Gail YappAssistant SecretaryAcute Care Reform
The future of subacute care in view of the report of the National Health and Hospitals Reform Commission
Second National Transition Care ForumCanberra, November 2009
Outline
• Subacute care in the health system and its benefits for patients.
• Australian Government commitmentand the National Partnership.
• Challenges.
• NHHRC proposals.
• Opportunities and next steps.
Strength under challenge
Increases in:– demand for health and hospital services;– costs and expenditure services;– inequities in access and outcomes.Concerns about:– safety and quality;– workforce shortages;– inefficiencies; and– fragmented responsibility.
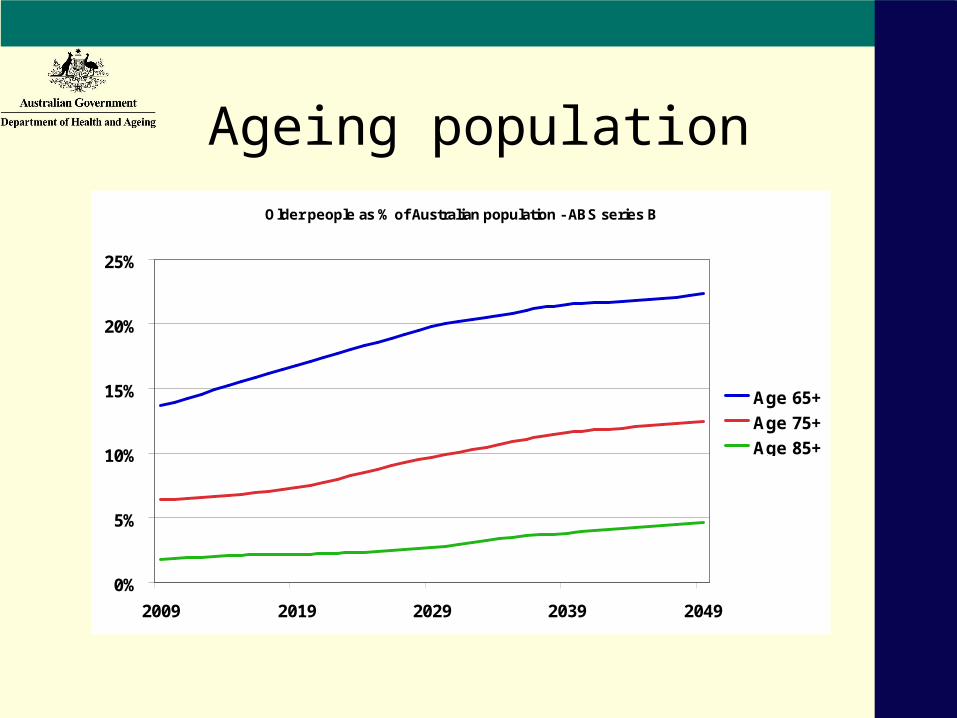
Ageing populationOlder people as % of Australian population - ABS series B
0%
5%
10%
15%
20%
25%
2009 2019 2029 2039 2049
Age 65+
Age 75+
Age 85+
Hospital use by people aged 65+
In the 10 years to 2005-06:
• separations for people 65+ increased from 30% to 36% of all separations; and
• patient days for people 65+ increased from 47% to 49% of all patient days.
Total separations increased 41% yet:
• separations, people aged 75-84, increased 98%;
• separations, people aged 85+, increased 109%.
Subacute care: benefits for the patient and the health system
• Improved patient outcomes.
• Restored independence.
• Acute and community care linked.
• Reduced hospital and residential aged care admissions.
• Cost effective care.
Outcomes are improving
E.g., data from Australian Rehabilitation Outcomes Centre show:– improving overall health outcomes;– decreasing lengths of stay;– increased aggregate functional
improvement; and– increased efficiency.
Not only more but better
Commonwealth, states and territories
working for change todirect resources to
• the right care,• at the right time• in the right place.
