Embed Size (px)
Citation preview

Functions of urinary system Anatomy of kidney Urine formation
glomerular filtration tubular reabsorption tubular secretion
Urine and renal function tests Urine storage and elimination

Is the passive transport of WATER across a selectively permeable membrane

Two kidneys
23-3
Two ureters
One urethra

Filters blood plasma returns useful substances to blood eliminates waste
Regulates osmolarity of body fluids, blood volume, BP acid base balance
Secretes renin and erythropoietin
Detoxifies free radicals and drugs Gluconeogenesis

Urea (most abundant) proteinsamino acids NH2 removed
forms ammonia liver converts to urea
Uric acid nucleic acid catabolism
Creatinine creatine phosphate catabolism
Renal failure azotemia is defined as BUN,
nitrogenous wastes in blood uremia is a term used more loosely =
toxic effects of nitrogenous wastes
Ornithine Cycle

Separation of wastes from body fluids and eliminating them; by four systems Lungs: CO2
Skin: water, salts, lactic acid, urea Digestive: water, salts, CO2, lipids, bile pigments,
cholesterol Urinary: many metabolic wastes, toxins, drugs,
hormones, salts, H+ and water
23-6
Position, weight and size retroperitoneal, level of T12 to L3 about 160 g each about size of a bar of soap (12x6x3 cm)
Shape lateral surface - convex; medial - concave
Connective tissue coverings renal fascia: binds to abdominal wall adipose capsule: cushions kidney renal capsule: encloses kidney like cellophane wrap
23-7

Renal cortex: outer 1 cm Renal medulla: renal columns, pyramids - papilla Lobe of kidney: pyramid and it’s overlying cortex
23-8

Notice where the nephron sits Where is the glomerulus?
Nephrons connect to collecting ducts

- Glomerulus (vascular) - Bowman’s Capsule (collecting)

Renal artery interlobar arteries (up renal columns, between lobes)
arcuate arteries (over pyramids) interlobular arteries (up into cortex) afferent arterioles glomerulus (cluster of capillaries) efferent arterioles (near medulla vasa recta) peritubular capillaries interlobular veins arcuate veins interlobar veins
Renal vein
23-11

23-12
The glomerulus is a portal system
no segmental veins

Proximal convoluted tubule (PCT) longest, most coiled, simple
cuboidal with brush border Nephron loop - U shaped;
descending and ascending limbs thick segment (simple
cuboidal) initial part of descending limb and part or all of ascending limb, active transport of salts
thin segment (simple squamous) very water permeable
Distal convoluted tubule (DCT) – typo on pg 901 cuboidal, minimal microvilli
Arcuate artery and vein
Interlobular artery and vein

Collecting duct several DCT’s join
Flow of glomerular filtrate: glomerular capsule PCT
nephron loop DCT collecting duct papillary duct minor calyx major calyx renal pelvis ureter urinary bladder urethra
23-14
Arcuate artery and vein
Interlobar artery and vein
Arcuate artery and vein
Interlobular artery and vein

True proportions of nephron loops to convoluted tubules shown
Cortical nephrons (85%) short nephron loops efferent arterioles branch off peritubular
capillaries Juxtamedullary nephrons (15%)
very long nephron loops, maintain salt gradient, helps conserve water
23-15
Arcuate artery and vein
Interlobular artery and vein

Peritubular capillaries shown only on right
23-16


23-18

Fenestrated endothelium 70-90nm pores exclude blood cells
Basement membrane proteoglycan gel, negative charge
excludes molecules > 8nm blood plasma 7% protein, glomerular
filtrate 0.03% Filtration slits
podocyte arms have pedicels with negatively charged filtration slits, allow particles < 3nm to pass
23-19

23-20
GFR = mls of filtrate formed per minute
filtration coefficient (Kf) depends on permeability and surface area of filtration barrier
Blood hydrostatic pressure is higher than usual capillaries
99% of filtrate reabsorbed, 1 to 2 L urine excreted

