Embed Size (px)
Citation preview
BritishJournal ofOphthalmology, 1992,76,375-379
Fundus albipunctatus associated with conedystrophy
Yozo Miyake, Noriyasu Shiroyama, Shintaro Sugita, Masayuki Horiguchi, Katsuya Yagasaki
AbstractWe describe five unrelated patients in whomthe typical signs of fundus albipunctatus were _ . .t.accompanied by colour vision defects, bull's ."' ..X.eye or similar macular lesions, and severelydiminished full-field cone electroretinogramsindicating widespread damage to cones outsidethe macula. Ali patients had noticed nightblindness from childhood. Signs of retinitispunctata albescens, a disease of similar .appearance but with characteristics resemblingretinitis pigmentosa, were absent. We cannotbe sure whether these patients represent aprocess of fundus albipunctatus or a distinctdisease entity or a casual combination of Fig lBfundus albipunctatus and cone dystrophy.
Department ofOphthalmology, NagoyaUniversity School ofMedicine, Nagoya, JapanY MiyakeN ShiroyamaS SugitaM HoriguchiK YagasakiCorrespondence to:Yozo Miyake, MD,Department ofOphthalmology, NagoyaUniversity School ofMedicine, 65 Tsuruma-cho,Showa-ku, Nagoya 466,Japan.Accepted for publication15 November 1991
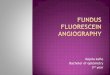
Figure I Fundusphotograph (A) andfluorescein angiography (B)ofthe left eye in case 1.
Fundus albipunctatus is a stationary disordercharacterised by myriads of yellow-white dots inthe fundus and an abnormally slow rate of darkadaptation. '4 The electroretinograms (ERGs)require a much longer dark adaptation time thannormal to reach maximum amplitude.Some reports have described cases of macular
degeneration associated with fundus albipunc-tatus.' 7-10 In the past 10 years we have had fivepatients in whom apparent fundus albipunctatuswas associated with macular degeneration. In allthe patients the rod function showed charac-teristic properties of fundus albipunctatus, butfull-field cone ERGs showed significantreduction.
Case reportsThe five unrelated patients had noticed nightblindness from childhood. The anterior segment,lens, and vitreous were normal in all patients,and none showed nystagmus or strabismus. The
Fig IA
results of general physical examinations androutine laboratory tests were also normal.
CASE 1A 49-year-old man with night blindness hadnoticed reduced vision over the previous 6years; his corrected visual acuity was 0-6 in eacheye. No one with night blindness or severely lowvision was found in his pedigree. His healthyparents were first cousins.
Discrete, dull white, uniform, dot-like lesions,seen over much of the fundi, were of greatdensity in the midperiphery of both eyes(Fig IA). The maculae each showed a bull's eyelesion. No attenuation of retinal vessels, opticatrophy, or pigmentary clumping was seen.Fluorescein angiography revealed irregular,spotty hyperfluorescence in the midperiphery,which did not correspond to the flecks; themacula showed ring-shaped hyperfluorescence(Fig IB). Visual fields were tested with theGoldmann perimeter using 3 ioptres. Theperipheral visual fields were normal, but centralsensitivity was slightly decreased in both eyes.Colour vision tests revealed severe blue-yellowand red-green defects. Dark adaptation wastested by using the Goldmann-Weeker adapto-meter in the right eye. A white test target of 110was presented at 150 of the upper retina. After 30minutes the visual threshold was approximately5 log units higher than normal. After 3 hoursit remained 0 5 to 10 log unit higher thannormal.
