Kopila kafle
Bachelor of optometry
3rd year
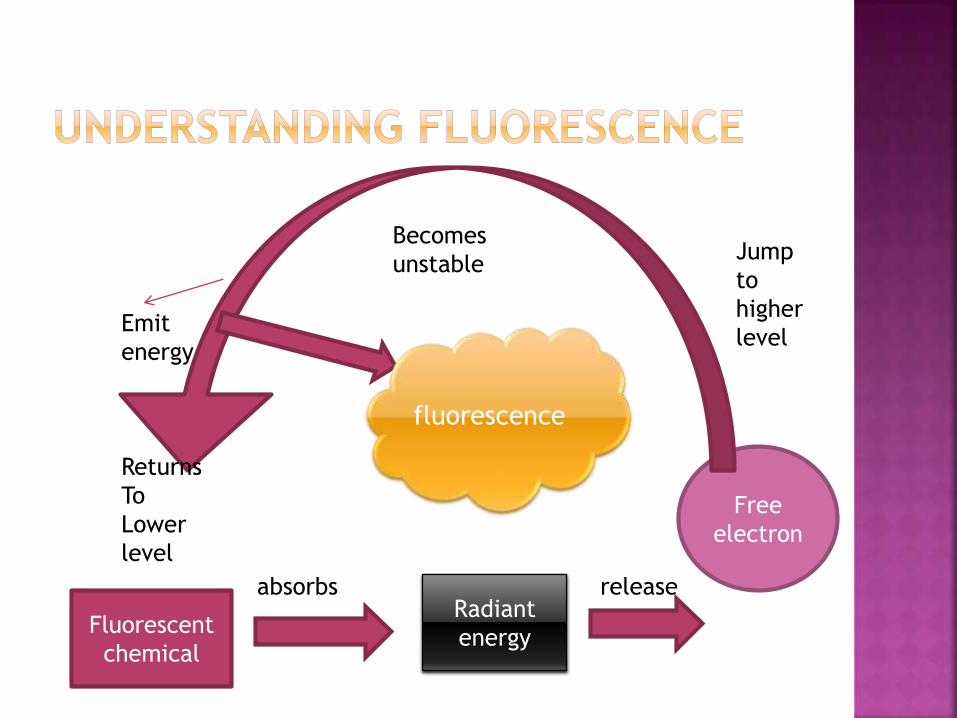
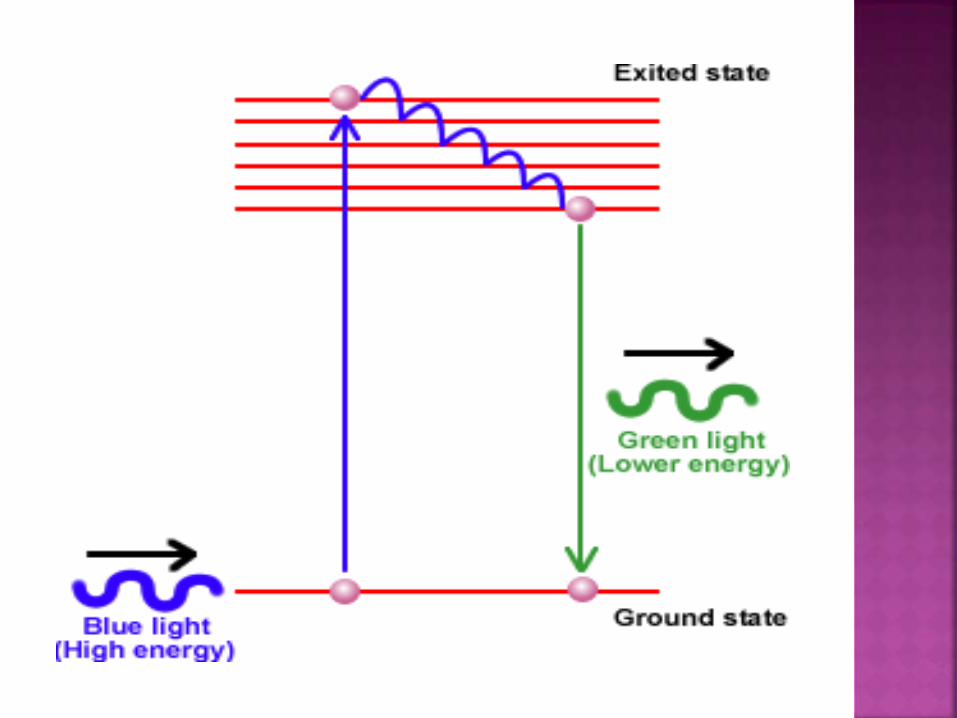
Fluorescent
chemical
absorbsRadiant
energy
release
Free
electron
Jump
to
higher
level
Becomes
unstable
Returns
To
Lower
level
Emit
energy
fluorescence
Absorbed radiant energy > emitted energy
AND
As energy – inversely proportional to –
wavelength
SO,
λ of emitted wave > λ of absorbed wave
Depending on the chemical to be excited,
the electromagnetic energy (excitation
light) must lie within a particular range of
wavelengths absorption spectrum
The wavelengths of fluorescent light emitted by a particular chemical substance lie within a characteristic range called
emission spectrum.
What is fluorescent material ? ?
What is the range of absorption spectrum ? ?
What is the range of emission spectrum ? ?
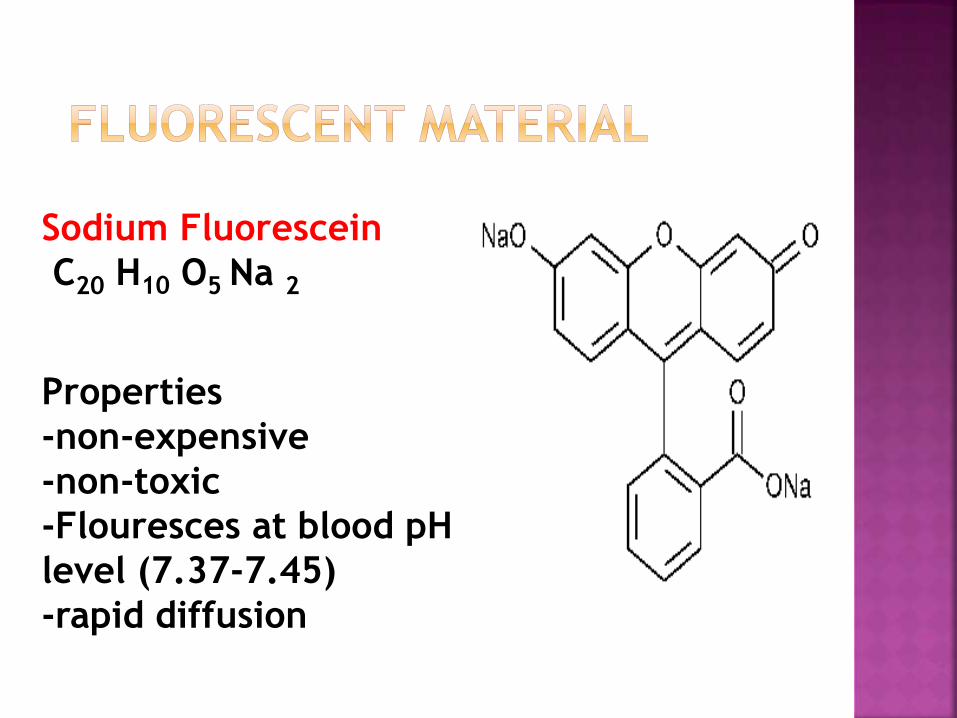
Sodium Fluorescein
C20 H10 O5 Na 2
Properties
-non-expensive
-non-toxic
-Flouresces at blood pH
level (7.37-7.45)
-rapid diffusion
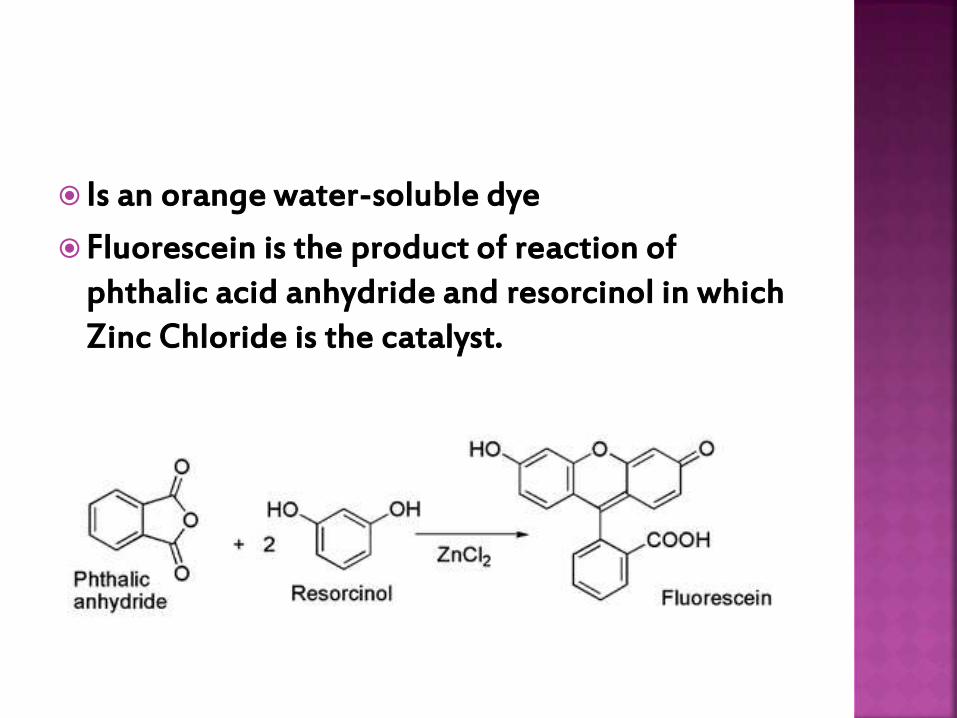
Is an orange water-soluble dye
Fluorescein is the product of reaction of phthalic acid anhydride and resorcinol in which Zinc Chloride is the catalyst.
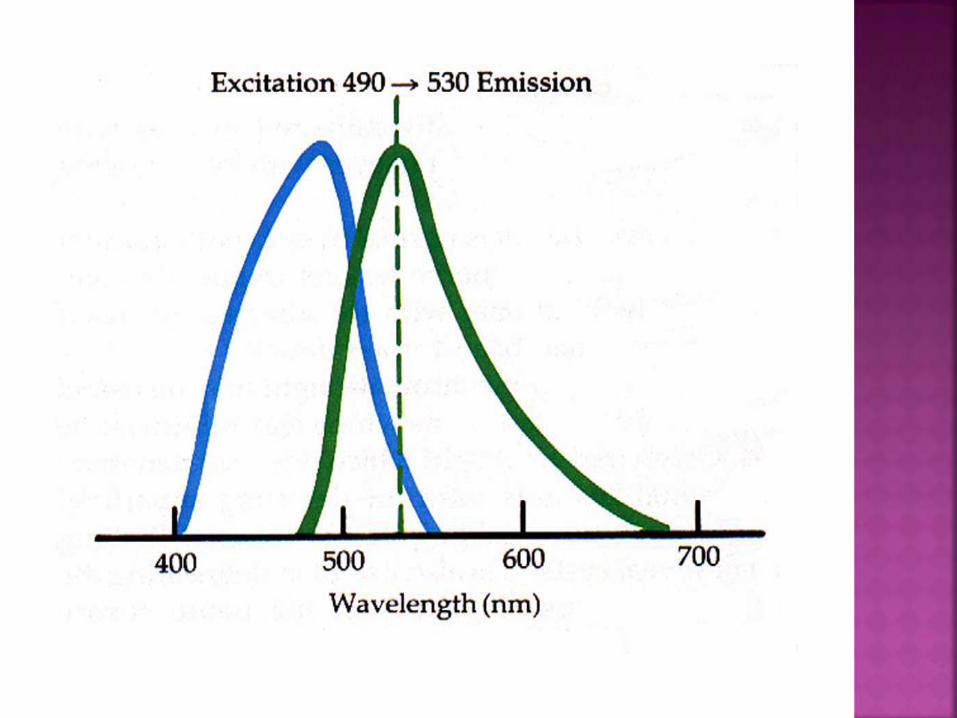
Lies between 465-490 nm
Excitation peak = 490nm(blue part of spectrum)
represents maximal absorption of light energy by fluorescein.
Lies between 520 – 530 nm
Emission peak = 530 nm
Represents green part of spectrum
studying the normal physiology of the retinal and choroidal circulation,as well as disease process affecting the macula.
Evaluation of the vascular integrity of the retinal and choroidal vessels
Check the integrity of the blood ocular barrier.
- outer blood retinal barrier breaks in CSR
- inner blood retinal barrier breaks in NVD,NVE
In clinical diagnosis
to determine extent of damage
To formulate treatment strategy for
choroidal and retinal disease
To monitor result of treatment
Indications
of FFA
Macular
disorders
Retinal diseases
1) Diabetic retinopathy
2) Retinal vein occlusions
3) Retinal artery occlusion
4) Retinal vasculitis
5) Coats disease
6) Familial exudativevitreoretinopathy
Macular diseases1) Central serous
retinopathy2) RPE detachment3) Cystoid macular
edema4) Macular hole5) ARMD6) Cone rod dystrophy7) Epiretinal membrane8) Vitiliform
dystrophies9) Stargardts dystrophy
Retinal vascular malformations and tumors
1) Capillary hemangioma of retina2) Cavernous hemangioma of retina3) Retinal AV malformation 4) Congenital tortuosity of retinal
vasculature5) Congenital hypertrophy of RPE6) Angioid streaks7) Astrocytic hamartoma
Choroidal lesions1) Choroidal
neovascularmembrane (CNV)
2) Hemangioma3) Nevus4) Melanoma5) Choroiditis6) Metastasis7) MEWDS8) APMPPE9) Choroidal folds
Optic nerve disorders
1) Optic atrophy
2) Papilloedema
3) Ischemic optic neuropathy
4) Optic disc pit
5) Optic disc drusen
6) Optic disc hemangioma
7) Melanocytoma
8) Myelinated nerve fibers
ABSOLUTE
1) known allergy to iodine containing compounds.