23-21
GFR = mls of filtrate formed per minute
filtration coefficient (Kf) depends on permeability and surface area of filtration barrier
Blood hydrostatic pressure is higher than usual capillaries
99% of filtrate reabsorbed, 1 to 2 L urine excreted

Hypertension ruptures glomerular capillaries Leads to scarring of glomeruli Scarred glomeruli have decreased permeability
thus decreased GFR Nitrogenous wastes accumulate Kidney failure

Inappropriate increase in GFR, urine output rises can result in dehydration and electrolyte depletion
If disease GFR wastes are not efficiently excreted (azotemia possible)
If MAP rose from 100 to 125 mmHg then, in the absence of control mechanisms, urine output would rise to 45 liters/day
GFR controlled by adjusting glomerular blood pressure 1. Autoregulation2. Sympathetic control3. Hormonal mechanisms: renin and angiotensin
23-23

Juxtaglomerular Cells dilate or constrict
arterioles secrete renin
Mesangial Cells Mysterious function Gap junctions
Macula Densa Cells monitors salinity inhibit renin release
23-24

Myogenic mechanism BP stretches afferent arteriole afferent
arteriole constricts restores GFR Tubuloglomerular feedback
Macula densa on DCT monitors tubular fluid for high salt and signals juxtaglomerular cells (smooth muscle, surrounds afferent arteriole) to constrict afferent arteriole to GFR
23-25
Why?

If BP constrict afferent arteriole and dilate efferent to bring GFR back to normal
If BP dilate afferent arteriole and constrict efferent
Stable for BP range of 80 to 170 mmHg (systolic)
Cannot compensate for extreme hypertension

Strenuous exercise or acute conditions (circulatory shock) stimulate afferent arterioles to constrict through both innervation and epinephrine effect
This results in GFR and urine production, redirecting blood flow to heart, brain and skeletal muscles
23-27

JG cells secrete renin when blood pressure drops
Renin is an enzyme that acts in the production of angiotensin II

23-29

Azotemia Uremia Glycosuria Pyuria Glomerulonephritis
Urinary incontinence Renal failure Oliguria Proteinuria UTI - cystitis

23-31
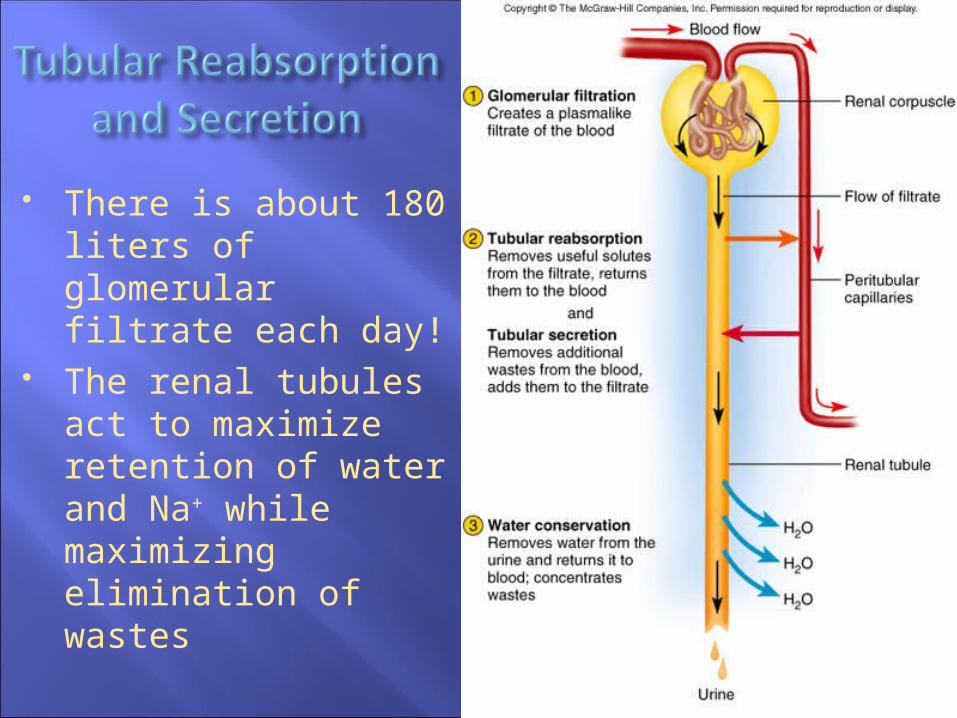
There is about 180 liters of glomerular filtrate each day!
The renal tubules act to maximize retention of water and Na+ while maximizing elimination of wastes

