ORIGINAL ARTICLE
Higher Dose and Dose-Rate in Smaller Tumors Resultin Improved Tumor Control
A. Mayer, M.D.,* E. Tsiompanou, M.D., A. A. Flynn, Ph.D.,
R. B. Pedley, Ph.D., J. Dearling, Ph.D.,
R. Boden, and R. H. J. Begent, M.D., F.R.C.P., F.Med.Sci.
Cancer Research UK Targeting and Imaging Group, Department of Oncology, Royal
Free Campus, Royal Free and University College Medical School, University College
London, London, UK
ABSTRACT
Small tumors are more sensitive to radioimmunotherapy (RIT) than larger ones.
A greater proportion of viable radiosensitive areas in small tumors, higher antibody
uptake, and radiation dose may be responsible. Six groups of mice with small (median
tumor size 0.06 cm3) or large LoVo xenografts (median tumor size 0.38 cm3) received
either RIT using a 131I-labeled anti-CEA antibody A5B7, 5-fluorouracil (5-FU)
modulated with folinic acid (FA), or no treatment. The % injected activity/gram,
antibody distribution in viable and necrotic areas, and dose distribution were
determined. High-power microscopy images of the original section were reconstructed
to estimate the proportion of viable areas. Mice with small and large tumors grew
significantly less rapidly when treated with RIT compared to the control group
(p , 0.0004 and p , 0.003, respectively), while 5-FU was ineffective. Small tumors
treated with RIT grew less than large tumors (p , 0.02). A higher amount of % injected
activity/gram of tumor (median 26.6% vs. 8.1%, p ¼ 0:0007Þ and a higher dose-rate
were found in small tumors at 24 hours post injection (viable areas: 56.2 ^ 23.7 vs.
13.3 ^ 7 cGy/h, necrosis 19.2 ^ 16.3 vs. 4.9 ^ 4.7 cGy/h, p ¼ 0:0007Þ: It appears that
as viable tumor masses grow the access to them decreases and this has a fourfold effect
on dose delivered for RIT in this example. These data support the consideration of use
of RIT for adjuvant treatment in colon cancer.
Key Words: LoVo xenografts; Radioimmunotherapy; Radioluminography; Dose-rate.
382
DOI: 10.1081/CNV-120018229 0735-7907 (Print); 1532-4192 (Online)
Copyright q 2003 by Marcel Dekker, Inc. www.dekker.com
*Correspondence: Astrid Mayer, Department of Oncology, Royal Free Campus, Royal Free and University College Medical School,
University College London, Rowland Hill Street, London NW3 2PF, United Kingdom; Fax: þ44 207 794 3341; E-mail:
CANCER INVESTIGATION
Vol. 21, No. 3, pp. 382–388, 2003
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
1/08
/14
For
pers
onal
use
onl
y.

INTRODUCTION
Colorectal cancer remains a leading cause of cancer
death.[1] Fifty percent of patients with Duke’s stage C
and 20% of patients with Duke’s stage B colon cancer
relapse within 5 years. Adjuvant treatment with modu-
lated 5-fluorouracil(5-FU) has lead to a 30% improve-
ment of 5-year survival in patients with Duke’s stage C
cancer.[2] Research into new and more effective
treatment strategies include targeted therapy that is
based on tumor-specific antibodies. These are either
linked with therapeutic moieties such as radionuclides in
radioimmunotherapy (RIT) or are effective in unconju-
gated form due to immunological mechanisms such as
antibody-dependent cellular cytotoxicity (ADCC). There
are currently two antibodies licensed for clinical use, i.e.,
the humanized monoclonal anti-HER2 antibody trastu-
zumab[3] in breast cancer and the chimaeric anti-CD20
antibody rituximab[4] in lymphoma. In spite of initially
promising results in colon cancer with the unconjugated
antibody 17-1 A,[5] adjuvant treatment with 17-1 A
proved inferior to 5-FU in a recently reported study.[6]
Radioimmunotherapy is potentially more effective
than an unconjugated antibody. It has shown only limited
response in advanced colon cancer,[7] while a response
rate of 26% was reported in small-volume (less than
2.5 cm) colorectal cancer.[8] This is in agreement with
experimental data, which indicated 10 times more
efficient localization of antibody in tumors of less
than 100 mg when compared with larger tumors.[9]
Blumenthal et al.[10] confirmed these data by demon-
strating that tumor nodule size affected the therapeutic
outcome of RIT using GW-39 colonic tumor xenografts
even at the microscopic level. As a result, very small
tumors can be eradicated while larger tumors exhibit a
growth reduction but not a cure.