Full-field ERGs of the right eye (Fig 2) weremade by the standard recording technique pre-viously described." The mean (with 2 SD)amplitudes in the normal subjects after 30minutes of dark adaptation were 325 (140) [tV(scotopic (rod) b wave), 59 (21) RV (photopic(cone) b wave), and 38 (191) [tV (30 Hz flickerresponses). After 30 minutes of dark adaptation(Fig 2, upper tracings in case 1), no scotopic
375
on 14 July 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.76.6.375 on 1 June 1992. Dow
nloaded from
Miyake, Shiroyama, Sugita, Horiguchi, Yagasaki
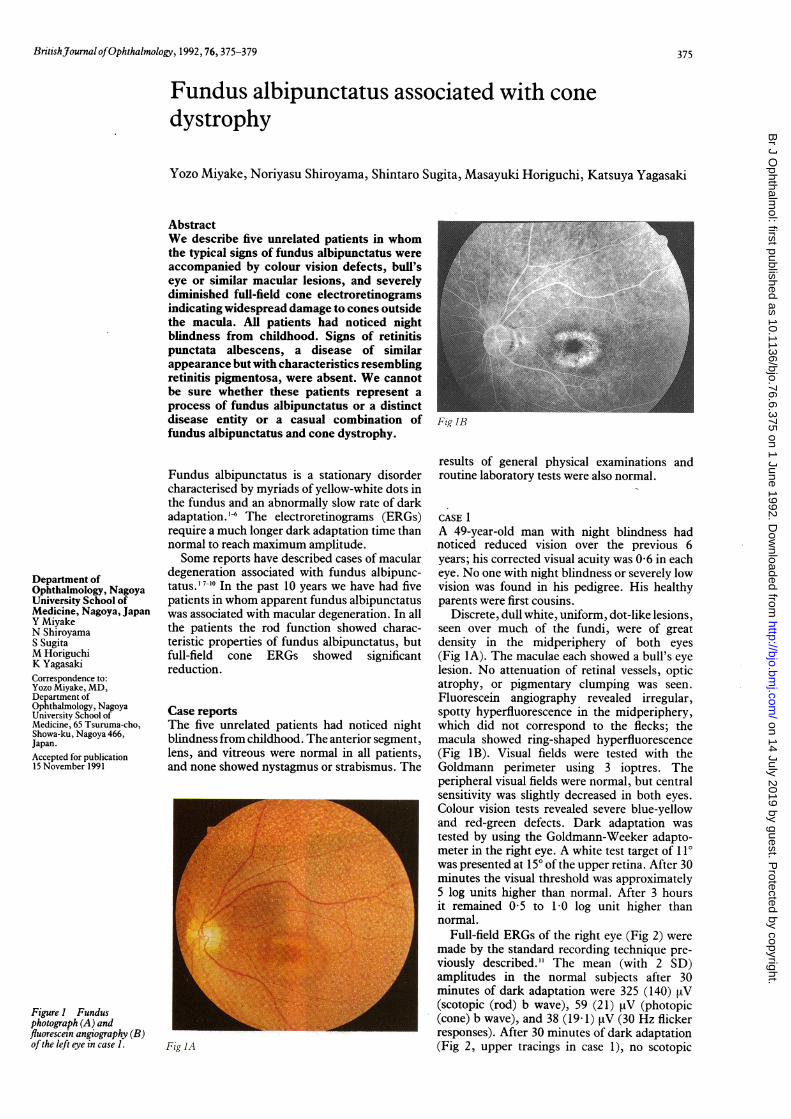
Figure 2 Full-fieldelectroretinograms ofanormal subject and cases Ito 5. In each case the uppertracings indicate theresponses recorded after 30minutes ofdark adaptation;the lower tracings indicatethe responses recorded afterprolonged dark adaptation(see textfor the details). Thearrows indicate the stimulusonset.
Scotopic Photopic 30Hz Flicker Bright white
Normal ' 4 ON OFFlOOgV100IlV L - 25AV 200AVS'Oms Sms 25¢L_ 252m
Case 1
Case 2
Case 3
Case 4 d-N$,i;
Case 5J\FJ\
(rod) or photopic (cone) ERG was recordable.The amplitudes of 30 Hz flicker responses were9-6 [tV with the delayed implicit time. A singlebright-flash (white bright) ERG showed severelydecreased b wave and moderately decreased awave. After 3 hours of dark adaptation (Fig 2,lower tracings in case 1), rod b wave was291 [tV in amplitude with normal implicit time.The cone b wave was 16-6 [tV in amplitude withdelayed implicit time. The 30 Hz flicker
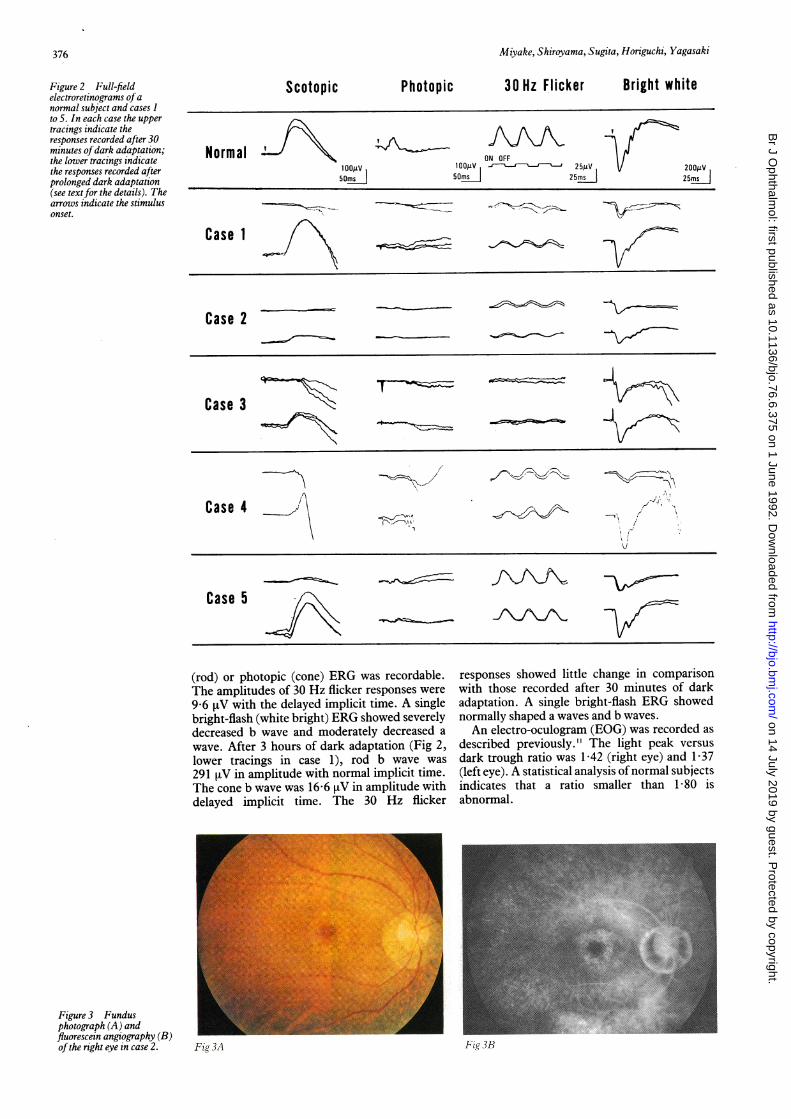
Figure 3 Fundusphotograph (A) andfluorescein angiography (B)ofthe right eye in case 2.
