-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
1/53
CCARTILAGEARTILAGEFFORMINGORMING
TTUMORSUMORS
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
2/53
CCARTILAGEARTILAGE FFORMINGORMING TTUMORSUMORS
Benign:
y Chondroma
y Osteochondroma
Maligna:y Chondrosarcoma
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
3/53
CCHONDROMAHONDROMA
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
4/53
CCHONDROMAHONDROMA
Benign and asymptomatic cartilaginous tumor ofbone which most
often occurs in adolescents oryoung adults;
It is an intramedullary cartilage lesion located incentral
metaphysis;
Intramedullary tumor develops in adjacentmetaphysis and may
eventually penetrates thediaphysis;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
5/53
Results from failure of normal endochondral
ossification below growth plate & represents a
dysplasia of the central growth plate;
y
If dysplastic process occurs in lateral growth plate,resulting
tumor is called osteochondroma;
y Dysplastic cartilaginous proliferation beneath the
perichondrium results in periosteal chondroma;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
6/53
SSITESITES OFOF INVOLVEMENTINVOLVEMENT::
Hand:
y The most common benign skeletal lesions of the hand
y Most often affects small tubular bones of hands or
feet (40-65%);
y It is a frequent cause of pathologic fracture;
May also affect proximal humerus and femoral
shaft;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
7/53
RRISKISKOFOF TRANSFORMATIONTRANSFORMATION::
Enchondroma usually becomes latent in adulthood,
& < 2% of asymptomatic solitary enchondromas
will transform to chondrosarcoma
Enchondromas of long bones have higher chance
for malignant transformation;
Risk of malignant transformation is about 10-25%;
Maffucci disease (multiple enchondromas andhemangiomas) risk is
near 100%;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
8/53
EXAMINATION:
Enchondroma does not cause symptoms unless
there is pathologic frx;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
9/53
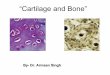
HISTOLOGY:
Lobules of different sizes separated by small
septa of fibrous tissue;
May see uniform cartilage cells with dark round
nuclei & some binucleate nuclei (which isnormal);
Often it is difficult to differentiate an
enchondroma from a low grade chondrosarcoma
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
10/53
RADIOGRAPHS:
Central radiolucent lesion w/ well defined miminallythickened
bony margin;
During active phase in adolesence, the lesion mayslowly
enlarge.
In children, cortex is usually thin and the lesion
isradiolucent;
Later, intralesional calcifications appear;
There is no periosteal reaction;
In latent phase, cartilaginous tissue may calcify w/diffuse
punctate pattern;
As lesion matures, it deveolops a reactive margin;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
11/53
RADIOGRAPHIC FINDING
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
12/53
OLLIERS DISEASE:
MULTIPLE
ENCHONDROMA.
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
13/53
BONE SCANS:
Demonstrate radioisotope uptake in margin,
related to activity of lesion;
While there is moderate uptake in the acitive
phase there will also be some activity in latentphase;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
14/53
TREATMENT:
Asymptomatic solitary enchondromas may be
followed non operatively
Prognosis for benign enchondroma is excellent.
If solitary or multiple enchondromas becomesymptomatic or begin
to enlarge, they may
require biopsy to r/o malignancy (the terrible
triad: pain, increase radioisotope uptake on bone
scan, & destructive changes on x-ray);
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
15/53
PPATHOLOGICATHOLOGIC HANDHAND ANDAND
FINGERFINGER FRACTUREFRACTURE::
Most cases the fracture is allowed to heal with
closed treatment;
Curettage and bone grafting is then required
after fracture healing;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
16/53
EXCISION:
Tumor is excised with a wide margin to reduce
recurrance
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
17/53
OOSTEOCHONDROMASTEOCHONDROMA(C(CARTILAGEARTILAGE--CCAPPEDAPPED
EEXOSTOSISXOSTOSIS))
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
18/53
OOSTEOCHONDROMASTEOCHONDROMA
Adevelopmental dysplasia of peripheral growth
plate which forms a cartilage capped projection of
bone found near metaphyses of long bones;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
19/53
Peripheral chondroblast grows outward from the
metaphysis, acting as an ectopic growth plate,
which ceases growth at skeletal maturation;
An excrescene of trabecular bone capped by athin zone of
proliferating cartilage;
