmental factors like obesity, lack of exercise and sedentary lifestyle sometimes lead to insulin resistance. Insulin resistance means that body cells do not respond appropriately when insulin is present.
Other important contributing factors:
increased hepatic glucose production (eg, from protein degradation) decreased insulin-mediated glucose transport in muscle and adipose tissues
(receptor and post-receptor defects) impaired beta-cell function - loss of early phase of insulin release in response to
hyperglycemic stimuli
This is a more complex problem than type 1, but is sometimes easier to treat especially in the initial years, when insulin is often still produced. Type 2 may go unnoticed for years in a patient before diagnosis, since the symptoms are typically milder (no ketoacidosis) and can be sporadic. However, severe complications can result from unnoticed type 2 diabetes, including renal failure, blindness, wounds that fail to heal, and coronary artery disease. The onset of the disease is most common in middle age and later life.
Diabetes mellitus type 2 is presently of unknown etiology or cause. Diabetes mellitus that has a known etiology, such as secondary to other diseases, known gene defects, or effects of drugs, is more appropriately called secondary diabetes mellitus. Examples include diabetes mellitus caused by hemochromatosis, pancreatic insufficiency, or certain types of medications (e.g. long-term steroid use).
About 90-95% of all North American cases of diabetes are type 2, and about 20% of the population over the age of 65 has diabetes mellitus type 2. The fraction of type 2 diabetics in other parts of the world varies substantially, almost certainly for environmental and lifestyle reasons. There is also a strong inheritable genetic connection in type 2 diabetes: having relatives (especially first degree) with type 2 is a considerable risk factor for developing type 2 diabetes. The majority of patients with type 2 diabetes mellitus are obese - chronic obesity leads to increased insulin resistance that can develop into diabetes, most likely because adipose tissue is a (recently identified) source of chemical signals (hormones and cytokines). Other research shows that type 2 diabetes causes obesity.1
Diabetes mellitus type 2 is often associated with obesity and hypertension and elevated cholesterol (combined hyperlipidemia), and with the condition Metabolic syndrome (also known as Syndrome X). It is also associated with acromegaly, Cushing's syndrome and a number of other endocrinological disorders
22
4.4 Comparative Chart
Classical Symptom Clinical Symptom Rationale
Polyuria
Polydipsia
Blurred Vision
Manifested- Patient verbalized frequent urinations a day
Manifested- Patient also verbalized episodes of thirst when ever her blood sugar is high
Not Manifested
Glucose attracts water, and an osmotic diuresis occurs, resulting in polyuria.Source: Medical – Surgical Nursing, Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition, p. 934
The loss of water and results in thirst and increases fluid intake. Losses of electrolytes such as potassium, magnesium, and phosphorus occur with the osmotic diuretic effect of glucosuria.Source: Medical – Surgical Nursing, Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition, p. 934
Changes in the retinal capillaries cause decreased blood flow to the retina, leading to retinal ischemia and possible retinal hemorrhage or detachment.Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p.382
23
Recurrent Infection
Paresthesias
Not Manifested
Not Manifested
Glucose accumulates in the epidermal layer of the skin. Moisture tends to collect under the armpits, breasts, groin, or genitalia. The higher the normal concentration of glucose in the skin coupled with moisture creates a perfect breeding area for microorganisms. Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p.382-383
Diabetic peripheral neupathies are bilateral sensory disorders. The manifestations appear first in the toes and feet and then eventually progress upward to involve the fingers and hands.Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p.382
24
IV. Nursing Interventions
Care Guide of Patient with Disease Condition
The nurse reinforces teaching and skills for clients with DM. The content of a teaching
plan includes the following points:
Information about normal glucose metabolism and how diabetes changes
metabolism
Dietary plan: How diet helps keep blood glucose in normal range; number pf kcal
required and why; why they should eat complex carbohydrate and foods high in
fiber but limit the intake of sugar, fat, sodium, and alcohol; concerns regarding
meal preparation; how to read food label for sugar, fat, and protein; integrating
personal food preferences; eating meals away from home; relationships between
diet, exercise, and medication. Fluid intake should be encountered, because the
thirst mechanism may be impaired.
Exercise: How it helps lower blood glucose; the importance of regular exercise
program; types of exercise; and integrating personal exercise choices
Glucose levels: Self-monitoring of blood glucose; how to perform the test
accurately; how to care for equipment; what to do for high or low blood glucose.
