21/03/2018
1
Headache Pathway OverviewHow can I help my migraine
patient?
Dr Elizabeth Leroux, MD, FRCPCHeadache ProgramUniversity of Calgary
Banff 2018
Faculty/Presenter Disclosure
• Faculty/Presenter: Dr. Elizabeth Leroux
• Relationships with commercial interests:
Grants/Research Support: Not Applicable
Speakers Bureau/Honoraria: Allergan, Eli Lilly, Teva, Novartis, Amgen, Aralez
Consulting Fees: Not applicable
Other: This presentation has received support from the Alberta College of Family Physicians in the form of a speaker fee and/or expenses.

21/03/2018
2
ACFP 63rd ASADisclosure of Commercial Support
This program has received financial support in the form of sponsorship from:
• Potential for conflict(s) of interest: Those speakers/faculty who have made COI disclosure are noted in the 63rd ASA Program and on the Salon A/B slide scroll.
Mitigating Potential Bias
• ACFP: → The ACFP’s Sponsorship Guidelines apply to ASA Sponsorship. The ACFP abides by the College of
Family Physicians of Canada’s Understanding Mainpro+ Certification Guidelines, the Canadian Medical Association’s Policy Guidelines for Physicians in Interactions With Industry and the Innovative Medicines Canada Code of Ethical Practices (2016). As a non‐profit organization, the ACFP complies with Canada Revenue Agency regulations. When deliberating acceptance of sponsorship, the ACFP considers and accepts sponsorship only from those whose products, services, policies, and values align with the ACFP vision, values, goals, and strategies priorities.
• ASA Planning Committee: → Consideration was given by the 63rd ASA Planning Committee to identify when Planning
Committee members’ and speakers’ personal or professional interests may compete with or have actual, potential, or apparent influence over program content.
→ Material/Learning Objectives and/or session description were developed and reviewed by a Planning Committee composed of experts/family physicians responsible for overseeing the program’s needs assessment and subsequent content development to ensure accuracy and fair balance.
→ The 63rd ASA Planning Committee reviewed Sponsorship Agreements to identify any actual, potential or apparent influence over the program.
→ Information/recommendations in the program are evidence‐ and/or guidelines‐based, and opinions of the independent speakers will be identified as such.

21/03/2018
3
Objectives
• Present the new Headache Pathway
• For each step of the pathway, present a clinical pearl and resources
10 steps of the Migraine Pathway
1 Detail the type of migraine
2 Identify and manage the co‐morbidities
3 Review the lifestyle and previous therapeutic trials
4 Explain the migraine diagnosis to patient and set up expectations
5 Train the patient to self‐monitor with a headache diary
6 Plan tailored behavioral interventions
7 Try adapted options for the migraine attack until success is reached
8 Try preventive treatments to reduce frequency of migraine headaches
9 Prevent, detect and withdraw medication overuse
10 Refer to neurology (CAT criteria)

21/03/2018
4
Diagnosing Headache is tough
SNOOPPP
S Systemic
N Neurologic
O Onset
O Older
P Previous
P Postural
P Progressive
P Pregnancy
ID MIGRAINE Migraine
Disabling 2/3 =Very probablymigraine
Sensory hypersensitivity(light sounds, smells)
GI symptoms, nausea, vomiting
Is it a secondary headache? Is it migraine?
What type of migraine is it?
Migrainephenotype
Aura
Frequency
Severity
Overuse
Symptoms
Disability
Pattern
Triggers

21/03/2018
5
Who is this migraineur?
Migraine &
Body
VascularStroke, CAD, Raynaud’s,
POTS, hypertension, low BP
PsychiatricAnxiety, depression, abuse, addiction, PTSD, ADHD, personality disorders
InflammatoryCrohn’s, arthritis, eczema
Other painFibromyalgia, pelvic pain, neck pain, post‐trauma
VestibularMeniere’s, BPPV
RespiratoryAsthma, sleep apnea
NeurologyEpilepsy, MS
OBGYNDysmenorrhea, contraception,
pregnancy, menopause
The Migraine Story
Childhood
Puberty
20‐30 40‐50 60
Pregnancy Menopause
10‐20
(Abuse) Head traumaStressors Overuse Medical dxGenes
Beginning Chronification Current state
Treatment Trials, ED Visits, tests, consultsDisability, guilt, powerlessness
Migraine Identity
Contraception

