Embed Size (px)
Citation preview

Brit. J. prev. soc. Med. (1975), 29, 157-169
Subacute myelo-optic neuropathy and cioquinolAn epidemiological case-history for diagnosis
T. W. MEADEMRC-DHSS Epidemiology and Medical Care Unit, Northwick Park Hospital, Harrow
Meade, T. W. (1975). British JournalofPreventive and Social Medicine, 29, 157-169. Subacutemyelo-optic neuropathy and clioquinol: an epidemiological case-history for diagnosis. Betweenabout 1955 and 1970, some 10 000 Japanese were diagnosed as having subacute myelo-optic neuropathy (SMON), a new disease characterized by abdominal and neurological mani-festations, the former nearly always preceding the latter. Circumstantial evidence obtained in1969-70 suggested that SMON might have been caused by clioquinol (CQL), a gastro-intestinal disinfectant, and led to the suspension of further sales of CQL in Japan.However, several inconsistencies for the CQL theory of SMON have now emerged; first,CQL had been widely used in Japan for nearly 20 years before SMON occurred. Secondly,the SMON epidemic began to subside several months before CQL sales were suspended.Thirdly, a large proportion of SMON patients-probably about one-third and possiblymore-had not taken CQL within six months of the onset of the disease (the modal intervalbetween first taking CQL and the onset ofSMON being about three weeks, and more than 100days in only 4% ofSMON patients); of the remaining two-thirds or so, many had taken CQLas part of the treatment of the first (that is, abdominal) symptoms ofSMON itself. Fourthly,there was no dose-response relationship. Finally, SMON rarely, if ever, occurredoutside Japan. CQL could, however, have been involved in the causation of SMON as an
optional enhancer of some other necessary cause; the history of post-war environmentalpollution in Japan is compatible with this hypothesis. Over-readiness to accept postulatedtoxic effects ofmedicines and chemicals as proven is likely to do at least as much harm as goodto individual and community health.
THE DISEASE, AND A SUSPECTED CAUSEDuring the mid- and late 1950s, doctors in Japan
were consulted by increasing numbers of patientswith an unusual combination of alimentary andneurological complaints. The common clinicalpicture was of abdominal pain and/or diarrhoea,followed within a few days or weeks by painfuldysaesthesiae; in addition to the predominantlysensory disturbances, upper and/or lower motorneurone signs occurred in just over 50% of cases,and visual disorders due to optic neuritis in about28% (Sobue et al., 1971). The disease was calledsubacute myelo-optic neuropathy, or SMON.Table I summarizes Kono's (1971) list of SMON's'cardinal' and other symptoms; of particular im-portance is that the abdominal symptoms nearlyalways preceded the neurological. Case-fatality
from SMON itself is hard to assess because thedisease was very often associated with other con-ditions, many having a poor prognosis; but it islikely that not more than 5% of SMON patientsactually died of the disease itself. On the other hand,probably 90% ofpatients were left with dysaesthesiae,and 50% with limb weakness, visual impairment, orboth; 10 to 15% were completely disabled (Kono,1971). By the time the epidemic was over, some10 000 Japanese were said to have developed SMON,a figure of the same order as the world wide total ofthalidomide-deformed children. The main epidemio-logical features of the disease are summarized inTable II; these have not been seriously contested bythe protagonists or antagonists of the hypothesis onaetiology with which this review is concerned.
157
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

T. W. Meade
TABLE I'CARDINAL' AND OTHER SYMPTOMS OF SMON
1. Abdominal, preceding neurological in most cases
'Cardinal' 2. Neurological(a) Acute or subacute onset(b) Sensory disturbances predominate, mainly in
lower part of body
Other Include motor, visual, psychological and sphincterdisturbances
For full details, see Kono (1971)
TABLE IIMAIN EPIDEMIOLOGICAL FEATURES OF SMON
Female incidence about twice that of male incidence (2-6and I 2/annum per 100 000 population of all ages)Incidence maximum in summer monthsIncidence maximum in seventh and eighth decadesMajority of patients from professional rather than labouringclassesFrequently associated with other diseases (see also Table IV)
See Kono (1971 and 1973)
Subacute combined degeneration (SCD) of thecord is the main neurological differential diagnosisof SMON; multiple sclerosis has also to be con-sidered. In addition to pernicious anaemia, SCDmay, of course, be associated with a number ofintestinal disorders resulting in impaired vitaminB12 adsorption-such as blind loops, strictures, andanastomoses. Coeliac disease, lead, mercury,arsenic, and thallium intoxications also give riseto both abdominal and neurological manifestations,so that SMON was by no means unique in theserespects. Neurologists are in general agreement thatSMON exhibiting all its neurological features,visual, motor, and sensory, was a distinct and realclinical syndrome, but it is clear that in its lesscomplete forms it was not easily distinguishablefrom other causes of peripheral neuropathy andmyelopathy. Since these incomplete forms (forexample, abdominal symptoms and dysaesthesiae)accounted for most cases, opportunities for mis-diagnosis were frequent, a fact with obvious implica-tions for epidemiological studies.For virtually the whole course of the epidemic,
which ran from 1955 to 1970, SMON was regardedas probably being an infectious disease (Ogata andJitsunari, 1970). The main points in favour of aninfective aetiology were a regular summer peak inincidence, and claims that the disease clustered inindividuals drinking faecally contaminated waterfrom the same source. Various workers (see Kono,1971) claimed to have identified or isolated micro-biological pathogens. The newness of the disease,
its predilection for the elderly rather than the young,and the absence of expected clinical and pathologicalfeatures of infective disease (for example, in thecerebrospinal fluid) were reasons against the infec-tive theory.
In 1963, a greenish colouration of the tonguewas noticed in some SMON patients (Tsubaki,Honma, and Hoshi, 1971a). Although this observa-tion was thought to be of some possible relevance tothe aetiology of SMON, it did not receive muchfurther attention at that time. In February 1970,however, Takasu, Igata, and Toyokura (1970)reported on greenish faeces, and in May 1970 Igata,Hasegawa, and Tsuji (1970) on greenish urine inSMON patients; the green colour was found to bedue to the iron chelate of clioquinol (CQL), agastrointestinal disinfectant agent which had untilthen been generally thought not to be adsorbedfrom the gut. The presence of a chelate of CQL inurine demonstrated, however, that the preparationcould be adsorbed, and this being so, it was atleast possible that CQL was neurotoxic. (David etal. (1933) had recorded the urinary excretion ofVioform many years previously.)