Medications:
o Insulin type, dosage, mixing instructions (if necessary); times of onset
and peak actions; how to get and care for equipment; how to give
injections; timing of insulin injections and mealtimes
o Oral agents: Type, dosage, side effects, interaction with other drugs
Complications:
o Factors that cause diabetic ketoacidosis or HHNS;
o Manifestations of each; what to do when they occur.
o Factors that cause hypoglycemia; manifestations; what to do when they occur
25
Safety precautions: Identify family to contract in an emergency; carrying ID card
and tag; carrying rapid-acting glucose; carrying insulin and glucagons kit
Hygiene: Skin, dental, foot care
Vision: Yearly exam, sources for vision aids such as magnifying sleeve for
insulin syringe or large-print instructions
Sick days: What to do about food, fluids, and medications
Communication and Follow-up:
o What signs and symptoms to report; whom to contact; when to report
o Importance of keeping follow-up appointments
26
2. Actual Patient Care
2.1.1 Nursing Assessment
Name of Patient: Mrs. Fe F. Soria
Impression/Diagnosis: Type II Diabetes Mellitus
Attending Physician: Dr. Armando Tan
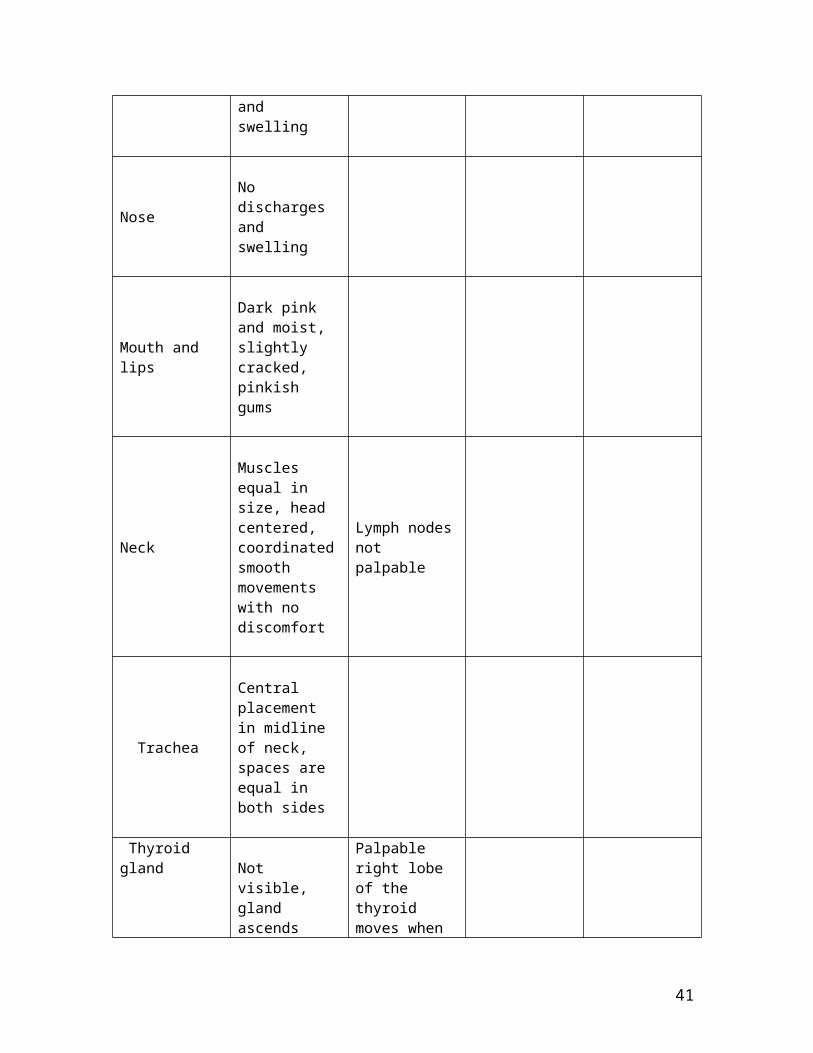
Body Part I P P A
Head
Rounded, (normocephalic) with frontal , parietal and occipital prominences/ smooth skull contour
Smooth, uniform in consistency, absence of nodules and masses.