21/03/2018
6
Explain the migraine diagnosis and set up expectations
KEY MESSAGES
• Migraine is a real neurological disease
• It is common (15% of people, 3d most common disease)
• It can be disabling (2d most disabling disease of ALL)
• It varies from one person to the other
• NO miracle or cure
• No one‐size‐fits all treatment
• Chronic disease, with phases over life
• Management is a mix of behavioral, acute therapy and preventive treatments (three‐pronged)

21/03/2018
7
Migraine Management: 3 tiered
Lifestyle and behavioralCare for your brain
Acute treatment
Treating individual attacks as they come
Preventive treatment
Lower attack frequency
Other resources and websites
• American Migraine Foundation• Migraine.com• Migraine Again• My Daily Migraine • The Migraine World Summit• Migraine Warriors Calgary (Facebook, private)• Move Against Migraine (Facebook US)
• But BEWARE....not everything is good on the web! • If you see the word «cure», be careful
14

21/03/2018
8
Train the patient to self‐monitor with a headache diary: SKILL #1
The goals of the headache diary are to:
• Establish the frequency of headaches of different severity
• Detect patterns and triggers
• Monitor the frequency of acute medication intake, prevent medication overuse
• Observe the efficacy of acute medications (attack control success rate)
• Determine the efficacy of prophylactic treatments (decrease in intensity and frequency of attacks). Some improvement may be subtle at the beginning.
The Headache Diary: our favorite tool

21/03/2018
9
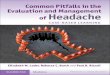
The 0‐1‐2‐3 technique
Headachefree day
Mild Moderate Severe
Intensity Pain free! Mild Moderate Severe
Accompanyingsymptoms
None May beabsent
Present Prominent
Acute treatment None Maybe not needed
Usually works May fail
Impact on function
None Can work Work slowed Workimpossible
Baseline: determine location (including neck), aggravating factors, circadianpattern, presence of sensory hypersensitivity, level of tolerability
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 T
Headache
0 1 2 3*0 0 0 1 1 2 0 0 0 3 2 0 0 0 0 3 3 3* 2 0 0 0 0 1 0 0 1 0 0 3 0
Aura V V
Period X X X X
Lifestyle E E E E E E E E
Tx IBU X X X X X X
Tx: ALMO X X X
Tx: Zomig X X X
Effect acute tx S F S P P F P S S
STABLE Prev Nadolol 80 mg Magnesium 300 mg
NEW #1 TPX 25 50 75 100
Notes
Headache diary: an example
Number of days for each HA severity
0 1 2 3 Tot
19 4 3 5 12
Total number of dayswith any acute medication intake
9
• This person has frequent episodic migraine (12 days per month). There is no medication overuse.
• One day was associated with missed work.
• Some attacks are with visual aura.
• She is exercising, but cannot exercise during bad migraine stretches.
• The attack during the period is worse and difficult to control.
• Using only Ibuprofen does not seem to control number 2s. Zomig seems to work better.
• She does not have clear overuse but she is using close to 10 days per month of acute treatments.
• This person is already taking 2 preventives, nadolol and magnesium.
• She is now trying topiramate (TPX). It is still too early to determine if there has been a benefit. If the
next 2 months show a frequency of 6 days/month, then TPX would seem effective.

