Embed Size (px)
DESCRIPTION
Pediatric Grand Rounds. Block 3, 2007 Lindsay Sherrard Ryan Foret Joey Patrick. What disease?. costs the US $3.5 billion each year? necessitates the average household to have 4-8 medicines? is the most common human illness?. Viral Upper Respiratory Infections in Kids. Epidemiology - PowerPoint PPT Presentation
Citation preview

Pediatric Grand Rounds
Block 3, 2007Lindsay Sherrard
Ryan ForetJoey Patrick

What disease?
• costs the US $3.5 billion each year?
• necessitates the average household to have 4-8 medicines?
• is the most common human illness?


Viral Upper Respiratory Infections in Kids
• Epidemiology• Pathogenesis• Clinical Features• Complications• Treatment• Prevention

Epidemiology of the Common Cold
• Children are the main reservoir• Infants: average 6 per year• Older kids: average 4-8 per year• Incidence declines with age except for a
spike in adults in their 20s• Families with the oldest child aged 1-4
are at higher risk• Families with a child in daycare or
school are at higher risk

So what causes colds?

Causes of Viral URIs• Rhinovirus: over 100 subtypes, cause
10-40% of colds (adults)• Coronavirus: 20% of colds (adults)• RSV: 10% of colds (adults)• Influenza, parainfluenza, adenovirus
cause more systemic symptoms• Enteroviruses (echovirus,
coxsackievirus) usually cause fever without cold symptoms
• Human metapneumovirus (HMPV)

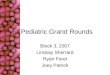
Seasonal Variations

Seasonal Variations
• Generally unknown why there are worldwide seasonal variations.
• No change in host resistance to rhinovirus based on exposure to cold climate
• Possibly due to variations in living conditions, schooling, and crowding

Seasonal Variations• Rhinovirus: early fall, spring• Parainfluenza: late fall• RSV: winter• Influenza: winter• Coronaviruses: winter• Adenovirus: fall, winter, spring• Enteroviruses: summer• Human metapneumovirus: late winter,
early spring

Quiz Question # 1
• You are asked to talk to local child care providers about infection control measures. You advise them that the single best intervention to reduce the spread of “common colds” to other children in the center is to:

Quiz Question # 1
• A. Exclude all ill children from the center.
• B. Have all providers wear masks.• C. Isolate sick children from the
center.• D. Limit outside playtime during the
winter months.• E. Wash hands and toys.

Quiz Question # 1
• E. Wash hands and toys.

Transmission

Transmission
• Rhinovirus→ nasal secretions • very small amount in saliva• Direct hand to hand contact and
contact with nasal mucosa or conjunctiva
• Large particle droplets on nasal mucosa or conjunctiva
• Inhalation of small particle aerosols (especially RSV)

Transmission
• Rhinovirus can survive 2 hours on the hands
• Rhinovirus can survive up to several days on hard surfaces, less on porous surfaces
• Children tend to shed more virus and for longer time

Pathophysiology

Pathophysiology• Symptoms begin 1-2 days (or up to 7
days) after inoculation• Viral shedding begins 12 hours after
inoculation, peaks at 48 hours, and may continue up to 3 weeks for rhinovirus
• Symptoms correlate with influx of PMNs into mucosa and submucosa (with immune response)
• Colored mucus is from neutrophil enzymatic activity but has no correlation with positive bacterial cultures

Pathophysiology• Bradykinins, IL-8, and other
inflammatory mediators increase • Histamine levels are not elevated• Elevated albumin levels suggest leaky
vasculature• Most symptoms are due to immune
response, not to destruction of epithelial cells by viral replication.
• Adenovirus and influenza-A are more cytotoxic than rhinovirus and coronavirus

Pathophysiology
• Immune response also explains asthma exacerbations during viral URIs
• Exacerbation may last up to 4 weeks
• Unknown if inflammatory mediators are produced locally in the lower respiratory tract or if they act from a distance

Quiz Question # 2
• A parent is concerned that her 4-year-old son “always has a cold.” Given what you know about the frequency of colds and the duration of their symptoms, what is the minimum number of “sick days” per year that would be considered excessive for a typical child?

Quiz Question # 2
• A. 75• B. 100• C. 125• D. 150• E. 175

Quiz Question # 2
• D. 150
• Having cold symptoms up to 140 days per year is normal for a young child.

Clinical Syndromes of Viral Respiratory Infections
• Common Cold• Sinusitis• Acute otitis media• Otitis media with effusion• Pharyngitis• Croup• Bronchiolitis• Pneumonia

Common Cold• Nasal discharge, often colored• Low grade fever for the first 2-3 days• Sore, scratchy throat (often the first
feature in older kids)• Cough• Irritability• Difficulty sleeping• Decreased appetite• Symptoms usually last 2 weeks in
children (1 week in adults)

Physical Exam Findings

Physical exam findings
• Inflamed, swollen nasal mucosa and pharynx
• Middle ear effusion• Cervical lymphadenopathy• Conjunctivitis

Quiz Question # 3
• A 3-year-old boy is coming to see you with what his mother describes as “probably just a cold.” On the phone, she said that he has had a runny nose and now has a worsening cough. Which piece of this patient’s past medical history would raise the greatest concern?