responses showed little change in comparisonwith those recorded after 30 minutes of darkadaptation. A single bright-flash ERG showednormally shaped a waves and b waves.An electro-oculogram (EOG) was recorded as
described previously." The light peak versusdark trough ratio was 1-42 (right eye) and 1-37(left eye). A statistical analysis of normal subjectsindicates that a ratio smaller than 1-80 isabnormal.
Fig 3B
376
Fig 3A
on 14 July 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.76.6.375 on 1 June 1992. Dow
nloaded from
Fundus albipunctatus associated with cone dystrophy
CASE 2A 49-year-old man with night blindness firstnoticed blurred vision and metamorphopsia inboth eyes in 1987. In 1989 his corrected visualacuity was 1 2 (right eye) and 1 0 (left eye), andin 1990 it was 0-6 (right eye) and 1-0 (left eye).No patient with night blindness was found in hispedigree, and his parents were not consan-guineous.The fundus and fluorescein angiography find-
ings (Figs 3 A, B) were similar to those of case 1.However, a localised, symmetrical chorioretinalatrophy was noted in the nasal inferior fundus ofboth eyes. Suggestive attenuation of retinalvessels was observed, and the optic disc wasnormal in both eyes. The peripheral visual fieldswere normal except for a depression in the areacorresponding to the chorioretinal atrophy; thecentral visual fields each had an annular scotoma.Colour vision tests revealed a severe blue-yellowdefect and moderate red-green defect. The visualthreshold was 3-8 log units higher than normalafter 30 minutes of dark adaptation and was 2 5log units higher than normal after 1 hour of darkadaptation.