After further investigations, including the demon-stration that many SMON patients had recentlytaken CQL, a public announcement to the effect thatCQL was probably the cause of SMON was madeearly in August 1970, and on 8 September 1970 theJapanese government suspended all further salesof the preparation (except for its very occasionaluse in exceptional circumstances such as the rarechildhood disorder acrodermatitis enteropathicain which CQL is said often to be life-saving).CQL is the generic name for a group of iodinated
hydroxyquinolines; in the West, it is chiefly used(under the brand names Entero-Vioform and Mexa-form) for the prophylaxis and treatment of'traveller's diarrhoea', although the evidence thatit is effective for these purposes is equivocal, atbest. In other parts of the world, however, the mainuse of CQL is in the treatment of amoebiasis.Having been available for many years, CQL hasnever been subjected- to formal clinical trials, butthe view of many physicians in countries whereamoebiasis is endemic is that the preparation iseffective in the treatment of the disease; furthermore,it is cheaper than other amoebicides such as metroni-dazole. Neurotoxic reactions (possibly dose-related)to huge doses of CQL have been described (Gholzand Arons, 1964), but these are not the same asSMON.To date, it has not been suggested, nor is there
any evidence, that some CQL preparations causeSMON while others do not, or that substances
158
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

Subacute myelo-optic neuropathy and clioquinol
other than CQL (such as different emulsifiers,contaminants, or degradation products of CQL)were responsible. Clioquinol (CQL) is thereforeused here in its generic sense, without implyingother substances with which CQL may be mixed orcontaminated, or to which it may be degraded(see later). Until the suspension of sales in 1970nearly 200 CQL-containing preparations were avail-able in Japan although most contained only smallamounts of CQL. Over-the-counter sales of CQLprobably accounted for one-third or even one-halfof total sales.
REASON AND EMOTION IN THE SMONCONTROVERSY
Two misconceptions which have so far substanti-ally clouded the issue when considering the epidemio-logical evidence for and against CQL as the causeof SMON need to be considered.
First, the fact that CQL sales were suspended inSeptember 1970 is not proof that the preparationcaused SMON. CQL sales were suspended for verygood reasons of public health. A prima facie casethat SMON might be caused by CQL had beenmade, and clearly needed to be answered. Since thetherapeutic value of CQL was not such that therewas any obvious likelihood of the sales suspensiondoing more harm than good, the decision to pro-hibit further sales was clearly prudent and correct.The scientific question ofthe nature ofthe associationbetween CQL and SMON is, however, quite separatefrom the issue of the suspension of sales and has tobe judged on different grounds from the practicalreasons for the latter. Secondly, the therapeuticvalue or otherwise of CQL, although certainlyrelevant to the decision to suspend sales, is irrelevantto the question of whether the preparation causedSMON. It is clearly illogical to base an assessmentof the harmful effects of a preparation on a beliefthat its beneficial effects may be limited. Yet it hasoften been assumed, both in Japan and elsewhere,that the sales suspension of a 'useless' preparationis evidence that CQL caused SMON.
Reactions to the CQL theory for SMON have tobe interpreted against the background of theJapanese experience of environmental pollution;from the radiation of the atomic bombs onwards,pollution in Japan has run at levels of an almostdifferent order of magnitude compared with therest of the world. Mercury poisoning caused thenotorius Minamata disease, and cadmium wasresponsible for Itai-Itai (ouch!-ouch!) bone disease.Asthma and bronchitis attributable to petrochemicalpollution of the atmoshere, and Kanemi rice oil
disease consequent on contamination of edible oilwith polychlorobiphenyl derivatives are otherexamples, although they by no means exhaust thelist (Ui, 1972). In addition, Japan was not only oneof the earliest countries to license thalidomide butalso virtually the last to withdraw it. That theJapanese approach to SMON was to assume that itwas caused by CQL unless proved otherwise wastherefore largely understandable, especially as thereare said to have been 10 000 victims, in contrastfor example, to perhaps 800 Minamata diseasepatients.
However, CQL had been used on a large scalefor some 20 years before the SMON epidemicstarted; this, and analogy with approaches to theinvestigation of alleged adverse effects of othermedicines, suggest that it is more appropriate toseek proof that CQL caused SMON, than that itdid not. Clearly, this point is arguable, and neitherthe positive nor the negative can be established withabsolute certainty; but to assume guilt in the absenceof proven innocence carries potentially dangerousimplications which are discussed later.
In the following review of the epidemiologicalevidence for and against the CQL hypothesis ofSMON, the data discussed are chiefly those of theJapanese investigators who believe a cause andeffect relationship between CQL and SMON tohave been established.
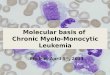
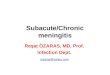
HISTORICAL AND TIME-SEQUENCE DATAFig. 1, from Kono (1973), shows the sales of
CQL in Japan from the mid-1930s and the numbersof SMON cases occurring each year. The unbrokenline in Fig. 2, from Kono (1971), shows the monthly
> 10 000.CUa,
a._
zo 1000O(0cn
0
6C 100-
CD
0
-J0oi 0co
j b.\ ,w.
COL produced .in Japan
*I0COL imported.SMON patients / ,
/*~ , 1/
/ ~ ,' A: I
935 40 45 SO 55 60 65Year
70
FIG. 1. Production of CQL and new cases of SMON, 1935-70.
159
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

T. W. Meade
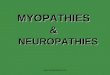
400-
FIG. 2. New cases ofSMON monthly; actual and projected, 1967-70.
numbers of new SMON cases in 1967-70. (Thebroken lines in Fig. 2 show projections, to bediscussed later).Two obvious questions are raised by Figs 1 and 2.
First, why was there apparently no SMON beforethe mid-1950s in spite of substantial CQL sales?Secondly, why did the decline and disappearance ofthe SMON epidemic antedate the suspension ofCQL sales?The first question is difficult to answer because
no sustained attempt was made to investigate howreal the apparent rise in SMON incidence was, atany rate until about 1972, well after the 15-yearepidemic was over. The ease with which incompleteforms of the SMON syndrome can be confused withother diseases makes it important to try to establishwhether:1. SMON was a new label applied to a condition
that had already been occurring for someconsiderable time (that is, had SMON beenunderdiagnosed before the mid-1950s?)