Temporal pulse: 78 bpm
Face
Symmetrical facial features, palpebral fissures equal in size, symmetric nasolabial folds and symmetrical facial movements
Smooth, no deformities, absence of nodules or masses. No tenderness over lacrimal gland
Resonant sound found upon percussion
EyesEyebrows symmetrically aligned equal movement. Eyelashes equally distributed and curled slightly upward, skin intact, n discharges and no discoloration. Lids close symmetrically.
27
Sclera is white, palpebral conjunctiva is shiny, smooth and pink. Eyes are black with pupils equally round and reactive to light and accommodation
Ears
Auricle in line with the outer canthus of the eyes, absence of lesions, discharges and swelling
Nose No discharges and swelling
Mouth and lips
Dark pink and moist, slightly cracked, pinkish gums
Neck
Muscles equal in size, head centered, coordinated smooth movements with no discomfort
Lymph nodes not palpable
Trachea
Central placement in midline of neck, spaces are equal in both sides
Thyroid glandNot visible, gland ascends
Palpable right lobe of the thyroid moves
28
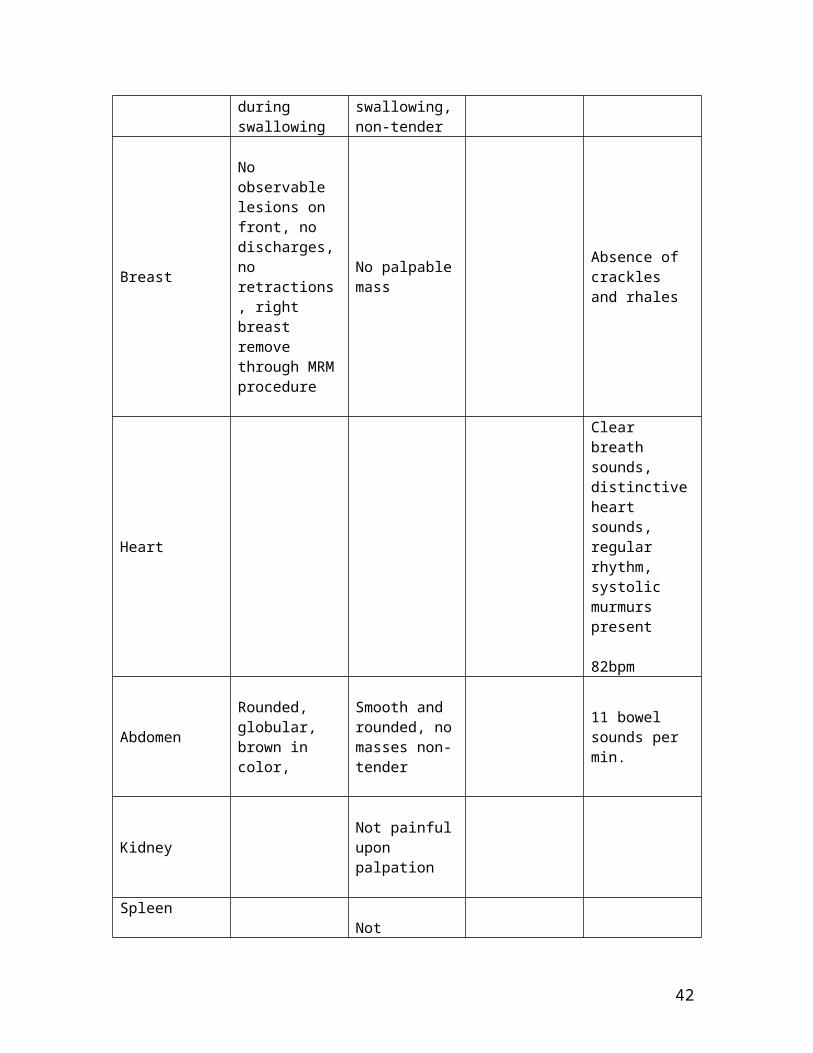
during swallowing
when swallowing, non-tender
Breast
No observable lesions on front, no discharges, no retractions, right breast remove through MRM procedure
No palpable mass
Absence of crackles and rhales
Heart
Clear breath sounds, distinctive heart sounds, regular rhythm, systolic murmurs present
82bpm
AbdomenRounded, globular, brown in color,
Smooth and rounded, no masses non-tender
11 bowel sounds per min.