As colorectal carcinomas progress they outgrow
their blood supply and heterogeneity of tumor masses
results. Central areas tend to be necrotic, while the well-
perfused periphery contains viable, radiosensitive cells.
Specific antibodies preferentially localize in the viable,
radiosensitive part of the tumor where the radiation dose
is most effective.[11] Penetration into the tumor is further
restricted by antibody size.[12] By contrast, cytostatic
drugs have a much smaller molecular weight (5-FU,
130.1 Da) and no affinity for tumor-associated antigens
and so penetration should be a relatively minor obstacle.
Indeed, a larger percentage of the tumor volume is
accessible for small molecules.[13] One explanation for
greater efficacy of RIT in small tumors would be a
greater proportion of radiosensitive viable cells, alter-
natively, uptake may decrease throughout the tumor
mass with increasing tumor size. It is important to know
the extent of any effect, and this can be studied by
making estimates of radiation dose delivered to the
viable and necrotic areas. Comparison of the effects of
RIT and modulated 5-FU make it possible to assess the
extent to which the size effect is specific for antibodies
compared with conventional cytotoxic chemotherapy.
MATERIALS AND METHODS
LoVo Xenograft and Treatment
The moderately well-differentiated carcinoembryo-
nic antigen (CEA)-expressing human colonic tumor cell
line LoVo[14] was used to develop a xenograft in the
flanks of female nude (nu/nu) mice. Passaging was done
by subcutaneous implantation of small tumor pieces.
Xenografts were grown in one group until they reached a
median size of 0.06 cm3 (range 0.02–0.11 cm3) and in
the second group until a median size of 0.38 cm3 (range
0.16–0.57 cm3). Mice weighed 20–25 g at the beginning
of the experiment and were weighed on the day of
treatment and on every subsequent third or fourth day.
Tumors were measured in three dimensions (length,
width, and height) and the volume estimated as
length £ width £ height/2. Mice with tumors exceeding
2 cm3 were killed. White blood cell (WBC) counts were
performed before the experiment and every subsequent
week to evaluate treatment toxicity.
Six mice of each group received 40mg of 131I
(Amersham, Little Chalfont, UK)-labeled A5B7, a
monoclonal anti-CEA antibody.[7] The A5B7, an IgG1
molecule, was raised against heat-treated CEA and
purified by protein A affinity chromatography. The
antibody was labeled by the Iodogen method[15] to a
specific activity of 370 MBq/ mg protein. Another six
mice per group were treated with 90 mg/kg folinic acid
(FA) (David Bull Laboratories, Warwick, UK) i.p.
followed by 27.5 mg/kg 5-FU (David Bull Laboratories,
Warwick, UK) i.v. 2 hours later for 5 days. Six mice of
each group were kept as controls.
Laboratory Gamma Counting
and Radioluminography
Tumors were weighed after removal and radioac-
tivity was measured in a laboratory gamma counter
(1470 Wizard, Wallac, Milton Keynes, UK). The
percentage injected activity/gram of tumor was
calculated.
Higher Dose and Dose-Rate in Small Tumors 383
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
1/08
/14
For
pers
onal
use
onl
y.

