GRAND GRAND ROUNDSROUNDS
September 1, 2006September 1, 2006
Denise A. JohnDenise A. John
St. Thomas HospitalSt. Thomas Hospital

CaseCase HPIHPI:: 60 y/o 60 y/o ♂ presents for an eye exam. ♂ presents for an eye exam.
ø ocular c/o’s ø ocular c/o’s
ROSROS:: (+) L temporal headache (+) L temporal headache All other systems unremarkableAll other systems unremarkable
FHXFHX:: Diabetes; HTN, stroke Diabetes; HTN, stroke
SHXSHX:: Quit ETOH ‘04; ø tobacco/IVDA Quit ETOH ‘04; ø tobacco/IVDA
AllergiesAllergies:: NKDA NKDA

Ocular ExamOcular Exam NLPNLP VVA SCA SC CF ‘4ft CF ‘4ft 20/200 20/200
MotilityMotility: Full OU: Full OU 44 IOPIOP 88
PupilsPupils: (+) RAPD OD: (+) RAPD OD

NO VIEW
B-Scan: Funnel-shaped retinal detachment


Differential Differential DiagnosisDiagnosis
InfectiousInfectious Indolent CMV retinitis Indolent CMV retinitis Toxoplasma retinitis Toxoplasma retinitis Acute retinal necrosis Acute retinal necrosis
(ARN) (ARN) Progressive outer Progressive outer
retinal necrosis (PORN) retinal necrosis (PORN) Choroidal Choroidal
pneumocystosispneumocystosis Cryptococcal choroiditisCryptococcal choroiditis TuberculosisTuberculosis CandidiasisCandidiasis SyphilisSyphilis
NeoplasticNeoplastic Ocular lymphomaOcular lymphoma MetastasisMetastasis
InflammatoryInflammatory SarcoidosisSarcoidosis VasculitidesVasculitides

More Info…More Info… PMHXPMHX::
HIV/AIDS (Dx ’04)HIV/AIDS (Dx ’04) CD4: 155 cells/mmCD4: 155 cells/mm33
(5/05)(5/05) HIV nephropathyHIV nephropathy Hepatitis CHepatitis C Chronic anemiaChronic anemia HTNHTN ChickenpoxChickenpox
POHXPOHX:: S/p steel injury ODS/p steel injury OD HZO OS (5/05)HZO OS (5/05)
ConjunctivitisConjunctivitis KeratitisKeratitis UveitisUveitis Post-herpetic NeuralgiaPost-herpetic Neuralgia
MEDSMEDS:: Acyclovir 400mg QID; Acyclovir 400mg QID;
HAART; lisinopril; atenolol; HAART; lisinopril; atenolol; bactrim; Refresh PMbactrim; Refresh PM
External ExamExternal Exam:: Left hypo-pigmented scar: Left hypo-pigmented scar:
CNVCNV11 distributiondistribution LUL Entropion & trichiasisLUL Entropion & trichiasis
SLESLE: : OD:OD: Shallow AC; 360 Shallow AC; 360° °
posterior synechiae; posterior synechiae; white white cataractcataract
OS:OS: PEE; posterior PEE; posterior synechiae;synechiae;
ø AC rxn; 2-3+ NSC/3-4+ ø AC rxn; 2-3+ NSC/3-4+ PSC; PSC;
ø vitritisø vitritis

Epidemiology: Epidemiology: HIVHIV
40 million individuals infected worldwide40 million individuals infected worldwide
~~ 900,000 in the U.S. 900,000 in the U.S.
70-80% treated for a HIV-related eye 70-80% treated for a HIV-related eye disorderdisorder CD4 count may be used to predict the CD4 count may be used to predict the
occurrence of specific ocular infectionsoccurrence of specific ocular infections

CD4 Count & Ocular CD4 Count & Ocular InfectionsInfections
< 500 cells/mm< 500 cells/mm33
Kaposi sarcomaKaposi sarcoma TuberculosisTuberculosis LymphomaLymphoma
< 250 cells/mm< 250 cells/mm33
PneumocystosisPneumocystosis ToxoplasmosisToxoplasmosis
< 100 cells/mm< 100 cells/mm33
Conjunctival/retinal Conjunctival/retinal microvasculopathymicrovasculopathy
CMV retinitisCMV retinitis Most commonMost common
VZV retinitisVZV retinitis 22ndnd most common most common
CryptococcosisCryptococcosis MicrosporidiosisMicrosporidiosis