2) H/O adverse reaction to FFA in the past.
RELATIVE
1) Asthma
2) Hay fever
3) Renal failure
4) Hepatic failure
5) Pregnancy ( especially 1st trimester)
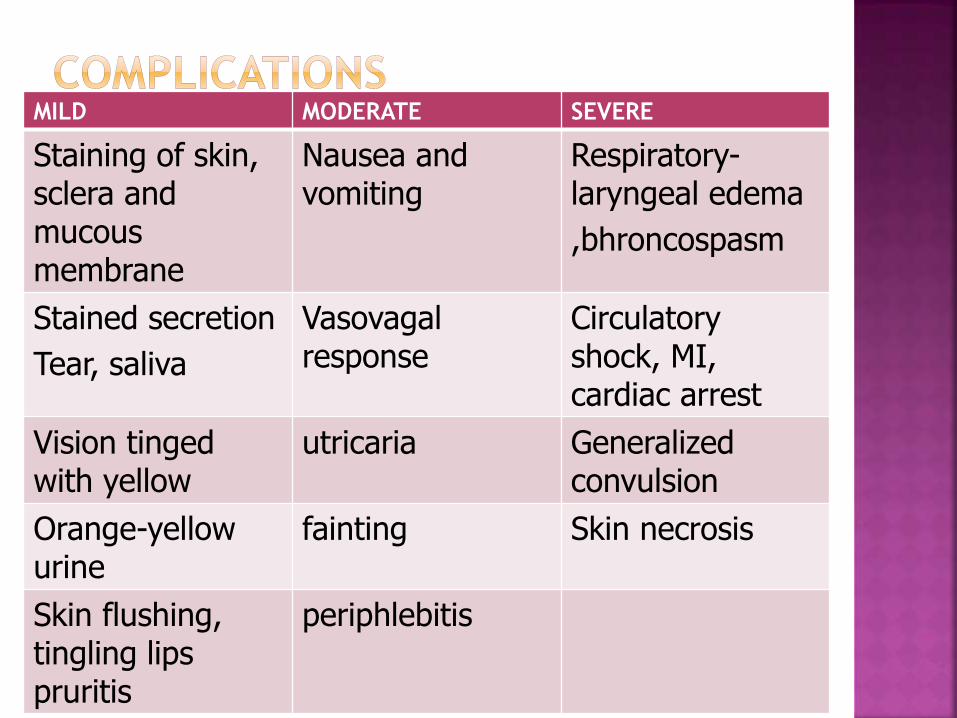
MILD MODERATE SEVERE
Staining of skin, sclera and mucous membrane
Nausea and vomiting
Respiratory-laryngeal edema
,bhroncospasm
Stained secretion
Tear, saliva
Vasovagalresponse
Circulatory shock, MI, cardiac arrest
Vision tinged with yellow
utricaria Generalized convulsion
Orange-yellow urine
fainting Skin necrosis
Skin flushing, tingling lips pruritis
periphlebitis
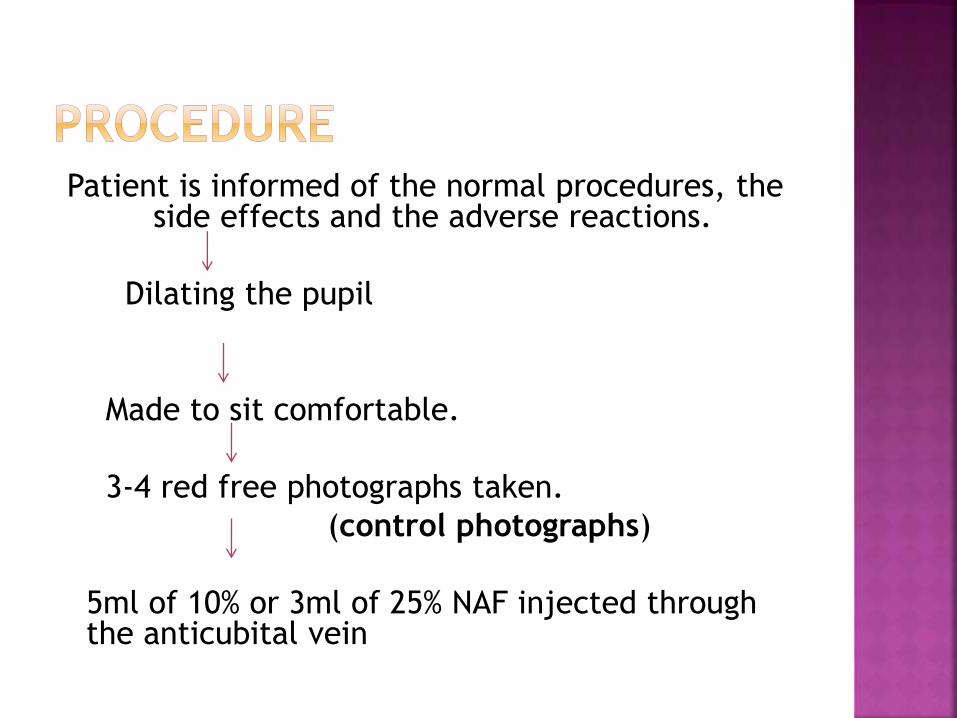
Patient is informed of the normal procedures, the side effects and the adverse reactions.
Dilating the pupil
Made to sit comfortable.
3-4 red free photographs taken.
(control photographs)
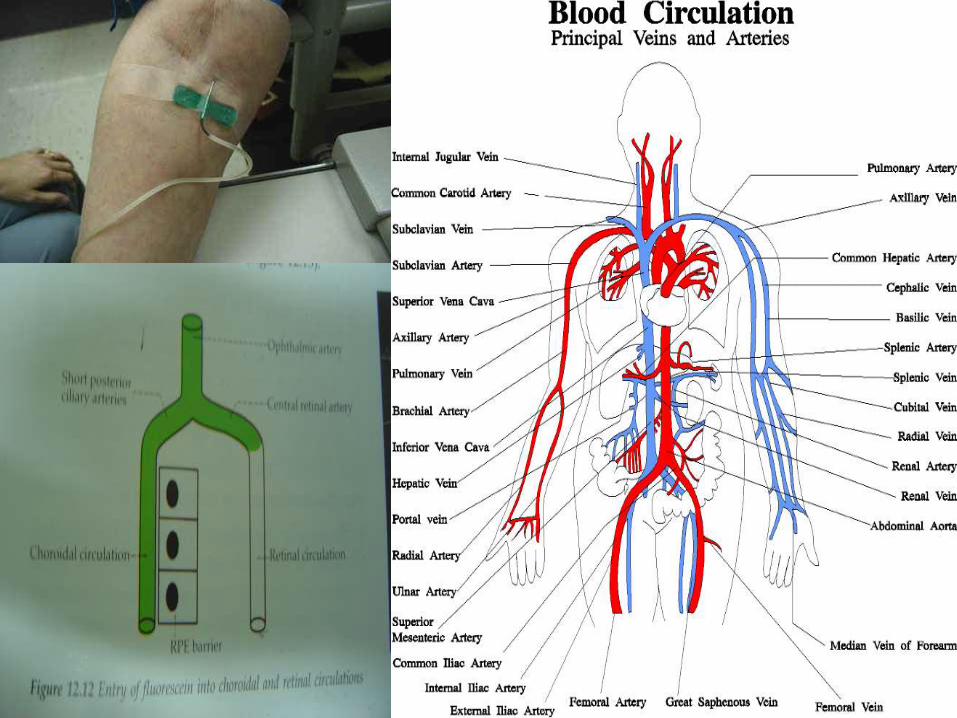
5ml of 10% or 3ml of 25% NAF injected through the anticubital vein
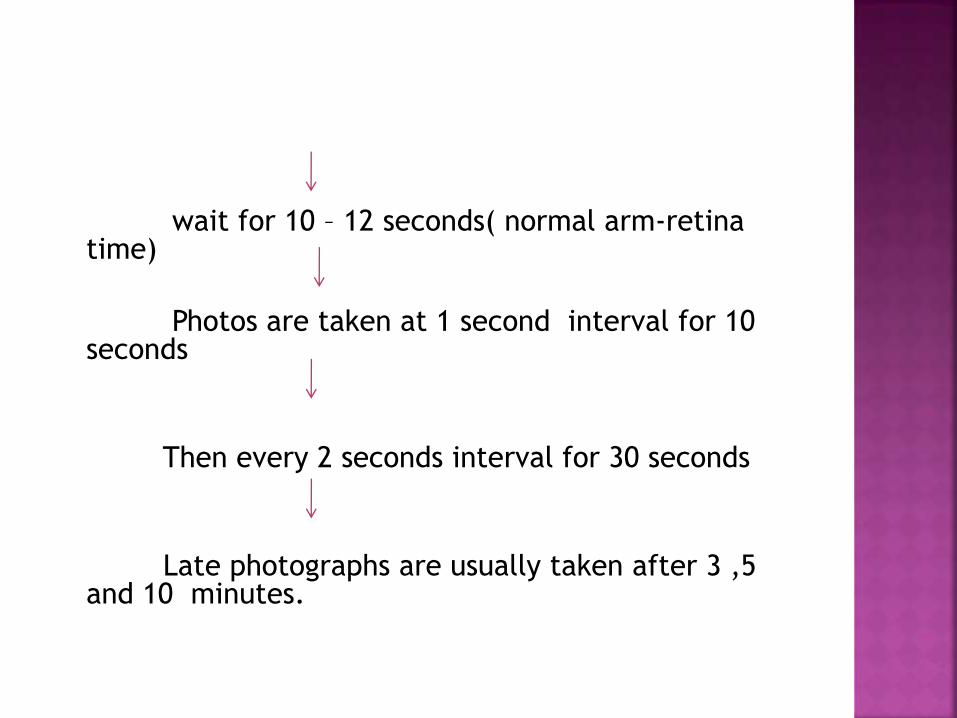
wait for 10 – 12 seconds( normal arm-retina time)
Photos are taken at 1 second interval for 10 seconds
Then every 2 seconds interval for 30 seconds
Late photographs are usually taken after 3 ,5 and 10 minutes.
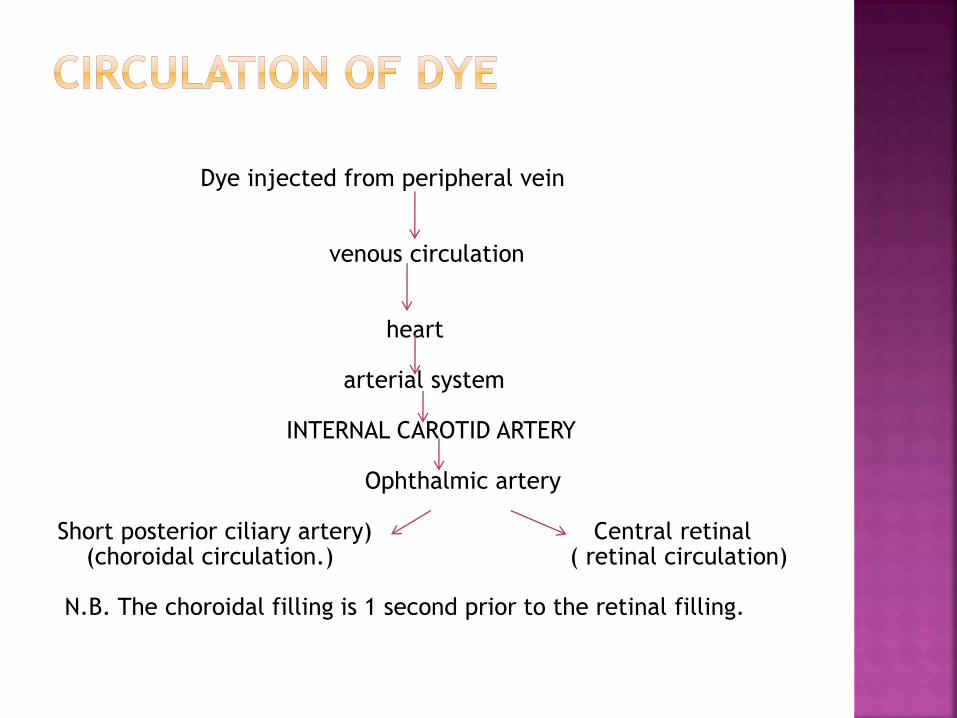
Dye injected from peripheral vein
venous circulation
heart
arterial system
INTERNAL CAROTID ARTERY
Ophthalmic artery
Short posterior ciliary artery) Central retinal (choroidal circulation.) ( retinal circulation)
N.B. The choroidal filling is 1 second prior to the retinal filling.