Storage phosphor plate technology[11] was used to
assess the distribution of the antibody in sections of
tumor in a separate study. Seven small tumors (median
0.07 cm3, range 0.05–0.11 cm3) and seven large tumors
(median 0.35 cm3, range 0.16–0.61 cm3) were included.
Tumors were fixed in 10% formalin for 48 hours,
embedded in paraffin, and 3mm-thick sections were cut.
After dewaxing, tumor sections were exposed to
phosphor plates for 7 days. The images were digitized
with a phosphor plate reader (Model 425 Phosphor-
imager, Molecular Dynamics, Chesham, UK) and
analyzed using software written in Interactive Data
Language. All sections were stained with haematoxylin
and eosin after scanning for comparison of radiolabeled
antibody distribution and tissue morphology. Necrotic
and viable areas were determined by histological
examination.
High-power microscopy images of sections taken
from the center of small and large tumors were acquired
using a Minolta Rd-175 digital camera (Minolta, UK)
mounted on a microscope. Images were taken of adjacent
areas of the entire section while ensuring there was an
overlap with surrounding areas. These images were
automatically reconstructed to form a mosaic of the
original section by iteratively searching for the
maximum cross-correlation between overlapping areas
of adjacent images.[16] Regions of interest were drawn
around viable tumor areas in the complete section. The
sum of the areas of these regions then gave a measure of
the relative amount of viable areas in the tumor. These
were used to estimate the equivalent thickness of a viable
shell in a spherical model of a tumor.
Low-resolution images of the stained sections were
also obtained using a desk scanner (Hewlett Packard Ltd,
Palo Alto, CA). Registration of radioluminographs and
corresponding histological section was performed
according to the cross-correlation method.[17] Regions
of interest were drawn around the viable and necrotic
areas on the digitized stained histological image and
were copied onto the corresponding radioluminograph
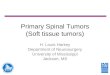
(Fig. 1). The ratio of mean counts per pixel in viable
relative to necrotic regions (X) was calculated and
compared for both large and small tumors. The
percentage injected activity/gram in viable and necrotic
areas was calculated using:
Viable ¼2XP
X þ 1and ð1Þ
Necrotic ¼2P
X þ 1ð2Þ
where P is the percentage injected activity/gram for the
whole tumor.
Dosimetry
Doserate is defined as the amount of radioactivity
deposited per unit of time. Higher dose-rate is known to
be important for the therapeutic effect of RIT as it allows
cells less DNA damage repair.
The mean dose-rate in the tumor was calculated
using the equation
R ¼ PA0e2ltS ð3Þ
where:
A0 is the injected activity, in Bq
l is the radionuclide decay constant (s21)
t is the time of observation, in seconds
S is the mean dose-rate per unit activity in the tumor
and is given by Bardies et al.[18] for each tumor size.
Beta point dose kernels[19] were used to generate the
dose-rate distribution from the images of antibody
distribution. The regions of interest that defined viable
and necrotic areas were then copied onto the image of
dose distribution (Fig. 1). This allowed the calculation of
Figure 1. Image of tumor morphology (A) enables the quantitation of antibody uptake (B) and dose-rate (C) in viable and
necrotic areas. (See color figure at end of issue.)
Mayer et al.384
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
1/08
/14
For
pers
onal
use
onl
y.

the ratio of dose-rate of viable and necrotic cells (X). The
actual dose-rate to viable and necrotic cells was then
estimated by setting P ¼ R in equations 1 and 2.
Data Analysis and Statistics
The natural logarithm of tumor size at each time point
was used to calculate the slope for each mouse based on a
least-square fit on Microsoft Excel 5.0. This allowed
comparison of tumor growth. Comparison between
groups was carried out using the unpaired t-test assuming
equal variances.
RESULTS
Growth of LoVo Xenografts and Toxicity
The growth of LoVo xenografts was measured for
22 days unless tumor size exceeded 2 cm3 prior to that.