In full-field ERGs recorded in the right eyeafter 30 minutes of dark adaptation (Fig 2, uppertracings in case 2), rod b wave was unrecordable,while cone b wave (15 ,uV) and 30 Hz flickerresponses (9-6 RV) were extremely reduced withdelayed implicit time. A single bright-flash ERGshowed severely decreased b and moderatelydecreased a waves. After 1-5 hours of darkadaptation (Fig 2, lower tracings in case 2) therod b wave was recorded with an amplitude of67 RV with normal peak time. Single bright-flash electroretinography recorded increased bwave amplitude. The cone and 30 Hz flickerresponses were not significantly different fromthose recorded after 30 minutes of dark adapta-tion.The EOG ratios were 1-75 (right eye) and 1 64
(left eye).
CASE 3This patient with night blindness was firstexamined by us in 1981 at the age of 40. Therewas no notable family history except that hisparents were first cousins. The fundus appearedto be typical of fundus albipunctatus, and themaculae were normal ophthalmoscopically. In1984 we found some pigmentary clumpings inthe nasal inferior area of the right eye which
developed into local chorioretinal atrophy duringa further 6-year follow-up.
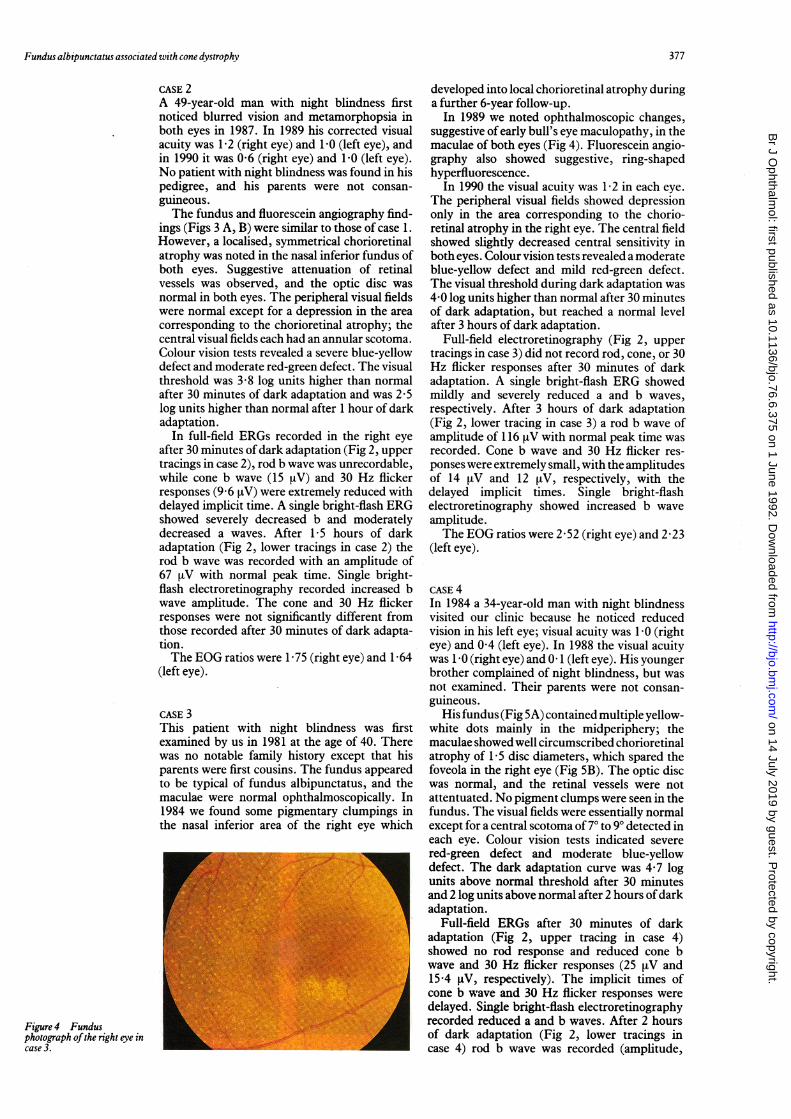
In 1989 we noted ophthalmoscopic changes,suggestive of early bull's eye maculopathy, in themaculae of both eyes (Fig 4). Fluorescein angio-graphy also showed suggestive, ring-shapedhyperfluorescence.
In 1990 the visual acuity was 1-2 in each eye.The peripheral visual fields showed depressiononly in the area corresponding to the chorio-retinal atrophy in the right eye. The central fieldshowed slightly decreased central sensitivity inboth eyes. Colour vision tests revealed a moderateblue-yellow defect and mild red-green defect.The visual threshold during dark adaptation was4-0 log units higher than normal after 30 minutesof dark adaptation, but reached a normal levelafter 3 hours of dark adaptation.