Quiz Question # 3
• A. Asthma• B. Croup• C. Otitis media• D. Sinusitis• E. Tonsillitis

Quiz Question # 3
• A. Asthma

Case 1: DB
• 12y BM with history of asthma presented with wheezing, cough and fever for one day
• Had runny nose for two days• Cough associated with chest pain
and vomiting x 2• Still coughing and wheezing after 3
albuterol nebs in the ER

Case 1: DB• PMH:
– asthma with one hospitalization at age 3 – irregular heartbeat with negative work-up
• SH: Lives with mom in carpeted trailer, no smokers, outdoor dog, doing well in the 7th grade
• FH: asthma-dad and uncle• Home meds: albuterol inhaler at home,
uses about once monthly; ran out of singulair and advair 2 months ago

Case 1: DB
• Vitals: T 102, P 95, R 18, SaO2 95 on room air
• PE: accessory muscle use, bilateral wheezing
• Labs: WBC 9.6, Hgb 12.7, platelets 241

Case 1: DB

Case 1: DB
• Admitted for asthma exacerbation secondary to viral URI
• On HD #2, his O2 Sat dropped in the 80s and he required up to 5L NC
• ABG: 7.40/33/85/20 on 5L NC

Case 1: DB
• Solu-medrol dose in ER• Prelone 1mg/kg/day• Resumed advair and singulair• Albuterol nebs, then inhaler• Finally improved on HD #3 and
was discharged on HD#4 • Told to monitor his peak flow,
especially when he gets a cold

Complications of the Common Cold
• Otitis Media• Sinusitis• Pharyngitis• Croup• Epistaxis• Lower respiratory infection
(bronchiolitis, pneumonia)• Asthma exacerbation

Signs a Cold may be Complicated
• Fever > 102• Fever still present after 3 days• “Double sickening”• Severe cough or respiratory
distress• No improvement within 10-14 days• Vomiting

Treatment of the Common Cold (Under age 2)
• Supportive therapy only is best• Hydration• Elevate head of bed• Humidifier• Nasal saline drops with bulb suction• Clearing the nose is important to
prevent dehydration from less PO intake• Fever/pain control with:
-Tylenol (over age 2 months) -Motrin (over age 6 months)
• Treat bronchospasm with bronchodilator

Quiz Question # 4
• Your parent information sheet “Colds in Infants” includes instructions on correct use of a bulb syringe. Normal saline, rather thans 1/8% phenylephrine drops (“Little Noses”), is recommended because:

Quiz Question # 4
• A. 4-month-old infants are primarily mouth breathers.
• B. Phenylephrine causes rebound congestion.
• C. Phenylephrine causes vasodilation.• D. Phenylephrine has been associated
with cardiomyopathy.• E. Phenylephrine must be given for 72
hours to be effective.

Quiz Question # 4
• B. Phenylephrine causes rebound congestion.

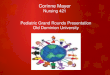
Instructions on using a bulb syringe
• Place the infant on his or her back. Using a clean nose dropper, place 1 to 2 drops of saline solution in each nostril. Wait two minutes.
• Squeeze and hold the bulb syringe to remove the air. Gently insert the tip of the bulb syringe into one nostril, and release the bulb. The suction will draw mucus out of the nostril into the bulb.
• Squeeze the mucus out of the bulb into a tissue.

Instructions on using a bulb syringe
• Repeat suction process several times in each nostril until most mucus is removed.
• Wash the dropper and bulb syringe in warm, soapy water. Rinse well, and squeeze to remove any water.
• The bulb syringe can be used two to three times per day as needed to remove mucus. It is best to do this before feeding; the saline and suction process can cause vomiting after feeding.
• http://www.cincinnatichildrens.org/health/info/newborn/home/suction.htm

Instructions on using a bulb syringe

Treatment of the Common Cold (Over age 2)
• Supportive therapy only is best• Hydration, chicken soup• Elevate head of bed• Humidifier• Nasal saline spray• Fever/pain control with:
-Tylenol (over age 2 months) -Motrin (over age 6 months)
• Treat bronchospasm with bronchodilator• Can consider cough/cold meds with
careful dosing guidance

Why not a little….

Do no harm…• Cough and cold medicines are
associated with fatalities in children under age two, presumably by accidental overdose.
• Metabolism and clearance is unknown and probably varies by age and by individual.
• The recommended dosing of these medicines has not been set by the FDA for children under two.