21/03/2018
10
The brain is bathed in its bodily environment
9 skills for migraine management
HEADACHESELF‐MANAGEMENTGood
medication use
SleepQuality
Nutrition andhydration
RelaxationStress
Management
TriggerManagement
ExercisePostureRoutine
Pacing LifestyleBalance
Self-Monitoring(Diaries)
CBT

21/03/2018
11
Plan tailored behavioral interventions
Easy Advanced
Sleep Basic tips on sleep hygeneOnline module
CBT, sleep clinic
Nutrition Regular meals, increase protein, reduce processed and high sugar, limit alcohol
Nutrition consultKetogenic dietFODMAP, gluten free, lactose free
Hydration Drink 1‐2 l of water per dayAvoid before bedtime
‐
Caffeine Limit to < 2oo mg/day Stop for 2 months
Exercise Regular and moderateCrossfit and HIIT not very good
Kinesiology or physio consultAthletes
Relaxation Breathing techniques, podcasts, apps
CBT, ACT, full mindfulness training
Pacing Books, simple advice Occupational Therapy eval
Do you need help to educate your patients?
• If you think that it would be helpful for yourpatients to have access to educationalsessions on migraine...
• Please email me at [email protected] the title «Help needed for migraine»

21/03/2018
12
Acute treatment: notes on triptans
• Patients vary in their response (efficacy and sideeffects)
• Try many before diagnosing «triptan non‐responder»
• Monotherapy with SSRI is NOT a contra‐indication
• Sulfa allergy is NOT a contra‐indication
• Raynaud is NOT a contra‐indication

21/03/2018
13
The treat early principle
• Many people delay treatment– «it’s not a migraine»– Financial «save the triptan dose»– Fear of side effects
• Treating early = more success• Be careful IF frequency is over 10/month• Use a diary to monitor as needed
• Refer to our Migraine Canada You Tube videos
Try adapted options for the migraine attack until success is reached
If monotherapy fails, then combination is warranted.
Many patients have 2 types of attacks and may need to tailor their treatment. • Attacks difficult to control include:• Fast rising attacks• Attacks starting during sleep or upon awakening• Attack with prominent nausea or vomiting• Attacks occurring during the menstrual period
If attacks are difficult to control, consider the following approaches:• Combinations (NSAID + triptan taken early together)• Use of adjunct therapy (anti‐emetics)• Use of parenterals (nasal sprays, suppositories, injectors)• Start prophylaxis (may increase efficacy of acute treatments)

21/03/2018
14
My favorite options for tough attacks
• Cambia (diclofenac powder 50 mg)
• Injectable ketorolac 30 mg (should be IM but SC works)
• Indomethacine suppositories
• Zomig nasal spray 5 mg
• Injectable sumatriptan 6 mg
Watch our teaching videos!

21/03/2018
15
Try preventive treatments to reduce frequency of migraine headaches
• Consider if > 6 days/month
• Choose according to comorbidity profile
• Use a headache diary
• 50% chance of success
• Side effects are a problem
• Increase dose (1 month), keep and observe (2 months)
• If successful, keep for 1 year, then reassess
Prevent, detect and withdraw medication overuse
• DO NOT PRESCRIBE NARCOTICS • Use a headache diary• Some patients chronify for other reasons• Stratify the subtype of patient
– Type 1 = easy: recent overuse, no psych, no narcotics– Type 2 = difficult: long history, previous attempt, narcotics, psych problems, addiction
• Start a preventive• Improvement will be partial in most• 10‐30% will not stop or not improve

21/03/2018
16
Indications for onabotulinum Type A
• Chronic migraine (and post‐traumatic)• Failed 2‐3 preventives• 2‐3 cycles to observe response• Success rate is still 50%• Excellent tolerability• Injector Network
Refer to neurology (CAT criteria)
• Enough information on the headache type
• Cluster headache will be expedited
• No urgent secondary headache is seen at CHAMP
• Detail migraine type and previous trial
• Failed at least 2 triptans
• Failed at least 2 preventives
• Be clear if post‐traumatic
• Mention narcotic use

21/03/2018
17
CGRP and migraine Why should we block it? will it cure migraine?
Results of the CGRP antibody trials
• Once per month injection, probably at home
• Mechanism of action is specific to migraine
• AS effective as existing preventives
• Some people respond very well
– 75% less migraine in 30% of patients
• Much better tolerated, almost no side effects
• Effect is seen faster (as early as 1 week!)
• Safety: so far no alarming vascular signal
• Cost is likely to be high (access challenge)
Recommended