Full-field electroretinography (Fig 2, uppertracings in case 3) did not record rod, cone, or 30Hz flicker responses after 30 minutes of darkadaptation. A single bright-flash ERG showedmildly and severely reduced a and b waves,respectively. After 3 hours of dark adaptation(Fig 2, lower tracing in case 3) a rod b wave ofamplitude of 116 ,tV with normal peak time wasrecorded. Cone b wave and 30 Hz flicker res-ponses were extremely small, with the amplitudesof 14 ,tV and 12 [tV, respectively, with thedelayed implicit times. Single bright-flashelectroretinography showed increased b waveamplitude.The EOG ratios were 2 52 (right eye) and 2-23
(left eye).
CASE 4In 1984 a 34-year-old man with night blindnessvisited our clinic because he noticed reducedvision in his left eye; visual acuity was -0 (righteye) and 0-4 (left eye). In 1988 the visual acuitywas 10 (right eye) and 0 1 (left eye). His youngerbrother complained of night blindness, but wasnot examined. Their parents were not consan-guineous.
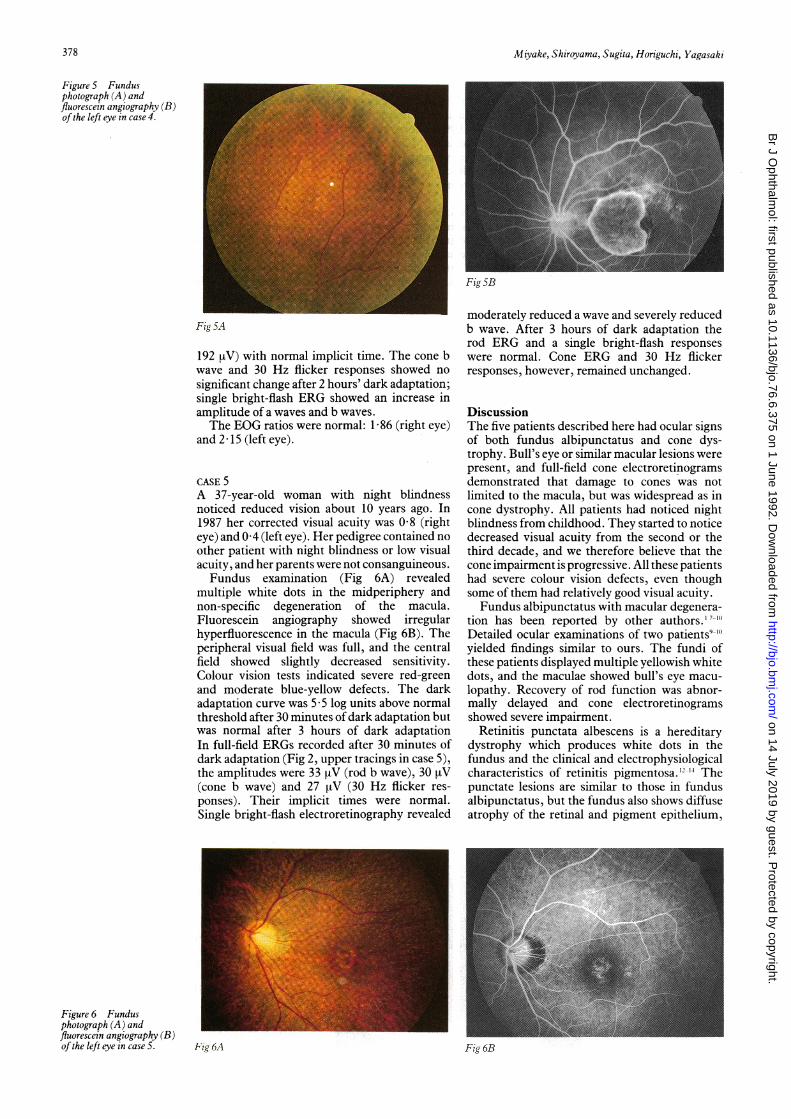
His fundus (Fig SA) contained multiple yellow-white dots mainly in the midperiphery; themaculae showed well circumscribed chorioretinalatrophy of 1 5 disc diameters, which spared thefoveola in the right eye (Fig SB). The optic discwas normal, and the retinal vessels were notattentuated. No pigment clumps were seen in thefundus. The visual fields were essentially normalexcept for a central scotoma of 70 to 90 detected ineach eye. Colour vision tests indicated severered-green defect and moderate blue-yellowdefect. The dark adaptation curve was 4 7 logunits above normal threshold after 30 minutesand 2 log units above normal after 2 hours ofdarkadaptation.