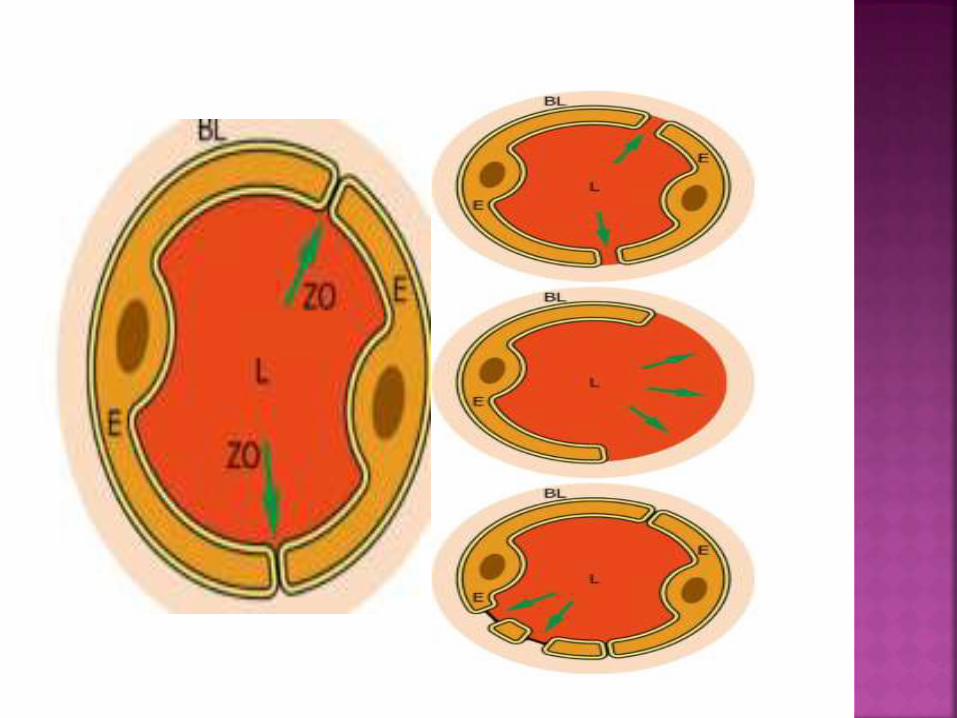
A.Choroidalcirculation
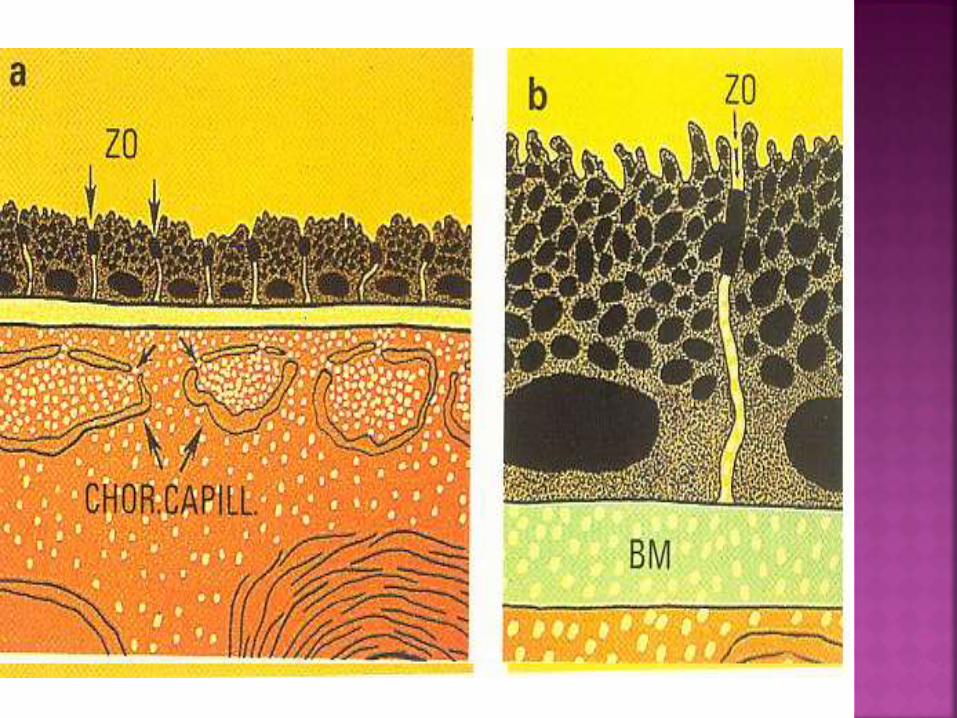
-choriocapillaries are fenestrated
-so allows dye to diffuse freely
BUT,
-outer blood-retinal barrier in RPE don’t let dye to reach retina
B.Retinal circulation
-endothelial cells of retinal blood vessels joined by tight junctions (inner blood retinal barrier)
-prevents leakage of dye from vessels
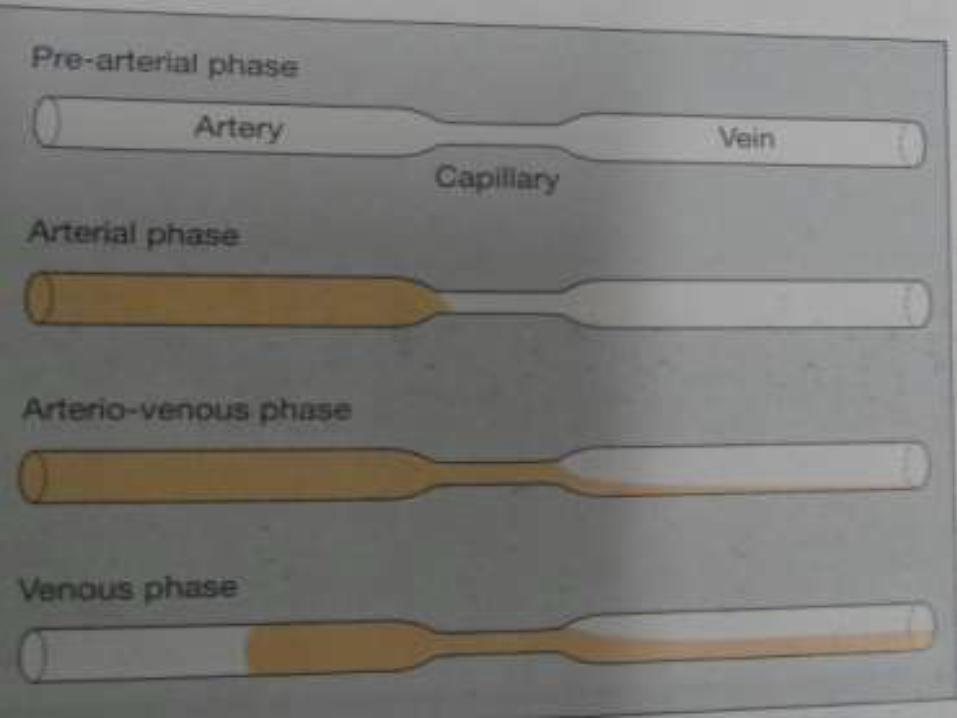
A) Choroidal (pre-arterial)
B) Arterial
C) Arteriovenous(capillary)
D) Venous and
E) Late(elimination)
Patchy filling
No leakage
No complication
WHY ???
Choriocapillaries has number of lobules
The lobules fill independently from one
another,
giving a transiently patched or blotched
appearance
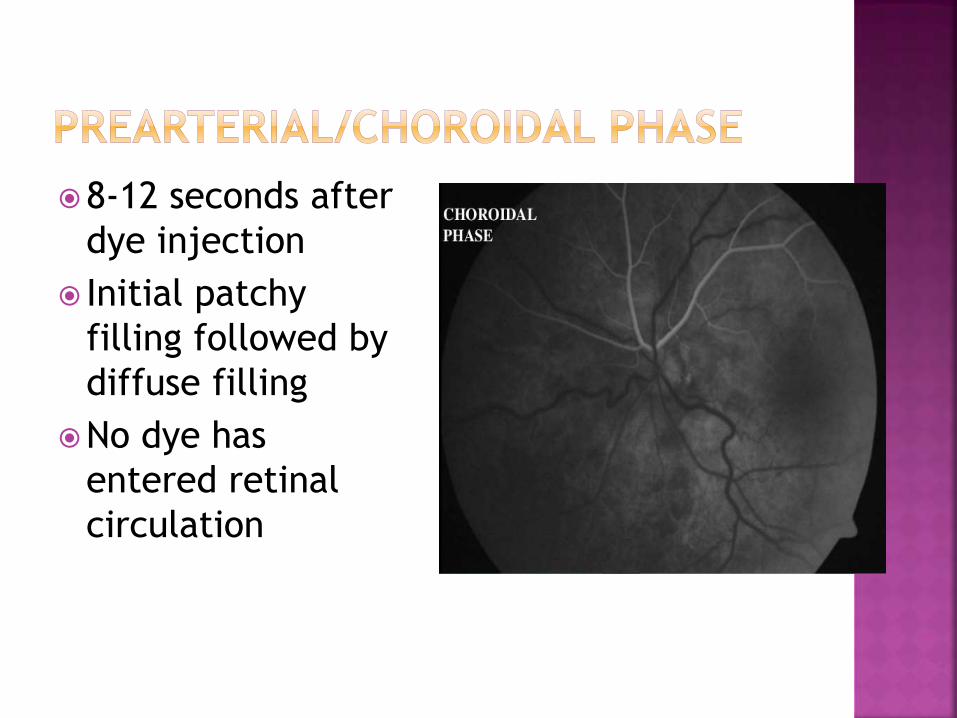
8-12 seconds after
dye injection
Initial patchy
filling followed by
diffuse filling
No dye has
entered retinal
circulation
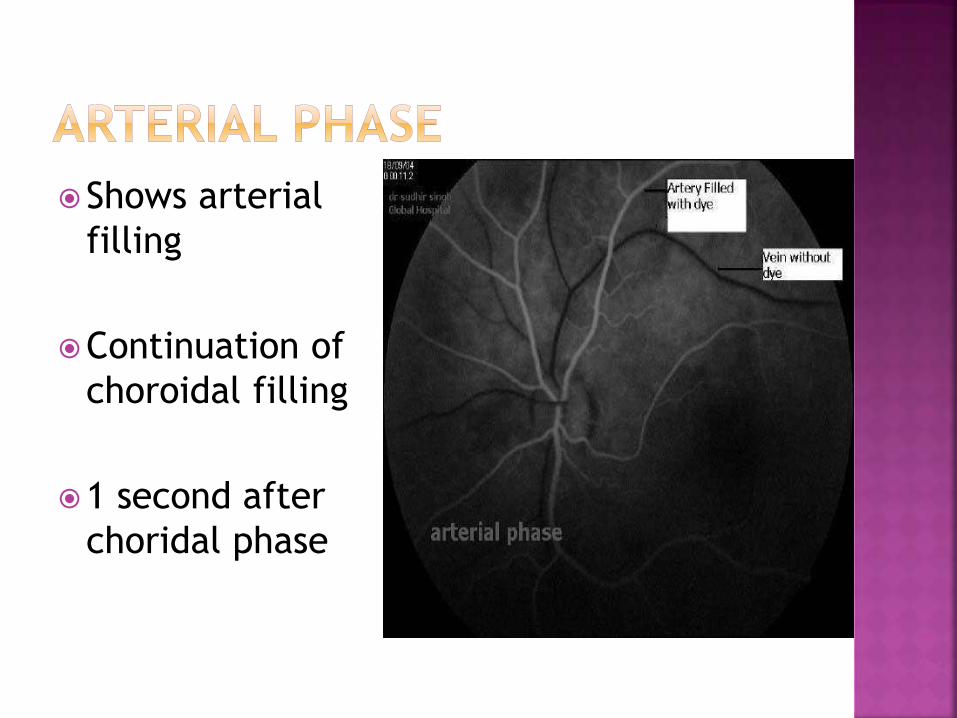
Shows arterial
filling
Continuation of
choroidal filling
1 second after
choridal phase
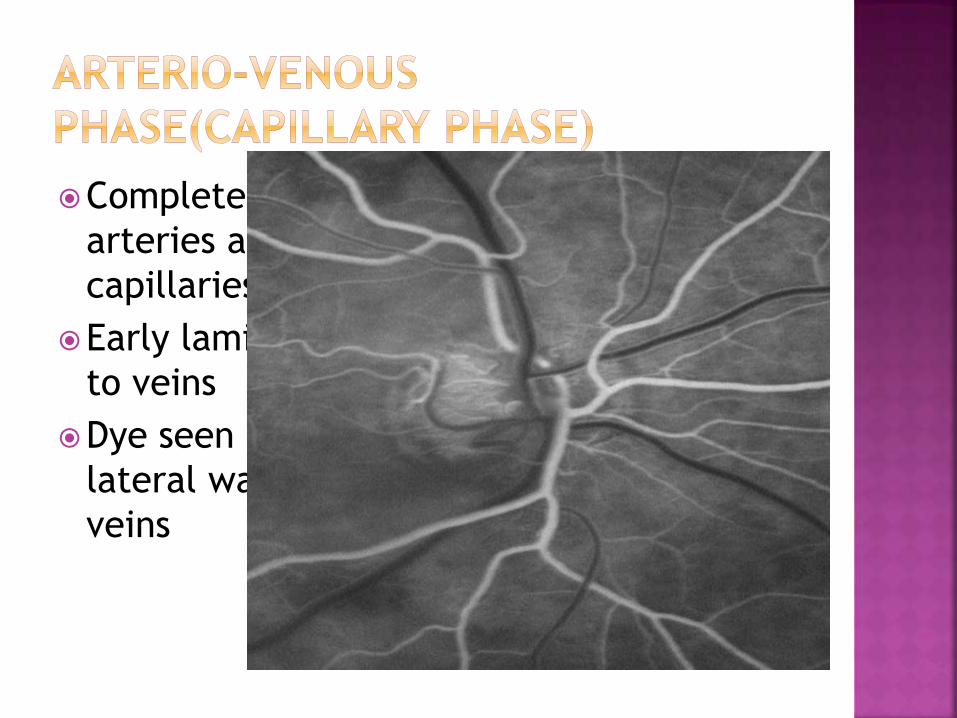
Complete filling of
arteries and
capillaries
Early laminar flow
to veins
Dye seen along
lateral wall of
veins