CMV RetinitisCMV Retinitis Occurs in Occurs in
immunocompromisedimmunocompromised Slow progressionSlow progression Starts in periphery Starts in periphery Spreads along retinal Spreads along retinal
vasculature towards vasculature towards posterior poleposterior pole
Dense Dense white/granular white/granular opacification (full-opacification (full-retinal thickness) retinal thickness)
HemorrhageHemorrhage Mild vitritisMild vitritis

Acute Retinal Acute Retinal NecrosisNecrosis
Occurs in Occurs in immunocompetentimmunocompetent >> 1 foci of full-thickness 1 foci of full-thickness
retinal necrosis with retinal necrosis with discrete bordersdiscrete borders
Spreads 360Spreads 360° ° circumferentially in circumferentially in peripheral retinaperipheral retina
Posterior pole Posterior pole involvement is spared involvement is spared until lateuntil late
VasculitisVasculitis Prominent inflammatory Prominent inflammatory
reaction (AC & vitreousreaction (AC & vitreous))

Progressive Progressive Outer Outer
Retinal Retinal NecrosisNecrosis

PORNPORN Rare form of necrotizing herpetic Rare form of necrotizing herpetic
retinopathy retinopathy
First described by Forster et al. (1990)First described by Forster et al. (1990) 2 pts: Fulminant outer retinal necrosis sparing 2 pts: Fulminant outer retinal necrosis sparing
the inner retina & vasculaturethe inner retina & vasculature
Occurs in the immunocompromised:Occurs in the immunocompromised: Immunosuppressed organ-transplant recipientsImmunosuppressed organ-transplant recipients Immune-deficient individuals:Immune-deficient individuals:
CancerCancer Advanced AIDSAdvanced AIDS

PathogenesisPathogenesis Varicella-Zoster VirusVaricella-Zoster Virus
Virus remains latent in sensory gangliaVirus remains latent in sensory ganglia Reactivated during times of loss of T-cell Reactivated during times of loss of T-cell
regulatory controlregulatory control Difficult to isolate/grow in-vitroDifficult to isolate/grow in-vitro
Only organism isolated in the retina via culture, Only organism isolated in the retina via culture, PCR & direct fluorescent antibody assayPCR & direct fluorescent antibody assay

PORNPORN Engstrom, et al. PORN: A variant of Engstrom, et al. PORN: A variant of
necrotizing herpetic retinopathy in necrotizing herpetic retinopathy in patients with AIDS. Ophth 1994. patients with AIDS. Ophth 1994. 38 38 ♂ ♂ pts (65 eyes): pts (65 eyes): CD4 count: 21 cells/mmCD4 count: 21 cells/mm3 3 (0-130 (0-130 cells/mmcells/mm33))
Largest study on PORNLargest study on PORN Retrospective chart reviewRetrospective chart review
Median f/u 3 months (0-10 months)Median f/u 3 months (0-10 months) Objective: Characterize the clinical features & courseObjective: Characterize the clinical features & course

PORNPORN History of cutaneous zoster History of cutaneous zoster : 67% : 67%
(22/33 pts)(22/33 pts) 41%: involved CNV41%: involved CNV11
12 of 15 pts: PORN occurred after a median of 12 of 15 pts: PORN occurred after a median of 2 months (2 months – 2 years)2 months (2 months – 2 years)
3 of 15 pts: PORN occurred concurrently3 of 15 pts: PORN occurred concurrently
12 of 38 pts: Taking oral acyclovir at the 12 of 38 pts: Taking oral acyclovir at the time PORN was diagnosedtime PORN was diagnosed 50%: Acyclovir 800mg 5x/day50%: Acyclovir 800mg 5x/day

Clinical FeaturesClinical Features Ocular complaintsOcular complaints
vision: Most common (54% eyes)vision: Most common (54% eyes) Constriction of visual fields (28% eyes)Constriction of visual fields (28% eyes) Floaters (11% eyes)Floaters (11% eyes) Pain (6% eyes)Pain (6% eyes)
7 pts with unilateral symptoms had 7 pts with unilateral symptoms had asymptomatic disease in the fellow eyeasymptomatic disease in the fellow eye