The most common benign bone tumor;
Usually occurs in long bones, but may occur any
bone that is preformed in cartilage;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
20/53
DDIFFERENTIALIFFERENTIAL DDIAGNOSISIAGNOSIS::
Multiple cartilaginous exostoses
y Patients have polyostotic tumors
y Look for short stature, clubbing of radius, & angular
deformity of the lower limbs;
y Have an increased risk for secondary chondrosarcoma
after the age of 30 years;
Parosteal osteosarcoma
y May present as a symptomatic "exostosis" that
increases in size in adults;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
21/53
TTUMORUMOR GGROWTHROWTH::
Lesion growths by enchondral ossification of
proliferatingcartilage cells in its cap;
Tumor will continue to enlarge during skeletal growth, butwill
become latent at skeletal maturity;
y However, the lesion may continue to grow into the 3rd
decade;
y Occcassionally a lesion grows more rapidly than expected;
Most common locations are proximal or distal femur,proximal
humerus, proximal tibia, pelvis, and scapula;
y In areas other than the knee, more likely to undergoemalignant
degeneration;
y May occur in the spine and cause neurologic damage;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
22/53
MMALIGNANTALIGNANT TTRANSFORMATIONRANSFORMATION::
Risk of sarcomatous transformation in solitary
exostosis is about 1%, but in MHE (Multiple
Hereditary Exostosis), risk approaches 10%;
Evidence for transformation: (to chondrosarcoma)y Cartilaginous
cap thicker than 1 cm in an adult (in child
may be 2-3 cm thick) as seen by MRI;
y Cudden or marked increase in uptake on bone scan in
an adult
y
Confirmation by CT or MRI imaging of a soft tissuemass or
displacement of a major neurovascular bundle;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
23/53
CCLINICALLINICAL PPRESENTATIONRESENTATION::
Look for a firm, nontender, immovable mass
arising near end of the long bone;
Asymptomatic lesion, may be caused by
irritation of overlying soft tissues which may goon to form a
fluid filled bursa;
Bursal fluid may be mistaken for a soft tissue
mass;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
24/53
DDIAGNOSTICIAGNOSTIC STUDIESSTUDIES::
X-ray appearance of an exostosis is either flat,sessile lesion
or a peduculated (stalk like)process;
Peduncultaed osteochondromas are oriented in
proximal direction; X-ray hallmark is blending of tumor into
underlying metaphysis;
Look for a well defined metaphyseal excrescenceof bone w/ a
mottled density;
Calcification:y Cartilaginous cap displays irregular areas
of
calcification;
y Amount of calcification and bone formation increase w/age
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
25/53
RADIOGRAPHIC FINDING
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
26/53
OsteochondromaOsteochondroma(4D USG)(4D USG)
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
27/53
MMICROSCOPICICROSCOPIC EEXAMXAM::
Cartilaginous cap is seen to have same pattern asnormal growth
plate but it will be less organized;
Underlying trabeculae form by endochondralossification of cap
and contain central cores of calcifiedcartilage.
Cartilage cells w/ small round or elongated nucleiwhich may be
positioned in rows similar to a physis;
Polymorphy and hyperchomasy of cartilage cells is anexpected
finding in young children;
Cartilagenous cap may be upto 1 cm in width inadolescence and
that a cap greater than 3 cm is
consistent w/ low grade chondrosarcoma;
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
28/53
OsteochondromaOsteochondroma microscopy:microscopy:
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
29/53
TTREATMENTREATMENT::
No treatment is required if the diagnosis is not in
doubt and if the patient is relatively
asymptomatic;
Surgical resection is indicated forpersistantirritation (from
bursitis) or for neurovascular
comprimise;
Surgical resection is also indicated for continued
osteochondroma growth after skeletal maturity
(in which case malignancy is suspected);
-
8/3/2019 Cartilage Forming Tumors Cartilage Forming Tumors
30/53
TTREATMENTREATMENT::
Definitive treatment includes marginal excisionof an active
exostosis, including the cartilaginouscap & overlying
perichondrium;
Deep bony base has minimal activity and may be
removed piecemeal The cartilaginous cap should not be
traumatized
during its removal;
Prognosis for a solitary exostosis is excellent (





![Cartilage - facultymembers.sbu.ac.irfacultymembers.sbu.ac.ir/rajabi/ppt toPDF/Cartilage [Compatibility Mode].pdfFibrocartilage • Fibrous Cartilage • is a form of connective tissue](https://img.pdfslide.us/doc/110x75/6012989a4318862a0e5813ae/cartilage-topdfcartilage-compatibility-modepdf-fibrocartilage-a-fibrous.jpg)