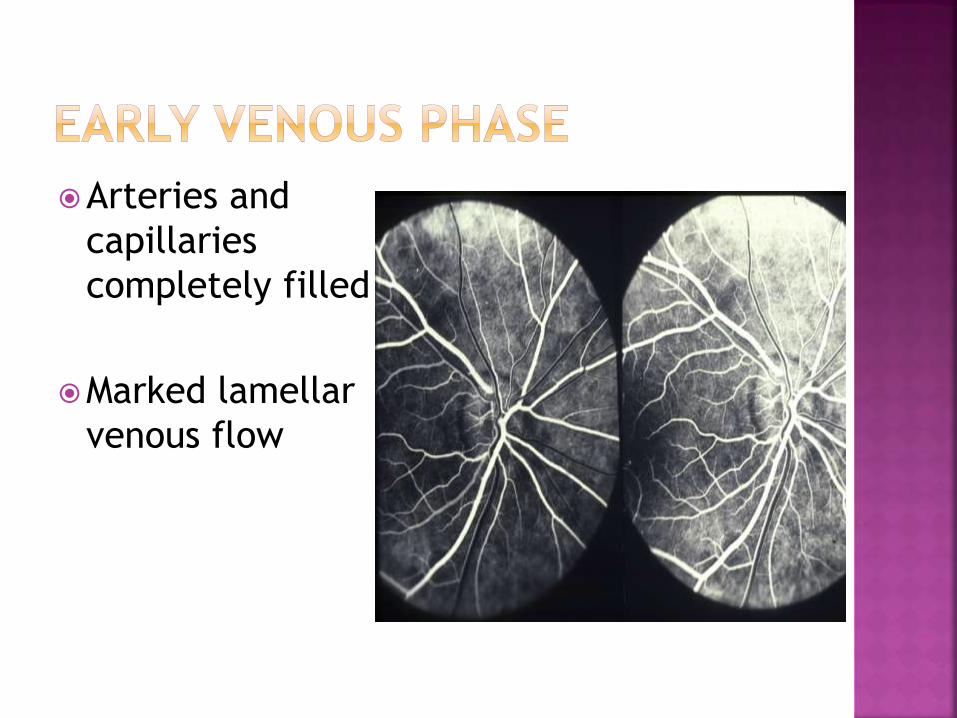
Arteries and
capillaries
completely filled
Marked lamellar
venous flow
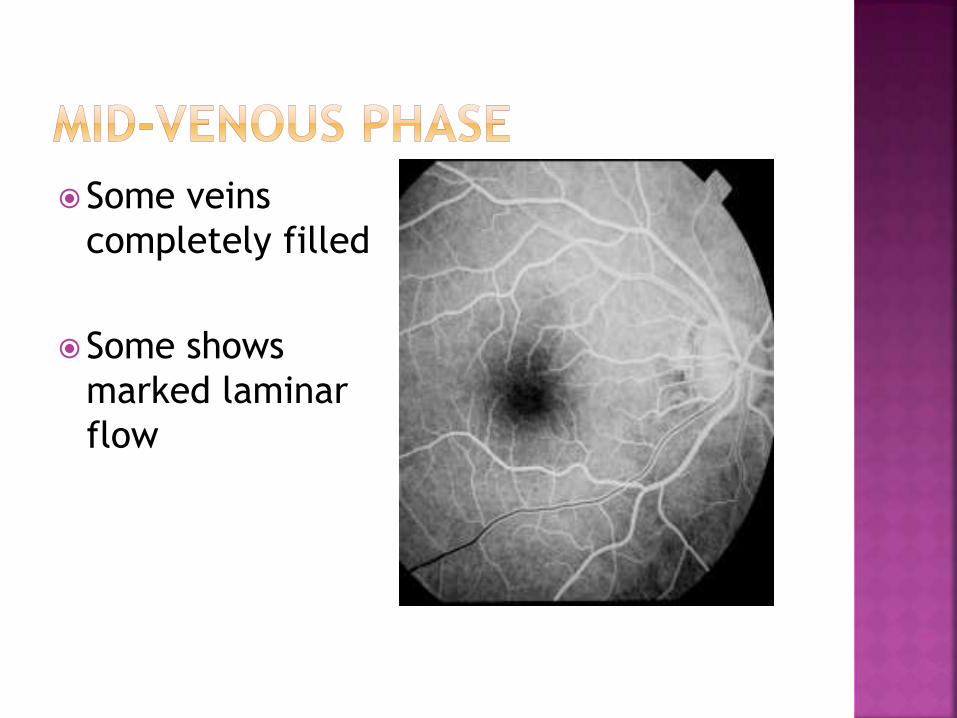
Some veins
completely filled
Some shows
marked laminar
flow
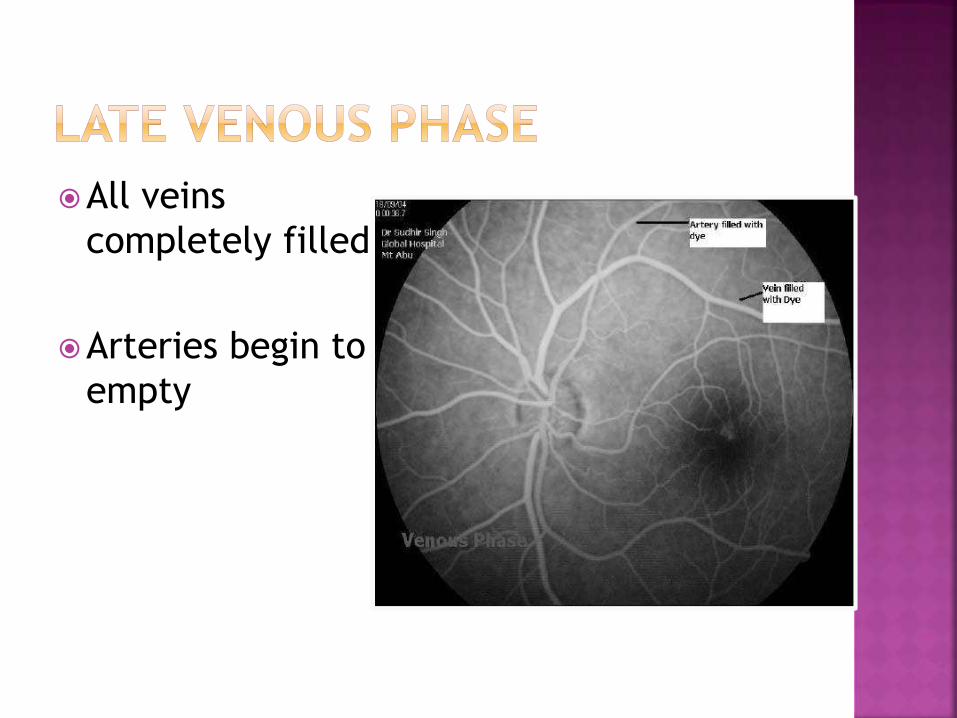
All veins
completely filled
Arteries begin to
empty
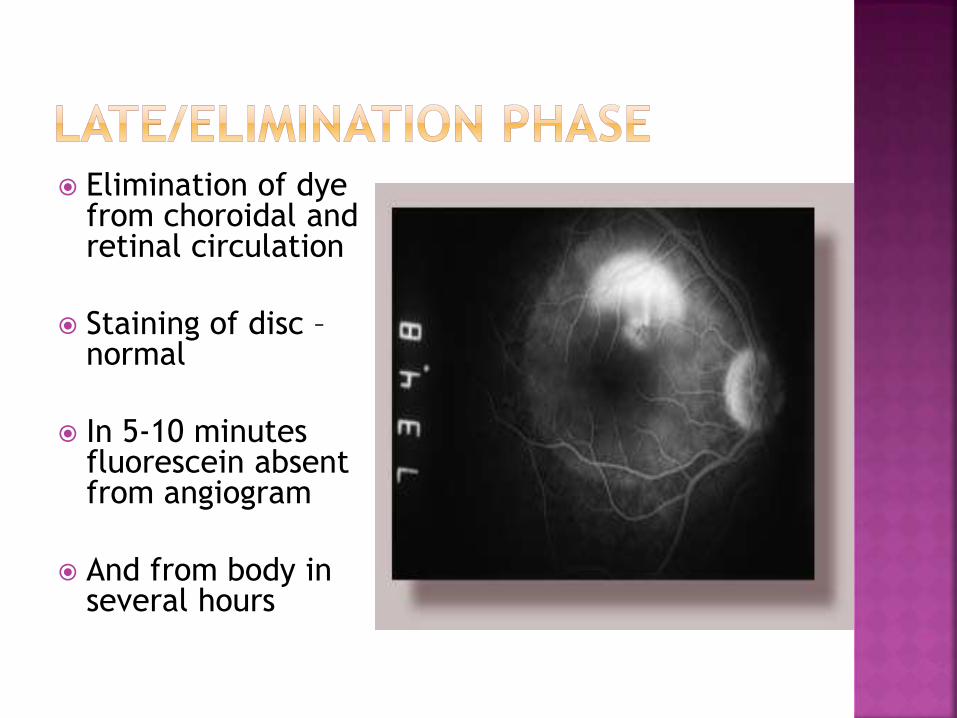
Elimination of dye from choroidal and retinal circulation
Staining of disc –normal
In 5-10 minutes fluorescein absent from angiogram
And from body in several hours
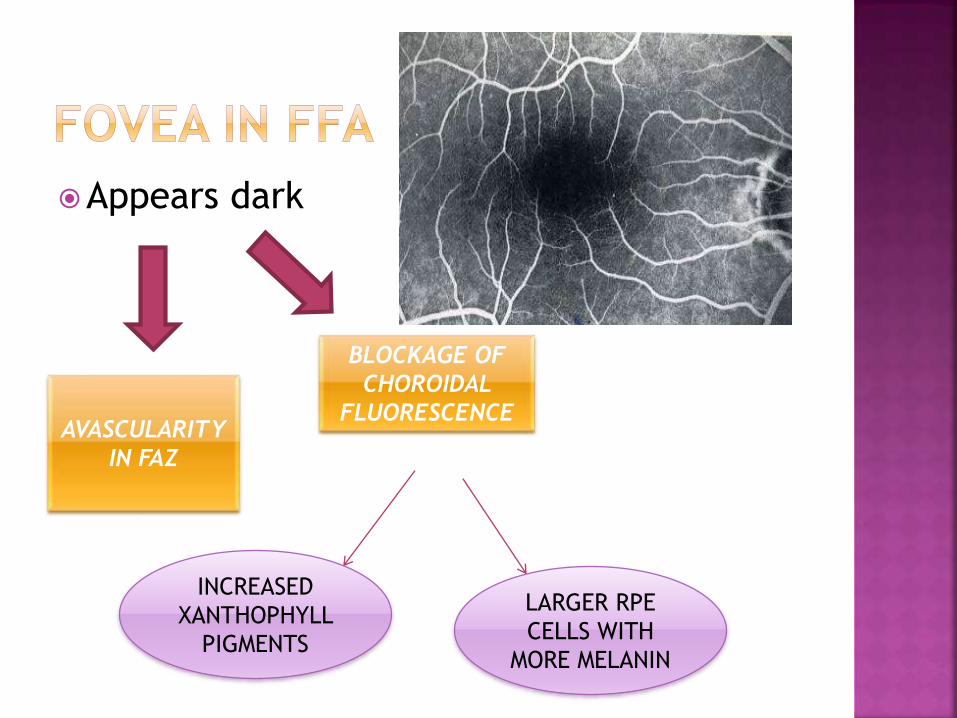
Appears dark
AVASCULARITY
IN FAZ
BLOCKAGE OF
CHOROIDAL
FLUORESCENCE
INCREASED
XANTHOPHYLL
PIGMENTS
LARGER RPE
CELLS WITH
MORE MELANIN
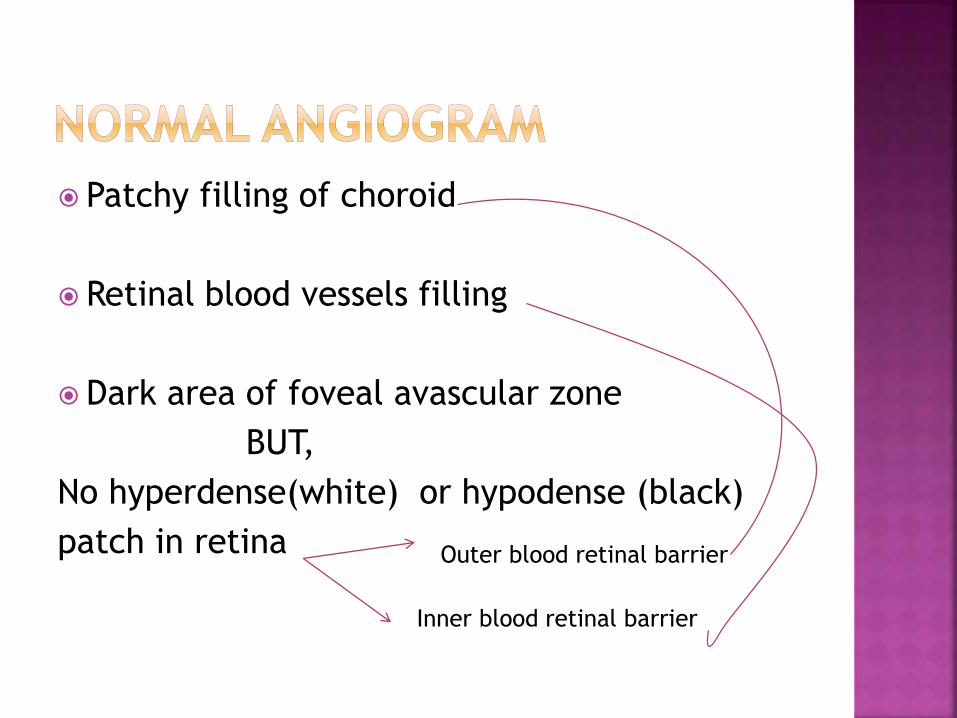
Patchy filling of choroid
Retinal blood vessels filling
Dark area of foveal avascular zone
BUT,
No hyperdense(white) or hypodense (black)
patch in retina Outer blood retinal barrier
Inner blood retinal barrier
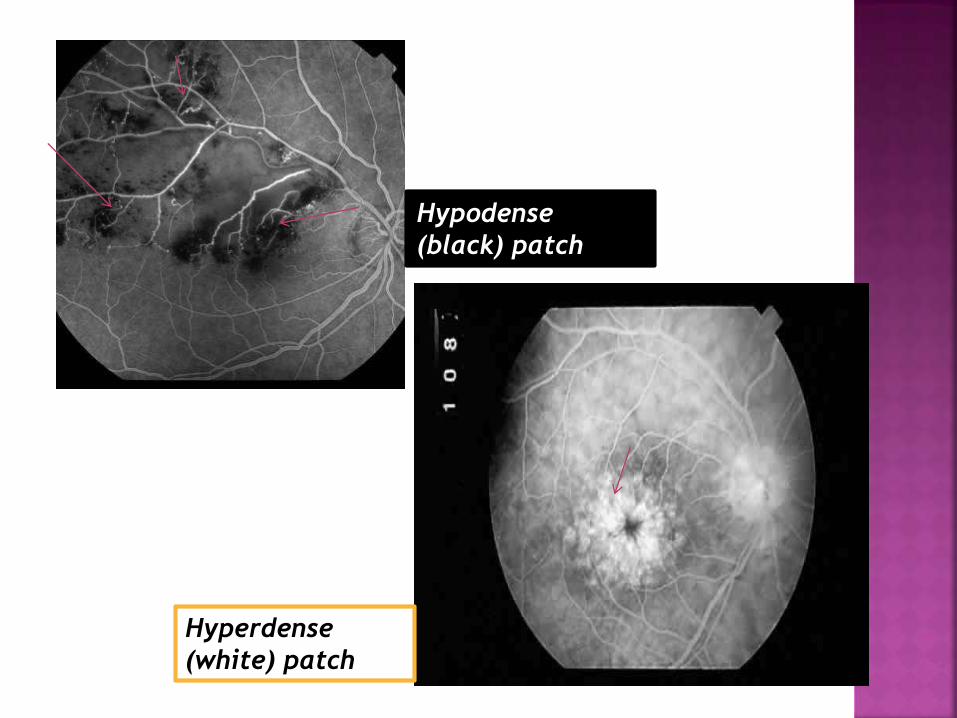
Hypodense
(black) patch
Hyperdense
(white) patch
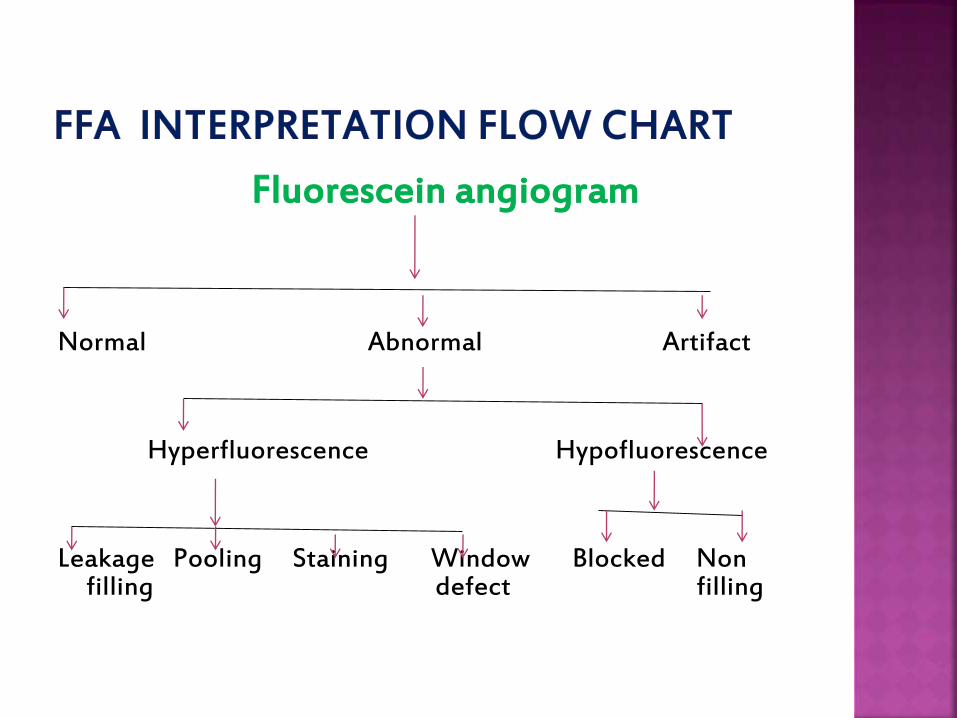
Fluorescein angiogram
Normal Abnormal Artifact
Hyperfluorescence Hypofluorescence
Leakage Pooling Staining Window Blocked Non filling defect filling