2. Unfamiliarity with a genuinely new diseasestarting in the 1950s resulted in its under-diagnosis until, say, the early 1960s
3. SMON was overdiagnosed in the later stages ofthe epidemic
4. The figures can be taken at their face valueOnly one of these possibilities has received any
real attention; a series of papers (Katahira, 1972;Katahira and Nakae, 1973; Katahira and Sonoda,
1972; Takasu et al., 1973) has recently claimed thatSMON did occur in the pre-war period. The mostdetailed of these (Takasu et al., 1973) reportedfindings in 703 typhoid patients admitted to hos-pital in 1937-38, of whom 30 were given CQL.Of these 703 patients, 16 were found to have dysaes-thesiae of the lower limbs; 'SMON was suspectedin one case, and it was possible to make a diagnosisof SMON (or it was impossible to deny a diagnosisof SMON) in the remaining 15. In six of thesecases, it was difficult not to admit a diagnosis ofSMON but there is some possibility that these sixdid not have the disease'. It was found that CQL-takers were admitted for nearly three times as longas non-takers; accordingly, only the 56 CQL non-takers admitted for more than 70 days were studiedfurther. Four of the 30 CQL takers and four of the56 CQL non-takers had dysaesthesiae (that is,were possibly SMON cases); the other eight (of the16 possible SMON cases) fell into the group ofCQL non-takers admitted for less than 70 days.
It is uncertain whether any of the 16 possibleSMON cases really had SMON and certainly verydoubtful for at least six. Of the 16 'cases', 12 hadapparently not taken CQL. After several stages ofselection, it is difficult to be convinced that like wascompared with like. Finally, neurological com-plications may occur in typhoid itself. This investiga-tion, therefore, failed to demonstrate convincinglythat SMON was a real clinical entity in Japan beforethe second world war (or that it was caused by CQL);
160
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

Subacute myelo-optic neuropathy and clioquinol
the same is true of the other studies. Indeed, Kata-hira and Nakae (1973) identified 20 reports between1929 and 1938 of side-effects of CQL, none of whichdescribed neurological symptoms or signs. However,some underdiagnosis of SMON in the early daysof its recognition is likely to have occurred, just assome overdiagnosis probably occurred later. Theseuncertainties, however, do not provide a firm basisfor other studies.
Fig. 2 suggests that the peak ofthe SMON epidemicmay have passed by mid- or late 1969, that is, a yearbefore the sales suspension, and that it had almostcertainly passed by March or April 1970, that is,several months before the announcement in August1970 of CQL's alleged toxicity and the suspensionof sales in September 1970. The broken lines of Fig. 2give three projections ofthe monthly numbers ofnewSMON cases that might have been expected had thetrend established in each previous 2-year-periodcontinued. Thus, one projection starts at the endof December 1968 (based on incidence figures forJanuary 1967-December 1968), one at the endof August 1969, and one at the end of September1969. Each projection gives similar results;together they indicate that the observed numbersofnew SMON cases began to be fewer than expectedin about September/October 1969. The usualinterval between starting CQL and the onset ofSMON was about three weeks and in only 4% ofSMON patients was it more than 100 days(Tsubaki et al., 1971a), so some change inCQL-taking habits in August/September 1969seems to be indicated if the CQL theory ofSMON is correct. (More detailed statistical analysesthan those on which the projections in Fig. 2 arebased could be performed, but are probably un-warranted given the non-specific nature of theincomplete, although commonly occurring, SMONsyndrome, and the lack of uniform diagnosticcriteria for epidemiological purposes (referred toin more detail in a later section). Moreover, thethree projections in Fig. 2 are in close agreementwith the calculations of the SMON ResearchCommittee (1972) in Japan.)From the data in Tsubaki et al. (1971a) on the
interval between the start of CQL administrationand the appearance of SMON it is also possible toestimate how quickly SMON should have dis-appeared after a total suspension of sales, on theassumption that CQL was the only cause of thedisease. New SMON cases would have been expectedin some numbers for a period of four months afterthe suspension; what was observed from Juneto October 1970, in terms of the rate of developmentof new cases (see Fig. 2), would have been expected
had there been a total sales supension in June 1970,that was immediately and completely compliedwith, on all CQL sales, over-the-counter as well asmedically prescribed. Even if all doctors hadstopped using CQL completely by June 1970,over-the-counter sales were still presumably madeuntil September 1970 and would have been expectedto result in the development of new cases untilJanuary 1971, almost certainly in larger numbersthan actually accurred; these numbers would havebeen determined by the pre-June proportion ofover-the-counter to total CQL sales, said to bebetween 30 and 50%. Experiences at the time(late 1960s) that certain types of pressurizedaerosols were implicated as a cause of suddendeath in asthmatics (see Fig. 2 of Doll (1973))indicate that doctors may, indeed, not onlybe aware of possible adverse effects beforethey are finally made known publicly, but also thatthey are likely to modify their practice accordingly.There is, however, no evidence that any Japanesedoctor knew about and communicated the possibilityof CQL as the cause of SMON in August/September1969, which would have been necessary to explainthe smaller than expected numbers of new SMONcases in September/October 1969 on the basis ofadvance information within the profession.
In summary, some decline in SMON incidencebefore September 1970 would not be incompatiblewith the CQL theory of the disease, although theonset of the decline may have been sufficientlylong before the green urine report and the salessuspension to raise serious doubts about this theory.The rate of the abrupt decline that was actuallyobserved can, however, be explained only if a verylarge proportion, perhaps most, of the lay public,as well as doctors, had advance warning and tookappropriate action; this inconsistency is separatefrom the question of when the peak of the epidemicwas passed.
In some areas of Japan, SMON did not apparentlyappear until well into the 1960s, and the disease
TABLE IIISMON IN TODA/WARABI, 1963-69
Year Confirmed/Suspected Unconfirmed Total
1963 2 0 21964 18 21 391965 3 2 51966 6 1 71967 6 3 91968 2 1 31969 1 2 3
Total 38 30 68
161
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

T. W. Meade
waned and virtually disappeared long before thegreen tongue/urine reports, let alone the suspensionof CQL sales. 'It was about the autumn of 1963that SMON cases first appeared' in Toda/Warabi(SMON Research Committee, 1972); SMON casesby year of onset in this area of Japan are shown inTable III. It seems clear that the local SMONepidemic reached its peak in 1964 and that by1968-69 it had almost entirely subsided. Anotherlocal inconsistency of this sort occurred in Okayamaprefecture (SMON Research Committee, 1972) whereno SMON was reported until 1967, although CQLhad been in use formany years, as elsewhere inJapan.