Kidney Not painful upon palpation
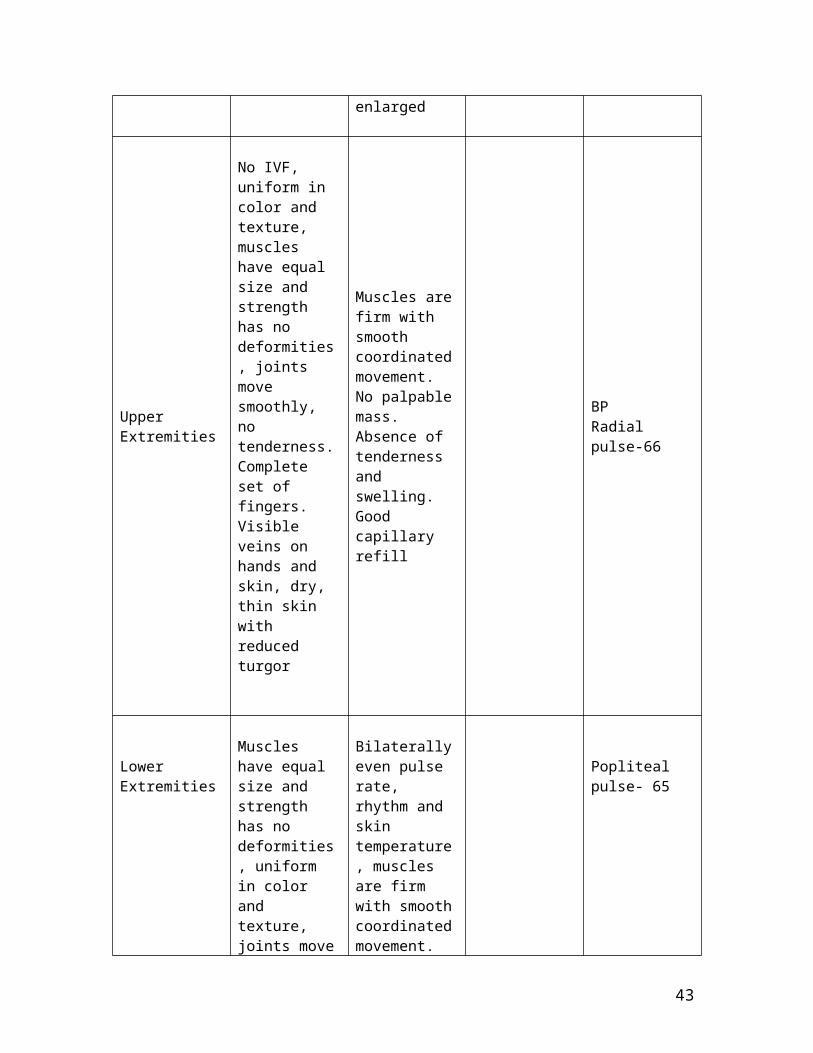
Spleen Not enlarged
Upper Extremities
No IVF, uniform in color and texture, muscles have equal size and strength has no deformities, joints move smoothly, no tenderness. Complete set of fingers. Visible veins on hands and skin, dry, thin skin with reduced turgor
Muscles are firm with smooth coordinated movement. No palpable mass. Absence of tenderness and swelling. Good capillary refill
BP Radial pulse-66
29

Lower Extremities
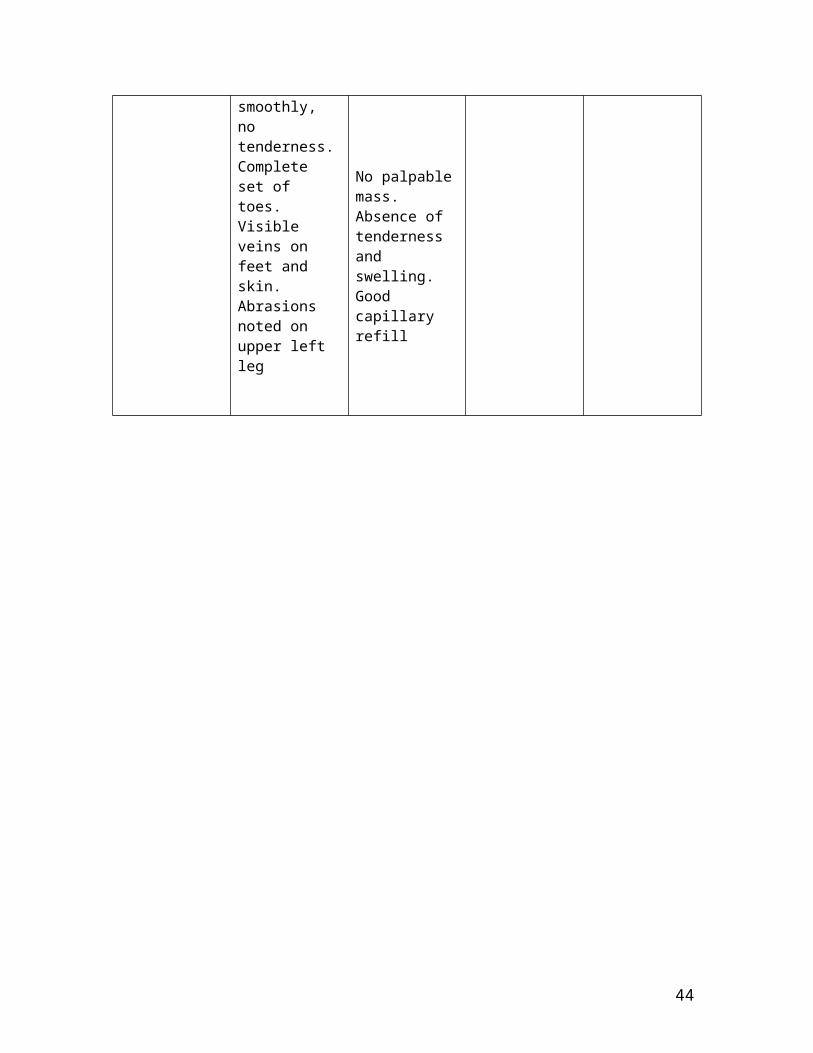
Muscles have equal size and strength has no deformities, uniform in color and texture, joints move smoothly, no tenderness. Complete set of toes. Visible veins on feet and skin. Abrasions noted on upper left leg
Bilaterally even pulse rate, rhythm and skin temperature, muscles are firm with smooth coordinated movement. No palpable mass. Absence of tenderness and swelling. Good capillary refill
Popliteal pulse- 65
30
2.1.2 Nursing Care Plan
Name of Patient: Mrs. Soria, Fe. F Age: 67 y. o.
Room/Ward: 233 Sex: female
Chief Complaints: Frequent urination, High Blood Sugar, and a Lump on her
Breast
Needs/ Problems/
Cues
Nursing Diagnosis
Scientific Basis
Objectives of Care
Nursing Intervention Rationale
I. physiologic
1. Altered Nutrition, More than Body Requirements: High Blood Sugar levels
- patient verbalized “ lami kayo ika.on sad ug mga tam.is”
- capillary blood sugar is elevated at about 196 mg/dl
- patients weight is above normal
Altered nutrition, more the body requirements: high blood sugar levels related to insufficient insulin production
The pancreas produces either normal or excessive amounts of insulin, but the body is unable to use it effectively, and glucose levels remain elevated. This defect is known as insulin resistance and is seen I type II DM. Fundamen
After 8 hours of holistic nursing care the patient will be able to verbalized optimal individual diet and health maintenance programs
Measures to:
- optimize health