Hyperfluorescence and hypofluorescence can
alternate in same location
Especially in inflammatory disorder
1st hypofluorescence due to retinal oedema
Later hyperfluorescence due to increased
vascular permeability
Greater level of fluorescence than would be
found in normal angiogram
Occur due to:
-window defect
-increased accumulation of dye
leakage
pooling
staining
Defect in RPE – increased transmission of
choroidal fluorescence
Sharply defined hyperfluorescence - does not
change in shape and size
LEAKAGE
POOLING
STAINING
Escape of fluorescein from vessels with
pathologically increased permeability
Progressive increase in size and intensity
Papilledema
Abnormal choroidal vasculature(CNV)
Breaking of inner blood retinal barrier(cystoid macular oedema)
Abnormal retinal or disc vasculature(retinal neovascularization)
Proliferative Diabetic Retinopathy(NVD,NVE)
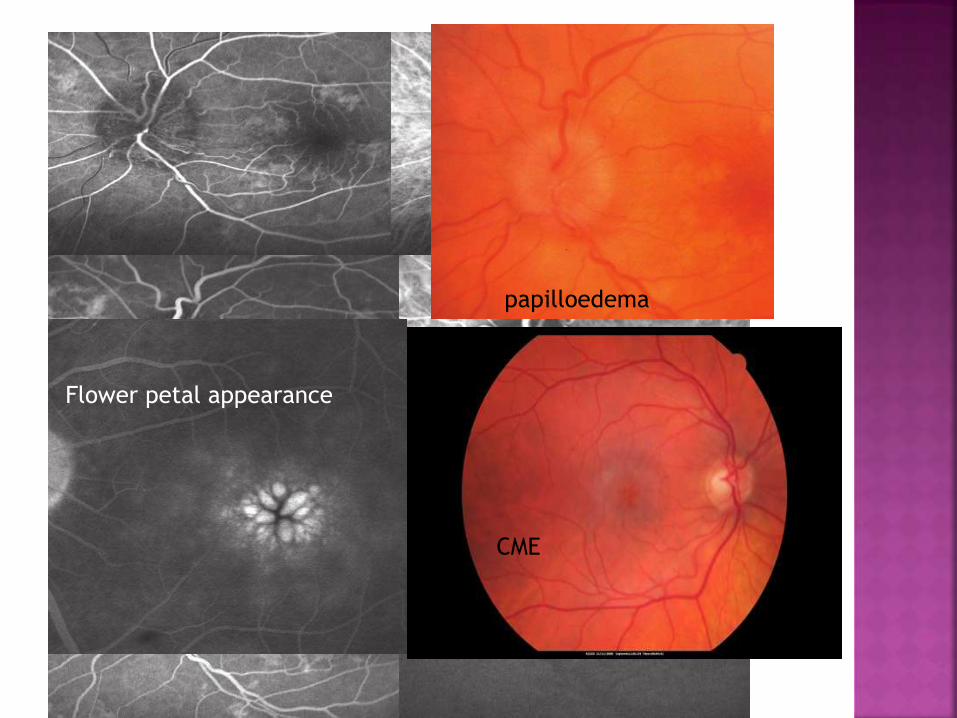
Flower petal appearance
CME
papilloedema
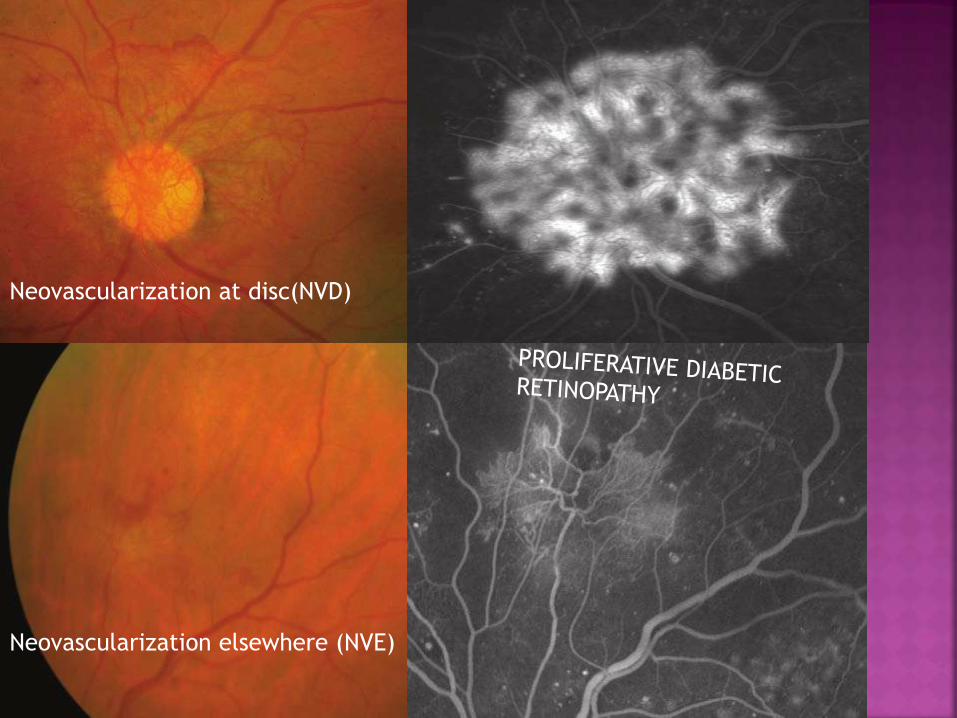
Neovascularization at disc(NVD)
Neovascularization elsewhere (NVE)
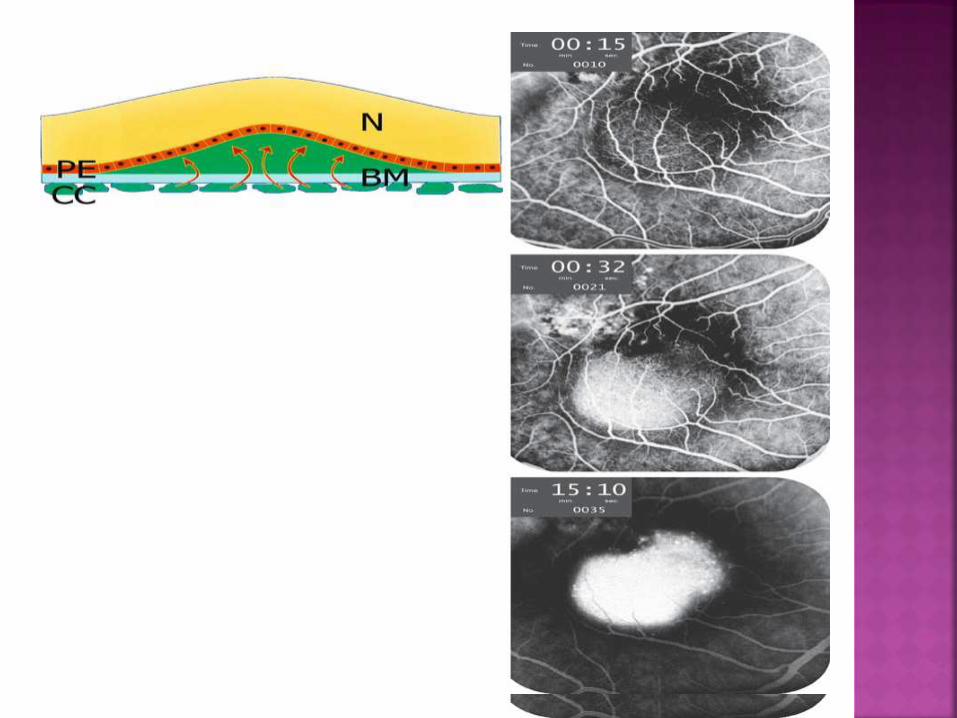
Accumulation of fluorescein in anatomical
space
Due to breakdown of outer blood retinal
barrier