COMPARATIVE STUDIESThe Japanese studies in which SMON patients
have been compared with non-SMON patients fortheir previous CQL intake, or in which CQL-takershave been compared with CQL non-takers for theirsubsequent SMON experience, form perhaps themost crucial part of the epidemiological evidenceavailable. These studies are unusually difficult toevaluate, mainly because little information isavailable on how far appropriate methods have beenconsidered or adhered to, and the lack of much ofthe control or comparative information that isessential in this particular case, and also becauseof the very unusual, perhaps unique, situation inSMON that its alleged cause was also often usedin its treatment.The SMON Research Committee's first nation-
wide study (1970) was mainly concerned withidentifying and characterizing patients with SMON;it included 4280 patients (62 4% 'firm' SMON;37-6% 'suspected'). The 'standards for diagnosis'in this survey were not really standard; the different
ways in which the disease was viewed by differentworkers, and the varying diagnostic details used bythree doctors involved in the study are in factexplicitly referred to. Definitions of physical signswere not given. There is little or no informationon response rates or completeness of data. However,a regional study in Okayama reported in the samevolume gave the results summarized in Table IV;it is not clear how the individuals without SMONwere selected, but previous histories of severaldisorders, including gastrointestinal conditions,were found in substantially higher proportions ofSMON patients than the non-SMON individuals;(a more intensive study of the SMON patients thanthose without it could be a partial or completeexplanation for the differences shown). Sobue etal. (1971) reported similar findings.The Committee reported also on further nation-
wide studies (1972) in which it dealt with the CQL-taking of SMON patients. The Committee calledfor details on all SMON patients in designatedcities and all prefectures who had attended orvisited various medical institutions from 1967 to1971. A detailed study appears to have been madeonly on patients whose intake of CQL before orafter the development of neurological symptomswas recorded-that is, it seems where a definitenote was lacking that CQL had or had not beentaken, these SMON patients were not included infurther studies. Before 1970 there was no reasonwhy CQL non-usage should have been speciallynoted; for the SMON patients where CQL wassaid not to have been taken there must have beendefinite information to this effect. The CQL-takingpart of the survey questionnaire was apparentlyrevised in the course of the work.
TABLE IVCOMPARISON OF PAST MEDICAL HISTORY OF 60 SMON PATIENTS AND 3107 INDIVIDUALS WITHOUT SMON
A BDisease 60 SMON patients 3107 non-SMON individuals A%/B%
No. % No. %Appendicitis* 27 450 507 16-3 2-8
Chronic gastritis .. 12 20-0 114 3-7 5.4
Allergicdiseases .. I1 18-3 127 4-1 4-5
Gastroptosis .. 9 150 131 4-2 3*6
Abortion**.. .. 8 13*3 133 4*3 3*1
Tuberculosis .. 6 10-0 140 4 5 2-2
Rheumatism 6 10*0 92 3 *0 3*3
Diarrhoea/enteritis .. 4 67 52 1-7 3 9
*Figures of 50% for A and 12% for B also quoted**Women onlyKono (1973) also reports frequent occurrence of SMON in diabetes and cancer, and after laparotomy
162
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

Subacute myeleo-optic neuropathy and clioquinol
TABLE VCQL-TAKING WITHIN SIX MONTHS BEFORE ONSET OF
NEUROLOGICAL SYMPTOMS OF SMON
*There is obviously an inconsistency between the inclusion of thiscategory in the table and indications elsewhere (see text) that thestudies were confined only to those whose recent CQL-takinghistory was known
**Of those whose CQL-taking histories were known
Although 9249 patients were eventually identifiedin the studies reported on in 1972, only 2456 wereincluded in the main analyses of CQL-taking,which are summarized in Table V. How the 2456patients were selected is not clear, and the authorsof this part of the report had serious reservationsas to how representative the group was. Someprefectures did not return any questionnairesalthough they often had hundreds of SMONcases. If any conclusions can be drawn from thisstudy, it is clear that even in those patients whereCQL ingestion status was known, 25% hadprobably not ('Never' and 'Apparently not') takenCQL. If the groups for whom there was no CQLinformation are also considered these figures couldbe even higher. It has already been pointed outthat the CQL-taking studies appear to have includedonly those whose CQL intake was definitely re-corded; it thus becomes difficult to attribute theSMON patients with no apparent history of CQL-taking to inaccurate recording or recall of CQLintake at a later date.Estimates of the proportions of SMON patients
who did not take CQL vary considerably. Theyrange from only 4% in the 171 hospital patientsstudied by Tsubaki, Honma, and Hoshi (1971b)through the figures just discussed, to about 50%in the series collected by the Japanese Ministry ofHealth and Welfare (1973). In the latter, 'nottaking chinoform' (CQL) was defined as no historyof the preparation having been taken for six monthsbefore the onset of SMON (although it might havebeen taken more than six months before or atany time after the onset), a definition which seemsreasonable in view of the data of Tsubaki et al.(1971a) on the distribution of intervals betweenstarting CQL and the onset ofSMON. The particularvalue of the six cases in the Ministry series withclinical onsets between February and July 1970(after the 'green tongue/urine' reports) and especiallyof the 17 cases with onsets between October 1970and September 1972 (after both the 'green tongue/
urine' reports and the sales suspension) is that theymust have been investigated especially thoroughlywith every expectation of positive CQL-takinghistories, and yet, no such histories were elicited. Itis difficult to accept that serious mistakes over boththe diagnosis ofSMON and the taking of CQL weremade in these patients, and there is thus strongevidence for believing that SMON does occurwithout CQL; the 17 CQL non-taking cases des-cribed after October 1970 constitute about 50%of the total of 30 or so new SMON cases apparentlyreported after this date.The observations so far described on the CQL-
taking histories of SMON patients were uncon-trolled; conclusions drawn from them rest on theassumption that the proportions of SMON patientswho took CQL are 'exceedingly high comparedwith the rate of administration of other drugs'(Kono, 1971). Certainly, it may sometimes beconcluded from uncontrolled observations that apreparation caused a disease; thalidomide is theoutstanding example. However, CQL-taking inSMON patients is almost certain to have been afrequent occurrence for at least two reasons. First,the fact that a high proportion of SMON patientshad had previous gastrointestinal disease makes itmore likely that they would have taken CQL (andother preparations) than individuals without SMON.Secondly, CQL is not only the postulated cause ofSMON, it may frequently be its unintentional orintentional treatment; in fact, Takasaki (1967),Kusui (1969), and Shibata and Osawa (1970)described its use in the actual management of thedisease. In the 752 cases of SMON studied bySobue et al. (1971), chronic abdominal disorders
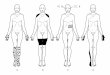
SMON1
Indications* for CQL
CQL taken
Onset of abdominal symptoms
Further CQL taken
Onset of neurological symptoms
*For example, diarrhoea, abdominal pain.The scheme assumes that these indications arenot themselves the abdominal manifestations ofSMON due to a previous course of CCL withinthe preceding 6 months.
FIG. 3. Course of events and onset of SMON, assuming SMONcaused by CQL.