1. monitor blood glucose levels regularly and report values below 60 mg/dl or above 200 mg/dl.
2. identify food preferences, including ethnic/cultural needs.
- clients with diabetes are at risk for hypoglycemia or hyperglycemiaSource: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition. p. 384
- clients are more likely to eat food they like and that meets their ethnic/ cultural requirements.Source: Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
31
- triceps skin fold is 30mm
tally, it is the failure of the pancreas to produce enough insulin to overcome this insulin resistance that precipitates clinical type II DM in predisposed individuals
Source: Medical Surgical Nursing Health and Illness PerspectivesPhipps, Wilma, et. al. 7th editionp. 930
3. encourage client to eat all of the prescribe diet
4. encourage patient to become involved in setting goals for dietary changes, documenting food intake, planning meals.
5. monitor percentage of meals and snaks that client eats.
- anorexia, gastric fullness, and abdominal pain can reduce oral intake. To prevent hypoglycemia, the client must consume the amount of food included in the diet plan.Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
- there is a greater probability that changes will be made when the patient is involved in planning those changes. Patients know their own likes and dislikes, financial resources and ability to make dietary changes. Participation allows the patient greater control over the situation.Source: : Medical Surgical Nursing Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition. p. 954
- monitoring of nutritional intake helps to determine the need for a dietary consult.Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
32

6. provide meals and snacks on time
7. include a high-fiber, high carbohydrate diet
8. teach or reinforce earlier teaching about the selected system of dietary management
9. teach client the sign and symptoms of hypoglycemia and how to treat it.