Comparison of the growth of small and large tumors
treated with RIT showed that small tumors grew
significantly less compared to large tumors (p , 0.02),
while there was no significant difference of small and
large tumor growth in the group treated with 5-FU and in
the control group. Small (p , 0.0004) and large
(p , 0.003) xenografts treated with RIT grew signifi-
cantly less when compared to the control group. There
was no significant growth delay for mice with large or
small LoVo xenografts treated with 5-FU. However,
small LoVo xenografts treated with RIT also grew
significantly less than small xenografts treated with 5-FU
ðp ¼ 0:00003Þ: Growth curves for small and large
xenografts are shown in Fig. 2.
Toxicity in terms of weight loss was not observed in
any of the groups with small LoVo xenografts, while a
mean drop in weight of 6% on day 7 was measured in
mice with large tumors receiving RIT and of 8% in mice
with large tumors receiving 5-FU/FA. There was no
weight loss in the control group. A drop of the WBC
count to less than 30% of the pretreatment values was
found on day 7 and day 14 in both groups receiving RIT
and in mice bearing large tumor xenografts treated with
5-FU/FA. The drop of WBC count in mice with small
xenografts receiving 5-FU/FA was very moderate
(,10%). The individual WBC counts showed a
considerable variance. The WBC counts recovered by
day 21, the drop in WBC counts is therefore most likely a
treatment-related side effect. One mouse treated with
RIT and bearing a large LoVo xenograft was found dead
on day 10. Death due to toxicity seems unlikely at this
dose level.
Antibody Uptake and Dosimetry
Laboratory gamma counting showed that the
counts/minute for large tumors were 12% higher
compared to small tumors. This was not significantly
different ðp ¼ 0:755Þ: However, the median percentage
injected activity/gram was 26.6% after 24 hours in small
tumors (range 19.9–59.2%) and 8.1% in large tumors
(range 1.6–12.5%), which was significantly different
ðp ¼ 0:0007Þ:
Figure 2. Comparison of tumor growth in mice with small
and large LoVo xenografts (mean values). A significant growth
delay was found in mice bearing small xenografts treated with
RIT when compared with the group receiving 5-FU/FA ðp ¼
0:00003Þ and the untreated control group (p , 0.0004). Large
tumors treated with RIT grew significantly less than the
untreated control group (p , 0.003). There was no significant
difference between the group treated with RIT compared with
5-FU/FA.
Higher Dose and Dose-Rate in Small Tumors 385
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
1/08
/14
For
pers
onal
use
onl
y.

Comparison of the percentage of the tumor volume
that is viable in small and large tumors showed a
significantly higher percentage of viable areas in large
tumors (85%) compared to small tumors (72%, p ¼
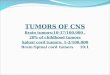
0:023Þ: The thickness of the viable shell increased with
tumor size (Fig. 3).
The ratio of counts per pixel in viable versus
necrotic areas was 2.5 in small tumors and 2.8 in large
tumors ðp ¼ 0:42Þ: However, % injected activity/gram in
both viable ðp ¼ 0:0007Þ and necrotic ðp ¼ 0:0006Þ parts
of small tumors was significantly higher than in large
tumors. Details are given in Table 1.
Dose rate at 24 hours post injection was significantly
higher in viable ðp ¼ 0:0007Þ and necrotic ðp ¼ 0:0006Þ
parts of small tumors compared to large tumors.
DISCUSSION
This experiment confirms the enhanced therapeutic
effect of RIT in small tumors. The small tumors used in
our studies had a median radius of 2.5 mm, while the
radius of the larger tumors measured 4.4 mm (median).
Comparison of the extent of viable, radiosensitive parts
in small and large tumors unexpectedly showed a higher
amount of viable areas in the group of the large tumors,
which resulted in rejection of the hypothesis that a higher
proportion of viable, radiosensitive areas in smaller
tumors causes the enhanced therapeutic effect of RIT.