163
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

T. W. Meade
(diarrhoea and pain) occurred in 84%, and in87 '4% of these, the abdominal symptoms precededthe neurological. Consequently, as Fig. 3 illustrates,any studies that simply measure CQL-taking inSMON patients over a short period of time, withoutdistinguishing CQL taken for an initial bout ofdiarrhoea or abdominal pain from CQL taken afterthe onset of the abdominal symptoms of SMONitself, are virtually guaranteed to find a spuriouslyhigh proportion of patients with a history of CQL-taking. The most striking features of SMON are theneurological ones, and results in the Japanesestudies of SMON patients have so far been almostexclusively presented in terms of CQL-taking beforethe onset of the neurological component of thedisease without allowance being made for thecrucial importance of the intervening onset of itsabdominal symptoms. Very few attempts have beenmade to deal with this difficulty, but in one group of255 patients 42% had taken CQL before the onsetof the prodromal abdominal symptoms (9% duringthe course of chronic abdominal disorders); 47%took it after the onset of the abdominal symptoms ofSMON and 11 % had not taken it at all (Sobue andAndo, 1970). In these terms, at least 58% of thepatients had not taken CQL before the onset ofSMON.
Several studies have described the subsequentSMON incidence in groups of CQL-takers andnon-takers; four appear to show a higher incidencein those who took CQL than in those who did not,and their results are summarized in Table VI. Ifthe apparent differences between CQL-takers andnon-takers could be interpreted at face value,they would provide compelling evidence for theCQL theory of SMON. There are, however, severalreasons why they cannot be so interpreted, at anyrate without further information.
TABLE VIONSET OF SMON BY CQL ADMINISTRATION
Administration Developed Did NotAuthors Year of CQL SMON Develop
SMON
Yoshitake 1970 Yes 34 (43 6) 44and Igata No 0 77
Kuratsune 1971 Yes 5 (4-3) 110et al. No 0 217
Aoki etal. 1971 Yes 17(3-2) 515No 4 (0'1) 3782
Tsubaki 1971b Yes 29 (11-0) 234et al. No 0 706
Percentages are given in parentheses
First, the proportions of CQL takers who thendeveloped SMON range widely, from 3 *2 to 43 *6%.This in itself suggests that there may have beendifferences in the methods used, or between CQL-takers and non-takers, that may have had a bearingon the results.
Secondly, each of the studies says very little aboutits methods or sources of material, or (most im-portant of all) to what extent the CQL-takers andnon-takers were comparable in other respects. Areconsideration of the main epidemiologicalcharacteristics of SMON patients (Table II) raisesthe possibility that if the CQL-takers in the fourstudies referred to in Table VI were (to take anextreme example, for illustrative purposes) elderlywomen from professional backgrounds with frequenthistories of other illnesses associated with SMON,and the CQL non-takers were young men in labour-ing occupations with few previous illnesses, ahigher incidence in the former than the latter wouldbe virtually guaranteed for reasons that might verywell have little or nothing to do with CQL-taking,which could simply be yet another 'marker' orcharacteristic of those prone to SMON. It is pre-sumably likely that the CQL-takers in the studiesreferred to in Table VI tended to conform to thefirst sterotype described; the characteristics of theCQL non-takers in these studies are, however,largely unknown. Yoshitake and Igata (1970)accept that some factor other than CQL may havebeen responsible for their findings (Table VI).At least one paper (Hino, 1972) claimed no
excess of SMON in CQL-takers compared withnon-takers although, again, methods were notspecified. The study of Takasu et al. (1973) onpossible SMON in typhoid patients (already dis-cussed) can also be interpreted as demonstrating noexcess of SMON in CQL-takers.
Since the four studies summarized in Table VIwere certainly reported, and presumably carriedout, after the CQL hypothesis for SMON wasadvanced, and as there is nothing to suggest thatSMON diagnoses were made independently ofinformation on CQL-taking, it may very well havebeen that SMON was in some cases diagnosedpartly, perhaps even mainly, because it was knownpatients had taken CQL.
DOsE-RESPONSE RELATIONSHIPSince adverse reactions to medicines can be
idiosyncratic or allergic as well as dose-related, theabsence of a dose-response relationship is notnecessarily evidence against the CQL hypothesis ofSMON. The presence of a clear dose-response
164
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

Subacute myelo-optic neuropathy and clioquinol
relationship would, however, be in favour ofthe hypothesis. It is sometimes claimed thatthe onset of SMON did not follow the relativelylow doses of CQL recommended outside Japan, forexample, by the British Committee on Safety ofMedicines (1973), which suggested that courses oftreatment should not exceed 7 * 5 g in total, separatedby intervals of at least four weeks. Data of Tsubakiet a!. (1971a) show, however, that while 20-29 gtotal was the modal dose in this series of 171patients, 15 patients had taken less than 10 g. Inone of the SMON Research Committee reports(1971) 62 out of 508 CQL-takers who developedSMON (there were also 102 cases who had nottaken CQL) had taken less than 10 g (mean 52 g).The report explicitly concluded that there was nodose-response relationship.To establish a graded dose-response relationship
for the incidence of SMON, data on CQL dosagesfor a comparison population are needed (as well asforSMON patients). Three ofthe studies summarizedin Table VI (Aoki et al., 1971; Kuratsune et al.,1971; Tsubaki et al., 1971b) are apparently theonly sources of such information, and none supportsa dose-response relationship. Data on CQL dosesin SMON patients do not support a dose-responserelationship for severity of SMON.
Aggregated regional and countrywide data onCQL sales and SMON incidence provide little or nouseful information on dose-response relationship.
INTERNATIONAL DATAIt is not certain how many cases ofSMON (if any)
have occurred outside Japan. The world literatureand case reports have been reviewed by independentexperts (Rose, 1974). In brief, there may be some 20patients whose diagnoses are compatible withSMON, although this is not to say they definitelyhad SMON. Even if there were 100 such cases,however, the numbers would be trivial comparedwith those in Japan, both absolutely and relatively,bearing in mind the numbers of people in the restof the world who have taken CQL. The followingcountries had per caput sales in 1969 of Entero-Vioform and Mexaform equal to or higher thanJapan:
LibyaSwitzerlandLebanonBelgium andLuxembourgMoroccoHollandItalyMexico
0-660-610 48
0 440-410-360-350-29
Norway 0*27Sweden 0*27Australia 0*27Western Germany 0*25Brazil 0*23Greece 0-23Egypt 019
The figure for Japan itself was 0 18These figures (Ciba-Geigy, 1974) are sales in
grams per person, based on the total populationsof the countries concerned, and this general pictureis not materially altered if sales of CQL in formsother than Entero-Vioform and Mexaform aretaken into account.