A . In subretinal space
As in CSR
Early hyperfluorescence
Increase in size and intensity
B . In sub RPE space
As in PED
Early hyperfluorescence
Increase in intensity but
not in size
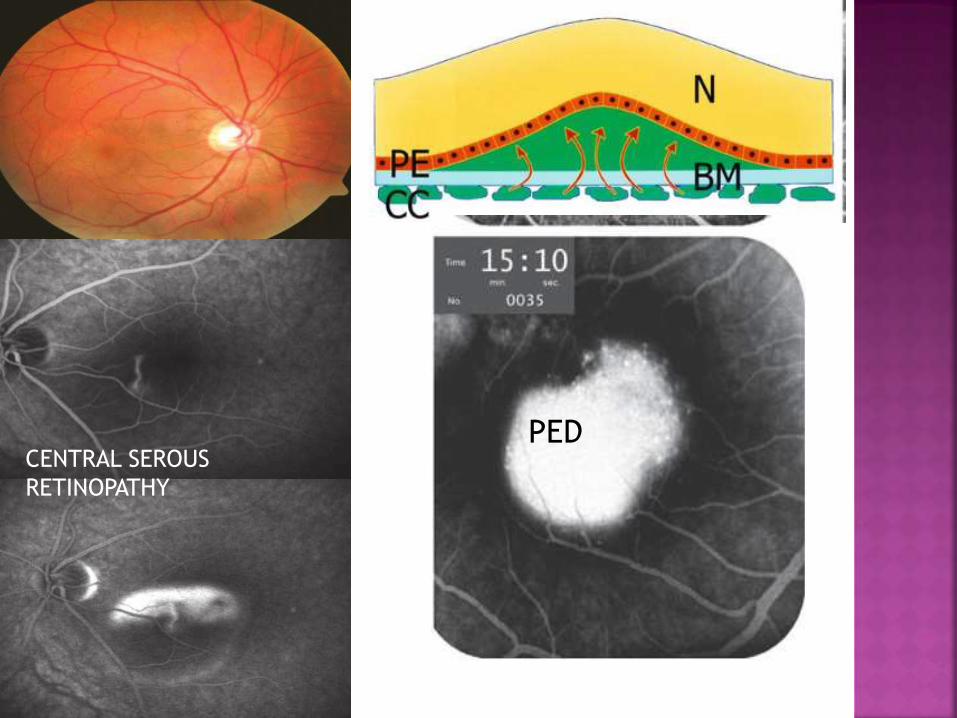
CENTRAL SEROUS
RETINOPATHY
PED
Accumulation of fluorescence within a tissue
Due to prolonged dye retention
Minimum hyperfluorescence in early and
midphase which increases in late phase
Can be seen in normal as well as
pathologically altered tissue
RETINAL
a. non-cystoid macular
oedema
b. Perivascular staining
SUB RETINAL
a. Drusens
b. Sclera
c. Lamina cribrosa
d. scars

Drusens in ARMD
Reduction or absence of fluorescein
Two causes
BLOCKED
FLUORESCENCE
VASCULAR
FILLING
DEFECTS
Optical obstruction (masking) of normal
density of fluorescein
Caused by lesions anterior to retina
Pre-retinal lesions eg.vitreousopacity,preretinal haemorrhage block all fluorescence
Deep retinal lesions eg.intraretinalhaemorrhage and hard exudates block only capillary fluorescence
Increased density of RPE eg.congenitalhypertrophy
Choroidal lesions eg.naevus
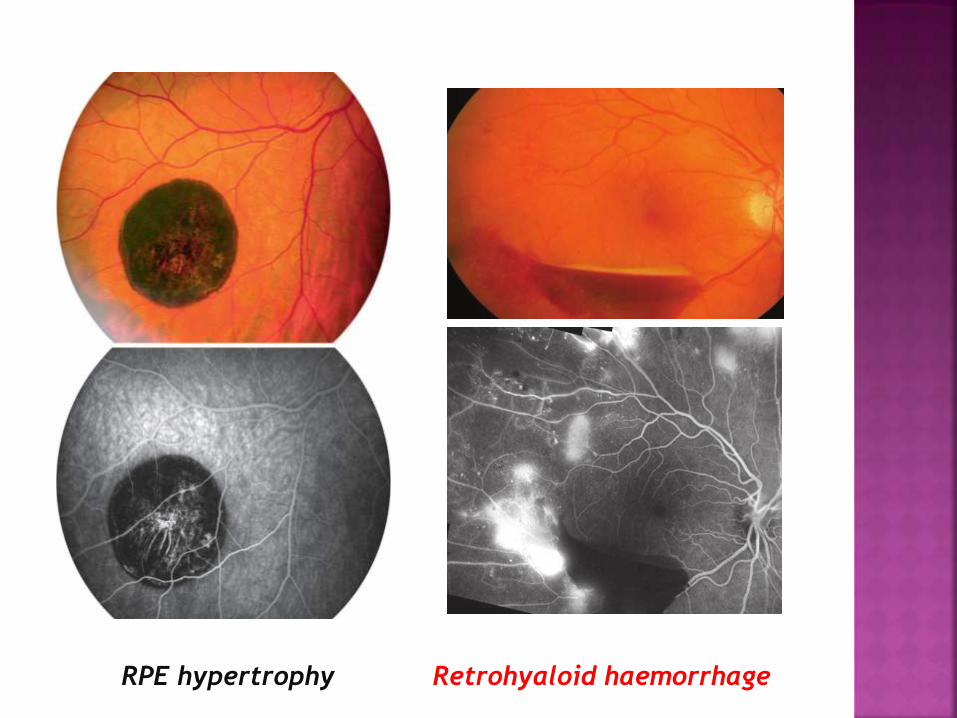
RPE hypertrophy Retrohyaloid haemorrhage
Inadequate perfusion of tissue with resultant
low fluorescein content