Clinical FeaturesClinical Features Usually bilateral diseaseUsually bilateral disease
28 of 38 pts: Unilateral disease at diagnosis28 of 38 pts: Unilateral disease at diagnosis 22ndnd eye became affected in 17 pts eye became affected in 17 pts median of 10 median of 10
days after diagnosis (3 days – 4 weeks) in 6 ptsdays after diagnosis (3 days – 4 weeks) in 6 pts
Intraocular inflammation is minimal to Intraocular inflammation is minimal to absentabsent 23 of 60 eyes: Anterior segment inflammation23 of 60 eyes: Anterior segment inflammation
61% mild AC reaction 61% mild AC reaction 11% keratic precipitates (fine, white deposits)11% keratic precipitates (fine, white deposits) 6% posterior synechiae6% posterior synechiae
15 of 61 eyes: Vitreous inflammation15 of 61 eyes: Vitreous inflammation 80% mild vitritis 80% mild vitritis

Clinical FeaturesClinical Features Multifocal, discrete lesions of the outer Multifocal, discrete lesions of the outer
retina retina rapidly progress to confluence & rapidly progress to confluence & full-thickness retinal involvementfull-thickness retinal involvement
Perivenular lucencyPerivenular lucency

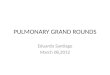
Clinical FeaturesClinical Features Characteristic Characteristic
macular lesionmacular lesion:: Parafoveal Parafoveal
opacification with a opacification with a “cherry-red spot”“cherry-red spot”
Ø contiguous with Ø contiguous with peripheral lesionsperipheral lesions
Peripheral lesions Peripheral lesions ++ posterior poleposterior pole Zone 1: 32% eyesZone 1: 32% eyes
øø lesions only in zone 1 lesions only in zone 1 Zone 2: 72% eyesZone 2: 72% eyes Zone 3: 86% eyesZone 3: 86% eyes
28% eyes all 3 zones28% eyes all 3 zones

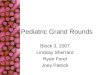
Clinical FeaturesClinical Features Disease Disease
quiescencequiescence Dense white Dense white
plaques: “cracked plaques: “cracked mud” appearancemud” appearance
Atrophic areas Atrophic areas ++ holesholes

Clinical FeaturesClinical Features Other manifestationsOther manifestations::
11 of 65 eyes: 11 of 65 eyes: Optic nerve abnormalitiesOptic nerve abnormalities Disc swellingDisc swelling HyperemiaHyperemia AtrophyAtrophy
11 of 29 pts: 11 of 29 pts: Afferent pupillary defectAfferent pupillary defect 13 of 61 eyes: 13 of 61 eyes: Retinal vasculopathyRetinal vasculopathy
Vascular sheathing/occlusionVascular sheathing/occlusion Areas within or near retinal necrosisAreas within or near retinal necrosis

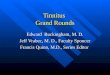
FA: PORNFA: PORN Walton et al. FA in PORN. Walton et al. FA in PORN.
Retina 16: 1996 Retina 16: 1996 EarlyEarly: Microvascular : Microvascular
changes changes
equatorial & peripheral equatorial & peripheral retinaretina
Confluent retinal diseaseConfluent retinal disease: : retinal vasculature & loss of retinal vasculature & loss of capillaries; RPE damage; capillaries; RPE damage; choriocapillaris leakagechoriocapillaris leakage
ReactivationReactivation: Brush-fire : Brush-fire pattern of choroidal leakage pattern of choroidal leakage at lesion borderat lesion border
PORN = RetinochoroiditisPORN = Retinochoroiditis

Management: Management: PORNPORN
Exact combination of antivirals & duration Exact combination of antivirals & duration of treatment not knownof treatment not known
Guided by anecdotal informationGuided by anecdotal information
Herpes-zoster traditionally treated with Herpes-zoster traditionally treated with acyclovir; however, may not be effective in acyclovir; however, may not be effective in pts treated long-term with the oral form 2pts treated long-term with the oral form 2° ° to resistanceto resistance