Blood has unusually high COP here, and BHP is only 8 mm Hg (or lower when constricted by angiotensin II); this favors reabsorption
Water absorbed by osmosis and carries other solutes with it (solvent drag)
23-33

Reabsorbs 65% of GF to peritubular capillaries
Great length, prominent microvilli and abundant mitochondria for active transport
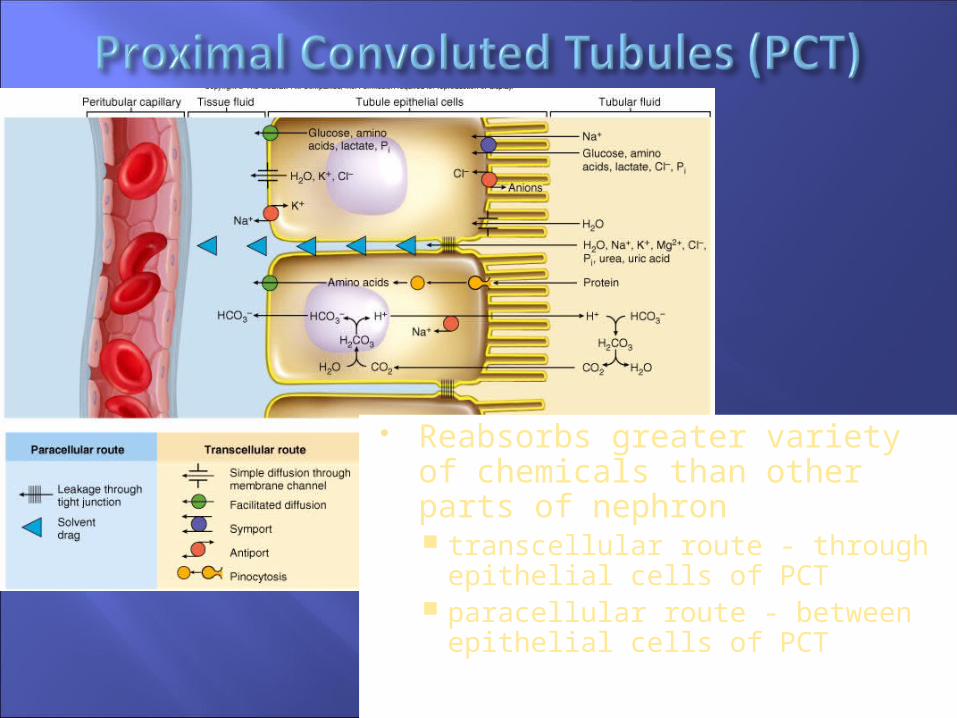
Reabsorbs greater variety of chemicals than other parts of nephron transcellular route - through
epithelial cells of PCT paracellular route - between
epithelial cells of PCT

Transport maximum when transport proteins of cell
membrane are saturated blood glucose > 220 mg/dL some
remains in urine (glycosuria) Solvent drag

Waste removal urea, uric acid, bile salts,
ammonia, catecholamines, many drugs
Acid-base balance secretion of hydrogen and
bicarbonate ions regulates pH of body fluids
23-37
Arcuate artery and vein
Arcuate artery and vein
Interlobar artery and vein
Primary function of nephron loop water conservation generates salinity gradient, allows DCT to concentrate urine also involved in electrolyte reabsorption