Do no harm…
• Cough and cold medicines have not been shown to relieve symptoms in kids of any age.
• In 2000, 5% of poison exposures reported to poison control were cough/cold preparations

Do no harm…

Antihistamines• Thought to work by anticholinergic effect• No difference in symptoms compared to
placebo in randomized controlled trials• Benefit: sedation in some kids, helps
them sleep instead of cough• Adverse effects: paradoxical agitation,
respiratory depression, hallucinations, thickened secretions (which may exacerabate asthma)

Antihistamines
• Equivocal data in adults showing less sneezing and nasal discharge but no decrease in total symptom score
• Consider use in patients older than 12 months with careful dosing, realizing the only benefit may be sedation

Decongestants (systemic)• No studies demonstrating efficacy in
children• Adverse effects: tachycardia,
palpitations, elevated DBP, nausea• In adults, shown to give a small
improvement in total symptom score and nasal patency
• Also shown to reduce cough symptoms in adults when combined with 1st generation antihistamine
• Not indicated, except possibly in teenagers

Decongestants (topical)
• Available as phenylalanine or ipratropium nasal spray
• May cause rebound congestion, which is particularly dangerous in babies
• Consider for older children, for 72 hours or less

Antitussives
• Several randomized trials with codeine, dextromethorphan, and placebo show no differences in symptoms
• Adverse effects: abuse potential, respiratory depression (dextromethorphan, hydrocodone, and codeine), insomnia (dextromethorphan), preventing asthmatics from coughing up mucus

Antitussives
• In adults, some studies show benefit from dextromethorphan, but there is no proven benefit for codeine in treating cough caused by the common cold
• Remind parents that cough is a protective reflex

Expectorants
• No studies in children show benefit• In adults, they may cause
perception of thinner secretions but no proven difference in quality or volume of secretions

Antivirals
• Intranasal interferon-alpha-2b has been studied in adults and looks promising, but much more research needs to be done

Zinc
• Studies in children and adults have conflicting results. Some studies do show more rapid resolution of symptoms with frequent zinc lozenges or suspensions, but most studies show no benefit
• Adverse effects: bad taste, nausea, sore throat, diarrhea
• Side effects likely outweigh possible benefits

Vitamin C• Has not been shown to reduce duration
or severity of colds in children or adults.• When taken regularly, at 200mg per day
or more as prophylaxis before cold symptoms it reduces duration of cold by 13% in children and by 8% in adults
• Prophylactic vitamin C reduces the incidence of colds by 50% for those routinely doing severe exercise in sub-arctic conditions
• Data not significant to recommend daily vitamin C supplementation for everyone

Echinacea
• Randomized trial shows no benefit in treating the common cold
• Adverse effect: rash• No shown benefit for treatment or
prevention in adult studies either• Data do not support using
Echinacea for the common cold

Prevention
• Handwashing• Virucidal agents such as iodine,
phenol/alchohol (Lysol)• Avoidance of touching mucous
membranes• Sneezing/coughing into a tissue• ? Exercise ? (shown to help
prevent colds in one adult study)

Prevention

Case 2: MV

Case 2: MV

Case 2: MV

Case 2: MV

Case 2: MV

Case 2: MV

Quiz Question # 5
• Why is it unlikely that a vaccine ever will be developed to prevent colds?

Quiz Question # 5
• A. Immunity to one viral serotype does not confer complete protection against others.
• B. More than 100 different viruses cause the common cold.
• C. There are numerous antigenic serotypes.
• D. A, B, and C.• E. B and C only.

Quiz Question # 5
• D. A, B, and C.

Take Home Points
• Watch for atypical presentations and “double sickening” that may be signs of more serious illness
• Avoid cough/cold meds in children less than 2
• Cough/cold meds not proven to work in any age kids

Take Home Points
• Ask parents what OTC meds they are giving to help avoid accidental overdose by additive medications
• Encourage single ingredient medications to prevent overdose
• Educate parents about what to expect with a typical cold and what treatments have been shown to best relieve symptoms

When viral URIs get admitted… We’ll be ready to send them home!

References• Crowe JE. “Human Metapneumovirus
Infections,” UpToDate, 2007.• Douglas RM et al. “Vitamin C for preventing
and treating the common cold.” Cochrane Database Syst Rev. 2004 Oct 18;(4):CD000980.
• Friedman ND and Sexton DJ. “The Common Cold in Adults,” UpToDate, 2007.
• Hay CM. “Microbiology and Pathogenesis of Rhinovirus Infections,” UpToDate, 2007.
• Hay CM. “Treatment and Prevention of Rhinovirus Infections,” UpToDate, 2007.

References• “Infant deaths associated with cough and cold
medications--two states, 2005.” MMWR Morb Mortal Wkly Rep. 2007 Jan 12;56(1):1-4.
• Kelly LF. “Pediatric Cough and Cold Preparations,” Pediatrics in Review. Vol.25 No.4 April 2004, pp.115-123.
• Munoz FM. “Epidemiology and Clinical Manifestations of Rhinovirus Infections in Children,” UpToDate, 2007.
• Pappas DE and Hendly JO. “The Common Cold in Children,” UpToDate, 2007.
• Simasek M and Blandino DA. “Treatment of the Common Cold,” American Family Physician. Vol. 75:4.
• Wald ER. “Clinical Features, Evaluation, and Diagnosis of Acute Bacterial Sinusitis in Children,” UpToDate, 2007.