However, our mathematical modeling (Fig. 3) suggests
that the proportional amount of viable areas will decrease
with tumor size above a certain threshold, which is
around 4 mm radius in LoVo tumors. The relationship
beween viable and necrotic areas seems to be more
complex in smaller tumors depending on blood vessel
development and oxygen diffusion.
Laboratory gamma counting showed that there was
no significant difference in the absolute amount of
radioactivity in large and small tumors. However, a
significantly higher percentage of radioactivity per gram
of tumor was found in small tumors, leading to a higher
dose throughout the tumor. Furthermore, radiolumino-
graphy confirmed the higher amount of antibody in
viable and necrotic parts of small tumors. Consequently,
the dose-rate, which gives a measurement of the amount
of radioactivity deposited per unit of time, was
significantly higher in viable and necrotic areas in
small tumors at 24 hours. Therefore, the enhanced
therapeutic effect in small tumors is due to the higher
dose and dose-rate throughout the tumor and to the viable
radiosensitive areas in particular. This leads to the
question: Why is the absolute amount of antibody
delivered to small and large tumors the same, i.e., the
delivery of antibodies less efficient in larger tumors?
We would like to discuss two possible explanations:
The amount of antibody available for localization in the
tumor is primarily determined by the concentration in the
blood and the total blood volume in the tumor. The total
blood volume in the tumor increases relatively less with
tumor size as the blood vessel density decreases, i.e., the
average vascular surface area decreases with tumor
growth, resulting in reduced transvascular exchange in
larger tumors compared to smaller tumors.[20] Therefore,
there is no significant difference in the absolute amount
of antibody in large and small tumors. Consequently, the
percentage injected activity per gram is inversely related
to the tumor volume. Alternatively, increased per-
meability of tumor vasculature may be responsible.
Studies of tumor blood vessels revealed that particularly
mature veins and venules at the tumor-host interface
showed increased permeability for circulating macro-
molecules using 70 and 150 kD fluorescinated dextrans,
while immature interface vessels and tumor-penetrating
vessels did not leak these macromolecular tracers
significantly.[21] Blumenthal et al.[22] found that the
vascular permeability was dependent on tumor size;
small untreated tumors were found to have a higher
vascular permeability than large tumors due to a
comparably lower interstitial pressure.
The extent of the increased radiation dose of
fourfold, as shown here, indicates that a major
therapeutic gain will result if RIT is used in small-
volume disease. The gain in efficacy for 5-FU/FA was
significantly less than for RIT, indicating that the effect is
particularly marked for antibody therapy. Clinical
results, so far, are in agreement with our experimental
data. A higher response rate with RIT was reported in
small-volume disease[8] compared to advanced colon
Figure 3. Variation of the thickness of the viable shell with
tumor radius.
Mayer et al.386
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
1/08
/14
For
pers
onal
use
onl
y.

cancer.[7] Radioimmunotherapy therefore seems favor-
able for adjuvant treatment in colon cancer.
ACKNOWLEDGMENTS
This work was supported by Cancer Research UK,
The European Society for Medical Oncology, and the
Ronald Raven Chair in Clinical Oncology Trust.
REFERENCES
1. Boyle, P. Some recent developments in the epidemiology
of colorectal cancer. In Management of colorectal cancer;
Bleiberg, H., Rougier, P., Wilke, H.J., Eds.; Martin
Dunitz: London, 1998; 19–34.
2. Moertel, C.G.; Fleming, T.R.; MacDonald, J.S.; Haller,
D.G.; Laurie, J.A.; Goodman, P.J.; Ungerleider, J.S.;
Emerson, W.A.; Tormey, D.C.; Glick, J.H.; Veeder,
M.H.; Mailliard, J.A. Levamisol and fluorouracil for
adjuvant therapy of resected colon carcinoma. NEJM
1990, 322, 352–358.
3. Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.;
Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.;
Wolter, J.; Pegram, M.; Baselga, J.; Norton, L. Use of
chemotherapy plus a monoclonal antibody against HER2
for metastatic breast cancer that overexpresses HER2.
NEJM 2001, 344 (11), 783–792.
4. Maloney, D.G.; Liles, T.M.; Czerwinski, D.K.;
Waldichuk, C.; Rosenberg, J.; Grillo-Lopez, A.; Levy,
R. Phase I clinical trial using escalating single-dose
infusion of chimeric anti-CD20 monoclonal anti-
body (IDEC-C2B8) in patients with recurrent B-cell
lymphoma. Blood 1994, 84 (8), 2457–2466.
5. Riethmuller, G.; Holz, E.; Schlimok, G.; Schmiegel, W.;
Raab, R.; Hoffken, K.; Gruber, R.; Funke, I.; Pichlmaier,
H.; Hirche, H.; Buggisch, P.; Witte, J.; Pichlmayr, R.
Monoclonal antibody therapy for resected Duke’s C
colorectal cancer: Seven year outcome of a randomised
controled trial. J. Clin. Oncol. 1998, 16, 1788–1794.
6. Punt, C.J.; Nagy, A.; Douillard, J.; Figer, A.; Skovsgaard,
T.; Monson, J.; Barone, C.; Jones, D.; Dethling, J.;
Colman, J. Edrecolomab (17-1A antibody) alone or in
combination with 5-fluorouracil based chemotherapy in
the adjuvant treatment of stage III colon cancer: results of
a phase III study. ASCO Proc 2001, 20, 123a, 487.
7. Lane, D.M.; Eagle, K.F.; Begent, R.H.; Hope-Stone, L.D.;
Green, A.J.; Casey, J.L.; Keep, P.A.; Kelly, A.M.;
Ledermann, J.A.; Glaser, M.G.; Hilson, A.J.W. Radio-
immunotherapy of metastatic colorectal tumours with
iodine 131-labelled antibody to carcinoembryonic anti-
gen: phase I/II study with comparative biodistribution of
intact and F(ab’)2 antibodies. Br. J. Cancer 1994, 70,
521–525.
8. Behr, T.M.; Liersch, T.; Canelo, R.; Woermann, B.;
Hiddemann, W.; Ringe, B.; Becker, H.; Becker, W.
Radioimmunotherapy of small volume disease of color-
ectal cancer: results of a clinical Phase I/II trial. EJC 1999,
35 (Suppl. 5), 93.
9. Pedley, R.B.; Boden, J.; Keep, P.A.; Harwood, P.J.;
Green, A.J.; Rogers, G.T. Relationship between tumour
size and uptake of radiolabelled anti-CEA in a colon
tumour xenograft. Eur. J. Nucl. Med. 1987, 13,
197–202.
10. Blumenthal, R.D.; Sharkey, R.M.; Haywood, L.; Natale,
A.M.; Wong, G.Y.; Siegel, J.A.; Kennel, S.J.;
Goldenberg, D.M. Targeted therapy of athymic mice
bearing GW-39 human colonic cancer micrometastases
with 131I-labeled monoclonal antibodies. Cancer Res.
1992, 52, 6036–6044.
11. Flynn, A.A.; Green, A.J.; Boxer, G.M.; Casey, J.L.;
Pedley, R.B.; Begent, R.H.J. A novel technique, using
radioluminography, for the measurement of uniformity of
radiolabelled antibody distribution in a colorectal cancer
Table 1. Comparison of amount of activity in large and small tumors.