It has been suggested that national CQL salesfigures in Japan are misleading, when comparedwith similar figures for other countries, becausedosage differed in Japan by being at high levelsand for long periods-that is, a great deal was givento relatively small numbers of patients. There areno objective data by which to judge this possibility,but dosage patterns in Brazil, for example, are saidto be very similar to those in Japan. Dosage levelsand durations in the Japanese Pharmacopoeia donot differ markedly, if at all, from schedules in otherpharmacopoeias.Only one possible case of SMON in a Japanese
outside Japan (he was on holiday) has been reported,although it is reasonable to assume that manyex-patriate Japanese have taken CQL. (CQL is notgenerally available in the USA, but there are otherJapanese communities in countries outside Japan,such as Brazil.) A genetic predisposition to SMONin the Japanese thus seems improbable.
There are, however, examples of chemicals whichfit the SMON time sequence better than CQL, beingvery much more heavily distributed in Japan thanin other countries at the relevant times. FAO datashow eight times the use of mercurial fungicidesper agricultural km2 in Japan in 1961-65 than, forexample, in the USA, and large differences in thelate 1960s between the heavy use of benzene hexa-chloride (BHC), DDT, aldrin, and dieldrin peragricultural km2 in Japan and their lighteruse in India, the USA, and other countries, (Foodand Agricultural Organization 1971-72). Concen-trations of mercury in various foods in Japangreatly exceeded those in the USA in the 1960s(Smart, 1968; Goldwater, 1971), and total BHClevels in human fat in the late 1960s and early 1970sin Japan were more than 20 times the figures in theUSA and UK (Doguchi, 1973). Furthermore, mostif not all these substances were introduced after thewar and their usage in Japan declined sharply inthe late 1960s as concern over their potential
165
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

T. W. Meade
hazards began to mount. The SMON epidemicconforms to time sequences of this sort considerablymore logically than to that of the availability ofCQL. The time lag between the marked decline in theuse of organomercuric fungicides in 1965 and ofchlorinated hydrocarbons in 1968-69, and the vir-tual disappearance of SMON in 1970 could beexplained by the time taken for food treated withwith these compounds to grow, be harvested,marketed, and consumed, and for toxic levels toaccumulate. It is not suggested that the specificcompounds named were the cause of SMON,but they are examples of how the use and subsequentcontrol of other environmental pollutants in Japancould fit the rise and fall of SMON incidence.One hypothesis for SMON in which CQL might
have played a causal role and which would explainthe apparent inconsistencies discussed is suggestedby these considerations. The necessary cause ofSMON might have been an environmental agent-for example, a medicine, virus (compare thepre-CQL theories about SMON), or chemical-that was much more widely distributed in Japan,and in higher concentrations, than in other countries.This agent might have appeared in Japan in theearly 1950s and disappeared in the late 1960s. Theagent would have been able to cause SMON on itsown, but, in combination with CQL, its potentialfor doing so would have been greatly enhanced;CQL on its own, however, could not have causedSMON except in very rare circumstances. Peoplesuffering from the diseases listed in Table IV mighthave been particularly susceptible to this agent(there are clinical examples, such as herpes inleukaemia, consistent with this suggestion).An explanation along these or similar lines would
account for:1. The absence of SMON before about 1955.2. The fact that the decline in the SMON epidemic
antedated the sales suspension.3. The CQL non-takers among the SMON
patients.4. The virtual absence of SMON outside Japan.
Apart from the indirect evidence on levels ofenvironmental pollutants in Japan already discussed,there is no real evidence for or against this theory.Nevertheless, interactions between two or morefactors as the possible cause ofsome environmentallydetermined diseases should not be overlooked,although these interactions are obviously likelyto be more difficult to investigate than instanceswhere only one factor is involved; the epidemio-logical study of possible interactions is, indeed, inits infancy. Which agent is 'causative' in these
circumstances, especially where both are necessary,is something of a philosophical question. In thecase of a two-factor hypothesis for SMON, CQLcould be an enhancer of a necessary cause butprobably not the necessary cause itself.
It is theoretically possible that SMON was theresult of the contamination of CQL with somethingelse. However, SMON occurred in some patientswho had taken Japanese preparations, and in somewho had taken imported preparations; there is noevidence or reason for believing that the samecontaminant was mixed with, and later excludedfrom, both Japanese and imported preparations.(The same general argument applies to CQLdegradation products.) In addition, the full SMONsyndrome is a specific clinical entity, which is notcharacteristic of known toxic substances. A con-tamination explanation for SMON thus seemsunlikely.
CONCLUSION ON SMONIt would be unreasonable to take an absolutely
rigid view about all the inconsistencies in the CQLhypothesis for SMON and to conclude that, solong as even one remained, the hypothesis couldnot be accepted. The thalidomide episode demon-strated that phocomelia sometimes occurred inthose with no apparent history of having taken thepreparation; in the case of sudden deaths in asthma,the eventual decline in mortality probably precededany formal warnings. Reasons have, however, beengiven for doubting that similar inconsistencies in thecase of CQL and SMON can reasonably beexplained within similar margins of tolerance; inaddition, the SMON controversy is characterizednot simply by one or two serious inconsistencies butby a series-the apparent absence of SMON untillong after the introduction ofCQL, its decline beforeCQL sales were suspended, a large proportion ofSMON patients who did not, apparently, take CQL,no dose-response relationship, and the virtualabsence of SMON outside Japan. (Finally, althoughoutside the scope of this review, there are at presentno convincing data from animal experiments.)