Principal cells (more abundant) – receptors for hormones involved in salt/water balance
Intercalated cells (lots of mitochondria) involved in acid/base balance K+ in, H+ out

Action affected by hormones ADH Atrial Natriuretic Peptide Aldosterone Parathyroid
Effect of ADH dehydration stimulates hypothalamus hypothalamus stimulates posterior
pituitary posterior pituitary releases ADH ADH water reabsorption urine volume

Atrial natriuretic peptide (ANP) atria secrete ANP in response to high blood pressure has four actions:1. dilates afferent arteriole, constricts efferent arteriole - GFR2. inhibits renin/angiotensin/aldosterone pathway3. inhibits secretion and action of ADH4. inhibits NaCl reabsorption
Promotes Na+ and water excretion, urine volume, blood volume and BP
23-40

Aldosterone effects BP renin release angiotensin II
formation angiotensin II stimulates adrenal cortex adrenal cortex secretes aldosterone
promotes Na+ reabsorption promotes water reabsorption urine volume maintains BP

Effect of PTH calcium reabsorption in DCT - blood Ca2+
phosphate excretion in PCT, new bone formation stimulates kidney production of calcitriol
23-42
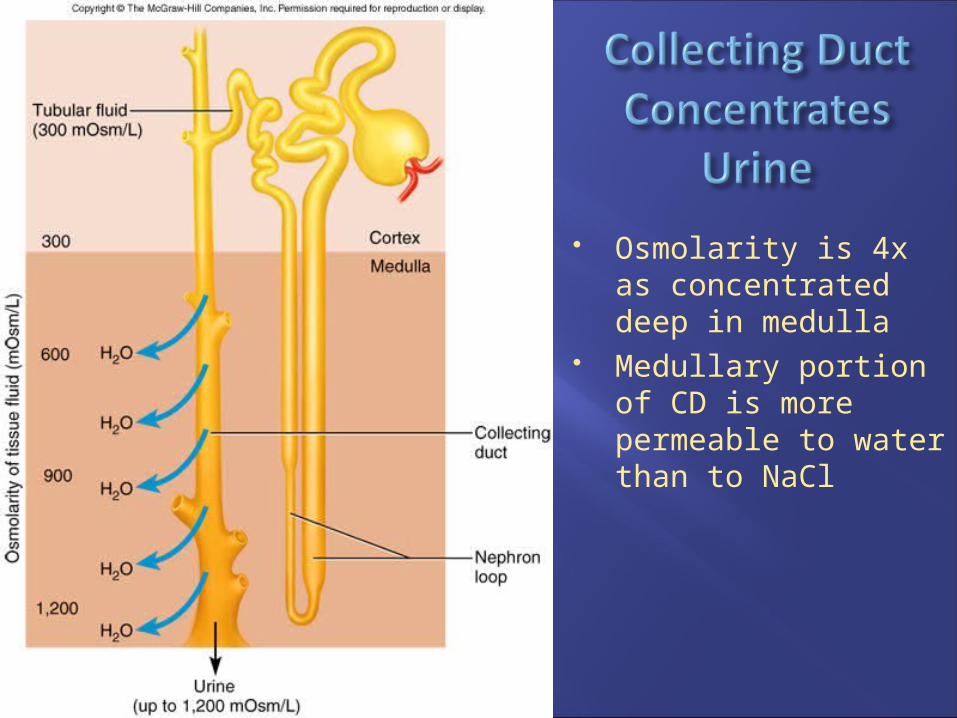
Osmolarity is 4x as concentrated deep in medulla
Medullary portion of CD is more permeable to water than to NaCl

Producing hypotonic urine NaCl reabsorbed by cortical collecting ducts (CD’s) water remains in urine
Producing hypertonic urine dehydration ADH aquaporin channels,
CD’s water permeability more water is reabsorbed urine is more concentrated is possible only because of the countercurrent
multiplier