Small tumors Large tumors p-value
Total amount of radioactivity
(counts per minute)
726092 819885 p ¼ 0:755
Percentage activity/gram after
24 hours
26.6% 8.1% p ¼ 0:0007
Mean viable area 71.6% 85.2% p ¼ 0:02
Activity in
Viable areas (mean counts/pixel) 47.7 11.1 p ¼ 0:0007
Necrotic areas (mean counts/pixel) 18.8 3.9 p ¼ 0:0006
Viable/necrotic tissue ratio 2.5 2.8 p ¼ 0:42
Dosimetry at 24 hours in
Viable areas (cGy/hr) 56.24 ^ 23.68 13.32 ^ 6.96 p ¼ 0:0007
Necrotic areas (cGy/hr) 19.24 ^ 16.28 4.88 ^ 4.74 p ¼ 0:0006
Higher Dose and Dose-Rate in Small Tumors 387
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
1/08
/14
For
pers
onal
use
onl
y.

xenograft model. Int. J. Rad. Onc. Biol. Phys. 1999, 43,
183–189.
12. Yokota, T.; Milencic, D.E.; Whitlow, M.; Schlom, J.
Rapid tumour penetration of a single chain Fv and
comparison with other immunoglobulin forms. Cancer
Res. 1992, 52, 1402–1408.
13. Krol, A.; Maresca, J.; Dewhirst, M.W.; Yuan, F.
Available volume fraction of macromolecules in the
extravascular space of a fibrosarcoma: Implications for
drug delivery. Cancer Res. 1999, 59, 4136–4141.
14. Blumenthal, R.D.; Sharkey, R.M.; Natale, A.M.; Kashi,
R.; Wong, G.; Goldenberg, D.M. Comparison of
equitoxic radioimmunotherapy and chemotherapy in the
treatment of human colonic xenografts. Cancer Res. 1994,
54, 142–151.
15. Mayer, A.; Chester, K.A.; Bhatia, J.; Pedley, R.B.; Read,
D.A.; Boxer, G.M.; Begent, R.H. Exemplifying
guidelines for preparation of recombinant DNA products
in phase I trials in cancer: preparation of a genetically
engineered anti-CEA single chain Fv antibody. Eur.
J. Cancer 1998, 34, 968–976.
16. Laroche, S. Managing very large-scale digital images in
microscopy. Microscopy and Analysis 1998, 7, 5–7.
17. Flynn, A.A.; Green, A.J.; Boxer, G.; Pedley, R.B.; Begent,
R.H.J. A comparison of image registration techniques for
the correlation of radiolabelled antibody distribution with
tumour morphology. Phys. Med. Biol. 1999, 44, 151–159.
18. Bardies, M.; Chatal, J.-F. Absorbed doses for internal
radiotherapy from 22 beta-emitting radionuclides: beta
dosimetry of small spheres. Phys. Med. Biol. 1994, 39,
961–981.
19. Berger, M.J. Distribution of absorbed dose around point
sources of electrons and beta particles in water and other
media; MIRD pamphlet no.7; Society of Nuclear
Medicine: New York, 1971.
20. Jain, R.K. Haemodynamic and transport barriers to the
treatment of solid tumours. Int. J. Radiat. Biol. 1991, 60,
85–100.
21. Dvorak, H.F.; Nagy, J.A.; Dvorak, J.T.; Dvorak, A.M.
Identification and characterization of the blood vessels
of solid tumours that are leaky to circulating macro-
molecules. Am. J. Pathol. 1988, 133, 95–109.
22. Blumenthal, R.D.; Kashi, R.; Sharkey, R.M.; Goldenberg,
D.M. Quantitative and qualitative effects of experimental
radioimmunotherapy on tumour vascular permeability.
Int. J. Cancer 1995, 61, 557–566.
Mayer et al.388
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
1/08
/14
For
pers
onal
use
onl
y.

From “Higher Dose and Dose-Rate in Smaller Tumors Result in Improved Tumor Control,” by A. Mayer et al.,
pp. 382–388.
Figure 1. Image of tumor morphology (A) enables the quantitation of antibody uptake (B) and dose-rate (C) in viable and
necrotic areas.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
Can
cer
Inve
st D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y C
DL
-UC
San
ta C
ruz
on 1
1/08
/14
For
pers
onal
use
onl
y.
Recommended