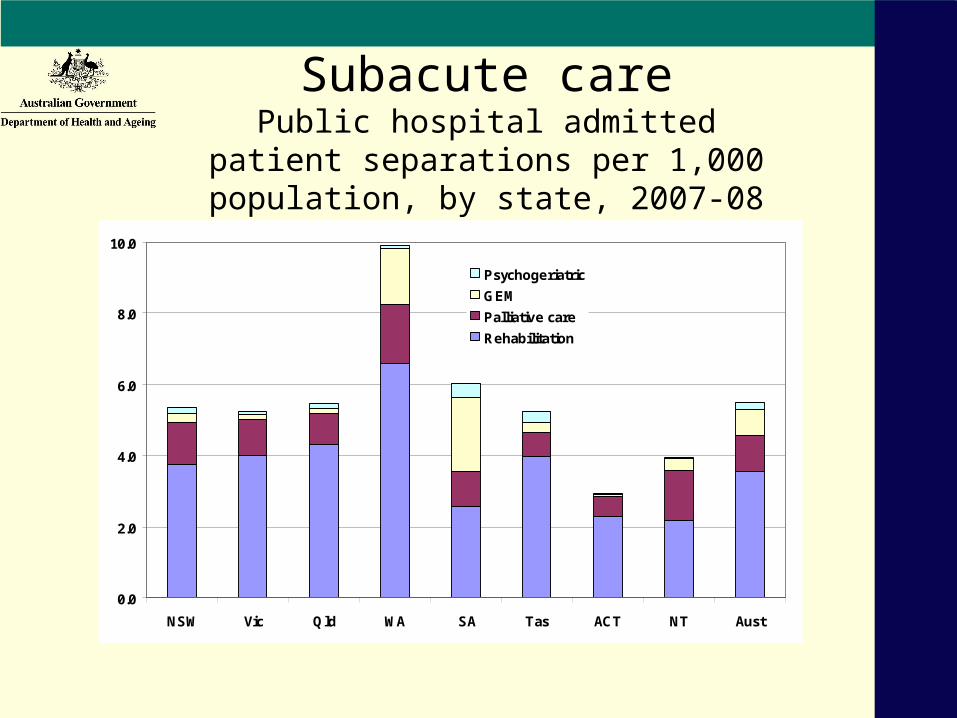
Subacute carePublic hospital admitted patient separations
per 1,000 population, by state, 2007-08
0.0
2.0
4.0
6.0
8.0
10.0
NSW Vic Qld WA SA Tas ACT NT Aust
Psychogeriatric
GEM
Palliative care
Rehabilitation
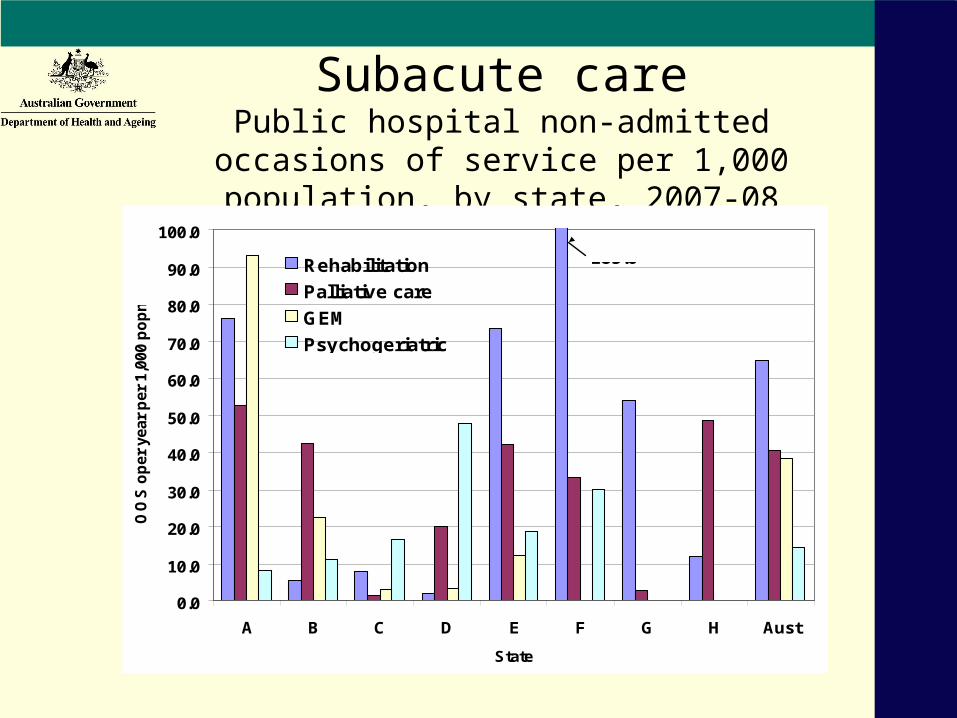
Subacute carePublic hospital non-admitted occasions of
service per 1,000 population, by state, 2007-08
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
A B C D E F G H Aust
State
OO
S o
per
yea
r p
er 1
,000
po
pn
Rehabilitation
Palliative care
GEM
Psychogeriatric
185.6
Subacute care
• Relates to patient’s functional status and quality of life.
