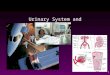
Functions of the Kidney
• Maintain electrolyte, acid-base balance
• “clear” the blood of toxins
• Make EPO, active Vitamin D
• gluconeogenesis, hormone metabolism

Kidney disorders
• Hyponatremia• Hypokalemia• Metabolic Alkalosis
– chloride responsive
– chloride unresponsive
• Metabolic Acidosis– anion gap
– non-anion gap
• Hypernatremia• Hyperkalemia• Calcium• Phosphate• Magnesium

Renal Failure
• A growing epidemic
• 350,000 on renal replacement therapy
• 80-90,000 new every year
• Over one million thought to be in pipeline


Creatinine
• Normal 0.8-1.2mg/dl; lower in pregnancy and cirrhosis and chronically ill/aged, higher in muscleheads, pts taking creatine and in rhabdo.
• Cephalosporins/ketosis change assay to increase creat, cimetidine and trimethoprim block secretion to increase

BUN
• Normal 5-10mg/dl
• Increased with GFR, heavy GI bleed, TPN, hypercatabolic states (steroids, sepsis) and prerenal volume depletion-( >20x creat), such as CHF, cirrhosis, nephrosis, sepsis and salt depletion.
• When >100mg/dl, often associated with uremia

Hematuria
• Definition
– straightforward- >3-5 RBC’s per high power field
– Definitions may vary

Causes of hematuria
• Anatomic• Kidney• Ureters• Bladder• Urethra• Prostate or GYN

Severe Lesions Moderate lesions
Bladder CancerRenal cell CancerProstate cancerObstructing stoneLymphomaTranitional cell cancerMetastatic disease
Renal disease
Aortic aneurysm
StonesUTIRefluxInterstitial cystitisBladder diverticulumRadiation cystitisPapillary NecrosisRenal diseaseAV fistulaBPHProstatitisUrethral stricture

URINALYSIS

URINALYSIS

URINALYSIS

Proteinuria
• Microalbuminuria-dip (-), 30-300 mg/day of albuminuria. Seen in diabetes, vascular dz
• Dip(+) urine, 300mg-2 g seen in glomerular and tubular disease
• Dip (+) urine, > 2g/day, glomerular disease
• Dip (-) urine, still can be overflow protein from myeloma, use SSA or UPEP

IVP

Renal Ultrasound

CT (spiral)

Hypertension
• Defined as resting, repeated BP > 140/90
• Risk parallels severity of increased BP and other risks for vasc. Dx-male, AA, smoking, diabetes, cholesterol, age
• Treat mild BP with diet, weight loss, exercise
• Move onto drugs when above fails
• Approx 5% of pts have secondary causes, more when BP severely elevated

HTN- secondary causes
• Truncal obesity- Cushing’s
• Labile HTN - Pheo
• Bruits- Renal artery stenosis
• Decreased fem pulses- Coarctation
• Abdominal/flank mass- Polycystic kidneys
• Increased creat/edema- Renal disease
• Hypercalcemia- Hyperparathyrodism
• Hypokalemia- Hyperaldosteronism/licorice/ Liddle’s syndrome

HTN- Rx
• Diabetics, renal disease with proteinuria, Cardiac injury- ACE inhibitors
• Must watch for reversible hyperkalemia, renal insufficiency, cough, angioedema
• Think bilateral renal artery stenosis when acute renal failure occurs.
• Do not use ACEi or ARBs in pregnancy

Glomerular disease
• Hematuria, proteinuria or both
• RBC casts, especially when proliferative
• Nephritis: hematuria, hypertension, renal insufficiency and edema
• Nephrosis; proteinuria (nephrotic>3.5g/d) with edema, hypoalbuminemia and hypercholesterolemia
• Idiopathic or part of systemic disease

FSGS

Membranous

MPGN

Diabetes

Amyloid

IgA Nephropathy

Chronic renal failure
• Diabetes
• HTN
• Glomerular disease (IgA, membranous, FSGS)
• PCKD
• SLE
• Interstitial disease
• Heriditary/ Congenital

PKD
• Autosomal dominant (1 in 800)
• > 2 cysts/kidney by age 30
• Large cysts with chance of infection/hemorrhage, assoc with berry aneurysm, diverticulosis, floppy valves, other organ cysts (liver/panc/ovarian)
• Treat infection with Cipro
• NO Rx for disease yet

ADPCKD

Interstitial disease
• Reflux nephropathy with pyelo
• NSAIDS/TYLENOL/Pb/heavy metals
• SLE/Sjogren’s/Sarcoid/TB
• Chinese herbs
• Usually mild HTN, mild proteinuria, pyuria– hypercalcemia for granulomatous disease

Chronic renal failure
• Clearance- if inadequate, dialysis/transplant
• Anemia- normochromic,normocytic treated with EPO and iron
• Bones- high phos and low Vit D cause low Ca++, high PTH--Rx with PO4 binders and Vit D
• Access- potential for steal/infection/high output heart failure

Stalling ESRD
• Blood pressure control
• ACE inhibitors/ ESRD
• Low salt, low protein diet
• ? Treatment of underlying disease
• Preventing toxicities

HYPERKALEMIA

Treating anemia
• Improves energy, sexual function, mentation, quality of life and possibly reduces LVH, angina, death
• Effective treatment with iron, EPO, NESP
• Careful to screen for other causes of anemia

Protecting the bones
• Limit phosphate intake
• Phosphate binders– Calcium or Renagel
• Vitamin D
• Monitor labs

Protect the heart??
• Exercise
• Healthy diet
• NO SMOKING, Limited EtOH
• ? Lipid management
• ?Aspirin

Dialysis
• Start for low clearance, esp if poor nutrition
• Outcome marker is albumin
• Hemodialysis most common, initial comp is dysequilibrium from rapid decrease of osmolality. Chronic complications of hypotension and cramping, arrythmia
• Death from heart disease, infection, cancer, access failure, discontinuation

Peritoneal dialysis
• Must do large volume, frequent exchanges for adequacy
• Less anemia and high blood pressure
• Peritonitis less common but still well represented. Usually Staph (70-80%) or E. coli (15-20%). Rarely fungal
• Treat with appropriate antibiotic IP, pull catheter if fungal or fails RX

Transplant
• Highly effective- 90 % 1 year success
• LRD>CAD
• Problems are immunosuppression, rejection
• Infections are early bacterial (post-op), viral after 1 month (CMV), PCP in first year;prophylaxis effective
• Technical problems;obstruction and renal artery stenosis have usual sequelae/RX

Transplant
• Loss of kidney function– Death (cards late, infection early)– Chronic rejection– Cyclosporine toxicity– Recurrent disease
• FSGS, MPGN, membranous, IgA, oxalosis
• NOT heriditary disease (PKD, cystinosis, Alport)
Recommended