WIDER IMPLICATIONS OF THE SMON CoNmovERsYIt would be easy to set SMON on one side as a
strange disease, confined to one country, and causedby a 'useless' medicine the precise role of which inthe SMON epidemic requires no further definitionthan it has already received. Yet the SMON con-troversy could prove something of a water-shed inthe study of the adverse effects of medicines.Contemporary reactions to suggestions that apreparation may have adverse effects are partly,
166
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

Subacute myeleo-optic neuropathy and clioquinol
perhaps largely, conditioned by the fact that theseclaims have so far usually been substantiated-forexample, chloramphenicol in aplastic anaemia,thalidomide in phocomelia, aerosols in asthmadeaths, and oral contraceptives in thromboembolicdisease. By contrast, several more recent episodeshave been much less easy to resolve than theseearlier ones. The nature of the relationship betweenpostoperative jaundice and exposure to holothaneis hotly disputed (see Inman and Mushin, 1974and subsequent correspondence); the demonstrationthat halothane affects liver function, as assessed bychanges in serum enzyme levels, (Wright et al.,1975; Trowell, Trowell, Peto, and Crampton Smith,1975) strengthens, but by no means settles, thecase. Whether tolbutamide causes rather thanprevents arterial complications in diabetics is anothercontroversial issue (Feinstein, 1971). Data on therelationship between reserpine and breast cancer(Armstrong, Stevens, and Doll, 1974; Heinonenet al., 1974; Boston Collaborative Drug SurveillanceProgram, 1974) have stimulated much criticaldiscussion about appropriate study methods anda growing realization of difficulties of interpretationthat may arise in this and similar cases. The prima.facie case that reserpine is involved in the aetiology ofbreast cancer remains strong, although in an inquiryin which both the breast cancer patients and thesubjects with whom they were compared came fromthe same defined population, Mack et al. (1975)found no association, and have thus introduced asubstantial element of doubt. The SMON epidemicshows signs of being assimilated into the case-lawof undisputed cause and effect associations (Lawsonand Wilson, 1974) although it is perhaps the bestavailable example of these much more open andunresolved episodes.The continuing production of powerful thera-
peutic agents carries with it the virtual certainty offurther unwanted reactions, while inquiries such asthe Boston Collaborative Drug Surveillance Program(1974) will ensure that many of these reactions aredetected, as indeed they should be. Associationsthat may at first sight seem to be of a causal nature,but eventually prove not to be, will almost cer-tainly also come to light under modern conditionsof surveillance. There is a great deal to be lost byfailing to distinguish true from spurious adverseeffects. A central concern in the halothane debate,for example, has rightly been that the value of thisgenerally accepted and widely used anaestheticshould not be compromised by allegations oftoxicity that may be unfounded. Many fearthat the use of other anaesthetics, consequent onanxieties of possible litigation in the event of
jaundice after halothane, could be against the bestinterests of thousands of patients undergoingsurgery.
Over-ready acceptance of the possible adverseeffects of medicines is only one aspect of a widerdebate about the costs and benefits not only ofmedicines but of other substances. There are signsthat the outcome of this debate could be to thedetriment of useful advances in the fields of com-munity health and clinical medicine. Environmentalhysteria, rather than objective appraisal, character-ized much of a recent campaign against DDTwhich, had it been successful, would almostcertainly have cost many lives. The 1958 DelaneyAmendment to the Food, Drug, and CosmeticAct in the United States (reviewed in PreventiveMedicine, 1973) and insistence on inappropriateand uniformative toxicological testing in animals(Lancet, 1973) are other examples of measures thatare probably more likely to delay progress thanprevent harm. Over-caution in prescribing maysometimes have disastrous consequences; in ampho-tericin pharmacophobia, Symmers (1973) reportedon five patients who died because amphotericinwas withheld, although it was obviously indicated.Wade (1974) used the examples of chloroform,cyclamates, oral hypoglycaemic agents, and oralcontraceptives to show how either the nature ormanner of a decision about possible adverse effectsmay have undesirable consequences.
It is only necessary to compare modem withearlier methods of treatment in diseases as differentas leprosy and hypertension to appreciate theadvances that pharmaceutical research and develop-ment have brought about. The conquest of manyother diseases, including under-nutrition, dependsinter alia on further advances of a similar kind.There is, however, an increasing number of obstaclesto further progress (Spinks, 1974; Weatherall,1974); one of these could easily turn out to beover-eagerness to accept scientifically unsub-stantiated allegations of adverse effects, especiallyif 'guilty until proved innocent' is the starting-point.This view is not by any means to argue for theunmonitored use of new compounds but it doesargue, among other things, for very searchinginvestigations in the study of alleged side-effects. Itis possible to define at least four purposes to whichthe results of such studies may be put. The first isthe decision whether or not to restrict the use of amedicine, and considerations of its clinical value areclearly relevant here. The second is to make a scientificevaluation of the probability that the agent is thecause of the unwanted effect, and here neither itsclinical value nor decisions about its continued use
167
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

T. W. Meade
are to the point; this evaulation may provide valuableinformation on the aetiology and prevention of otherdiseases, which makes it especially important that itshould be entirely objective. Doll (1971) has rightlypointed out that different study techniques are neces-sary in different circumstances; itmay therefore not beuseful to try to draw up routine methods or criteriaby which to judge the likelihood of a cause andeffect relationship. However, the case against a
medicine should be able to command fairly generalagreement before it is finally accepted as such. Thethird use depends very much on the second and isthe fair and swift compensation of those affected,where cause and effect have been shown to bereasonably likely. Fourthly, the pharmaceuticalindustry will have to decide what further researchand development it will or will not pursue.-Theseare fairly distinct issues, and the balance of evidencecould be used to make different decisions underdifferent headings-for example, a medicine couldbe withdrawn from use under the first, while thescientific and legal questions remained unresolved.However, therapeutic progress in the future standsto suffer if decisions against the further use ofmedicines under the first heading become, or aremade to become, the basis for decisions under theother three. SMON has provided an excellentopportunity to review and re-assess all the scientificand social implications of the whole field.
I am grateful to a number of people for help with thisreview, but especially to Mr W. R. S. North and Mr P. J.Brennan for advice on statistical points, and to MrsAnita Rohan for clerical and typing assistance. Englishtranslations of papers published in Japanese wereprovided by Ciba-Geigy Ltd., Basle; the JapaneseEmbassy in London kindly provided some of the materialreviewed.
Requests for reprints: T. W. Meade, MRC-DHSSEpidemiology and Medical Care Unit, Northwick ParkHospital, Watford Road, Harrow, HAl 3 UJ.
REFERENCES*AOKI, K., OTANI, M., SOBUE, I., and ANDO, K. (1971).
Relationship between chinoform administration andSMON incidence observed in some medical institutes.Presented at the meeting of SMON Research Com-mittee, 1 March 1971.
ARMSTRONG, B., STEVENS, N., and DOLL, R. (1974).Retrospective study of the association between use ofrauwolfia derivatives and breast cancer in Englishwomen. Lancet, 2, 672.
BOSTON COLLABORATIVE DRUG SURVEILLANCE PROGRAM(1974). Reserpine and breast cancer. Lancet, 2, 669.
BRmsH COMMITEE ON SAFETY OF MEDICINES (1973).Report for 1972. HMSO, London.
CIBA-GEIGY (1974). Personal communication.DAVID, N. A., JOHNSTONE, H. G., REED, A. C., and
LEAKE, C. D. (1933). The treatment of amebiasis withiodochlorhydroxyquinoline. J. Amer. med. Ass., 100,1658.
DoGucHI, M. (1973). Chlorinated hydrocarbons in theenvironment in the Kanto Plain and Tokyo Bay.International Symposium on New Methods in Environ-mental Chemistry and Toxicology, Susono, Japan,November 1973.