ManagementManagement Moorthy et al. Management of VZVR in Moorthy et al. Management of VZVR in
AIDS. Br J Ophth, 1997. 20 pts (39 eyes); AIDS. Br J Ophth, 1997. 20 pts (39 eyes); 11 pts using oral acyclovir at time of 11 pts using oral acyclovir at time of diagnosisdiagnosis
Retrospective chart reviewRetrospective chart review median f/u 6 months (1-26 months)median f/u 6 months (1-26 months)
Objective: Investigate visual outcomeObjective: Investigate visual outcome
2 week IV treatment2 week IV treatment:: Acyclovir (10mg/kg Q8h) Acyclovir (10mg/kg Q8h) Ganciclovir (5mg/kg Q12h x 2 weeks; then Ganciclovir (5mg/kg Q12h x 2 weeks; then
5mg/kg/day) 5mg/kg/day) Foscarnet (180mg/kg/day in 2 or 3 divided Foscarnet (180mg/kg/day in 2 or 3 divided
doses) doses) Ganciclovir + foscarnetGanciclovir + foscarnet

ManagementManagement ResultsResults::
Rates of NLP Rates of NLP :: acyclovir (9 of 10 eyes) & acyclovir (9 of 10 eyes) & foscarnet (3 of 5 eyes)foscarnet (3 of 5 eyes)
Ø VØ VAA > 20/200 > 20/200 Rates of NLP Rates of NLP : : combination therapy (5 of 18 combination therapy (5 of 18
eyes) & ganciclovir (2 of 6 eyes)eyes) & ganciclovir (2 of 6 eyes) VVAA > 20/200 > 20/200
Combination therapy: 3 of 18 eyesCombination therapy: 3 of 18 eyes Ganciclovir: 1 of 6 eyesGanciclovir: 1 of 6 eyes
Conclusion: Treatment with IV combination Conclusion: Treatment with IV combination therapy or ganciclovir associated with a therapy or ganciclovir associated with a better final vbetter final vAA VS acyclovir or foscarnet VS acyclovir or foscarnet alonealone

ManagementManagement Ciulla, et al. PORN: Successful treatment Ciulla, et al. PORN: Successful treatment
with combination antiviral therapy. Ophth with combination antiviral therapy. Ophth Surgery & Lasers. 1998. Surgery & Lasers. 1998. 6 pts with AIDS6 pts with AIDS
Retrospective chart reviewRetrospective chart review Median f/u 29 weeks (27 -38 weeks)Median f/u 29 weeks (27 -38 weeks)
Objective: Assess 2-drug combination therapyObjective: Assess 2-drug combination therapy
IV Treatment duration: median 29 weeks (27-IV Treatment duration: median 29 weeks (27-38 weeks)38 weeks)
Ganciclovir (5mg/kg Q12h) + acyclovir (500mg/mGanciclovir (5mg/kg Q12h) + acyclovir (500mg/m2 2
Q8h)Q8h) Foscarnet (60mg/kg Q8-12h) + ganciclovirFoscarnet (60mg/kg Q8-12h) + ganciclovir Foscarnet + acyclovirFoscarnet + acyclovir

ManagementManagement ResultsResults::
All 6 pts had resolution of diseaseAll 6 pts had resolution of disease 1 of 6 pts had recurrence1 of 6 pts had recurrence At diagnosis 3 of 12 eyes without disease At diagnosis 3 of 12 eyes without disease
remained uninvolvedremained uninvolved 10 of 12 eyes developed RD10 of 12 eyes developed RD
Conclusion: Prolonged combination therapy Conclusion: Prolonged combination therapy arrested progression of retinitis; maintained arrested progression of retinitis; maintained remission & prevented fellow eye remission & prevented fellow eye involvement; does not prevent retinal involvement; does not prevent retinal detachmentdetachment Role of ganciclovir intraocular implant & oral Role of ganciclovir intraocular implant & oral
agents in combination therapy is unclearagents in combination therapy is unclear

ManagementManagement Intravitreal injection (ganciclovir & Intravitreal injection (ganciclovir &
foscarnet);foscarnet);
intravitreal ganciclovir implantintravitreal ganciclovir implant No protection for fellow eyeNo protection for fellow eye

ComplicationsComplications Retinal necrosisRetinal necrosis
Retinal tears/holesRetinal tears/holes
Rhegmatogenous retinal detachmentRhegmatogenous retinal detachment

ManagementManagement Prophylactic laser retinopexyProphylactic laser retinopexy
Engstrom et al. 1994Engstrom et al. 1994 14 of 54 eyes: Laser 14 of 54 eyes: Laser ~~ 1 week after diagnosis 1 week after diagnosis
93% developed a RD93% developed a RD Median interval Median interval ~~ 3 weeks 3 weeks
Ø significant difference: laser VS no laser: Ø significant difference: laser VS no laser: Zone of involvement of RDZone of involvement of RD Extent of RDExtent of RD Interval from diagnosis to RDInterval from diagnosis to RD