Avascular occlusion of choroidal circulation
or retinal arteries,veins and capillaries
Loss of vascular bed eg.severe myopic
degeneration – choroideremia
Emboli
arteriosclerosis
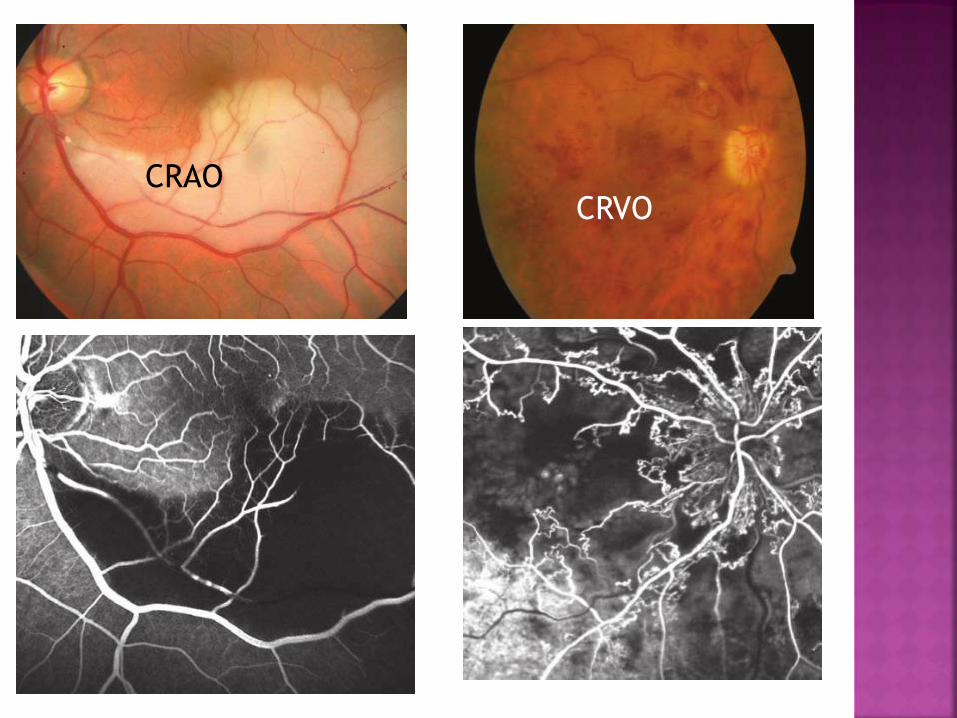
CRAOCRVO
All the process of occurrence of hyper or
hypo-fluorescence can be described under
following 3 phenomenons
A. OPTICAL PHENOMENON
B .MECHANICAL PHENOMENON
C. DYNAMIC PHENOMENON
Normal neurosensory retina is transparent
Normal RPE and Bruch’s Membrane are
semitransparent
Hence, we can see choroidal fluorescence
BUT, this transparency can be pathologically
increased or decreased
In case of blocked fluorescence ,
transparency is lost
SO, WE DO NOT SEE CHOROIDAL
FLUORESCENCE
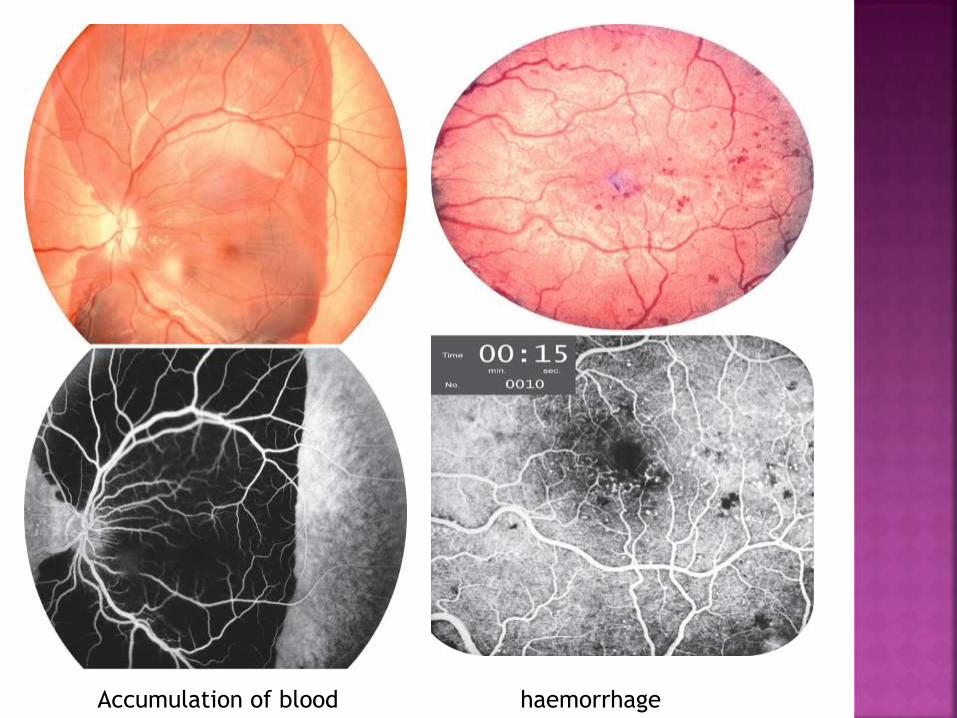
Accumulation of blood haemorrhage
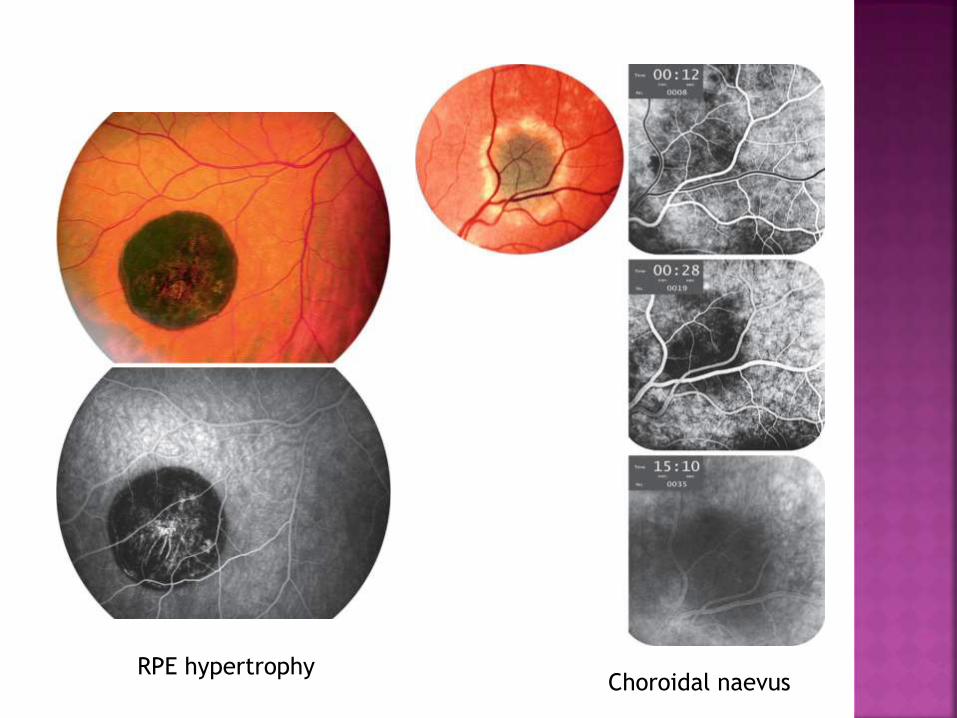
RPE hypertrophyChoroidal naevus
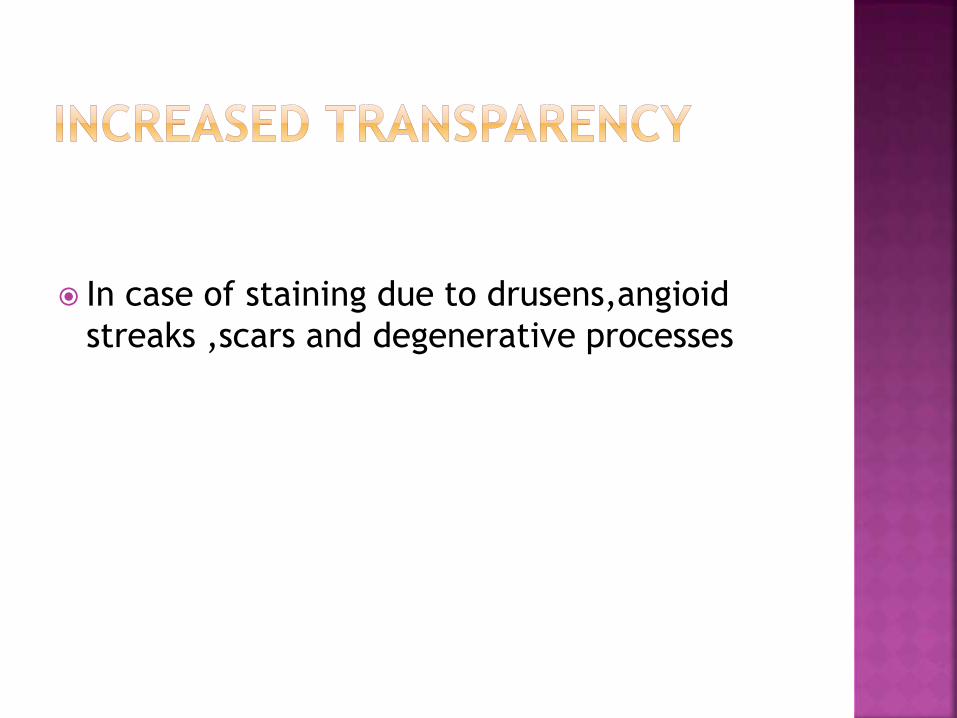
In case of staining due to drusens,angioid
streaks ,scars and degenerative processes
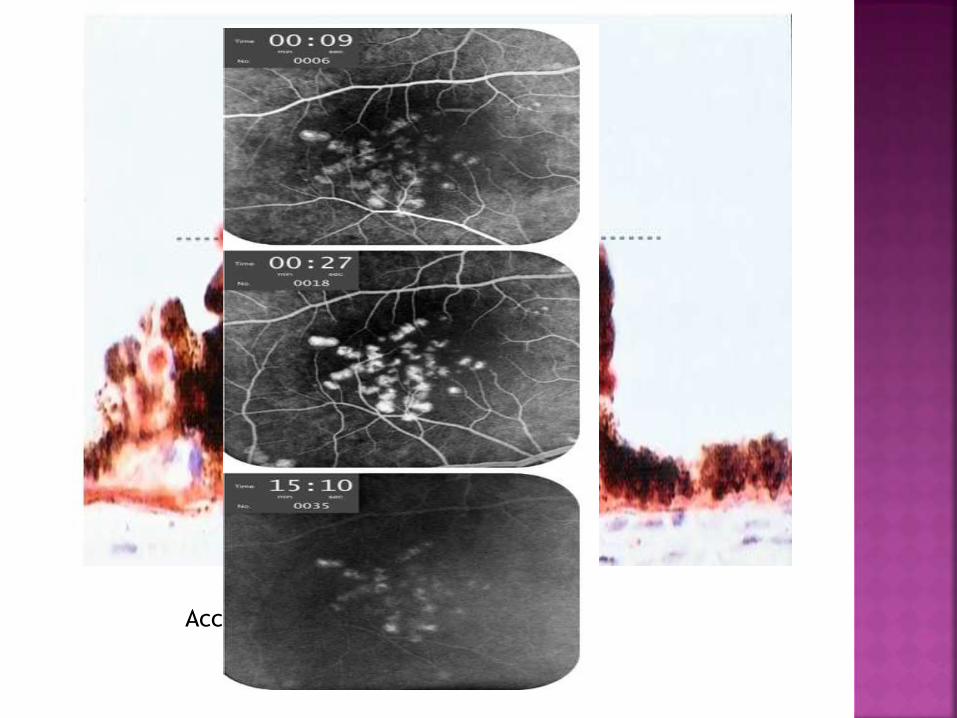
Accumulation of drusens under RPE
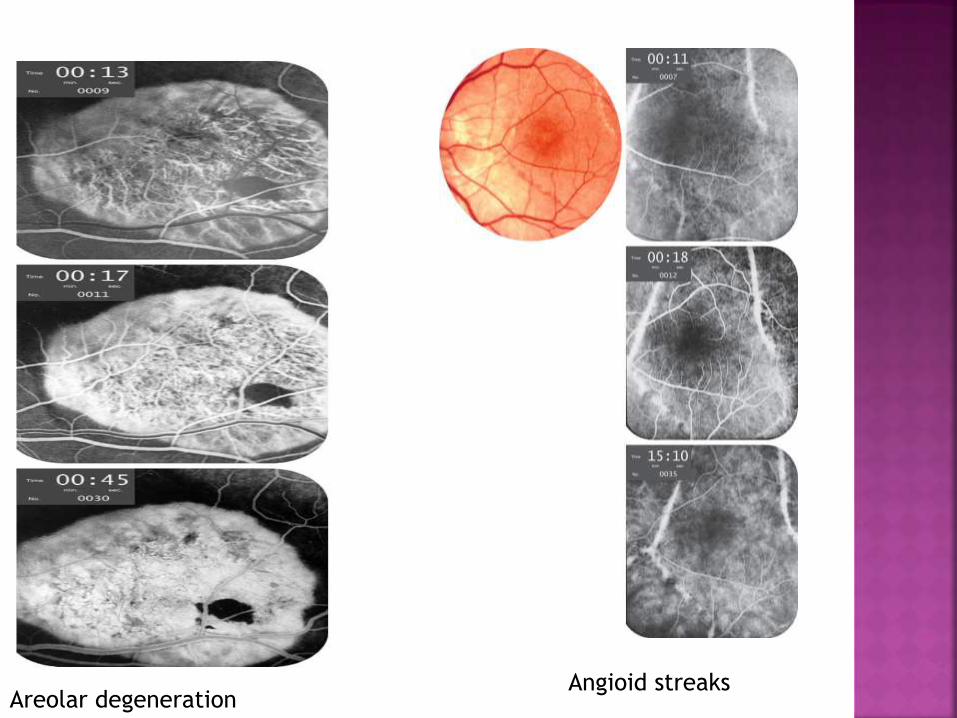
Angioid streaksAreolar degeneration
Related to adhesion of RPE to Bruch’s
Membrane