DOLL, R. (1971). Unwanted effects of drugs. Brit. med.Bull., 27, 25.- (1973). Monitoring the National Health Service.Proc. roy. Soc. Med., 66, 729.
FEINSTEIN, A. R. (1971). Clinical biostatistics: UDGPstudy. Clin. Pharmacol. Ther., 12, 167.
FOOD AND AGRICULTURAL ORGANIZAnON (1971-72).Production Year Books 25 and 26.
GHOLZ, L. M. and ARONS, W. L. (1964). Prophylaxisand therapy of amebiasis and shigellosis with iodo_chlorhydroxyquine. Amer. J. trop. Med. Hyg., 13, 396
GOLDWATER, L. J. (1971). Mercury in the environment.Scd. Amer., 224, (5), 15.
HEINONEN, 0. P., SHAPIRO, S., TUOMINEN, L., andTURUNEN, M. I. (1974). Reserpine use in relation tobreast cancer. Lancet, 2, 675.
*HINO, S. (1972). Clioquinol and SMON. Chiryo, 54.*IGATA, A. HASEGAWA, S., and TsuJI, T. (1970). On the
green pigment found in SMON patients: Two casesexcreting greenish urine. Jap. med. J., No. 2427, 25.
INMAN, W. H. W., and MUSHIN, W. W. (1974). Jaundiceafter repeated exposure to halothane. Brit. med. J.,1 5.
*JAPANESE MINISTRY OF HEALTH AND WELFARE (1973).Survey of SMON cases not taking clioquinol, (by Y.KuROIwA and A. KosAKA).
*KATAHIRA, K. (1972). Suspected SMON patients inJapan from 1937 to 1938. Report 18 atSMON ResearchCommittee meeting, 18 December 1972.*- and NAKAB, K. (1973). Medication with clioquinoland out-break of SMON-like cases in pre-war days.Igaku no Ayumi, 84, 525.
*.. and SONODA, K. (1972). Bibliographicconsiderationof clioquinol, Part 1. Report 19 at SMON ResearchCommittee meeting, 18 December 1972.
KoNo, R. (1971). Sub-acute myeloneuropathy, a newneurological disease prevailing in Japan. Jap. J. ned.Sci. Blol., 24,195.
* (1973). Challenging the incurable disease. ModernMedicine, April 1973, 10.
168
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from

Subacute myelo-optic neuropathy and clioquinol
*KURATSUNE, T., NISHIzuMI, M., Kocm, S., YOSHIMURA,T., MATSUZAKA, J., and TOKUTOMI, N. (1971). Epi-demiologic survey on the relationship between SMONand chinoform. Presented at the meeting of SMONResearch Committee, 1 March 1971.
*KusUi, K. (1969). Shindan to Chiryo, 57, 1587.
LANCET (1973). Human toxicology: research versus
testing. Lancet, 1, 871.LAWSON, D. H. and WILSON, G. M. (1974). Detecting
adverse drug reactions. Brit. J. hosp. Med., 12, 790.MACK, T. M., HENDERSON, B. E., GERKINS, V. R.,ARTHUR, M., BAPTTA, J., and PIKE, M. C. (1975)-Reserpine and breast cancer in a retirement community-New Engl. J. Med., 292, 1366.
*OGATA, M. and JrrsuNARI, F. (1970). Epidemiologicalstudies on encephalomyelitis accompanied by ab-
dominal symptoms. Nihon Koshu Eisei Zasshi, 17, 357.PREVENTIVE MEDICINE (1973). Guest editorials on theDelaney Clause. Prev. Med., 2, 123.
ROSE, F. C. (1974). SMON outside Japan. 10th Inter-national Congress of Neurology, Barcelona. ExcerptaMedica, Amsterdam.
*SHIBATA, T. and OSAWA, H. (1970). Clinical Report, 4,1281.
SMART, N. A. (1968). Use and residues of mercurycompounds in agriculture. Residue Reviews, 23, 1.
SMON RESEARCH COMMIrTEE, (1970, 1971, 1972).Reports.
*SOBUE, I. and ANDO, K. (1970). Meeting of SMONResearch Committee, 13 November 1970.
-, IIDA, M., TAKAYANAGI, T., YAMAMURA, Y.,and MATSUOKA, Y. (1971). Myeloneuropathy withabdominal disorders in Japan. Neurology, 21, 168.
SPINKS, A. (1974). Future invention in a harsher world.Proc. roy. Soc. Med., 67, 969.
SYMMERS, W. ST.C., (1973). Amphotericin pharmaco-phobia. Brit. med. J., 4, 460.
TAKASAKI, H. (1967). Encephalomyelopathy with Pre-ceding Episode of Intestinal Symptoms, p.99, IgakuShoin, Tokyo.
*TA"U, T., IGATA, A. and TOYOKURA, Y. (1970). Onthe green tongue observed in SMON patients. Igakuno Ayumi, 72, 539.
*-, TOYOKURA, Y., NAKAE, K., KATAHIRA, K., andSUGIYAMA, S. (1973). Suspected cases of SMON inJapan in 1938. Nihon Rinsho, 31, 204.
TROWELL, J., PETO, R., and CRAMPTON SMrrH, A. (1975).Controlled trial of repeated halothane anaesthetics inpatients with carcinoma of the uterine cervix treatedwith radium. Lancet, 1, 821.
*TsUBAKI, T., HONMA, Y., and HOSHI, M. (1971a).Epidemiological study of clioquinol as etiology ofSMON. Nihon Iji Shinpo, 2448, 29.
q ~~, and - (1971b). Neurological syndromeassociated with clioquinol. Lancet, 1, 696.
Ui, J. (ed.) (1972). Polluted Japan, Tokyo.WADE, 0. L. (1974). Instant wisdom. A study of decisionmaking in the glare of publicity. Scientific Proc. of theCardiff Med. Soc., 8 January 1974.
WEATHERALL, M. (1974). Limitations on the discoveryand supply of medicines. Proc. roy. Soc. Med., 67,1287.
WRIGHT, R., EADE, 0. E., CHISHOLM, M., HAWKSLEY,M., LLOYD, B., MOLES, T. M., EDWARDS, J. C., andGARDNER, M. J. (1975). Controlled prospectivestudy of the effect of liver function of multipleexposures to halothane. Lancet, 1, 817.
YOSHITAKE, Y. and IGATA, A. (1970). SMON casesfollowing abdominal surgery. Igaku no Ayumi, 74, 598
*denotes original in Japanese
169
Protected by copyright.
on June 4, 2022 by guest.http://jech.bm
j.com/
Br J P
rev Soc M
ed: first published as 10.1136/jech.29.3.157 on 1 Septem
ber 1975. Dow
nloaded from