Full-field ERGs after 30 minutes of darkadaptation (Fig 2, upper tracing in case 4)showed no rod response and reduced cone bwave and 30 Hz flicker responses (25 vtV and15-4 [tV, respectively). The implicit times ofcone b wave and 30 Hz flicker responses weredelayed. Single bright-flash electroretinographyrecorded reduced a and b waves. After 2 hoursof dark adaptation (Fig 2, lower tracings incase 4) rod b wave was recorded (amplitude,
Figure 4 Fundusphotograph ofthe right eye incase 3.
377
on 14 July 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.76.6.375 on 1 June 1992. Dow
nloaded from
Miyake, Shiroyama, Sugita, Horiguchi, Yagasaki
Figure 5 Fundusphotograph (A) andfluorescein angiography (B)ofthe left eye in case 4.
Fig SB
Fig SA
192 [V) with normal implicit time. The cone bwave and 30 Hz flicker responses showed nosignificant change after 2 hours' dark adaptation;single bright-flash ERG showed an increase inamplitude of a waves and b waves.The EOG ratios were normal: 1-86 (right eye)
and 2-15 (left eye).
CASE 5A 37-year-old woman with night blindnessnoticed reduced vision about 10 years ago. In1987 her corrected visual acuity was 0-8 (righteye) and 0 4 (left eye). Her pedigree contained noother patient with night blindness or low visualacuity, and her parents were not consanguineous.Fundus examination (Fig 6A) revealed
multiple white dots in the midperiphery andnon-specific degeneration of the macula.Fluorescein angiography showed irregularhyperfluorescence in the macula (Fig 6B). Theperipheral visual field was full, and the centralfield showed slightly decreased sensitivity.Colour vision tests indicated severe red-greenand moderate blue-yellow defects. The darkadaptation curve was 5 5 log units above normalthreshold after 30 minutes of dark adaptation butwas normal after 3 hours of dark adaptationIn full-field ERGs recorded after 30 minutes ofdark adaptation (Fig 2, upper tracings in case 5),the amplitudes were 33 [tV (rod b wave), 30 iV(cone b wave) and 27 [tV (30 Hz flicker res-ponses). Their implicit times were normal.Single bright-flash electroretinography revealed
moderately reduced a wave and severely reducedb wave. After 3 hours of dark adaptation therod ERG and a single bright-flash responseswere normal. Cone ERG and 30 Hz flickerresponses, however, remained unchanged.
DiscussionThe five patients described here had ocular signsof both fundus albipunctatus and cone dys-trophy. Bull's eye or similar macular lesions werepresent, and full-field cone electroretinogramsdemonstrated that damage to cones was notlimited to the macula, but was widespread as incone dystrophy. All patients had noticed nightblindness from childhood. They started to noticedecreased visual acuity from the second or thethird decade, and we therefore believe that thecone impairment is progressive. All these patientshad severe colour vision defects, even thoughsome of them had relatively good visual acuity.Fundus albipunctatus with macular degenera-
tion has been reported by other authors.' 7-10
Detailed ocular examinations of two patients9`"yielded findings similar to ours. The fundi ofthese patients displayed multiple yellowish whitedots, and the maculae showed bull's eye macu-lopathy. Recovery of rod function was abnor-mally delayed and cone electroretinogramsshowed severe impairment.
Retinitis punctata albescens is a hereditarydystrophy which produces white dots in thefundus and the clinical and electrophysiologicalcharacteristics of retinitis pigmentosa. 12-14 Thepunctate lesions are similar to those in fundusalbipunctatus, but the fundus also shows diffuseatrophy of the retinal and pigment epithelium,
Fig 6A
Figure 6 Fundusphotograph (A) andfluorescein angiography (B)ofthe left eye in case 5.