ManagementManagement Rhegmatogenous retinal detachmentRhegmatogenous retinal detachment
Engstrom et al. 1994Engstrom et al. 1994 43 of 65 eyes: Median interval 4 weeks43 of 65 eyes: Median interval 4 weeks
No relationship to extent of disease or disease No relationship to extent of disease or disease activityactivity
Vitrectomy/endolaser/silicone oilVitrectomy/endolaser/silicone oil 16 of 43 eyes: Retinas successfully attached 16 of 43 eyes: Retinas successfully attached
in all eyesin all eyes Re-detached in 4 eyesRe-detached in 4 eyes NLP in 56% (laser) VS 63% (no laser)NLP in 56% (laser) VS 63% (no laser)

PrognosisPrognosis Visual prognosis is poorVisual prognosis is poor
Macular involvementMacular involvement Ineffectiveness of antiviral agentsIneffectiveness of antiviral agents
RecurrenceRecurrence Engstrom, et al. 1994Engstrom, et al. 1994
At least 10 pts despite being on maintenance therapyAt least 10 pts despite being on maintenance therapy Characterized by development of new disease fociCharacterized by development of new disease foci
In 6 pts associated with In 6 pts associated with discontinuation/reduction in maintenance dose; discontinuation/reduction in maintenance dose; median time to recurrence was median time to recurrence was
2 weeks (1-6 weeks)2 weeks (1-6 weeks)
~ 50% of individuals ~ 50% of individuals deceased 5 months after deceased 5 months after diagnosisdiagnosis

Back To Our Back To Our Patient…Patient…
Patient admitted to medicinePatient admitted to medicine Infectious disease consultedInfectious disease consulted
Received IV foscarnet (40mg/kg Q12 x 14 days)Received IV foscarnet (40mg/kg Q12 x 14 days) øø Progression of lesions Progression of lesions VVAA improved to 20/60 (+1.75) improved to 20/60 (+1.75) Discharged on oral acyclovir 800mg 5x dayDischarged on oral acyclovir 800mg 5x day

Take Home Take Home Points…Points…
Progressive outer retinal necrosis is a Progressive outer retinal necrosis is a rapidly progressive necrotizing retinitis rapidly progressive necrotizing retinitis occurring in immunocompromised occurring in immunocompromised individuals, esp. AIDS ptsindividuals, esp. AIDS pts
Management is anecdotal: use of high-Management is anecdotal: use of high-dose IV anti-virals may be beneficialdose IV anti-virals may be beneficial
Poor visual prognosisPoor visual prognosis

ReferencesReferences E-Medicine: Ocular manifestations of HIVE-Medicine: Ocular manifestations of HIV Forster et al. Rapidly PORN in AIDS. Am J Ophth 110: 341. Forster et al. Rapidly PORN in AIDS. Am J Ophth 110: 341.
19901990 Moorthy et al. Management of VZV retinitis in AIDS. Br J Moorthy et al. Management of VZV retinitis in AIDS. Br J
Ophth, 1997.Ophth, 1997. Walton et al. Fluorescein angiography in PORN. Retina 16: Walton et al. Fluorescein angiography in PORN. Retina 16:
19961996 Ciulla, et al. The PORN: Successfully treatment with Ciulla, et al. The PORN: Successfully treatment with
combination antiviral therapy. Ophth Surgery & Lasers. combination antiviral therapy. Ophth Surgery & Lasers. 19981998
BCSC. Retina & Vitreous. AAO. 2004-05BCSC. Retina & Vitreous. AAO. 2004-05 BCSC. Uveitis & Intraocular Inflammation. AAO. 2004-05BCSC. Uveitis & Intraocular Inflammation. AAO. 2004-05 Yanoff. Ophthalmology, 2Yanoff. Ophthalmology, 2ndnd Ed. Mosby. 1121-22 Ed. Mosby. 1121-22 Kanski. Clinical Ophthalmology, 5Kanski. Clinical Ophthalmology, 5thth Ed. Butterworth Ed. Butterworth
Heinemann. 288-93. 2003Heinemann. 288-93. 2003
Recommended