• Is goal directed.
• Patients may have multiple diagnoses.
• Happens in a variety of settings
• Can happen without hospital admission or after a hospital stay.
The Commonwealth andsubacute care
• Pathways Home – $250 million over four years from 2002-03.
• National Action Plan: From hospital to home: improving health outcomes for older people, 2004-08.
• Long Stay Older Patients initiative – $150 million over four years to 2009-10.
• Transition Care from 2004-05.
Commonwealth action now
Working with the states and territories• 2,000 more Transition Care places• COAG $64 billion package, Nov. 2008
– includes $500 million for subacute care reform, 2009-10 to 2013-14
. . . steps toward further growth and reform.
National Partnership Agreement on Health and Hospital Workforce Reform
Subacute care reform element includes $500m to states in June 2009 to:– enhance subacute care services in hospitals
and in the community by 5% p.a. or 20% over four years from 2009-10;
– improve the available mix of services; and – improve data collections and performance
measurement.
National Partnership Agreement on Health and Hospital Workforce Reform
Subacute care reform element:• published subacute care implementation
plans;• published annual reports on performance
measures and service growth targets; and• collaborative work on measures, data
development, reporting and benchmarks.
Challenges
• Expansion of services
– Increasing demand, with:
• ageing population; and
• greater longevity despite chronic illness.
– Geographical disparities in service availability.
– Inadequate levels of public sector subacute services.
Challenges
• Workforce
– Shortages in particular occupations and locations.
– In some occupations staff availability varies greatly from state to state.
– Large losses of qualified people in some occupations; growing workforce in others.
The National Health and Hospitals Reform Commission
• Announced 25 February 2008, by the Prime Minister and the Minister for Health and Ageing.
• To report on a long-term health reform plan to provide sustainable improvements in the performance of the health system.
The National Health and Hospitals Reform Commission
The National Health and HospitalsReform Commission
Reform goals:• tackling major access and equity issues;• redesigning our health system to meet
emerging challenges; and• creating an agile and self-improving
health system,... with governance reforms and recommendations to implement change.
The National Health and HospitalsReform Commission
Access and equity priorities• Aboriginal and Torres Strait Islander people.• People with serious mental illness.• People living in remote and rural areas.• Timely access to quality care in public
hospitals.• Dental care.• National access targets.
The National Health and HospitalsReform Commission
Integrating and connecting• Redesign health services around people.• Access to the right care in the right setting.• Rethink planning and use of highly specialised
services provided by hospitals.Based on:• best value from our hospitals — wise use of assets
and skills;• more options for care in the community —
specialist services to ‘bridge’ between primary health care services and hospitals.
The National Health and HospitalsReform Commission
Funding the ‘missing link’.
The Commission finds urgent need for:• substantial investment in subacute services; and• substantial expansion of subacute services.
• The Commission proposes that the Commonwealthpay:• 100% of efficient cost of public hospital non-admitted
care (incl. subacute) with capped, activity-based budget;• 40% of efficient cost of admitted public patient care and
attendances at public hospital emergency departments.
The National Health and HospitalsReform Commission
Subacute care: visible and accessible• Funding more directly linked to growth and delivery
of services.• Activity-based funding models for subacute services
. . . plus incentive payments.• Improvements in national data and definitions.• Clear targets.• Planning and action for the right workforce.• Attention to equipment, aids, and other devices.• New rehabilitation facilities, that are not hospitals,
for both admitted and ambulatory care.
The National Health and HospitalsReform Commission
• Palliative care:
– building the capacity and competence of primary health care services for generalist palliative care,
. . . with educational support and collaboration with specialist palliative services;
– strengthened access to specialist services;
– investment in specialist services for care in the home.
• Advance care planning funded and implemented nationally
The National Health and HospitalsReform Commission
The NHHRC:• says more subacute care could release up to
531,000 bed days p.a. of acute care– around 80,000 people p.a. with faster access
to acute care.• recommends:
– up to $1.5 billion in infrastructure costs; and– at least $460 million increase in annual
recurrent funding.
Opportunities for change
• New services
• Improved models of care and care pathways
• Workforce reform
Next steps
• The Government is considering the NHHRC’s recommendations and consulting the community.
• The yourHealth website – submissions invited.
• Public consultation events – listening tour.
• Meeting of the Council of Australian Governments on health and hospitals reform in December 2009.
• Further COAG meeting in early 2010: Commonwealth will a reform plan to the states and territories.
Questions
Recommended