378
Fig 6B
on 14 July 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.76.6.375 on 1 June 1992. Dow
nloaded from

Fundus albipunctatus associated with cone dystrophy
arterial narrowing, disc pallor, and often some
black pigment spicules. The symptoms includepermanent night blindness, peripheral field loss,and sometimes a loss of central vision. Someauthors consider that these disorders form a
continuum, but convincing evidence indicatesthey are separate entities. Using fundus reflec-tometry to study two brothers with fundusalbipunctatus, Carr and associates'5 noted thatthe slow dark adaptation that characterised thedisorder clinically corresponded to an abnor-mally slow rate of visual pigment regeneration.Thus our concept of fundus albipunctatus andretinitis punctata albescens is that the former is a
stationary disorder of visual pigment regenera-tion, while the latter is a progressive dystrophythat permanently damages the photoreceptorsand pigment epithelium.Our patients did not have retinitis punctata
albescens, because they had abnormally delayedrecovery of rod function, no attenuation ofretinal vessels (only case 2 showed suggestiveattenuation of retinal vessels), no disc pallor, anda normal or only slightly constricted peripheralvisual field. Moreover, it should be noted thatthe rod b wave after prolonged dark adaptationshowed normal implicit time in all patients. Itseems more likely that fundus albipunctatus wasassociated with cone dystrophy. Two of our
patients (cases 2 and 3) showed some pigmentspicules, localised in the midperipheral retina.Cone dystrophy may also show such changesduring the course of progression.' In theadvanced stage of cone dystrophy rods may alsobe affected, retinal vessels become attenuated,and pigment clumps and diffuse atrophy of theretinal pigment epithelium become apparent.
Once these characteristics have developed, thedifferential diagnosis from retinitis punctataalbescens may not be easy.
At present we cannot establish unequivocallywhether these patients represent a process offundus albipunctatus or an independent clinicalentity or simply the combined manifestations oftwo different diseases.Presented at the Annual Meeting of the Association for Researchin Vision and Ophthalmology, Sarasota, Florida, USA, 30 April1991.
I Krill AE. Hereditary retinal and choroidal diseases. Hagerstown:Harper and Row, 1977; 2: 739-824.
2 Carr RE. Congenital stationary night blindness. Trans AmOphthalmol Soc 1974; 72: 448-87.
3 Marmor MF. Dystrophies of the retinal pigment epithelium.In: Zinn KM, Marmor MF, eds. The retinal pigmentepithelium. Cambridge: Harvard University Press, 1979:424-53.
4 Francescheti A, Francois J, Babel J. Chorioretinal heredo-degeneration. Springfield: Thomas, 1974; 222-50.
5 Vannas S, Setala M. On atypical night blindness.Acta Ophthalmol (Kbh) 1958; 36: 849-59.
6 Miyake Y, Asano T, Sakai T, Watanabe I. ERG and EOG inretinitis punctata albescens. Acta Soc OphthalmolJ7pn 1972;76: 247-56.
7 Gass JDM. Stereoscopic atlas of macular diseases. Diagnosis andtreatment. 2nd ed. St Louis: Mosby, 1977: 184-5.
8 Scouras J, Chevaleraud J, Papastratigakis B. Macular involve-ment in retinitis albescens. J Fr Ophtalmol 1979; 2: 613-7.
9 Weleber RG. Retinitis pigmentosa and allied disorders. In:Ryan SJ, Ogden TE, eds. Retina. St Louis: Mosby, 1989; 1:346-8.
10 Sato S, lijima H. A case of fundus albipunctatus associatedwith cone dysfunction. Rinsho Ganka 1987; 41: 1307-10.
11 Miyake Y, Yagasaki K, Horiguchi M, Kawase Y, Kanda T.Congenital stationary night blindness with negative electro-retinogram. A new classification. Arch Ophthalmol 1986;104: 1013-20.
12 Lauber H. Die sogenaunte retinitis punctata albescens. KlinMonatsblAugenheilkd 1910; 48: 133-48.
13 Tamai A, Setogawa T, Kandori F. Electroretinographicstudies on retinitis punctata albescens. Am J Ophthalmol1966; 62: 125-31.
14 Ellis D, Heckenlively J. Retinitis punctata albescens. Fundusappearance and functional abnormalities. Retina 1983; 3:27-31.
15 Carr RE, Ripps H, Siegel IM. Visual pigment kinetics andadaptation in fundus albipunctatus. Doc Ophthalmol ProcSer 1974; 4:193-204.
379
on 14 July 2019 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.76.6.375 on 1 June 1992. Dow
nloaded from