- glucose and insulin control is more effective when meals are eaten on time.Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
- it has been shown to decrease insulin requirements and cholesterol. It has been shown to increase satiety, which might help with weight reduction.Source: Medical Surgical Nursing Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition. p. 949
- knowledge increases the likelihood of compliance Source: Medical Surgical Nursing Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition. p. 955
- patient receiving oral hypoglycemic agents must be concerned about hypoglycemia ; they need to know how to identify and handle it.Source: Medical Surgical Nursing Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition. p. 955
- to prevent
33
2. Activity Intolerance: Fatigue
- patient verbalized “ kapoy man cge ako lawas”
- disinterest in surroundings
- decreased drive in performing activities
- sometimes irritable
Activity intolerance: fatigue related to poor utilization of glucose
Fatigue is a common symptom of diabetes and also related to increased age or anemia. Diabetes leads to loss of fat deposits under the skin, loss of glycogen, and catabolism of body proteins
Source: : Medical – SurgicalNursing Care Burke, Karen, LeMone, Priscilla ,
- state that fatigue is reduced and energy is returning to normal
10. give oral hypoglycemic agents as ordered
-measures to reduce fatigue
1. teach patient that improvement in metabolic control will decrease fatigue.
2. monitor severity of patients fatigue
3. encourage patient to prioritize daily
hyperglycemia, oral hypoglycemic agents must be given on time. Altered times might be necessary when food is delayed or diagnostic procedures are being done. Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
-understanding the relationship between metabolic abnormalities and fatigue increases the likelihood of compliance with the prescribed treatment regimen.Source: Medical Surgical Nursing Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition. p. 955
- a baseline assessment is necessary for later comparisons and to determine treatment effectivenessSource: Medical Surgical Nursing Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition. p. 955
- fatigue compromises one’s ability to participate in daily activities. It is
34
and Mohn-Brown, Elaine,1st
Edition., p. 368
activities when feeling fatigued and to let go of unessential tasks.
4. explore strategies to modify existing activities, conserving energy when possible; seek assistance and delegate activities; and pace activities through the day to allow a balance between activity and rest.
5. encourage patient to obtain at least 8 hours of uninterrupted sleep at night.
important that the patient’s available energy be used to complete priority activities until blood glucose are regulated.Source: Medical Surgical Nursing Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition. p. 955
- many daily activities can be modified to consume less energy, but this requires the patient’s willingness to think about routine activities in a different way. It may not be possible for the patient to perform all desired activities until she is metabolically stable.Source: Medical Surgical Nursing Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition. p. 955
- effective nighttime sleep patterns help decrease daytime fatigueSource: Medical Surgical Nursing Health and Illness Perspectives Phipps, Wilma, et. al. 7th edition. p. 955
35
3. Risk for Infection: Left Leg Abrasions
- scratch marks on her left leg
- the patients disease condition could further worsen the would especially when body defenses cannot fight thoroughly because altered inflammatory process and impaired would healing.
Risk for infection: left leg abrasions related to ineffective body defenses
Persons with diabetes are at increased risk of infection. The effectiveness of the skin as a first line of defense can be diminished. Hyperglycemia can hamper the inflammatory response and wound healing and impair leukocyte function, migration of leukocytes to the site of infection, phagocytosis, and bacterial killing, al of which are involved in combating infection.
- prevent occurrence of infection - identify management to avoid complications.
- measures to avoid infection
1. monitor manifestations of infection: fever, chills; tachycardia; abnormal breath sounds; cloudy, foul smelling urine; redness, pain swelling, or discharge at injury site.
2. use and teach meticulous handwashing
3. keep skin clean and dry, using mild soap and lukewarm water.
4. maintain meticulous sterile technique when performing wound care or
- early diagnosis and treatment of infections can control their severity and decrease possible complications.Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
- handwashing is the best method for preventing the spread of infection.Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
- clean intact mucous membranes are the first line of defense against infection.Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
- these prevent infection in existing wounds or introduction of bacteria into the body.Source: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine
36
Sources: Medical Surgical Nursing Health and Illness PerspectivesPhipps, Wilma, et. al. 7th editionp. 967
any invasive procedure.
5. turn client and encourage coughing, deep breathing, and activity as tolerated.