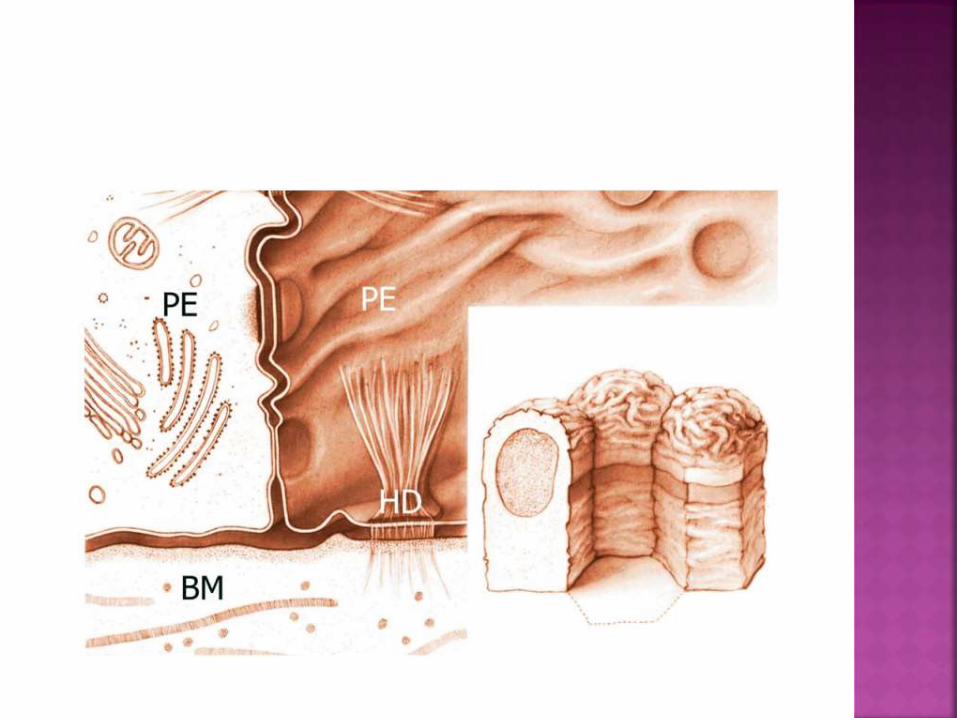
RPE firmly attached to Bruch’s membrane by
hemidesmosomes
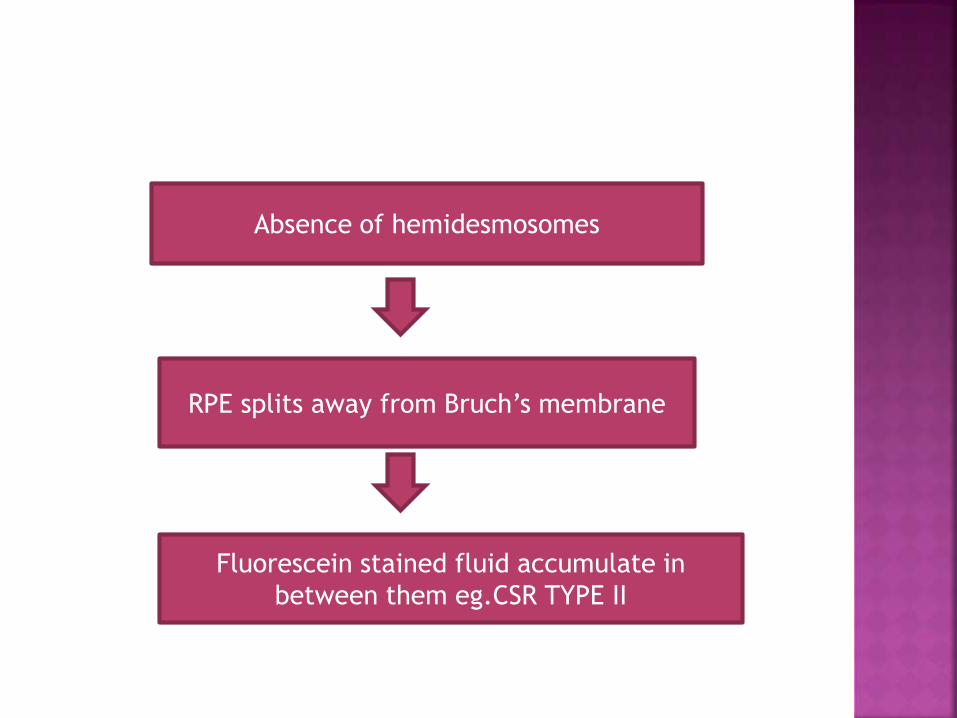
Absence of hemidesmosomes
RPE splits away from Bruch’s membrane
Fluorescein stained fluid accumulate in
between them eg.CSR TYPE II
Related to diffusion of fluorescein in ocular
tissue
Determined by inner and outer blood retinal
barrier I.E DIFFUSION BARRIER
Normal retinal vessels do not leak fluorescein
- due to zonula occludents in between
endothelial cells
These zonula occludents open up during
inflammatory process
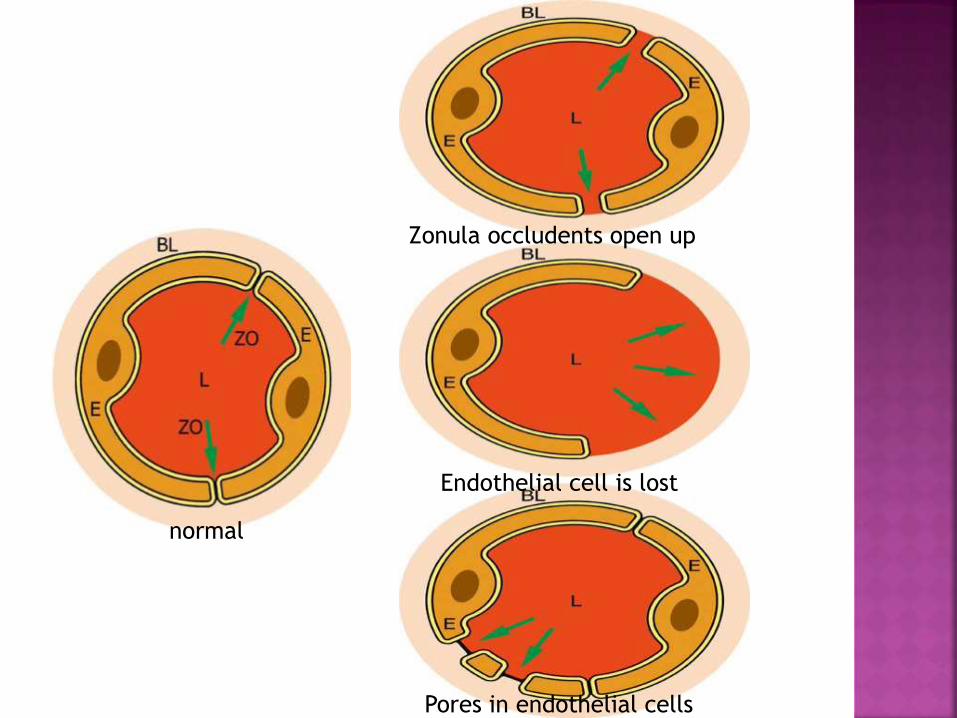
Zonula occludents open up
normal
Endothelial cell is lost
Pores in endothelial cells
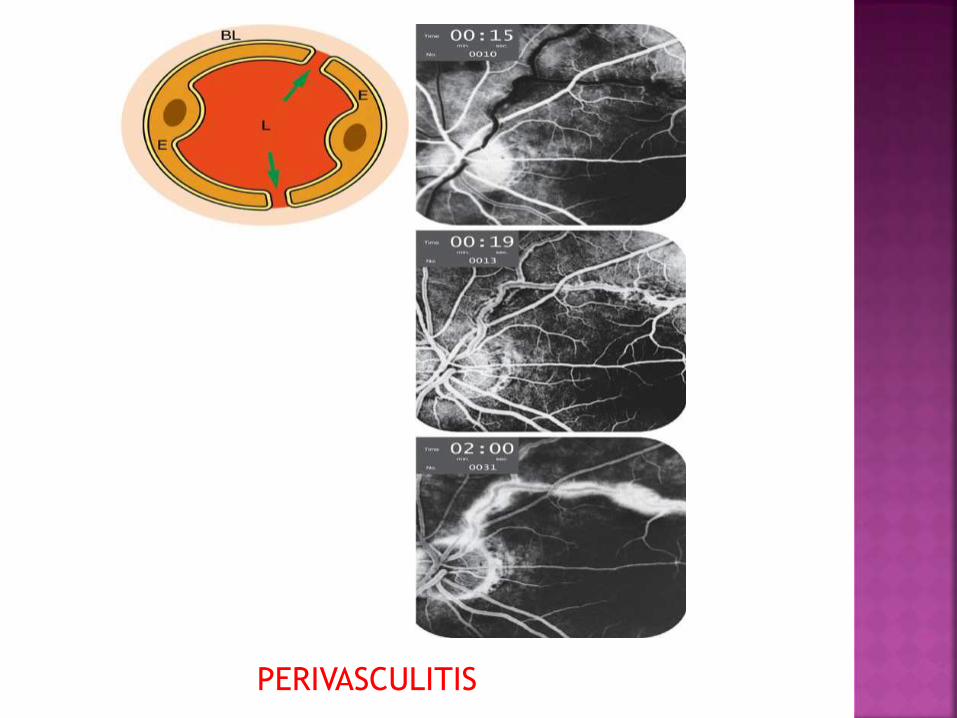
PERIVASCULITIS
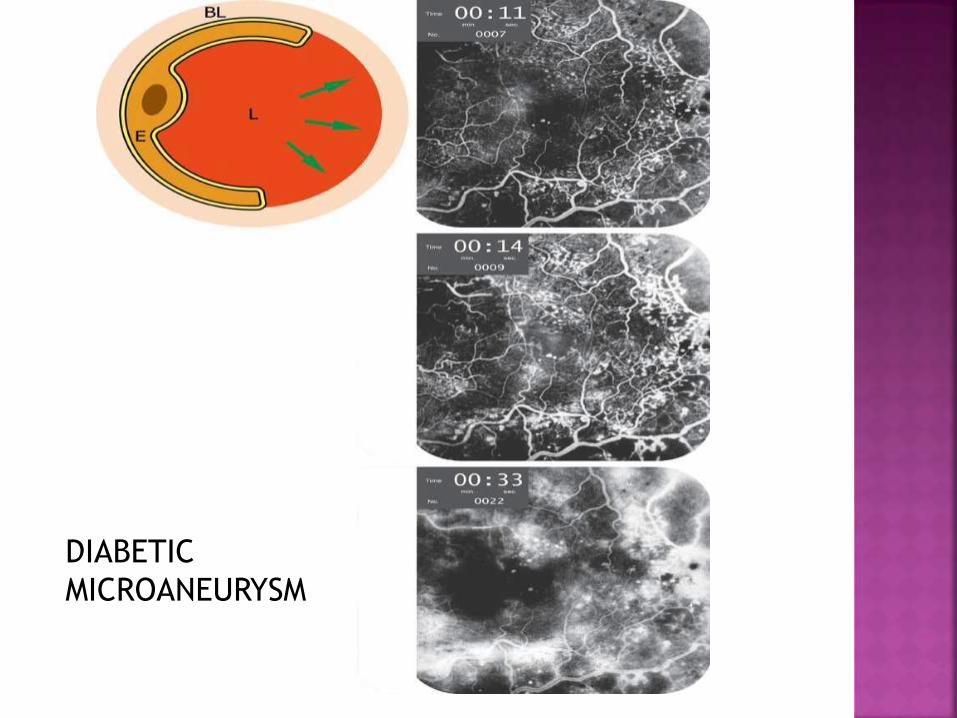
DIABETIC
MICROANEURYSM
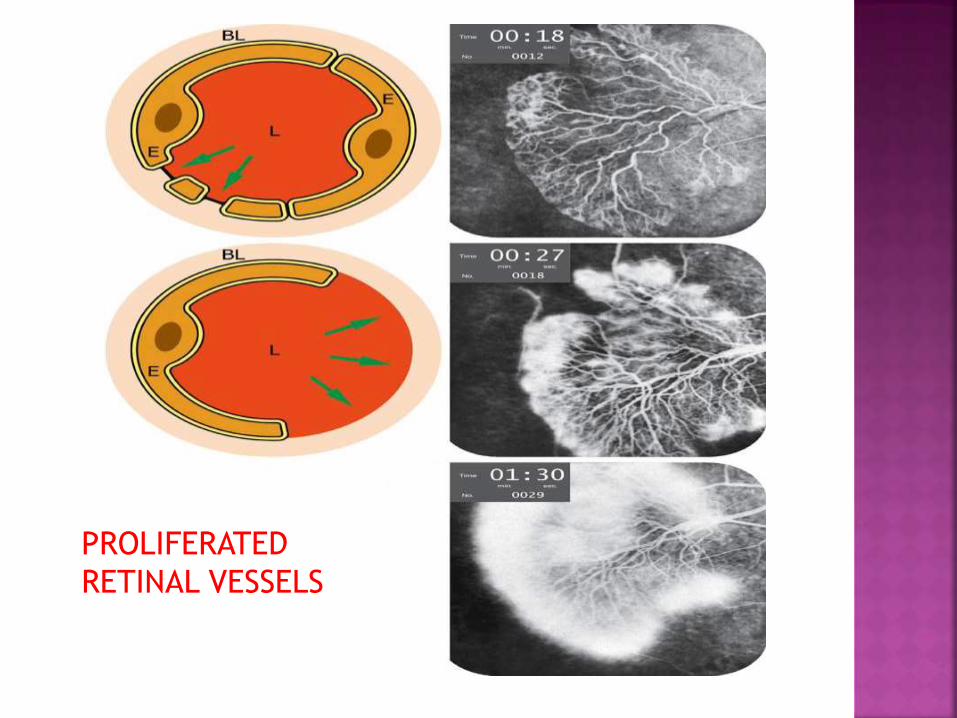
PROLIFERATED
RETINAL VESSELS
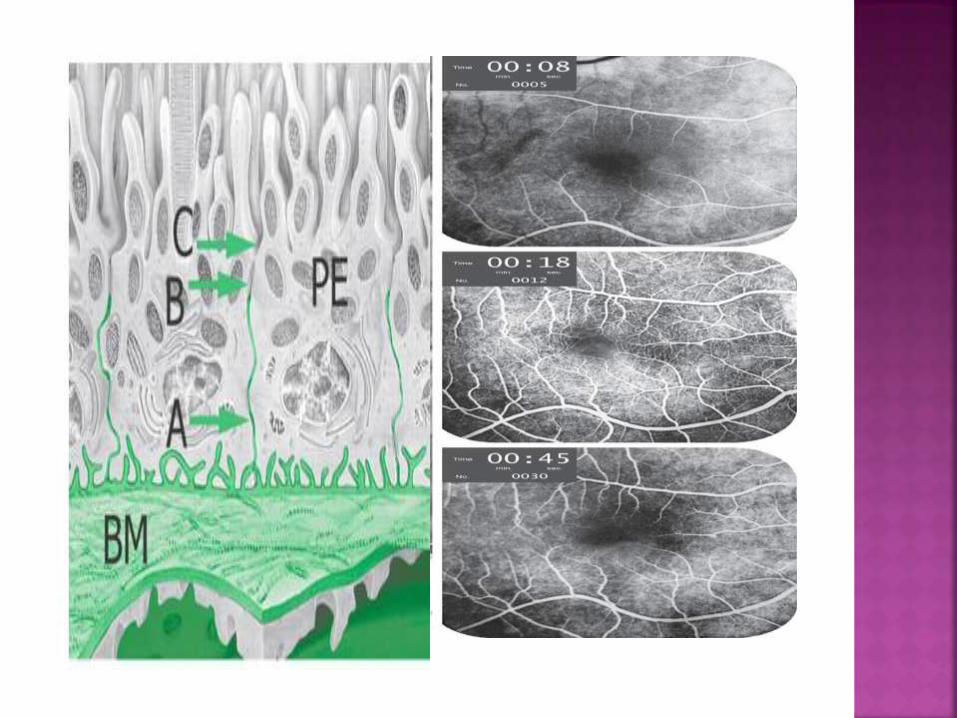
Normal RPE is tight
zonula occludens seal portion of all the
intercellular spaces of the pigment epithelial
monolayer.
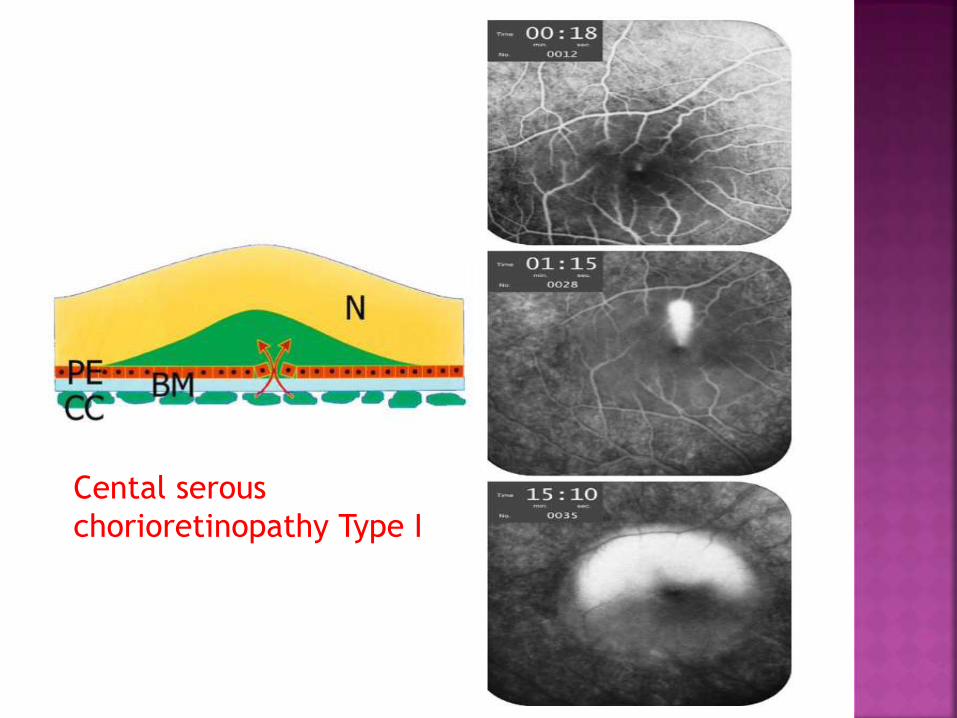
Cental serous
chorioretinopathy Type I
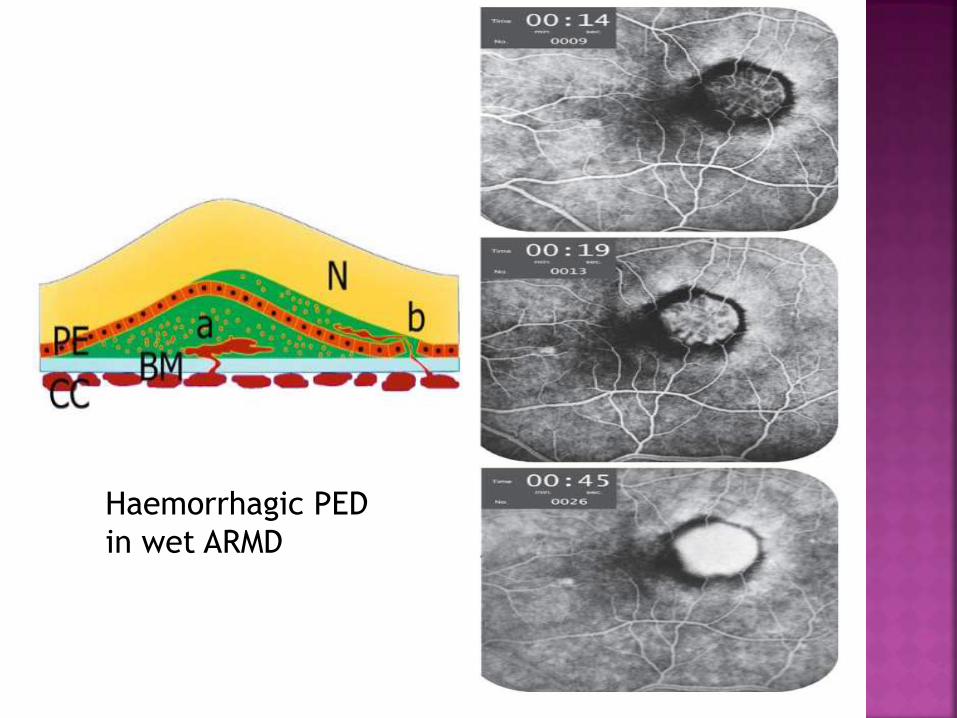
Haemorrhagic PED
in wet ARMD
Recommended

