Recaptures NaCl and returns it to renal medulla Descending limb
reabsorbs water but not salt concentrates tubular fluid
The thick segment of the ascending limb reabsorbs Na+, K+, and Cl-
maintains high osmolarity of renal medulla impermeable to water tubular fluid becomes hypotonic
Recycling of urea: collecting duct-medulla urea accounts for 40% of high osmolarity of medulla


Formed by vasa recta provide blood supply to medulla do not remove NaCl from medulla
Descending capillaries water diffuses out of blood NaCl diffuses into blood
Ascending capillaries water diffuses into blood NaCl diffuses out of blood



Some species of E. coli live harmlessly in your GI tract A few types of bacteria, usually E. coli strain O157:H7,
cause food poisoning and are nephrotoxic Shiga toxin enters the bloodstream, attaches to renal
endothelium and initiates an inflammatory reaction leading to acute renal failure (ARF)
The toxin also initiates destruction of RBCs and platelets

Appearance almost colorless to deep amber; yellow color due to
urochrome, from breakdown of hemoglobin (RBC’s) Odor - as it stands bacteria degrade urea to ammonia Specific gravity
density of urine ranges from 1.001 -1.028 Osmolarity - (blood - 300 mOsm/L) ranges from
50 mOsm/L to 1,200 mOsm/L in dehydrated person pH - range: 4.5 - 8.2, usually 6.0 Chemical composition: 95% water, 5% solutes
urea, NaCl, KCl, creatinine, uric acid

Normal urine does not contain glucose
Normal volume - 1 to 2 L/day Polyuria > 2L/day Oliguria < 500 mL/day Anuria - 0 to 100 mL/day

Chronic polyuria of metabolic origin With hyperglycemia and glycosuria
diabetes mellitus I and II, insulin hyposecretion/insensitivity
gestational diabetes, 1 to 3% of pregnancies ADH hyposecretion
diabetes insipidus; CD water reabsorption

Effects urine output blood volume
Uses hypertension and congestive heart failure
Mechanisms of action GFR tubular reabsorption

Renal clearance: volume of plasma cleared of a waste in 1 minute
Determine renal clearance (C) by assessing blood and urine samples: C = UV/P U (waste concentration in urine) V (rate of urine output) P (waste concentration in plasma)
Determine GFR: inulin is neither reabsorbed or secreted so its GFR = renal clearance GFR = UV/P
Clinical GFR estimated from creatinine excretion

Ureters (about 25 cm or 10 inches long) from renal pelvis passes dorsal to bladder and
enters it from below, with a small flap of mucosa that acts as a valve into bladder
3 layers adventitia - CT muscularis - 2 layers of smooth muscle with 3rd
layer in lower ureter urine enters, it stretches and contracts in peristaltic
wave mucosa - transitional epithelium
lumen very narrow, easily obstructed


Located in pelvic cavity, posterior to pubic symphysis 3 layers
parietal peritoneum, superiorly; fibrous adventitia rest muscularis: detrusor muscle, 3 layers of smooth muscle mucosa: transitional epithelium
Trigone: openings of ureters and urethra, triangular rugae: relaxed bladder wrinkled, highly distensible capacity: moderately full - 500 ml, max. - 800 ml

3 to 4 cm long External urethral orifice
between vaginal orifice and clitoris
Internal urethral sphincter detrusor muscle thickened,
smooth muscle involuntary control
External urethral sphincter skeletal muscle voluntary control

much longer than the female urethra
Internal urethral sphincter External urethral sphincter
3 regionsprostatic urethra
during orgasm receives semenmembranous urethra
passes through pelvic cavityspongy (penile) urethra

200 ml urine in bladder, stretch receptors send signal to sacral spinal cord
Signals ascend to inhibitory synapses on sympathetic neurons micturition center (integrates info from amygdala, cortex)
Signals descend to further inhibit sympathetic neurons stimulate parasympathetic neurons
Result urinary bladder contraction relaxation of internal urethral sphincter
External urethral sphincter - corticospinal tracts to sacral spinal cord inhibit somatic neurons - relaxes