6. encourage adequate nutrition and fluid intake
1st Edition., p. 384
- sedentary clients are prone to developing atelectasis and/or pneumoniaSource: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
- maintaining satisfactory food and fluid intake reduces susceptibility to infectionSource: Medical – Surgical Nursing Care Burke, Karen , LeMone, Priscilla , and Mohn-Brown, Elaine 1st Edition., p. 384
2.1.3 Drug Therapy Record
Hospital No.: 187908 Service: Medical
37
Physician: Dr. Armando Tan Impression: Type II Diabetes Mellitus
Drug/ Route/
Frequency/ Route
Classification/ Mechanism of
Action
Indications/ Contraindications/
Side Effects
Principles of Care Treatment Evaluation
1. Unasyn 750 mg 1 tab BID P.O.8 AM
2. Glucophage (Metformin)
Antibacterial
Bind bacteria cell wall, resulting in cell death.
Oral hypoglycemic
Indications;
-Upper and lower respiratory tract infection- UTI and pyelonephritis- Skin and soft tissue infections- gonoccocal infections
Contraindications;
- History of allergic reaction to any penicillin.
Adverse effects;
GI: GI disturbancesDerm: Skin raches, itchingCV: Phlebitis, boold disorders, anaphylaxis and superinfection
Indications:
1. Asses patient for infections
2. Monitor vital signs 3. Monitor intake and output of the patient.
4. Before initiating therapy, obtain a history to determine previous use of and reactions to penicillin or cephalosporins.
5. Observe patient for signs and symptoms of anaphylaxis.
1. Administer metformin with
1. Provide safety
2. inform the patient of the possible side effects of the drug
3. Tell patient to notify physician if diarrhea and fever occurs.
4. Advise patient to report signs of superinfection and allergy.
1. Observe patient for
The patient WBC is in normal range and did not experience any side effects
Patient serum
38
500 mg BID 1 TAB P.O. give with meals.
agents
Decreases hepatic production of glucose, decreases intestinal absorption of glucose, increases sensitivity to insulin
- Type II Diabetes Mellitus, monotherapy or in combination with other oral antidiabetics
Contraindication:
- Diabetic coma- Ketoacidosis- renal impairment- chronic liver disease- cardiac failure and recent MI- alcoholism- hypoxemia- shock- pregnancy
Adverse Effects:
GI: nausea, vomiting, diarrhea, abdominal bloating, unpleasant metallic tasteEndo: hypoglycemiaF and E: Lactic ascidosisMisc: decreased vit. B12 levels
meals to minimize side effects
2. Patients stabilized on a diabetic regimen who are exposed to stress, fever trauma, infection, or surgery may require administration of insulin. Withhold metformin and reinstitute after resolution of acute episode
3. Withhold metformin during studies requiring IV administration of iodinated contrast media.
signs of hypoglycemic reactions
2.Monitor CBC prior to and at least annually throughout therapy
3. Monitor serum glucose and glycosylated hemoglobin to evaluate effectiveness of therapy
glucose remained in normal level through the course of the therapy.
2.1.4 Health Teaching Plan
39
Patient’s Name: Mrs. Fe F. Soria Impression: Type II Diabetes
Mellitus
Complaints: Frequent urination Physician: Dr. Armando Tan
High Blood Sugar and a Lump on her Breast
Objectives Content Methodology EvaluationGeneral After 8 hours of teaching – learning activities the patient and significant others will be able to have a clear picture about her present condition
Specific After 45 mins. of varied teaching – learning activities the patient and significant other will able to:
1. define and identify fact about Type II Diabetes Mellitus
2. identify the risk factors for
Definition of Type II Diabetes Mellitus- is characterized by insufficient insulin production or resistance. Sufficient insulin is produced to prevent the breakdown of fats; therefore, ketosis does not occur. However, the amount of available insulin is inadequate to lower blood glucose levels through the uptake of glucose by muscle and fat cells. While it can occur at any age, Type II DM is usually seen older people. Heredity plays an important role in its transmission.
Risk Factors of Type II Diabetes Mellitus
Lecture – Discussion
Lecture – Discussion
The patient was able verbalize and demonstrate necessary knowledge, attitude and skills in managing this disease condition like stating the necessary information needed in type II diabetes mellitus, managing hypoglycemia and demonstrating
40
this disease condition.
3. enumerate possible complication that may arise in Type II Diabetes Mellitus
4. state the management of hypoglycemia
5. demonstrate proper wound
- obesity- increasing age- belonging to high-risk ethnic group
Complications of Type II Diabetes Mellitus- Hyperglycemic Hyperosmolar Nonketotic Syndrome
characterized by severely elevated blood glucose levels, extreme dehydration, and an altered level of consciousness. Infection, surgery, and dialysis are a few factors that can trigger HHNS
- Hypoglycemia cause by too much
insulin, overdose of oral antidiabetic agents, a little food , or excess physical activity. The onset is sudden, and blood glucose is usually les than 50 mg/dL.
Management of Hypoglycemia- people with hypoglycemia should take about 15 g of rapid acting sugar. Examples of fast-acting glucose are:
3 glucose tablets ½ cup of fruit juice or
regular soda 6 oz of skim milk 6 to 8 Life Savers
candies 2 to 3 tsp of sugar or
honey
Wound Care Prepare the and assemble
Lecture – Discussion
Lecture – Discussion
Discussion – Demonstration
how to perform wound care.
41
care
6. appreciate the importance of the management of Type II Diabetes Mellitus to prevent further complications.
all needed the equipment Remove binders or
adhesive tapes if used Remove and dispose of
soiled dressings appropriately
Clean the wound with gauze swabs moistened with cleaning solution
Use a separate swab for each stroke , and discard each swab after use
Dry the surrounding skin with dry gauze swabs as required. Do not dry the incision or wound itself.
Apply the ordered powder or equipment
Apply dressings to the drain site or incision.
The patient will be able to verbalize the importance of the management of this disease condition to prevent further complications.
– Return Demonstration
Sharing - Discussion
V. Evaluation and Recommendation
42
After rendering holistic care, the patient and the nurse were able to achieve the
specific objectives. The patient went home with an improved condition as evidenced by
having the sufficient knowledge, attitude and skill in managing her disease condition;
increased energy levels as evidenced by performance of activities of daily living and a
wound that steadily healing and free from any signs of infection. She was given discharge
health teaching about her diet, management of complications, and importance of wound
care. Discharge medications instruction was also given.
VI. Evaluation and Implication of This Case Study To:
Nursing Practice
This case study provides information about Type II Diabetes Mellitus and
nursing interventions and therapeutic techniques used with patients who have this
disease. It also provides information about the plan of care for patients who have
this disease condition for efficient nursing care.
Nursing Education
To nursing education, this case study would help by providing information
about the disease condition Type II Diabetes Mellitus. The student nurses, as
well as the teachers could gain additional information about this disease that is
common in children, so that it could better equip them for efficient nursing care
in the future.
Nursing Research
To the research team, that they will be able to come up with a new and
better interventions, whether medical or nursing, to treat the disease at an early
duration as well as knowing the latest facts to prevent the occurrence of the
disease, diabetes mellitus.
VII. The Referral and Follow-up
43
The patient was asked to visit her doctor, Dr. Armando Tan, one week after
discharge for a follow-up check up. She was also advice to have a strict
compliance on her medications and refer for any signs of complications.
44
VIII. Bibliography
Burke, Karen , LeMone, Priscilla ,and Mohn-Brown, Elaine. Medical – Surgical Nursing
Care. 1st Edition. Upper Saddle River, New Jersey: Pearson Education, Inc., 2003.
Deglin, Judith and Vallerand, April. Davis’s Drug Guide for Nurses. 5th Edition.
Philadelphia, Pennsylvania: 1997
Kozier, Barbara, ET. Al. Fundamentals of Nursing: Concept, Process and Practice. 5th
Edition. USA: Addison-Wesley Longman, Inc., 1998.
Martini, Frederic. Fundamentals of Anatomy and Physiology 6th Edition. USA: Pearson
Education, Inc., 2004.
Phipps, Wilma, ET. Al. Medical – surgical Nursing, Health and Illness Perspectives. 7th
Edition. St. Louis, Missouri: Mosby, Inc. 2003
Potter, Patricia and Perry, Anne Griffin. Fundamentals of Nursing: Concept, Process and
Pracitce. 3rd Edition. St. Louis, Missouri: Mosby, Inc., 1993
Smeltzer, Suzanne and Brenda Bare. Textbook of Medical Surgical Nursing. 9th Edition.
Philadelphia, PA: Lippincott Williams and Williams, 2000.
Thibodeau, Gary and Patton, Kevin. Anatomy and Physiology 5th Edition. USA:
Mosby, Inc., 2003.
45
Recommended